
1. Introduction and methodology
The NHS Patient Survey Programme is delivered by the Care Quality Commission (CQC) on behalf of NHS England and the Department of Health and Social Care. The Survey Coordination Centre at Picker, coordinates the NHS Patient Survey Programme on behalf of CQC. There are five surveys within the Programme: Adult Inpatient, Maternity, Children and Young People, Community Mental Health and Urgent and Emergency Care Surveys.
This report has been produced by Solutions Strategy Research Facilitation Ltd (Solutions Research) and NHS England to share national insights from qualitative thematic analysis of written responses provided by respondents that took part in the NHS Patient Survey Programme. The aim of this endeavour is to identify opportunities for learning and improvement through an in-depth understanding of experiences of care.
The focus of this report is on the Children and Young People’s Patient Experience Survey 2024, which captured feedback from 25,821 children and young people and their parents and carers. The sampled patients were aged 15 days to 15 years at the time of discharge and had received care in hospital during March, April and May 2024.
Further information on the survey is available on the CQC website.
Qualitative data analysis
Two open questions were included in the survey which allowed respondents to use their own words to respond. The questions were positioned at the end of the survey and included the instructions as follows:
- Parents of 0-7, 8-11 or 12-15: ‘Is there anything else you want to share about your child’s time in hospital? For example, anything really good or that could have been better.’
- Children aged 8-11 or 12-15: ‘Is there anything else you want to share about your time in hospital? For example, anything really good or that could have been better.’
To ensure a robust approach a purposive sampling method was used for thematic qualitative analysis:
- Parents of children aged 0-7, 8-11 and 12-15: 630 comments were analysed as a sample from 11,103 viable comments.
- Children aged 8-11 and 12-15: 631 comments were analysed as a sample from 5,526 viable comments.
Once the total sample of 1,261 comments had been analysed it was seen that data saturation had been reached i.e. no new themes were emerging from the data. Had this not been achieved, additional comments would have been added to the sample as necessary, in line with best practice in qualitative analysis. Further detail can be found in Appendix 5: Methodology and Appendix 6: Sampling Approach.
Use of illustrative quotes
Throughout the report, quotes are included to illustrate respondents’ experiences in their own words and substantiate the findings. Quotes indicate if the respondent is a parent or carer (parent/carer of a child aged x), a child or young person (CYP aged x), and the age of the child (0-7, 8-11, 12-15). Please note that the data is not edited in the interests of correct spelling and punctuation for example, to stay as true to the words of respondents as possible.
Certain information from the qualitative comments used in the report has been redacted to protect the identity of survey respondents and any other individuals referenced. Information that has been removed includes:
- names of patients or staff replaced with “[name]”
- names of wards, units or hospitals replaced with “[location name]”
- names of specific services replaced with “[service name]”
- specific dates replaced with “[date]”
Use of quantitative data
Where possible in the findings section, themes are presented in context of the most relevant quantitative survey data. This allows for insights to be considered more holistically and to provide a greater opportunity for reflection and learning.
Statistics from the parents and carers sample reference the question number using ‘Qp’, and statistics from the children and young people sample reference the question number using ‘Qc’. To reflect the statistical release, results for the two cohorts are reported separately.
When analysing the comments provided in the child section of the survey, a small number of these were interpreted as likely to have been written by a parent/carer judging by the terminology used (e.g. ‘my child’). Where quotes from these comments have been used, that is indicated in brackets following the quote.
Context to support interpretation
There is evidence that some respondents were not solely commenting on the specific hospital visit they were asked about in the survey. Some feedback referenced multiple visits or visits to multiple hospitals if not also experiences of other NHS services.
Comments reveal varied reasons for the patient visiting the hospital, including planned and emergency visits and a range of length of stays which included those who had not stayed overnight. These factors shaped how patients and their parents/carers responded to their experience. Themes are closely interwoven and often interlink, and this report highlights these connections throughout. For instance, good communication to many parents/carers and children and young people was underpinned by feeling listened to, which was influenced by multiple factors spanning the themes of ‘Staff’, ‘Treatment’, ‘Communication’ and ‘Discharge and aftercare.’
Where feedback varied by age of child or where a theme was only found in one age group, this is highlighted in the report. If no distinction is made the findings are applicable to all ages of children.
