
Improving discharge patient flow from acute settings
Contents
- For action: Improving discharge patient flow from acute settings
- Annex A: hotel accommodation
- Annex B: independent sector providers for hospital at home services
- Annex C: Designated Setting Indemnity Support
Classification: Official
Publication approval reference: C1055
To:
• CCG accountable officers
• Local authority directors of adult social care
• System discharge leads
CC:
• NHS regional discharge leads
• Chairs of local resilience forums
• NHS England and NHS Improvement regional directors
Dear Colleagues
For action: Improving discharge patient flow from acute settings
This letter sets out three schemes that systems can immediately implement for discharging people home from hospital. All of these options can be funded from the £588m hospital discharge ‘scheme two’ fund up until 31 March 2021. They will support a reduction in length of stay for people in hospital and ensure they are discharged when they no longer meet the ‘criteria to reside’ in a hospital bed.
- Use of hotel accommodation as a short term measure (days, rather than weeks) where there are delays in arranging care at home support – see Annex A for more details.
- Utilise the national framework for independent sector providers for hospital at home services and reablement/rehab services to immediately increase capacity in local providers – see Annex B for more details.
- Where local systems do not have an operating designated care home facility (due to issues with getting indemnity cover from their insurers), the Department of Health and Social Care (DHSC) will provide time limited indemnity cover to the small number of designated care home facilities that need this support – see Annex C for more details. In all circumstances, the current safe discharge policies set by the Government must be followed before any individual is discharged to a care home.
These options will not be needed in all areas of England, but can be used in any local system where they will make an immediate difference. Trust and clinical commissioning group (CCG) accountable officers must ensure the usual accounting and value for money controls are properly in place.Additionally, DHSC has announced £120m to support workforce in the social care sector. This will also support local systems to ensure enough social care workforce is available to support timely discharges from hospital.
Yours faithfully
Matthew Winn | Director of Community Health | NHS England and NHS Improvement
Annex A: hotel accommodation
Hotel accommodation can be used as an additional method to the usual discharge routes. NHS and local government partners, based on local need, will need to agree to implement hotels as a new destination on discharge from acute care. Use of hotel accommodation should only be used as a short term measure (days, rather than weeks) for the specific purpose of reducing length of stay for people in hospital and ensuring they are discharged when they no longer meet the ‘criteria to reside’ in a hospital.
The following groups may benefit from a hotel discharge scheme:
- Those who will be discharged on pathway 1 but are awaiting the start of care at home package of care
- Those awaiting community equipment and minor adaptations to their housing
- Those who are homeless/have no right of recourse to public funds/no place to safely discharge to
The care support provided to individuals in a hotel can be provided through any combination of unpaid and paid carers (operating in line with current Government lockdown guidance), Care Quality Commission (CQC) registered domiciliary care providers, virtual ward approaches, or utilising capacity of providers on the NHS SBS Patient Discharge Service Framework.
A simple set of data will need to be collected locally to ensure accountability on the use of public expenditure and to support evaluation of the effectiveness of this model of discharge. Data will need to include the number of hotel rooms used, length of stay and associated cost.
How do I discharge into hotel accommodation?
- All people transferring to the hotel should have a care and support plan that details their needs, organised by the discharge team.
- Careful consideration should be taken of an individual’s mental health and safeguarding needs as well as their capacity to consent.
- Local areas should ensure consent to transfer into the hotel accommodation is provided and recorded, in line with other discharge methods.
- Any person transferring to a hotel from a hospital will do so under the normal discharge planning processes in place in all areas of England.
- Local systems will need to ensure specific teams or individuals are identified to oversee the arrangements in the hotel and ensure the safe transfer of the person back to their home (with the right support) as soon as possible.
- Individuals are still entitled to normal health care support from primary care and community/mental health services during their time staying in the hotel including access to out of hours care services, as they would be if living in their own home. Local providers of this care will need to be alerted by the discharge teams with details of the hotels that people are being transferred into
Will there be additional registration or insurance requirements?
Any health or social care provided to a person within the hotel should be provided on the basis that the hotel is the person’s temporary address and as such, the usual indemnity/insurance cover of health and social care providers should apply. No additional clinical negligence or indemnity cover will be required. As the hotel will not be providing clinical services, they do not need clinical negligence cover. The usual hotel services that it provides would be covered by the hotels’ existing public and employers’ liability cover. Registration of the hotel with the CQC is not required. Registration of the provider who is providing the personal care is also not required if the provider is already registered with CQC.
However, these providers who are already registered, will need to notify CQC under Regulation 12 of the Care Quality Commission (Registration) Regulation 2009 of the change to their statement of purpose and to do this within 28 days of making these changes. If the provider of personal care is not registered with CQC, then registration will be required.
Where does accountability and responsibility lie?
Accountability for safe discharge into the hotel accommodation sits with the discharge authority, in line with Government national discharge guidance.
Clinical accountability for the care delivered within the hotel setting will lie with the organisations providing that care, as is the case in a person’s own home.
