
Speech by Simon Stevens, CEO NHS England, to the NHS Confederation Annual Conference 2014
Thinking like a patient, acting like a taxpayer – from NHS challenges to new solutions?
We meet here in Liverpool at a defining moment in the history of our National Health Service.
A time when the standards of care for the vast majority of our patients in the vast majority of our communities continues to be extremely high. For which we owe you, and the staff of the NHS, clear and unequivocal thanks.
But also a time of the most intense public focus ever on the quality and safety and dignity of our care. And rightly so.
Coinciding with the most sustained budget crunch since the Second World War. Now in Year Five of essentially flat health funding.
Against the backdrop of multiple fundamental, long-range, health challenges:
- the challenge of a growing population – three million more people in England by the end of the decade
- the challenge of an aging population – we now look after more pensioners than children
- the growing challenge of obesity, dementia, multimorbidity; alongside…
- more expansive and more expensive treatments.
These challenges are now quite well understood. The NHS Confederation’s ‘2015 Challenge’ lays them out well. The NHS, patients groups, professional bodies, successive governments, think tanks have also put great effort into classifying, describing and quantifying them.
But as I’ve spent the past couple of months out and about around the country, talking to clinicians and managers, listening to patients and carers, my sense is this.
We’re now done with analysing the challenges.
People want to get on with developing the solutions.
Of course thinking about tomorrow doesn’t mean we can take our eyes off today. This year we’re going to have to continue to move heaven and earth to guarantee our patients the high performance their lives are depending on. Speedy access to emergency services. Short waits for planned surgery. High quality cancer care. Modern mental health care. Safe staffing, compassionate care, and a culture of openness and improvement. And more besides.
So: Thank you for everything you’re doing. These achievements matter so deeply to the people we serve. Please keep on achieving! We should never compromise on these critical patient-facing standards.
—
I know there are enormous pressures. But the NHS is up for change. Necessity truly is the mother of invention.
So how do we mobilise for the next stage of the NHS’ journey – respectful of our history but not hostage to it?
A single national roadmap would be to miss the point. It’s the energy and commitment of NHS staff, of our patients and our partners that can generate the answers. Direction without dictation. Different answers for diverse communities. It’s hugely encouraging that three quarters of NHS staff say they can make suggestions about how care can be improved. Our task is to job is to make it far easier for these ideas to be acted on.
Today I want to offer some direction on some of the big ticket items we’ve got to solve for over the next five years, and perhaps reframe some of our recent debates. In doing so I won’t repeat the thoughts I shared on CCGs at their annual NHS Clinical Commissioners meeting, or the views I offered at the recent Kings Fund annual summit on the inclusive leadership the NHS now needs.
Instead today I specifically want to focus on three aspects of how we, as NHS leaders, can together take the next steps to improve care – and in so doing help future proof the NHS for years ahead. They are:
First, by improving the sophistication of our commissioning system. A new focus on outcomes for patients and value for taxpayers.
Second, by accelerating the redesign of care delivery, with far greater local flexibility to meet the health and social care needs of the people we serve.
And third, by actively exploiting the fundamental transformations now occurring in modern western medicine. Shifting the frontier of what is possible.
1. NHS commissioning for outcomes and value
So let me start with commissioning. What are we trying to achieve?
NHS commissioners exist to unleash more health and care bangs for the buck. To drive greater value than would be obtained from just perpetuating the status quo.
Talk to the public and to patients – as I’ve been doing around the country – and there’s quite wide agreement about what our fellow citizens want from the NHS. It’s neither surprising nor unreasonable – which doesn’t mean it’s easy or inevitable. Our neighbours, relatives, colleagues, want reassurance that care will be readily available when it’s needed. Care that’ll be safe, treatments that work, services where the left hand and the right hand know what they’re doing. Staff who always take patients’ dignity and preferences seriously. Care that is fair and non-discriminatory and non-wasteful. In short, an expectation that all of us who work in the NHS will think like a patient and act like a taxpayer.
At a national level, these broad democratic aspirations are fleshed out through the Mandate, which the elected government now sets for NHS England – and through us for the NHS.
So for anyone who wants to know what NHS commissioners are here to do, these are the five overarching domains we are tasked with improving. This is how our impact will ultimately be judged:

The simple clarity of these outcomes – which require some incredibly complex causal chains – should constantly prompt us to question why we’re doing things a particular way. That’s where commissioning comes in.
