We want to hear from you. Help us understand your digital experience by taking part in our user research. Find out more now.

Executive summary and action required
Following the previous Board paper outlining a risk assessment and proposed changes required to Board risk appetite, an updated proposal on our approach to improving data transparency was requested. This proposal builds on feedback from the Board and reflects;
- the expectation for a shift in organisational culture towards the 10YHP ambition to become the most transparent health care system in the world. To release all (aggregate/non-disclosive) data by default, consistent with the November Board discussion– which considered the risks balanced against the mitigating safeguards.
- a more permissive environment for sharing of aggregate data across the NHS, where legal and governance advice is sought where there is specific legitimate cause for a potential exception to the sharing of aggregate data default position.
We outline in this paper the approach that the NHS England Data and Analytics sub-directorate has taken, under the above instruction, to improve data transparency, to support the improvements expected in quality of care and accountability, in line with the commitments of the 10YHP. Our approach ensures that robust safeguards are in place to protect patient data and privacy, upholding public trust and confidence. We have established an interdisciplinary team to take this work forward, working closely with colleagues across Programmes, medical directorate and the National Quality Board. Further work is required to communicate and embed a more permissive pro-transparency culture across our NHS England and the wider NHS system.
We ask the NHS England Board to:
- Note the establishment of a new priority programme of work within Data & Analytics for “Reporting, Insights, Publications & Transparency”
- Note early deliverables including information for the public (NOF, League Tables) and changes to our user-access policy (for the NHS) to be more permissive by default
- Approve the proposed next steps to release ‘Open Benchmarking’ data aligned with the 10YHP ambition.
- Discuss the required frequency and any initial focal areas for reporting back to this Board (and National Quality Board)
- Discuss how to engender wider organisational support and promotion of the pro-transparency culture and expectation for open data sharing by default
Context
1. The 10 Year Health Plan, Fit for the Future stated ambition is to “make the NHS the most transparent healthcare system in the world”. NHS England Board has also reiterated the expectation that NHS aggregate data/insights should be shared openly by default. A more permissive and open approach will empower people to make informed choices and hold services to account, while also driving service improvement through openness and accountability.
2. Early progress on some of the 10YHP transparency commitments has been made via the publication of the public data dashboard, updates to user-access policies for analytical tools across the NHS, and the NHS oversight framework including the publication of segmentation and league tables.
3. The expectation is to continue to build upon these foundations and improve access to data and insights across the health service. At the 6 November 25 Private Board a paper responding to an ask regarding risk review and risk appetite was presented. In response, the Board provided a steer to:
- Confirm the organisational position and culture must be pro-transparency, with aggregate data release and sharing as the default, consistent with the 10-Year Health Plan and supporting effective performance management and improvement
- Drive a cultural shift to establish a permissive environment for aggregate data sharing, where legal and governance advice should be sought on specific cases rather than used to shape organisational policy, acknowledging a higher risk tolerance at Board level.
4. Our work on improving transparency, both within and across the NHS and for the public has been categorised into three dimensions, with the initial focus being on points (a) and (b) below as pre-requisites, and to establish the change in organisational position and permissive culture. The three categories are:
- Improving access for NHS professionals: Providing wider and more permissive access to operational and aggregate data/statistics and metrics within and across the NHS to support delivery and improvement.
- Working openly by default: Open access to insights designed for the NHS (e.g. benchmarking tools) so that analysts, researchers and interested parties beyond the NHS can also support service improvements driven through openness and accountability.
- Tailored public insights: Providing meaningful data and insights which are curated to public/patient need. Co-create content with and for the public, in accessible forms, to support patient choice and accountability.
5. The work of Reporting, Insights, Publications and Transparency team, is also contributing to, and aligned with the forthcoming Quality Strategy and National Quality Board remit to derive a core set of quality measures and to lead the delivery of the commitments of a ‘new transparency of quality of care’ from the 10YHP.
Progress to date and proposed future approach
6. The 10 Year Health Plan makes a series of transparency commitments; it recognises transparency as key to achieving the three big shifts at pace “ushering in a new era of transparency” and sharing the ambition to “make the NHS the most transparent health care system in the world”, including the publication of “easy to understand league tables”. Internally, increased transparency leads to more informed decision-making, supports cross-team collaboration, drives up quality standards and can help drive efficiencies. There are also significant reputational benefits; research has shown that increased transparency is a key factor in building public trust and accountability
7. In late 2025 we established the Reporting, Insights, Publications and Transparency interdisciplinary team across data and analytics, to focus on improvements in data transparency, reporting and automation. David Ashby (Director of Clinical and Improvement Analytics) is leading this programme of work with our Chief Statistician (Chris Roebuck) and Analytics lead for the Exec team (Lara Dearing).