2. Headline findings
Thematic analysis of the qualitative data revealed the following key themes:
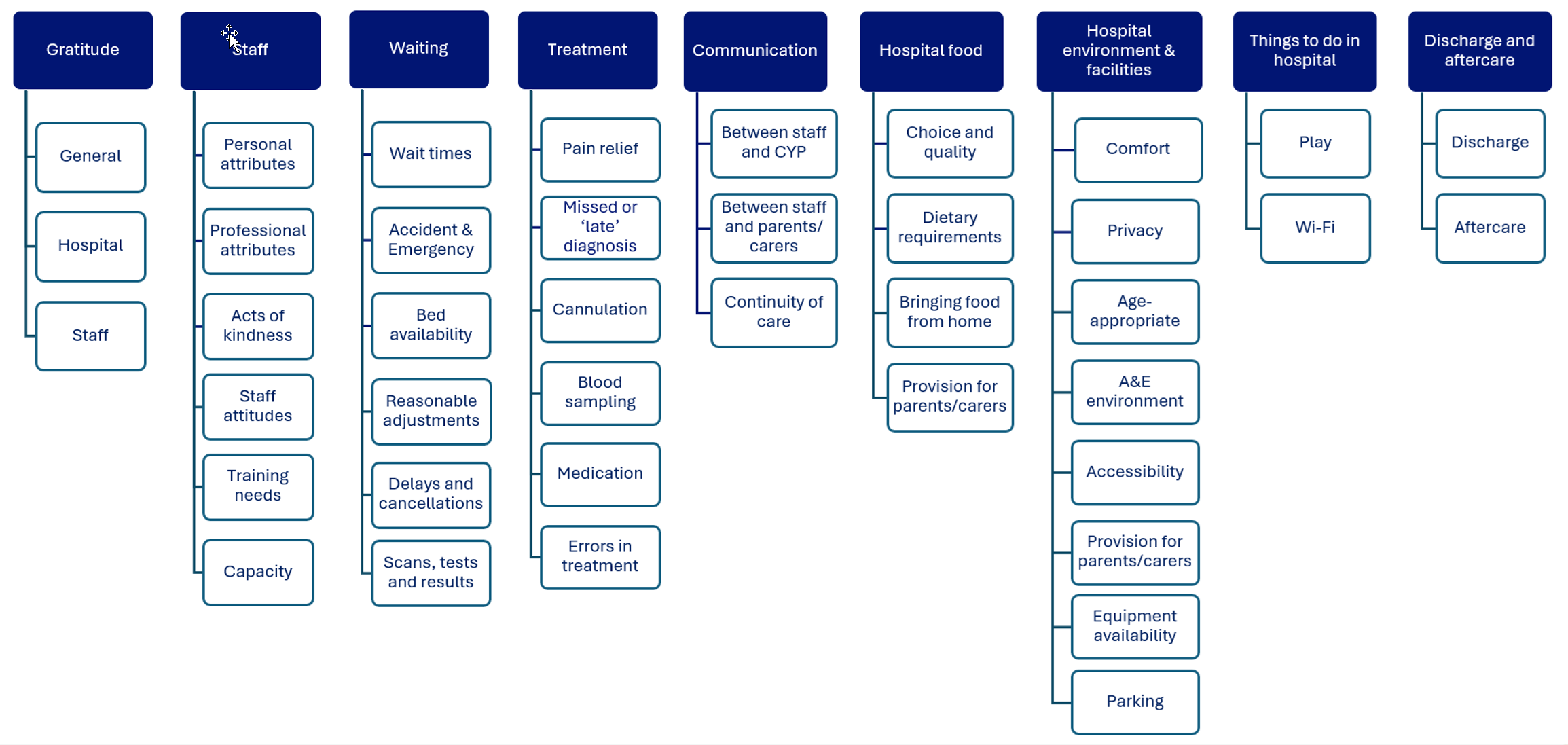
Image text:
Gratitude
- General
- Hospital
- Staff
Staff
- Personal attributes
- Professional attributes
- Acts of kindness
- Staff attitudes
- Training needs
- Capacity
Waiting
- Wait times
- Accident and Emergency
- Availability of beds
- Reasonable adjustments
- Delays and cancellations
- Scans, tests and results
Treatment
- Pain relief
- Missed or ‘late’ diagnosis
- Cannulation
- Blood sampling
- Medication
- Errors in treatment
Communication
- Between staff and CYP
- Between staff and parents/carers
- Continuity of care
Hospital food
- Choice and quality
- Dietary requirements
- Bringing food from home
- Provision for parents/carers
Hospital environment and facilities
- Comfort
- Privacy
- Age-appropriate
- A&E environment
- Accessibility
- Provision for parents/carers
- Equipment availability
- Parking
Things to do in hospital
- Play
- Wi‑Fi
Discharge and aftercare
- Discharge
- Aftercare
3. Key themes
Nine key themes were identified from the thematic analysis, listed below. Within each key theme are several sub-themes which support interpretation and use of the insights. There are 40 sub-themes in total.
- gratitude
- staff
- Waiting
- treatment
- communication
- hospital food
- hospital environment and facilities
- things to do in hospital
- discharge and aftercare
This section of the report contains the detail of each theme with a range of quotations shared to substantiate and exemplify the experience of respondents using their own words.
Theme: Gratitude
What does the quantitative survey data tell us?
- 71% of parents/carers of 0 to 7-year-olds said their child was ‘very well’ looked after in hospital (Qp70)
- Of parents/carers of 0 to 7-year-olds who left a viable comment, 66% said their child was ‘very well’ looked after in hospital (Qp70)
- 73% of CYP aged 8 to 15 said they were ‘very well’ looked after in hospital (Qc26)
- Of CYP aged 8 to 15 who left a viable comment, 68% said they were ‘very well’ looked after in hospital (Qc26)
A recurring theme was expressions of gratitude, with both general praise and appreciation specified to hospitals or staff involved in the patient’s care.