As a nation we’ve just taken the unique step anywhere in the world of entrusting frontline clinicians with two thirds – £67 billion – of our health service funding. Many CCGs are now harnessing clinical insight and energy to drive change in their local health systems in a way that frankly has not been achievable before now.
Here’s a practical example. On Sunday evening as I was thinking about this speech I pulled the data off the web for Liverpool CCG. These show that as commissioners, as a health system, as a community here in Liverpool, if we can reduce premature deaths to levels similar to other comparable communities – I’m not talking Cheshire or Surrey, so this is a relevant comparison – we can save 409 lives a year, in these specific disease areas alone. 400 families no longer losing a loved one in their prime. That’s why we’re here.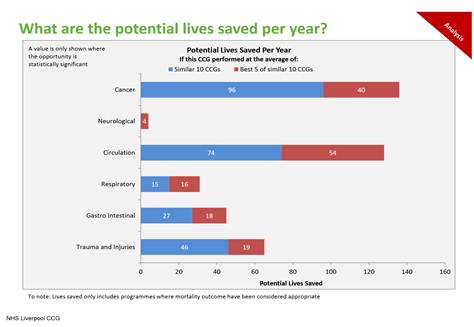 Tackling the wider determinants of health. But also aligning providers’ funding with the improvements we want to see. How we do so will vary by the type of service being commissioned, and will evolve at different paces in different parts of the country. Over time – in partnership with Monitor – we’ll be testing new reimbursement models for some elective conditions, an expansion of ‘year of care models’ for people with long term conditions, and alternative funding arrangements for emergency and urgent care. We need to focus on care pathways, for example to better connect the commissioning of bariatric surgery with upstream preventive action on obesity. Or to better connect the specialised commissioning of £1 billion of medium and low secure psychiatric services with local mental health service planning.
Tackling the wider determinants of health. But also aligning providers’ funding with the improvements we want to see. How we do so will vary by the type of service being commissioned, and will evolve at different paces in different parts of the country. Over time – in partnership with Monitor – we’ll be testing new reimbursement models for some elective conditions, an expansion of ‘year of care models’ for people with long term conditions, and alternative funding arrangements for emergency and urgent care. We need to focus on care pathways, for example to better connect the commissioning of bariatric surgery with upstream preventive action on obesity. Or to better connect the specialised commissioning of £1 billion of medium and low secure psychiatric services with local mental health service planning.
We need to take a new look at incentives. NHS England is currently expecting to spend up to £2.7 billion on various performance incentives for community and acute providers (CQUIN), for GMS GPs (QOF), and for CCGs (Quality Premium). We’ll be undertaking a hardnosed review of how these various schemes are structured, and what we’re getting for the money.
More broadly, across all NHS-funded services, we’ll be pushing for a steadily increasing proportion of payments tied to performance, quality and outcomes. And different approaches to sharing utilisation risk for particular services along the spectrum, from volume-based payments at one end through to delegated capitated budgets at the other.
We’ll be using a combination of evidence from the NHS’ past experiences, new local experiments, and learning from established international commissioners to calibrate these new commissioning approaches appropriately.
We’ll also be raising the sophistication of NHS commissioning in various other respects, including:
- coherent, timely and actionable information for commissioners.
- a pragmatic look at the evolving division of labour between CCGs, CSUs and NHS England.
- driving our world-class quality and safety transparency agenda, in partnership with CQC.
- new ways of giving individual patients more clout.
- working with local authorities on effective ways of targeting joint budgets, including the Better Care Fund.
- working with the Third Sector on new ways to commission services – for people with learning disabilities, with cancer, and with mental health problems, for starters.
- flexibly supporting new models where the commissioner/provider split is differently placed along the demand/supply continuum.
- in partnership with Public Health England, beginning to measure and manage not just the ‘flow’ of health care consumption, but the ‘stock’ of population health risk (which in time would convert into future health care consumption).
- giving consideration to population-based virtual commissioning budgets that blend primary care, local hospital and community, and specialised services, as a basis for fairer allocations.
- defining more rigorously the data that will be used to reveal whether commissioners themselves are doing a good job.
These actions will be important enablers of the broader care improvement we want to bring about.
2. Redesigning care models
Which brings me to the second major theme I want to talk about this afternoon – how we accelerate the redesign of care delivery, with far greater local flexibility to better match the health and social care needs of the people we serve.
Rather than constantly debating the reorganisation of our management tiers, let’s now ask the more profound questions about how care is actually being delivered.
