
NHS dental contract reform and arrangements letter
Contents
Publications approval reference: C1133
To: All NHS primary care dental contract holders
29 March 2021
An electronic copy of this letter, and all other relevant guidance from NHS England and NHS Improvement can be found online here.
Dear colleagues,
As the NHS restores patient access back to pre-pandemic levels across the breadth of its services and tackles the backlog of care, our dental teams have faced real challenges. The proximity between a dental professional and a patient’s airway and the relatively high proportion of aerosol generating procedures (AGPs) have affected the way care is provided. But thanks to the hard work and professionalism of dental teams, access for urgent dental care has been back at pre-pandemic levels for many months now, and NHS dental activity levels have risen safely and significantly. In February mean performance was 59% of contracted Units of Dental Activity (UDAs).
In December 2020, following discussion with the Department of Health and Social Care (DHSC) and NHS England, the return to usual pre-pandemic NHS contract arrangements was confirmed, ending income protection as rapidly as proves practicable.
However, we are also mindful that:
- current IPC arrangements will continue to act as a brake on full recovery
- practices want as much stability as possible, and the ability to plan ahead; and
- the profession seeks faster progress on reform of the current UDA contract.
DHSC commits to publishing this summer the results and lessons learnt from the dental contract reform prototypes, including the design and implementation challenges that prevent wider rollout beyond the current participating practices, in its current form. The commitment and engagement of the prototype practices throughout this period have generated invaluable learning, on which we will want to build.
DHSC has asked NHS England to lead the next stage of dental contract reform, working with the BDA and government, developing a revised reform process focused on designing implementable proposals that address the key challenges facing the delivery of NHS dentistry, leverage changes in the wider primary care system and meet the key tests described below. DHSC will work to gain cross government agreement to any proposals and expedite any necessary legislative change that is required as part of this necessary reform process.
For national contract reform to be viable, six aims need all apply.
Contract changes must:
- Be designed with the support of the profession
- Improve oral health outcomes (or, where sufficient data are not yet available, credibly be on track to do so)
- Increase incentives to undertake preventive dentistry, prioritise evidence-based care for patients with the most needs and reduce incentives to deliver care that is of low clinical value
- Improve patient access to NHS care, with a specific focus on addressing inequalities, particularly deprivation and ethnicity
- Demonstrate that patients are not having to pay privately for dental care that was previously commissioned NHS dental care
- Be affordable within NHS resources made available by Government, including taking account of dental charge income.
As part of the new process, should it prove possible to make rapid, modest and marginal changes to the existing national contractual arrangements, that are consistent with these six aims, we will do so at the earliest opportunity.
NHS England is also today sharing with its regional commissioners a new flexible commissioning toolkit that is intended to make it easier to target local dental priorities, using the flexibility that exists in the current contractual arrangements.
It is hard for dental teams to plan ahead with only three months’ notice. For this reason, we confirm today arrangements we expect to last for the first six months of 2021/22. We will monitor the impact of these new arrangements.
Contracts will continue to be in place for 100% of normal volumes, and our expectation is that all NHS funded capacity is used to deliver the maximum possible volume of safe care for patients. In recognition of the ongoing constraints to practice capacity due to COVID-19 there will be ongoing contractual protection for practices unable to deliver normal contracted activity for the first six months of 2021/22. During this period clawback will not be applied to practices delivering at least 60% of contracted UDAs and 80% of contracted UOAs (Units of Orthodontic Activity). The rate of clawback will then reduce linearly down to the existing lower threshold of 36% UDAs and 56% UOAs. Below these levels normal clawback will apply. The payment for activity not delivered, exempt from clawback by these arrangements, will continue to be adjusted by 16.75% to take account of variable costs not incurred.
The exceptions process will remain in place. Full guidance can be found here and there is a help desk available to support queries that can be contacted at this address: yearend@pcc-cic.org.uk
Prototype practices will be contacted separately.
The conditions of income protection remain as previously described, including that practices ensure that face-to-face urgent dental care is available for all attenders via direct contact or referral via 111, that efforts are directed towards patients at highest clinical risk, and to addressing health inequalities. Regional commissioners will also maintain arrangements for Urgent Dental Centres (UDCs).