General
Overall gratitude was a key theme for parents and carers, most often expressed broadly or at the NHS generally. For some this was the only comment made. Some children and young people also shared positive sentiments about their experience overall.
“Very happy! 😘 Thank you for taking care of me!” (CYP aged 8-11)
“Every thing is good !Thank you for all kind of help.” (CYP aged 8-11)
“I will always remember your amazing effort. Kind regards, NHS.” (CYP aged 8-11)
“I think it was amazing.” (CYP aged 8-11)
“Experience in hospital was perfect.” (CYP aged 12-15)
“We thank the NHS for all the hard work they do and for always looking after my little boy.” (parent/carer of child aged 0-7)
“I was well pleased with how my daughter was attended to and how the whole procedure went.” (parent/carer of child aged 0-7)
“Very grateful for the NHS, wonderful care and treatment.” (parent/carer of child aged 8-11)
“I truly appreciate the NHS for handling surgeries like my son’s so efficiently.” (parent/carer of child aged 8-11)
“Brilliant excellent care all round.” (parent/carer of child aged 12-15)
An observed pattern in comments from parents/carers was gratitude when there was clarity on the treatment plan.
“My son was treated well in hospital and had a clear plan of treatment when he left. This condition is now resolved. Thank you for your help.” (parent/carer of child aged 8-11)
“The staff were great I have so much respect for what they do and the treatment plan we now have in place to manage my child’s asthma has meant a real improvement in her symptoms and management of her condition.” (parent/carer of child aged 8-11)
Hospital
Parents/carers and children and young people sometimes extended thanks to the hospital where the patient was treated.
“It was a very good hospital and the staff are. Very nice. Thank you.” (CYP aged 8-11)
“I want to use this opportunity to thank the trust and the wonderful team for the sincere love they’ve shown during our visit to (location name) hospital.” (parent/carer of child aged 0-7)
“I can’t thank enough the staff at (location name) that supported us and took care on my son. I have never received a bad word or attitude from any staff member. They’re all very special and meant to work in a hospital.” (parent/carer of child aged 12-15)
“The team in the (location name) centre for children and young people have provided us with excellent care over the years, this last visit was also very good.” (parent/carer of child aged 12-15)
Staff
Other comments highlighted specific teams or staff roles when expressing gratitude.
“My baby was looked after really well by the nurses and doctors and I have no complaints. I’d like to thank them all for their support.” (parent/carer of child aged 0-7)
“My overall experience was good and I will say kudos to the paediatric department of (location name).Thanks.” (parent/carer of child aged 0-7)
“The ladies and men that work in neonatal are the real superheroes, they looked after him so well I can’t thank them enough, they saved his life. They will always hold a special place in my heart.” (parent/carer of child aged 0-7)
“The whole experience was fab. From our Initial conversations with the surgeon, to our care on the day.” (parent/carer of child aged 12-15)
Individual staff were singled out, seen in both parents/carers and children and young peoples’ feedback, even if the latter did not always remember the person’s name. Expressions of gratitude about staff links to the ‘personal attributes’ sub-theme later in this report though comments were less detailed on specific qualities that drove their positive interactions.
“A big thank you to Dr (name)and Dr (name) for their care through the years.” (CYP aged 8-11)
“The lady who spoke to me about going to sleep was really funny and me feel less worried I have seen her before and I think she remembered me I liked her a lot please tell her I said thankyou.” (CYP aged 8-11)
“I do want to send a thank you to the nurse in Urgent care who looked after me when I nearly passed out in that waiting room.” (CYP aged 8-11)
“Dr (name) and his team including everyone who dealt with (name) were incredible – an absolute credit to the hospital and NHS. Thank you!” (parent/carer of child aged 0-7)
“The staff have been amazing, I would like to personally thank Mr (name) and his team for sorting my son and also the nurses, (name), (name), (name) and the play specialist (name) too. All have been amazing during our hospital stay and made it much easier for both myself and my son. They should be so proud of the jobs they do!” (parent/carer of child aged 0-7)
“I wanted to put on record just how impressed I was with the playworker, who came to talk to my son and helped explain what a general anaesthetic would be like, in non-frightening terminology. She literally turned around what had been a very scary and stressful morning and turned (name’s) tears into smiles.” (parent/carer of child aged 8-11)
Theme: Staff
What does the quantitative survey data tell us?
- Among parents/carers of 0 to 7-year-olds, 64% said they ‘always’ had confidence and trust in the staff caring for and treating their child (Qp52)
- Among CYP aged 8 to 15, 81% said staff looking after them were ‘very’ friendly (Qc11)
Staff have a pivotal role in shaping the experience of both children and young people, and their parents and carers, when visiting hospital. The comments demonstrate how each individual staff member can have meaningful impact on patient experience.
Personal attributes
Positivity about staff and the personal attributes they displayed was the most prevalent theme in feedback from both parents/carers, and children and young people. This was articulated as staff being gentle, nice and kind.