And, by the way, there’s almost no administrative permutation that hasn’t at some time or another been contemplated in the NHS. Here are secret cabinet papers discussing a future reorganisation:
“Proposals for an integrated [health] service had been generally welcomed. [But] the reorganised Health Service would not come under local authority control…the Ministerial Committee were unanimous that it was ruled out by considerations of financial accountability and by the opposition of the medical profession. The Government was answerable to Parliament for the NHS; and the Accounting Officers concerned had to answer to the Public Accounts Committee for the expenditure involved. Efficient management would be of critical importance…it should include individuals whose training and experience comprised both medical and managerial skills.”
The same Cabinet meeting also decided that health services for the under 5s should be a local authority responsibility, and debated the London underground, top salaries in the public sector, and flooding of the Thames.
That was January 1970. Harold Wilson as Prime Minister, Dick Crossman was Secretary of State.
—–
But while historical debates on NHS management structures have a somewhat repetitive quality to them, the way health care itself is actually delivered continues to evolve.
Like every health system in the western world, medical advances and the search for efficiency mean the NHS has been developing new services – and closing unneeded beds – since the day it was created. Antibiotics for TB, antipsychotics for mental health problems, fast acting anaesthetics and minimally invasive surgery – all have cut the time patients have to spend in hospital.
The Birmingham maternity hospital where I was born has long since closed. The children’s hospital where as a boy I was a patient for a couple of months – long gone. The Victorian psychiatric hospital I once ran – closed. The general hospital where I started work – now a community hospital. Guys and St Thomas’ – merged but thriving.
In each case I say: fair enough. Our vital interest – as patients and as staff – is in care and health, not bricks and mortar. Yes we do need healing facilities and modern equipment, but the where, and the how, is bound to keep changing. For good reason, some beds and buildings will doubtless continue to close over the coming decade, just as they will in France, Germany, the US, Canada, Australia, Sweden and any other country you care to name.
Some treatments are going to be further concentrated. Acute stroke services are the example du jour, and the stroke patients I met recently at Charing Cross Hospital who’d be blue light ambulanced from across North and West London – often driving right past other hospitals on the way – would certainly agree.
Which is why – under the fantastic leadership of Bruce Keogh – at NHS England we’re working with commissioners and hospitals across the country to designate 40-70 major emergency centres, alongside roughly the current number of existing emergency departments.
And as we take a hard look at NHS England’s £14 billion portfolio of specialised commissioning, on grounds of quality or efficiency for some tertiary conditions we are going to choose to work with a smaller number of leading hospitals. Our selection of these long term partners will also be influenced by the maturity of the relationships these hospitals exhibit, both in terms of win/win contractual behaviours over the next 12-24 months, and their shared understanding of the medium term financial context within which the whole NHS is having to operate.
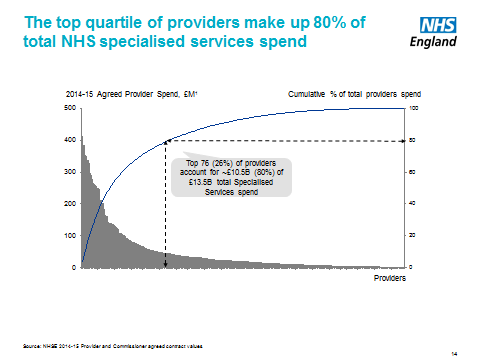
Although 175 service lines across 280 providers are now defined as ‘specialised’, just 76 providers account for 80% of the spending. So we need a more realistic categorisation.
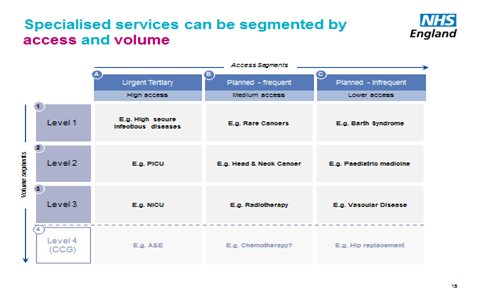
 For those our commissioning approach will be influenced in part by access and quality/volume considerations. Only around a third of current spend is for planned, infrequent services where access considerations are of least importance. And only about 10% is for highly specialised / rare conditions. So we’re clearly not talking about centralising £14 billion of care.
For those our commissioning approach will be influenced in part by access and quality/volume considerations. Only around a third of current spend is for planned, infrequent services where access considerations are of least importance. And only about 10% is for highly specialised / rare conditions. So we’re clearly not talking about centralising £14 billion of care.