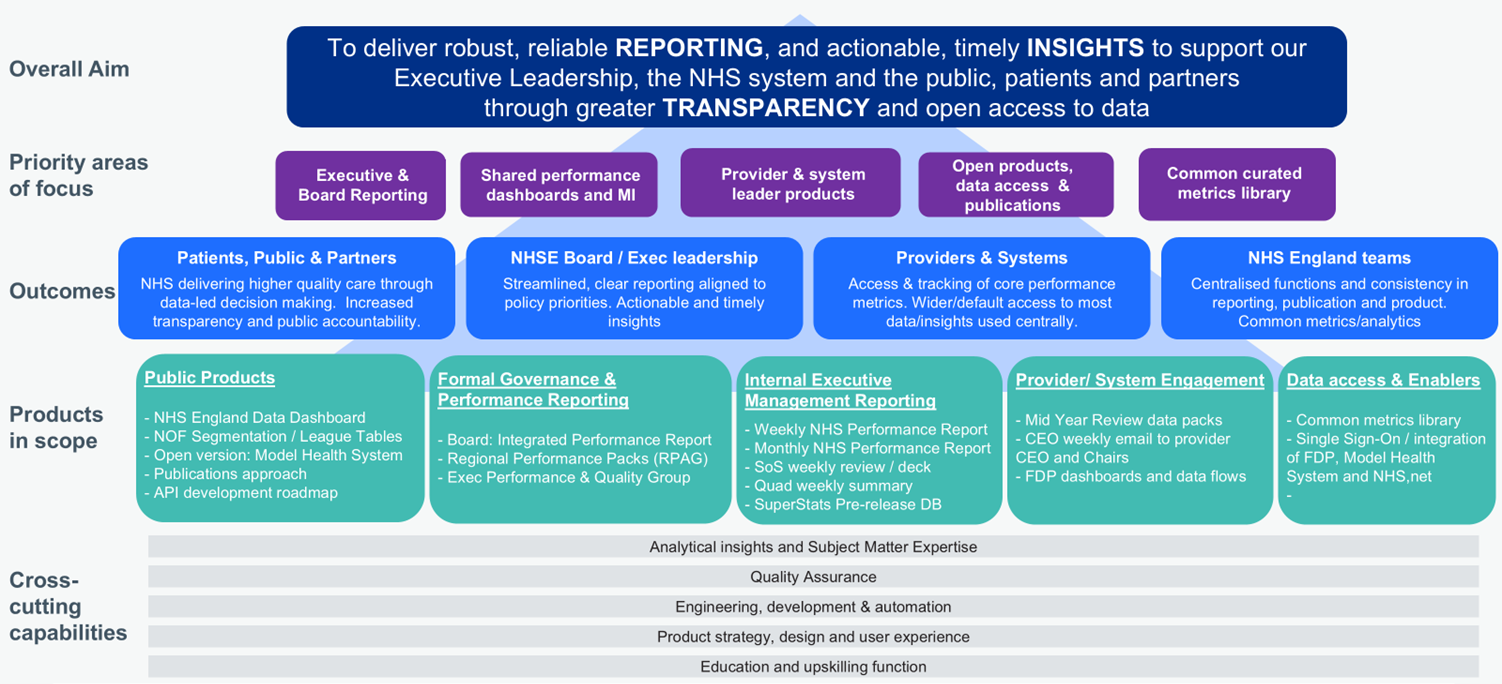
8. Our aim is to lead and stimulate transparency becoming embedded across the system. This will empower people to make informed choices and hold services to account, while also driving improvement through openness and accountability. We have outlined in Annex A how we envisage bringing together the various elements across Reporting, Publications and Transparency.
9. Our focus for the programme starts with NHS England and national aggregate data. We need to create a more permissive, open and transparent culture where data-sharing across the NHS is the norm, and where more aggregate/non-disclosive data insights and products are openly available to the public by default. We will work across the three areas defined in Point 4 above – and have sought to make early progress with both (a) improving access for NHS professionals; and (b) working openly by default. The tailoring of insights, specifically curated for patients and the public, will be part of the forthcoming Quality Strategy and requires close alignment with Digital (NHS App) and Comms/Strategy teams.
10. The default approach of the programme is to publicly release aggregate data in line with the organisational risk appetite, with specific legal or governance advice sought only where there are specific cases for them to answer. We have already released more accessible data insights for the public through our NHS England data dashboard and publication of an interactive dashboard to support the NHS Oversight Framework, segmentation and league tables.
11. An update was provided to NHS Executive Board in late 2025, following the creation of the Reporting, Insights, Publications and Transparency team, and detailed early deliverables of the team including:
- For the public:
- Release of NHS Oversight Framework (NOF) public dashboard , provider segmentation and ‘league tables’
- Release of the NHS Acute Provider Table dashboard of monthly provider performance across seven key operational statistics.