“I liked how everyone was gentle and caring with me. I liked how they tried to keep me happy or cheer me up. I really liked all of it. Thank you! ☺️.” (CYP aged 8-11)
“The Dr’s and nurses were nice and looked after me.” (CYP aged 8-11)
“The staff I had were very nice and chill.” (CYP aged 12-15)
“(Name) was very kind.” (CYP aged 12-15)
“All staff were kind, compassionate and patient.” (parent/carer of child aged 0-7)
“Anaesthetist was a super kind and very caring lady a real credit to your team as we’re all who helped us during our visit.” (parent/carer of child aged 8-11)
“They’re all very good and they all very nice and my child was very happy with them.” (parent/carer of child aged 12-15)
“Staff were, without exception, fabulous/kind/thorough.” (parent/carer of child aged 12-15)
“The staff was absolutely wonderful—they were so gentle and patient, always making sure my child felt safe and comfortable.” (parent/carer of child aged 12-15)
Play therapists were highlighted by both parents and carers and children in feedback, as having a positive impact on their experience.
“The play therapist was the best thing about the whole experience. She was able to get my son to do things he wouldn’t have done otherwise. She made sure his special needs were met and was really brilliant.” (parent/carer of child aged 0-7)
“The staff on the day op ward were fantastic, as was Play specialist [name]. Fantastic care, compassion and empathy.” (parent/carer of child aged 0-7)
“The playworkers were absolutely brilliant.” (parents/carer of child aged 0-7)
“The lady that came to my room and did paintings with me and printed pictures of Pokémon people I like, she was really kind to me.” (child aged 8-11)
“The play therapist was amazing she helped me qhen I was scared her name was [name] she made my experience much better.” (child aged 8-11)
“Play specialists really help, can they come on the weekend?” (parent/carer of child aged 8-11)
In a few cases, parents/carers and children and young people, mentioned support staff and their positive attributes that made them stand out during their visit.
“Amazing tea staff.” (CYP aged 12-15)
“The nurses, doctors, play staff and cleaners were very nice.” (CYP aged 12-15)
“Domestic staff were great, kind, smiley and respectful.” (parent/carer of child aged 0-7)
Professional attributes
There was also positive feedback about the efficiency, competence and professionalism of staff which made patients and their parents/carers feel reassured and safe. This was noted more often by young people aged 12 to 15.
“All staff were really warm and professional.” (CYP aged 8-11)
“(Name) our allergy nurse always is very knowledgeable about me and always helps and reassures me.” (CYP aged 12-15)
“The asthma team have always wanted what I want to be better, they have helped me so much and are always lovely, when the first lot of injections did not work they made it so I had a different one which is better.” (CYP aged 12-15)
“I truly appreciate the NHS for handling surgeries like my son’s so efficiently. They managed everything quickly, and I was pleased with the efforts of everyone involved from the moment we arrived at the hospital.” (parent/carer of child aged 8-11)
“Appointments and operations have always been arranged promptly and run very smoothly to ensure the best outcomes. We feel so lucky to have worked with, and continue to work with, such an amazing team!” (parent/carer of child aged 8-11)
“All staff were absolutely fantastic, extremely professional and helpful, and they went above and beyond to help my son with his operation both before and after.” (parent/carer of child aged 12-15)
Some parents/carers, and patients had positive experiences with staff who demonstrated understanding and sensitivity, including an example of a video being a useful tool to explain to a child what was going to happen to them.
“I am autistic and have ADHD, so I don’t like talking to people I don’t know or making eye contact with them. When my mum told the staff this, they were quite good at respecting that. I don’t like long waits. Most of the time I was seen quickly, but some of the time not. I get annoyed and find it hard to not get cross, and to sit still, even though mum brings things for me to do and my phone. This makes everything more stressful for me. But everyone was nice and kind.” (CYP aged 8-11)
“My little boy since he was a baby, has been in & out of hospital with bronchitis, as his got older, nearly every time he gets a cough & cold, he also gets a viral wheeze, my boy has autism & is non verbal, every time we come to hospital he does get really distressed & refuses to take medication, every single doctor or nurse we’ve seen over the years have been outstanding! They’re so patient with him, are sympathetic towards him & me as his mom, as you can imagine it’s heart breaking seeing my little boy having to go through this, and have plenty of times sat there in tears & been comforted by the staff, every each one of the staff we’ve came into contact with, are an absolute credit to your Trust!.” (parent/carer of child aged 0-7)
“My sons care was priority and he was well taken care of. We were both very pleased with how it all went – especially the ipad video to help him understand what would happen – perfect for his ASD and understanding.” (parent/carer of child aged 8-11)
Acts of kindness
A few respondents highlighted small acts of kindness, not related to treatment, which were notable and for which they were grateful. This included where they perceived staff to have gone above and beyond what was expected. While this links to the ‘Personal attributes’ sub-theme, the examples here stand out as they were the sole focus of the comment and indicate that these acts defined the experience of care.