 —
—
But how typical are these sorts of specialised services, where greater concentration is now required?
Nye Bevan famously said he “would rather be kept alive in the efficient if cold altruism of a large hospital than expire in a gush of warm sympathy in a small one”. (In fact he died, at home, in Buckinghamshire.)
But partly as a legacy of tightly controlled NHS spending from the late 1970s until the late 1990s, England now has quite concentrated acute services, with a stronger degree of regionalisation than in many other western nations. Even our smaller acute hospitals tend to have an average of around 400 inpatient beds, and there is little convincing evidence that the minimum efficient scale is higher than that. Monitor are doing similar empirical work in this area, and will be publishing their findings soon.
In any event, beds are increasingly an anachronistic currency for assessing the clinical content of a local acute hospital, a community or cottage hospital, an urgent care centre, an elective care centre, an expanded primary care centre and so on. This traditional taxonomy is now blindsiding us to new ways forward.
Now I know there are pushes and pulls here.
A push for larger hospitals often driven by aspirational medical staffing norms, and in some cases by local recruitment difficulties. And competing claims about safety, which is why my colleagues Bruce Keogh, Tim Kelsey and Jane Cummings are rightly pushing so hard for transparency of safety and quality data.
Just as there’s been a push for centralisation there’s been a pull for more local and community-orientated services – increasingly feasible as other countries are showing through new technologies including e-consultations, remote monitoring, teleradiology and even e-ICUs. Let’s also remember that treatment approaches are never static – the history of medicine is the history of the diffusion of tests or procedures, that yesterday were the preserve of the teaching hospital and tomorrow will be out in the community clinic. Miniaturisation and digitisation are cutting scale effects and speeding diffusion.
The changing needs of our patients – often frail, some with dementia, many with comorbidities – and the changing opportunities offered by new treatments and technologies mean that if we think creatively and if we challenge some of our self-imposed constraints we’re going to find we’ve got some new options.
What do I mean by self-imposed constraints? As was widely reported last week, coming back to the NHS after a decade of working internationally I’ve been struck by certain features of how we organise care. While we tend to regard them as self-evident, they are in fact just contingent choices whose original rationale is now either forgotten, irrelevant or on balance unhelpful.
I agree with the Royal College of Surgeons that inflexible European Court reinterpretations of what the European working time directive was meant to achieve are undermining medical training in some specialities, and distorting hospital provision in some geographies. We do of course need high quality training for the next generation of health professionals – we should never go back to the days of overworked and overtired junior doctors that was widespread when I started work for the NHS in the 1980s. But does our historical assumption hold for all time that just about every NHS acute hospital needs a full complement of trainee doctors to keep services afloat? That may have been a pragmatic response during the decades when the number of hospital consultants was so constrained. But with a 76% increase in full-time-equivalent NHS hospital consultants since 2000, what if some smaller NHS hospitals decided on a different medical staffing model, more akin to that of some European hospitals?
And just to pursue the argument, as the Royal College of Physicians Future Hospital initiative has shown, consultant expansion has often meant more subspecialisation which while desirable in its own right has sometimes fragmented care for older inpatients with multimorbidity – who of course are now the majority of medical inpatients on any given day. One study has shown that using single condition-specific guidelines a 79-year woman with type 2 diabetes, hypertension, COPD, osteoarthritis and osteoporosis could be prescribed 19 doses of conflicting and adversely interacting medicines each day.
That’s why some would like to see more general physicians or ‘hospitalists’ working alongside consultant specialists. Together with advanced nurse practitioners, sessional GPs, and networked staffing arrangements with neighbouring trusts. In our heart of hearts we know that, despite the theoretical flexibilities offered by Agenda for Change, to date much of this work has been assigned to the ‘too difficult’ box. It’s good to see NHS Employers, Health Education England, and a number of the medical royal colleges all now beginning important work in this area.
But let me clear. I am definitely not suggesting a wholesale reorganisation of medical training and staffing across England.
What I am arguing is that medical training and staffing should not drive the wholesale reorganisation of district general hospitals across England.
The tail should not be wagging the dog.
If we want to be evidence-informed in our policy making and commissioning lets pay heed to research from Martin Gaynor, Mauro Laudicella and Carol Propper at Bristol University. They’ve spotted the striking fact that between 1997 and 2006 around half of the acute hospitals in England were involved in a merger. Their peer-reviewed results found little in the way of gains.