- Working openly by default – Opening access to aggregate clinical, operational and productivity benchmarking through the Model Health System
- Changes to user-access policy across the entire NHS
- Updated log-in (using NHS.net) to enable easy access
- Open variant (no login required) developed for release in Q4
12. The demand for data and insights across our products continues to grow:
- On the initial launch of the NOF and league tables (September 25), we achieved over 550k unique users in the first 24hrs of launch.
- The Federated Data Platform Performance Overview Dashboard (POD) has over 2,700 registered users, with 93% ICB penetration
- Over 2000 users registered attendance at our Model Health System and NOF webinar in September.
- The Model Health System has over 76,000 registered users and 100% penetration at both Provider and ICB level. Usage is equivalent to 1,200 users per working day, with growth at 11% over the last year.
Recent progress to achieve a more permissive approach to NHS data access
13. In late 2025 we initiated a number of user-access policy changes to our benchmarking insight tools on model.nhs.uk. These changes now enable all NHS staff, as registered users, to access all Model Hospital / Model Health System data for all Providers and Systems.
14. Furthermore, to promote more permissive access and reduce friction when trying to access data, we developed and released a feature which enables any individual with an NHS.net email to access aggregate data held within the Model Health System, using their NHS.net credentials.
15. This means that theoretically, everyone with a valid NHS.net account can now enter the Model Health System, without the additional friction of having to register separately for access. We outlined more in the November 2025 Board paper on access controls and risks, and deem there to be sufficient safeguards in place with these aggregate, non-disclosive data to utilise the NHS.net to identify. This also means that our scope has extended beyond Provider and ICB staff. As a result, the Model Health System can now potentially be accessed by approx. 1.6m users across the NHS. Wider access to the NHS Model Health System enables more leaders and clinicians to identify unwarranted variation, share best practice, and drive consistent improvements in quality, productivity and patient outcome.
16. These access changes also provide the foundations for cleaner integration across the NHS FDP and Model Health System so that user-journeys and data/visualisation access is simplified into one place.
17. We have also developed a ‘open benchmarking’ variant of the Model Hospital which will enable unrivalled public-access to NHS benchmarked data and visualisations, aligned with our ‘working openly by default’ commitment. This is planned to be ready for release from late February 2026 and will be a significant step forward in 10YHP commitments including providing public access to clinical improvement data (e.g. GIRFT). A summary of the proposed content to release in the first public/open version of the Model Hospital is in Annex B.
18. Disclosure control options for the public release of the Model Hospital/Model Health System have been discussed at the Disclosure Control Panel and the recommendation reviewed by DDaTC.
19. Segmentation and League Tables: We have now also released the Q2 refresh of the NHS Oversight Framework (NOF) segmentation and league tables publicly – allowing members of the public to understand NHS providers’ overall ranking and drill into individual metrics to understand their performance in more depth. This includes the publication of a NOF public dashboard and the NOF compartment in Model Health System. A summary of changes between Q1 and Q2 has also been released.
20. We have delivered a set of public-facing tables and charts summarising NHS organisations’ monthly performance, using best practice Government Digital Service standards for accessibility. We will expand the content of this to cover other areas and have developed a section for public launch summarising workforce and activity changes through time.
21. Key deliverables that the Reporting, Insights, Publications and Transparency team expect to deliver over coming months include:
- Launch the public workforce and activity dashboard (Exec request)
- Launch Open Benchmarking / Model Health System open version
- NOF public dashboard refresh (accessible replacement for PowerBI)
- New weekly reporting Executive Dashboard (NHS FDP)
- Automated weekly, monthly and Board reporting packs
Additional future considerations, interdependencies and wider implications
22. We have identified five wider domains relevant to our transparency work, which are being considered and may warrant a future discussion at DDaTC, NQB and/or Board. These are summarised as points of note in paragraphs 23 to 27 below. We would welcome further discussion on any of these points as requested by Board.
23. Open APIs for third parties. Developing a new era and culture of transparency across our organisation and the NHS will also create significant opportunity for third party organisations to develop solutions, insights, narrative and outputs to support accountability and quality improvement. We expect to release much of our data as open APIs (a service offering connections online to enable automated use of the underlying data) for third parties to use and develop. We would be interested to understand the Board’s appetite for NHS England to actively promote and stimulate engagement with media, researchers, commentators and industry to utilise these data to develop new content and insights.
24. Access to data for Research and innovation: The approach outlined here has focused on data used within/across the NHS and for information to provide to the public/patients. However, additional consideration regarding expediting more timely access to data assets for research (e.g. record level, potentially disclosive/sensitive health data – e.g. HES data, PROMS, registries, activity, etc). This area is being led our Data Access and Partnerships team and would involve consideration of the Data Access Request Service (DARS) and the Sudlow review, HDRS investment, etc.