“The nurses were really nice, they sang happy birthday to me and also got me a card and present. I miss them. Thank you very much.” (CYP aged 8-11)
“The staff were really nice and knew I didn’t like bananas so they gave me some strawberry lip balm to take away the banana smell of the gas.” (CYP aged 8-11)
“The receptionist, I didn’t get he’s name but he made me feel very welcome and even printed activity pages for me to do while I waited.” (CYP aged 8-11)
“Staff very kind . I was given an Easter egg!” (CYP aged 12-15)
“The person who ran the play area…she was absolutely the best! I will be always greatfull for having had this lady on the day of the operation as she made it a great experience for my daughter and for us. She explained about how she was going to be put to sleep and she even got a gown for my daughters teddy.” (parent/carer of child aged 0-7)
Of note, a few parents/carers shared feedback about access to food and drink offered to them. A cup of tea might be considered a small gesture but clearly made a big difference to the experience for parents/carers.
“These little gestures of kindness from staff go a long way. Only at [location name] do we get offered hot drinks, hot tea and coffee; helps so much when you’re the only parent staying overnight.” (parent/carer of child aged 0-7)
“In the morning, we both got a drink along with some toast, which was the best!” (parent/carer of child aged 8-11)
“They offered both myself and partner food and drink throughout our time in A&E. A nurse also went out of her way to make me a decaf tea to help my health during pregnancy as the machines did not offer this.” (parent/carer of child aged 0-7)
Staff attitudes
Negative feedback on staff often focused on experiences where staff attitudes were reported as the source of anxiety and unhappiness. There are links between this feedback and insights shared later in this report on ‘Pain relief’ and ‘Communication’. Examples of staff being rude or patronising were typically shared by parents/carers, though it is notable that a few children and young people also shared similar comments.
“The nurse was not any help because I hate blood and it was every where I was tired and she just carried on saying “calm down, calm down” basically trying to shut me up in a way and now I am a lot more hesitant about needles.” (CYP aged 8-11)
“Doctors know better about us but they are very patronising, all of. And can be very fool of themselves. Lots of them lack empathy.” (CYP aged 12-15)
“The two doctors told me I shouldn’t be in pain and looked like they were laughing at me , it made me cry.” (CYP aged 12-15)
“NHS staff members are very rude,they are not doing their job in a professional manners.” (CYP aged 12-15)
“The consultant was very rude when speaking to my daughter who was in a lot a pain and distress before her operation and was given no pain relief before going to theatre some 7 hours after her arrival.” (parent/carer of child aged 0-7)
“I couldn’t believe how Doctor (name) spoke down on me and my husband, in front of his medical team. He disrespected us in the most unkind, rude and uncompassionate way. All we asked if it was possible to have an additional check carried out on our daughter… we were very concerned worried parents asking about checks he showed a disrespectful attitude. He even raised his voice at us saying… N0!!!!!!!!!!!!!!!!! It is my decision!!!” (parent/carer of child aged 8-11)
“The doctor who initially saw us in A&E seemed surprised that an 8 year old would be upset/distressed about being told she was about to have surgery and seemed to belittle her reaction when she was crying.” (parent/carer of child aged 8-11)
“They were very abrupt with him and almost rude to an extent which caused a rift with the care he received.” (parent/carer of child aged 12-15)
These negative experiences included respondents describing that they hadn’t been listened to, and several shared how they were left deeply upset by comments from staff.
“The main doctor was terrible. Spoke to us like we were making it up despite just being told I could have had something which could have killed me. Told us he’s the doctor he knows more than anyone and knows what he’s doing.” (CYP aged 8-11)
“Medical staff (primary Drs) often assume parents have little/no knowledge about medical procedures illnesses and didn’t take into account my professional as well as my understanding of my child on some occasions.” (parent/carer of child aged 0-7)
“As a parent we gave our views on what we though was up and felt we wasn’t listened to. We believe the staff could have done more in the period of time my daughter was left in a bed getting worse and worse for weeks,” (parent/carer of child aged 0-7)
“The surgeon was very unprofessional, vexatious and dismissive of me and my daughters wishes.” (parent/carer of child aged 8-11)
Training needs
There were examples which indicated how parents/carers and children and young people believed that further training was needed for staff. The examples below largely cover communication needs for neurodivergent patients, which links to accessibility discussed in ‘Hospital environment and facilities’ later in this report. In addition, other training needs highlighted can be found in the ‘Cannulation’, ‘Blood sampling’ and ‘Errors in treatment’ sub-themes later in the report.
“I’m autistic and although the staff did tell me what was happening it was all quite overwhelming and they wanted to rush through it rather than spending the time to talk with me slowly so that I could get a better understanding. I also suffer with panic attacks and with them rushing everything I ended up having a panic attack and then I wasn’t able to focus on everything they were saying to me, instead they just spoke to my parents so that they could move om quicker which made me really annoyed as I felt like I wasn’t being listened too properly. Overall the care I received was good but feel that staff could learn that people with autism or any other form of mental health need a bit more time to process information and will need a bit more help and Compassion in order to feel more safe and understood.” (CYP aged 12-15)
“My son’s pediatrician goes above and beyond for my son he is amazing. When visiting A&E the staff need more training on understanding autism and non verbal children.” (parent/carer of child aged 0-7)
“The nurse doing the scans and talking to us did not understand our SEN requirements, and made our child very anxious. The nurse made us feel like we were in the wrong for having bladder issues, as our child couldn’t do what she thought was normal due to her additional needs. I feel staff need to be fully aware of how Autism, ADHD, Dyspraxia, and Dyslexia can have affects on how we manage our health, and that what is considered normal, is not easy for everyone.” (CYP aged 8-11 – parent completion)
“Staff need more training around autism and autism in girls and masking.” (parent/carer of child aged 8-11)
“Some of the doctors could be a little more understanding/patient when my child doesn’t want to make eye contact or doesn’t feel comfortable with speaking a lot.” (parent/carer of child aged 12-15)
“Overall we have had an excellent experience but on a couple of occasions our consultant was busy and we ended up with registrars who knew very little or nothing about our history. One registrar in particular was quite poor when speaking to a child with autism and he got very confused about her approach and couldn’t respond.” (parent/carer of child aged 12-15)
Two parents mentioned Avoidant/Restrictive Food Intake Disorder (ARFID), highlighting the lack of understanding of the condition and need for further staff training.