So rather than uncritically adopting the merge and centralise as our overriding ‘meme’, let’s go with ‘horses for courses’.
In some places mergers and traditional reconfigurations will – after careful stress-testing – clearly be needed, and they will have NHS England’s full support.
But let’s also allow complementary models to emerge, be tested, and adapt over time, in different communities, reflecting their different legacy care patterns and the heterogeneity of their patients.
In many places our current models are successful and durable. But here are a few examples of some potential new variants:
- In many parts of the country there’s now real momentum building in favour of testing some new models of general practice and extended primary care.
- And what if in a few parts of the country – rather than perpetuate the increasingly arbitrary boundary between GP and community-based care on the one hand, and hospital-based outpatient, diagnostic and even some inpatient care on the other – these health professionals and perhaps even social services wanted to form new multispecialty provider groups? Perhaps taking delegated multiyear budgets to manage defined populations, while committing to use the dividend from more efficient team working to put the local NHS on a sustainable financial trajectory?
- What if some of these groups decided to team up with their local community or acute hospital?
- Or what if some decided the exact opposite – to have direct admitting rights to the local hospital without managing it, perhaps funding the marginal costs of admissions on an activity-based payment, and the facilities’ fixed costs on a unitary payment.
- Or what if some of these smaller hospitals, realising the benefits of shared back offices, informatics, and wanting to spread know-how about efficient care processes, chose to form non-contiguous networks with other like-minded institutions across the country?
- And what if for some services – as patients gain more influence over how their own care is commissioned – we see groups of midwives coming together to offer packages of support in the way that the Women’s Institute and NCT have argued many women want but aren’t always currently able to get? What if we saw new types of mental health services that help expand access to IAPT-type therapies for the millions of our fellow citizens living with untreated anxiety and depression? Or following the terrible situation at Winterbourne View, more user and carer- directed local, non-institutional services for people with learning disabilities overseen by the Third Sector?
Each of these ideas – and several others like them – offers some promise.
But none of these ideas should be imposed on the NHS, as a national blueprint or reorganisation.
Instead, what I want to see – and I’m confident this is a shared view with Monitor and TDA – is an NHS that is more flexible, more adaptable, where national and local thinking converges to create different clinically and financially sustainable paths for particular communities.
And in every case we should embark on them only having very carefully stress-tested the assumptions on which they are built. The new models need to show how they help solve the particular issues confronting that particular health community. With proper safeguards against unintended consequences. Patients need to be able to make meaningful choices. Providers showing they are equitable, can meet high clinical standards, and live within the locally sustainable funding envelope. There’ll need to be independent evaluation, and regular performance benchmarking against comparable areas. With periodic opportunities to decide whether to continue, with or amend, the arrangements.
3. Harnessing the coming innovations in modern medicine.
When you’re in the heat of the here and now it’s sometimes hard to stand back and see some of the bigger changes unfolding, some of the wider opportunities ahead. But now is the time to do that.
I say that in part because I believe that all industrialised countries stand on the cusp of at least three quite fundamental shifts in the practice of modern medicine. Will we in the NHS embrace them and harness them to our cause – or will we wait for them to wash over us, while trying to muddle through? That’s our choice.
First, personalisation. A decade and a half on from the Human Genome Project, we’re still in the early days of the clinical payoff. But as biology becomes an information science, we’re going to see the wholesale reclassification of disease aetiologies. As we’re discovering with cancer, what we once thought of as a single condition may be dozens of distinct conditions. So common diseases may in fact be extended families of quite rare diseases. That’ll require much greater stratification in individualised diagnosis and treatment. From carpet-bombing to precision targeting. From one-size-fits many, to one-size-fits-one.
The NHS should be at the forefront of this global medical revolution. That’s one reason why I’m announcing today that NHS England will be launching a competitive process for the nation’s leading teaching hospitals and clinical research centres to join the UK’s new 100,000 genome programme – one of the world’s highest profile initiatives in this area. We expect to issue the ITT at the end of this month, followed by two bidders’ days and final submissions in July, and the announcement in the autumn of the successful wave one trusts who will begin sample acquisition in early 2015. In parallel we will be consulting on moving to a new model for regional genetics labs to upgrade and industrialise NHS capabilities in this area.