Yours faithfully,
Ian Dodge | Executive Director of Primary Care, Community Services and Strategy | NHS England
Jo Churchill | Parliamentary Under Secretary of State Prevention, Public Health, and Primary Care | Department of Health and Social Care
Sara Hurley | Chief Dental Officer England
Annex: Contractual arrangements 1 April 2021- 30 September 2021
Figure 1: UDA threshold applicable from April to September 2021
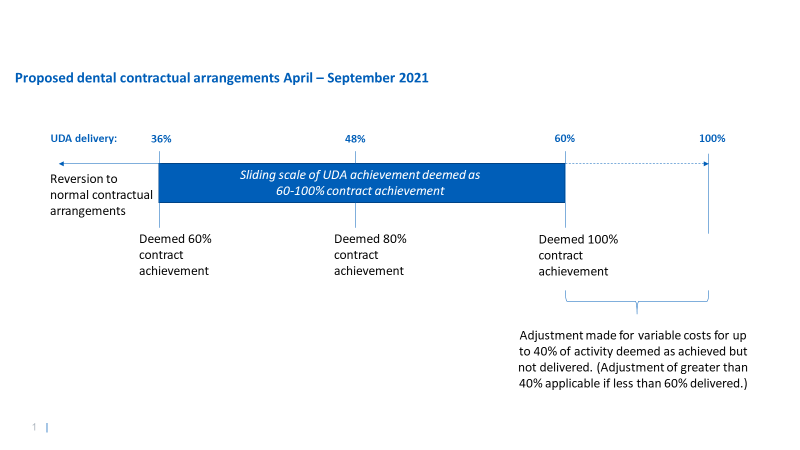
Where contractors deliver at least 60% of this 60% cumulative activity in April to September (ie at least 36% of contracted activity for this period), we will waive some clawback rights. If a practice delivers X% of activity, where X falls between 36% and 60%, delivery will be deemed to be (X/60) %.
For example, if 40.5% of contracted activity in this period is delivered, this will be deemed to be 67.5% of contracted activity in this period; or, if 53% of usual activity is delivered in this period, 53% / 60% = 88.33% will be deemed to have been delivered. Where contractors deliver less than 60% of this 60% cumulative activity in April to September (ie less than 36% of contracted activity for this period), contractors will be deemed to have delivered only the actual activity delivered in the months April to September.
Figure 2: UOA threshold applicable from April to September 2021
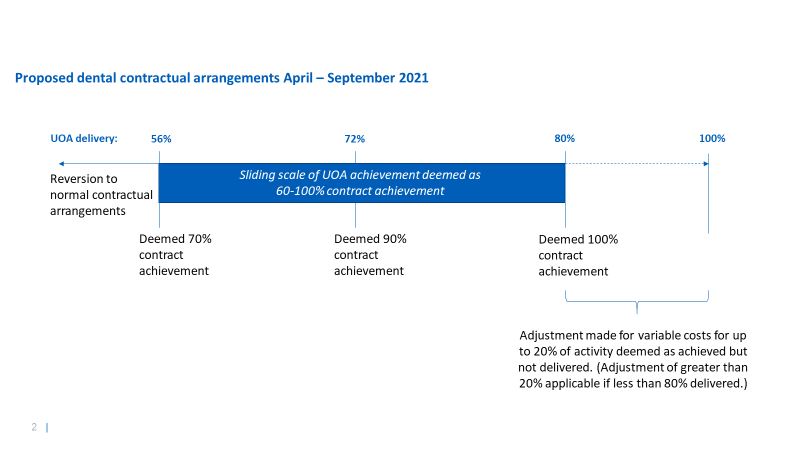
Where contractors deliver at least 70% of this 80% cumulative activity in April to September (ie at least 56% of contracted activity for this period), we will waive some clawback rights. If a practice delivers X% of activity, where X falls between 56% and 80%, delivery will be deemed to be (X/80) %.
For example, if 57% of contracted activity in this period is delivered, this will be deemed to be 71.25% of contracted activity in this period; or, if 73% of usual activity is delivered in this period, 73% / 80% = 91.25% will be deemed to have been delivered. Where contractors deliver less than 70% of this 80% cumulative activity in April to September (ie less than 56% of contracted activity for this period), contractors will be deemed to have delivered only the actual activity delivered in the months April to September.
Payment conditions
Practices are asked to meet, and declare that they have met, a set of conditions to be eligible for clawback rights to be waived. Breach of these conditions will result in the application of the usual contractual arrangements and clawback, instead of any waiver of clawback rights. We ask practices to make the following commitments:
- Maximise safe throughput to meet as many prioritised needs as possible.
- Remain open throughout contracted surgery hours and prioritise care for patients who are considered at highest risk of oral disease, in line with the prevailing dental SOP and guidance.
- Use NHS funding to the full for the provision of NHS services.
- Ensure full compliance with Clause 59 of GDS/PDS contract agreements – that practices will not advise that NHS services are unavailable with a view to gaining their agreement to undergoing the treatment privately
- Continue preventative work (such as confirmation via the FP17 data that best practice prevention advice has been given to patients) and target efforts in a way that will reduce health inequalities (eg by agreeing to see irregular attenders as well as usual patients). This will be auditable by local teams with an expectation that practices will be able to provide evidence of their efforts.
- Prioritise all known and unknown patients to the practice who require urgent dental care if contacted directly or via 111 services, as capacity allows.
- Keep contractual premises open throughout contracted surgery hours unless otherwise agreed via the regional commissioner.
- Complete and keep under review all staff risk assessments.
- Do not seek any duplicate or superfluous funding from the NHS or other government sources – including furlough or additional sick or parental leave pay that was not used to pay for cover.