“When visiting A&E the staff need more training on understanding autism and non verbal children. Also need education on ARFID (eating disorder).” (parent/carer of child aged 0-7)
“My child has ARFID. Avoidance restrictive food intake disorder. Nobody seemed to have heard of it at the hospital. I specifically told a member of staff not to force my child to eat. This wasn’t listened to and made my child become upset and anxious and then she was sick from the food being forced under her nose. This disorder needs to be recognised by medical staff and taken seriously.” (parent/carer of child aged 8-11).
Capacity
What does the quantitative survey data tell us?
- 67% of parents/carers of 0 to 15-year-olds said staff were ‘always’ available when their child needed attention (Qp43)
A few respondents, mainly parents/carers, commented on staffing levels as an area for improvement. Feedback demonstrated how when patients observed the capacity challenges the NHS workforce can face, this can lead to appreciation of positive experiences with staff. Examples were given where respondents felt delays or issues experienced by their child were driven by staff shortages or perceptions that the staff were overwhelmed.
“The staff were brilliant but the ward did seem very understaffed and the staff overworked.” (CYP aged 8-11)
“The staff are always really busy and still do a fantastic job. Sometimes waiting takes a bit longer when they’re short staffed.” (CYP aged 12-15)
“think the issue with delay around medication was likely due to not enough staff.” (parent/carer of child aged 0-7)
“Not enough staff on Day Unit – only 1 doctor who was also covering A&E.” (parent/carer of child aged 0-7)
“Staff were trying their best but the trust is clearly understaffed and these guys are being worked to the bone.” (parent/carer of child aged 8-11)
“Staff are helpful and do as much as possible. I never see them idle. They are very busy and any problems seem to come from not enough staff.” (parent/carer of child aged 12-15)
Theme: Waiting
What does the quantitative survey data tell us?
- 57% of parents/carers of 0 to 15-year-olds stated their child’s visit to hospital was an emergency, while 43% were a planned visit (Qp28)
- 82% of parents/carers of 0 to 15-year-olds said their child had to wait in a hospital waiting area. Most commonly, CYP waited in the accident and emergency department (41%), followed by on the ward (38%) and anywhere else in hospital (12%) (Qp29)
- 63% of parents/carers whose child had to wait in a waiting area in the hospital said their child was ‘always’ able to get help from staff if they needed it (Qp31)
Feedback on the experience of waiting was predominantly negative, with examples across a range of contexts. Experiences demonstrated the difficulties of waiting with a child or young person and the impact that waiting can have on both the patient and their family/carers. This is further evidenced by the noteworthy exceptions where parents/carers shared surprise at the speed patients were treated. Please note there is relevant insight shared within the theme ‘Hospital environment and facilities’ as to other factors which impacted on the experience of waiting.
Wait times
Waiting time was a prevalent theme in responses across all age groups, with largely negative feedback shared. In some cases, this was the only comment written by a respondent, though they did not always provide detail on how long they were waiting or where the waiting happened. Descriptions often stated the wait was ‘too long’ and the evidence suggests that what is considered a reasonable timeframe is subjective and variable across patients.
“Need to reduce the waiting time.” (CYP aged 8-11)
“I wait in the hospital for hours.” (CYP aged 8-11)
“I didn’t like the long wait time.” (CYP aged 8-11)
“Hospital waiting time is too long. I was in pain and crying and had to wait for treatment for 8 hours. It’s too long.” (CYP aged 12-15)
“Waiting times need to improve and more explanation of what’s going to happen next.” (parent/carer of child aged 0-7)
“The waiting time was too long other than that everything was ok.” (parent/carer of child aged 8-11)
“Waiting times always too long for children.” (parent/carer of child aged 8-11)
“Waiting time made me doubt whether my child would receive the help he needed.” (parent/carer of child aged 8-11)
Accident and emergency
Where feedback was clearer on context, waiting times in accident and emergency (A&E) were commonly highlighted as an area for improvement by both parents/carers and children and young people. Children and young people waiting for pain relief while in A&E was described as particularly difficult to experience and manage.