The hotel will be accountable for provision of all usual hotel services, including the cleaning regimes in line with government guidance for the hospitality sector.
Local systems should agree a lead organisation to be responsible for:
- The organising and booking of hotel accommodation
- Co-ordination of the required care and support for individuals to ensure use of hotel accommodation is a short term, interim solution and enables a timely discharge.
Existing safeguarding processes and escalation routes will apply to people transferred into hotel accommodation, in line with local arrangements. Consideration will need to be given to both the safety of the environment as well as the safety of individuals and suitability for them to transfer into the hotel and be supported there.
How do I book hotel accommodation?
There are two options available:
- Book space directly with a local hotel with costs being charged, via CCGs, into the hospital discharge scheme two budget
- Similar to that of booking accommodation for key workers throughout the pandemic, use the booking system provided by Corporate Travel Management (CTM), with pre-negotiated rates with a number of hotel operators across the country. This will involve using a specific booking code which is attributable locally but charged to the hospital discharge scheme two budget. The hotels used by CTM will all be able to fulfil the requirements to be used for the purpose of discharge.
CTM contact details: 01274 726424 (choosing ‘Hotel team’, then ‘Option 1’)
CTM email: Covid19@travelctm.com
Experience from existing hotel schemes and is that the lead-in time from standing up a hotel to accepting the first people is between two and 10 days, dependent on level of current staffing/activity.
What support is available?
Practical guidance is available including a hotel specification. This includes resources such as care plan templates and FAQs.
Support is available for case queries, support with planning and any other queries. Please email: england.covid-discharge@nhs.net.
Annex B: independent sector providers for hospital at home services
The approach uses independent sector organisations and capacity who must be commissioned in a complimentary and interdependent way with existing services and providers.
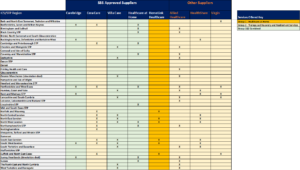
Where additional capacity is required, a national framework for Patient Discharge Services, managed by NHS Shared Business Services (NHS SBS), can be used to commission these services quickly through call off contracts. This framework is available for use by health and other public organisations and has 16 suppliers delivering services across three lots. There are two relevant lots:
Lot 1 (Discharge to assess services) – to support the recovery, rehabilitation and reablement needs of those discharged home.
Lot 3 (Medical Care at Home) – to support a wide range of subacute health service in peoples’ homes.
[NB: The independent sector providers covering the country are shown on the next page against each STP/ICS footprint. Where suppliers have capacity but are off framework, subcontracting options are possible through the framework and we would encourage you to speak directly with suppliers or to the national team for further information and support.]
What support is available?
Practical guidance is available. This includes resources and FAQs.
Support is available for case queries, support with planning and any other queries. Please email: england.covid-discharge@nhs.net.
For access to this framework please contact NHS Shared Business Services: NSBS.contractenquiries@nhs.net; tel: 0161 212 3940.
Further information can be found through the website.
SBS approved suppliers
Annex C: Designated Setting Indemnity Support
New arrangements have been established by DHSC to provide indemnity cover for care homes operating designated settings, specifically where insurance is the only barrier to the care home accepting COVID-19 patients on their discharge from hospital. The priorities are:
Priority A – the small number of designated settings that are ready to operationalise but insurance is the only blocker.
Priority B – care home providers already operating as a designated setting but at risk due to indemnity and insurance renewal challenges.
Priority C – local areas that need to stand up extra designated setting capacity quickly.
How is it to be implemented?
The scheme is administered by NHS Resolution on behalf of DHSC and requires NHS trusts to put in place sub-contracting arrangements with the care home on behalf of the local system.
The costs of the designated facilities will continue to be met from the funding made available to the NHS to support delivery of the Hospital Discharge Service (scheme two discharge budget). Reimbursement routes are set out in section 10 of the Hospital Discharge Service: Policy and Operating Model, dated 21 August 2020.
Funding will flow from the CCG to the NHS trust to the sub-contracted care home provider of the designated settings facility, via the payment provisions of the relevant NHS Standard Contract and sub-contract. CCGs will draw down from the hospital discharge scheme two budget as they currently do.
- The NHS aftercare service will be commissioned from the relevant NHS trust by the CCG in line with the published Government guidance for local authorities on commissioning designated settings. The trust’s existing NHS Standard Contract with the relevant commissioner(s) can be varied to incorporate this if necessary.
- The trust will transfer the person to the care of the operator of the designated setting, as a continuation of the commissioned pathway, sub-contracted to the care home operator of the designated setting.
- The NHS trust is thereby given and retains overarching clinical and care responsibility for the person/patient and holds the designated care home operator to account for delivery of that care via the sub-contract. The transfer to the designated setting is therefore a change in where the care is provided as the pathway continues rather than a discharge and start of a new pathway.
What support is available?
Support is available for case queries, support with planning and any other queries. Please email: England.bettercarefundteam@nhs.net