25. Clinical audits and registries: The ‘Outcomes & Registries Directions, 2024’ originated from the government response to the Cumberlege Inquiry and place expectations on unifying our approach to clinical audits and registries whilst also building new assets such as the Medical Devices Outcomes Registry (MDOR). Making these data more readily and consistently available has been considered within the work of the Audits & Registries expert reference group and ‘Best Practice Guide’. Focus on this, and the expectations to transform our approach to this clinical data area will be considered in the forthcoming Quality Strategy.
26. Beyond NHS care; the independent sector: Data transparency across sectors (including into private/independent sector provision) is complex. Much of our focus to date has been on improving transparency in NHS funded/delivered care. However, it is recognised that quality improvement across sectors to improve patient experience and reduce harm is critical. The Paterson Inquiry Recommendation 1 included expectations around transparency across ‘whole practice’ of a clinician’s work. Again, discussions are ongoing to ensure that whilst we continue to deliver in improving NHS transparency that we are also supporting and partnering to improve transparency across sectors.
27. Public-curated content: Our focus to date has been in improving transparency across the NHS and working openly to improve accountability. This is necessary, but not sufficient. Further work is required to align relevant data and insights into the NHS App and nhs.uk to support choice and local accountability. Again, as part of the Quality Strategy links are being made to ensure future NHS App development roadmaps consider the expectations and commitments outlined in the 10YHP.
28. Finally, it should be noted that there remains a delivery risk (to timescales) as a result of the potential loss of up to a third of the internal NHS England analytical capacity through the Voluntary Redundancy Scheme. This, coupled with existing vacancies is equivalent to a reduction of 49% of analysts compared to our full establishment. Whilst the delivery of this programme of work is a priority across Data and Analytics, we expect to need to re-organise and rebalance the teams and portfolio. We must also ensure that the public transparency of data assets and insights is sustainable – and that we have sufficient resource allocated to deliver updates once released, to mitigate against data quality concerns and/or knock-on reputational impact and public trust.
Annex A: Outline summary for the new multidisciplinary team; Reporting, Insights, Publications and Transparency
Annex B: Summary of proposed content to be released in the open-access Model Hospital (Q4 25-26)
B.1. In Q4 (late Feb/early March 2026) we expect to be ready to release a public/open version of the Model Health System in line with commitments made in the 10YHP and forthcoming Quality Strategy. Initial focus areas are listed below and primarily cover areas benchmarked for clinical improvement, including supporting the GIRFT programme.
B.2. For the initial release we are proposing to include a wide range of compartments. These cover various acute clinical areas from specialties like anaesthetics and perioperative medicine, to areas like orthopaedics and general surgery. Much of this reflects our clinical improvement programme work with GIRFT, from which we will share metrics that provide meaningful data and insights to support patient choice and accountability. We are also including compartments focussed on care settings like outpatients, diagnostics, imaging, productivity and efficiency. We are also reviewing metrics on workforce and population metrics for strategic commissioning.
Proposed data areas for initial candidate release of the public Model Health System | |
|
Alcohol |
NHS Oversight Framework |
|
Anaesthetics & Perioperative Medicine |
Obstetrics |
|
Antimicrobial Resistance |
Ophthalmology |
|
Blood Transfusion |
Oral & Maxillofacial |
|
Breast Surgery |
Orthopaedic Surgery |
|
Cardiology |
Outpatients |
|
Clinical Audits |
Outpatients Quality Improvement |
|
Culture, Staff Experience, and Engagement |
Paediatrics |
|
Dentistry |
Pathology |
|
Dermatology |
Patient Safety |
|
Diabetes & Endocrinology |
Plastic Surgery & Burns |
|
Ear, Nose & Throat |
Productivity & Efficiency |
|
Endocrine Surgery |
Respiratory |
|
Equality, Diversity & Inclusion |
Rheumatology |
|
Estates & Facilities |
Spinal Services |
|
Evidence Based Interventions |
Strategic Commissioning Insights |
|
Gastroenterology |
Tobacco |
|
General & Acute Medicine |
Urology |
|
General Surgery |
Vascular |
|
Geriatric Medicine |
Waiting Times |
|
Gynaecology |
Wellbeing |
|
Imaging |
|
|
Medical & Clinical Oncology |
|
|
Mental Health Quality Improvement |
|
|
Neurology |
|
B.3. The content areas selected for the initial launch (above), are of higher data quality due to clinical involvement and mature datasets. Therefore, the risk of misinterpretation of data is reduced, which will further be mitigated by overarching notes / caveats displayed on the product. Due to the scale of the release, the risk of misinterpretation will not entirely be eliminated but this should be outweighed by the positive impact of transparency.
B.4. The chart below is an example variation chart showing the variation in length of stay for primary hip replacement across all providers in a single time period. In addition it can also be presented as a trendline, showing the chosen providers value against the national median, peer median and a benchmark or target level where relevant.