“I waited ages in a&e.” (CYP aged 8-11)
“I have waited with my mum in the waiting area for 9 hours in A&E until I was seen to,in extreme pain. My mum was constantly asking reception why it takes so long and why people who came after us have been seen to and not me. I was given pain relief only once in all those hours when I started screaming in pain and my mum was crying.” (CYP aged 8-11)
“Six hour wait in A&E is not acceptable.” (CYP aged 12-15)
“The wait at A&E was very long.” (CYP aged 12-15)
“I didn’t like being left in A&E for hours in pain on a uncomfortable chairs, even when the surgeons came down they where not happy to find me left on a chair, it took too long for surgeons to see me as well.” (CYP aged 12-15)
“Waiting time to see a Dr for our baby was approx 8 hours. It was 1am by the time we were triaged and in the children’s waiting area.” (parent/carer of child aged 0-7)
“The wait before being seen by a doctor in A and E was too long.” (parent/carer of child aged 12-15)
“My child had a compound fracture on his right arm. We waited in A&E for a few hours and weren’t given pain relief.” (parent/carer of child aged 12-15)
Availability of beds
Some respondents commented on long waits to move from A&E or other parts of the hospital onto a ward due to availability of beds. While further detail wasn’t always shared, there were indications that this consistently had a negative impact on experiences of care.
“When I was sent to (name) ward I was left in a wheelchair for ages, I wasn’t given a bed.” (CYP aged 8-11)
“Even after being visibly sick and with high temperature, i was sent back into the waiting room for another 3 hours as there were no beds available.” (CYP aged 8-11)
“The morning session ran over and so we were waiting in the waiting area a very long time waiting for the bed.” (CYP aged 12-15)
“A&E staff friendly had to wait 6 hours for a bed on the ward.” (parent/carer of child aged 8-11)
“My only small issue was we had to wait in recovery till a bed came available.” (parent/carer of child aged 8-11)
“After a long time waiting in a&e , we also waited in child ward waiting area because lack of bed. From at 8pm to 2 am we just waited for a bed for my son.” (parent/carer of child aged 12-15)
Reasonable adjustments
Hospital environments were described as overwhelming by some respondents, as waiting in unfamiliar surroundings could be challenging for children and young people. This echo’s feedback in sub-themes ‘Comfort’ and ‘A&E environment’ later in this report. There are indications that children who may be more vulnerable required support to minimise the negative impact of waiting.
“Waiting at the emergency department was so long and so loud and so bright that it added to my stress and made me feel worse.” (CYP aged 12-15)
“There wasn’t or at least didn’t seem to be any thought or consideration for my child’s additional needs. Autism/Non-verbal/Incontinence. The constant noise and disturbances made it very difficult to keep my child calm in such a busy environment.” (parent/carer of child aged 8-11)
“Our child is quite anxious and nervous, especially in new situations. We were asked to be on the ward by 7.15am for a planned operation. We didn’t go down to theatre until just before 1pm. Although the staff was lovely and popped in our room a couple of times to check on us, this was still a very long time for her to wait which increased her anxiety and stress levels.” (parent/carer of child aged 8-11)
“Prior to the MRI Scan we were told that the Play Specialist would bring information to my teenager to explain the process to them to held relieve their anxiety – this did not happen despite the wait being a few hours for the Scan.” (parent/carer of child aged 12-15)
Delays and cancellations
Respondents expressed frustration at delays to planned operations or procedures which resulted in long waits.
“When I had surgery on my toe, I was in the hospital for about 12 hours, taking me from 4:00 in the morning.” (CYP aged 8-11)
“We were asked to be on the ward by 7.15am for a planned operation. We didn’t go down to theatre until just before 1pm.” (parent/carer of child aged 8-11)
“The procedures were carried out youngest to oldest. The older children became anxious with waiting over two hours or more for their procedure.” (parent/carer of child aged 12-15)
“Waiting time for procedure arrived at 12.15 pm op was not until 4.15 pm.” (parent/carer of child aged 12-15)
Frustrations were further exacerbated by having to abstain from food or drink as a fast, particularly if the operation was then cancelled. This was highlighted as an issue by both children and young people and their parents/carers.
“I waited in the hospital all day and the doctor told me not to eat. I’ve been hungry all day. I waiting for my surgery. But the doctor gave my surgery time to someone else without any notice, unannounced kept me waiting all day. What a terrible service.” (CYP aged 8-11)
“On my first attendance for my operation I was starved all day and cancelled at 4pm. I found this very upsetting and was not made aware at anytime that I might be cancelled.” (CYP aged 12-15)
“Only issue was her operation was delayed so she was fasting from breakfast until after 5pm.” (parent/carer of child aged 0-7)
“My child was waiting for a space in theatre and was due in at 11am and ended up going down at 8pm. She was nil by mouth from 6.30am!” (parent/carer of child aged 0-7)
“He’d waited all day for an op. and was told the op wasn’t going ahead until the next day. An explanation was given and he understood why – due to emergencies – and it couldn’t be helped. Think he was weary from being nil-by-mouth.” (parent/carer of child aged 8-11)
“We were told we’d have to stay in hospital until Monday with my child nil by mouth in case an operation was agreed upon.” (parent/carer of child aged 8-11)
Scans, tests and results
Both patients and their parents/carers expressed discontent with what they perceived as long waits for tests, scans and/or results.