We’re never going to be the country that pays the highest prices, or that adopts new treatments regardless of how well they work – just so we can say we’re ‘innovative’. We’ll happily leave that accolade to others. But what we should be is rigorously pro-science, pro-research, and pro-the rapid spread of useful improvement. That’s where AHSCs and AHSNs have such an important role. If we get our act together, what the NHS potentially has to offer – that many other health systems don’t – is a unique combination of biomedical research, population-orientated primary and specialist care serving diverse patient groups, longitudinal data (to allow matching of phenotypes wit genotypes), an aligned financing system, and a rigorous focus on value creation.
A second area where we’re going to see major opportunities is by using data to drive transparency, quality improvement and the move to more proactive and anticipatory care. For example, researchers have shown that real time analysis of clinical data from electronic health records could have identified increased risk of heart attacks associated with one diabetes drug at least five and half years earlier than actually happened. Similarly while cancer outcomes have been improving dramatically – Cancer Research UK point out that half of all cancer patients now survive at least 10 years, compared to only a quarter in the 1970s – we also know that perhaps a quarter of cancer patients are only diagnosed when they arrive in A&E, and that as result their prognoses are substantially worse. So proper data linkage between GP systems and hospitals and other health care providers to create secure, confidential longitudinal information that allows us to target prevention and quality improvement, as well as help discover new treatments and cures, is essential if the NHS is to deliver for the people of England. That’s why getting programmes such as care.data right is so fundamentally important.
Third, we stand on the cusp of a revolution in the role that patients – and also communities – will play in their own health and care. Harnessing what I’ve called this renewable energy is potentially the make-it or break-it difference between the NHS being sustainable – or not. That’s why NHS England has, for example, just launched an initiative to support 150,000 people with so-called patient activation tools. It’s why we’re backing the new NHS Citizens Assembly. It’s why a number of patient groups are arguing for personal health budgets that put service users in control. It’s why we should be doing more to support the 1.4 million full time unpaid carers across the country. It’s why the £500 million-worth of volunteer support for the NHS (which I suspect is an underestimate) should be nourished and stimulated. Above all it’s why we should recognise that achieving change in the NHS is not merely a techno-rationalist activity, it’s health as a social movement, working with communities and civil society organisations and local government and faith groups and patients groups and many others.
So – a coming revolution in biomedicine, in data for quality and proactive care, and in the role that patients play in controlling their own health and care. The NHS has to grab these opportunities with both hands, rather than just letting them wash over us, or hoping they’ll bypass us so we can carry on with business as usual.
An NHS five year Forward View
So these are the sorts of questions and ideas we will be working with you, with other NHS bodies, and with our partners on over the coming months. By the autumn – and following NHS England’s Call to Action last year – we’ve committed to giving our point of view on the NHS over the next 5 years.
Not a “5 Year Plan” with a capital ‘P’– that can’t be done in isolation from knowing what NHS funding will be over the next Parliament. But a 5 Year “Forward View”. Which clearly describes the opportunities in front us and the big ticket questions we need to solve. The sort of new care models that could succeed. The more locally permissive policy and regulatory environment that would support them. Alternative scenarios for demand and for efficiencies – and what both imply. The comparative advantages that a National Health Service offers – and how we can further capitalise on them. And how investment in the NHS supports a prosperous and growing Britain.
Nationally we will be working with other key partners on these critical questions. Locally our next steps – together with Monitor and TDA – will be to compare and triangulate your 5 year views which each CCG and provider will have drafted by the end of June. We will use those to identify the particular pressure points and constraints that stand in the way of sustainable solutions. In early July we’ll then set out the next steps locally on the forward strategy process.
—-
The last time the NHS faced one of its defining moments was in the early 2000s. Under quite different economic circumstances we received a big cheque from the British people for catch-up investments in 160,000 more health professionals, modern infrastructure, better cancer and cardiac care, and an end to notoriously long waiting times. Payment systems to stimulate activity and hold down inflation, hospital governance to incentivise institutional performance were both means to those ends.
But the challenges facing us today are somewhat different, and so we should be open-minded and pragmatic about how we move forward. Of course resourcing will matter. But let’s also think more creatively about our options – disentangling means from ends, and discarding false dichotomies.
Then let’s pay the same attention to effective implementation as to creative system redesign. Let’s chart out what it’s going to take. And then get on with it.
So let me end where I began.
I know times are tight, and the NHS is under great pressure.
But the British people’s support for our health service is undimmed.
The need for the superb care our staff strive to offer has never been greater.
So if we pull together, I’m optimistic we can get this right.
Thank you for everything you do.