“Wait of 3 days for results from MRI when there was suspected sepsis.” (CYP aged 12-15)
“There was a long time waiting for a CT scan and the we doctor helped to chase up it was hours.” (CYP aged 12-15)
“My child has waited 4 hours for a blood test to be done while staff are just sat around.” (parent/carer of child aged 0-7)
“Staff need to be a little more pro active when it comes to tests. My son had blood tests and we had to wait 3 hours for results… This was because they were left in a box for collection by a porter so there was no urgency of getting them to the lab. Had I walked the bloods to the lab myself I would have been home a lot sooner.” (parent/carer of child aged 0-7)
Noteworthy exceptions
A few parents/carers gave positive feedback on the speed with which their child was seen, diagnosed and/or treated. There were indications in the comments that this was appreciated, particularly where expectations were exceeded.
“We never had to wait long before being seen. I’m glad that my teeth were made better.” (CYP aged 8-11)
“I am satisfied I got the right treatment and I got surgery quickly. Thanks.” (CYP aged 12-15)
“Generally we are pleased with the care he got. It was both through and quickly dealt with.” (parent/carer of child aged 0-7)
“Treatment was quick, which was great.” (parent/carer of child aged 8-11)
“Very quick at assessing my child and making a decision.” (parent/carer of child aged 8-11)
“Grateful for the quick response from a blood test in the morning to being diagnosed. And the amazing work throughout.” (child aged 12-15)
“Very prompt service. As soon as issue was known we got seen really quickly and moved to a quieter area.” (parent/carer of child aged 12-15)
Theme: Treatment
Feedback demonstrated that patients and their parents/carers who did not feel they had been listened to, had a lack of confidence in their treatment. The evidence suggests that even the more common aspects of treatment, such as medication and cannulation, can cause difficulties and distress to children and young people, defining the experience without compassionate handling by staff.
Pain relief
What does the quantitative survey data tell us?
68% of parents/carers of 0 to 15-year-olds said that staff ‘definitely’ did everything they could to help with their child’s pain (Qp61).
Lack of adequate pain relief was highlighted as an area for improvement across all ages of children and young people. Seeing children and young people in pain could clearly be distressing for parents/carers, and they expressed frustration when pain relief wasn’t offered. This links to the ‘Staff attitudes’ sub-theme explored earlier, where patients or parents/carers felt they weren’t listened to or their concerns were dismissed.
“When I was in A&E I was in so much pain when my arm had been crushed and the bone was sticking out but no one was getting me any medicine to help the pain.” (CYP aged 8-11)
“The reason I came to hospital is because I was in lot of pain, and I needed stronger painkillers I came Home with the same pain that I went in hospital with.” (CYP aged 12-15)
“I had to beg for paracetamol because my child was constantly crying and even the medicine took 30-40 minutes while my son was still crying alot.” (parent/carer of child aged 0-7)
“I felt powerless and very upset when my child was not given pain medication because they hadn’t been seen by the consultant.” (parent/carer of child aged 12-15)
“No pain relief when he was sent for his X-rays too. It was awful to watch him in so much pain and not one person who was caring for him offered him pain relief. We had to ask for it several times.” (parent/carer of child aged 12-15)
Missed or ‘late’ diagnosis
Both children and young people, and parents/carers, described situations where they were initially sent home, most commonly after an A&E visit, before an accurate diagnosis and corresponding treatment were received. Examples focussed on patients whose conditions worsened after visiting A&E, included multiple visits, as well as patients discharged after an inpatient stay. A common thread in these comments was parents or carers who advocated strongly for their child by continuing to ask for help or seeking additional clinical advice. There are notable links to the ‘Between staff and parents/carers’ communication sub-theme which demonstrates the importance of parents/carers feeling listened to.
“A&e could have been better, my mum and dad took my there 5 times before they realised I had meningitis and I was really poorly and scared but they kept sending ne away.” (CYP aged 8-11)
“My experience in children’s A&E was not positive as initially when I came to the hospital they did not perform an assessment that was in depth enough and sent me home.” [Later had surgery] (CYP aged 12-15)
“A&E was terrible. The staff didn’t think I was ill. Lots of people listened to my chest and said it was clear. My mum demanded an x-ray which showed I actually had pneumonia.” (CYP aged 8-11)
“The first day we went to A&E for his little finger, an x-ray was done, and he had a fracture. No cast was put on the finger … A member of staff just put plaster on the finger. A week later, we went to the hospital for another x-ray. It was worse than before, and he was booked for an operation. If there was cast, it would have prevented the bone from getting out of place.” (parent/carer of child aged 0-7)
“Once seen after very minimal tests, temperature, blood sugar level check we were told there was nothing wrong and sent home. A week later I took him to (location name) A&E where we told within a couple of hours that he was in heart failure and was sent straight into intensive care.” (parent/carer of child aged 0-7)
“Child discharged twice as having a viral stomach infection. Admitted to (location name) Children’s hospital the day after discharge to have life saving emergency surgery due to a missed bowel obstruction.” (parent/carer of child aged 0-7)
“Despite asking multiple times we were not given access to her blood reports – they kept referring us back to our GP who tried her best but herself didn’t have access to latest reports. It was only on my third A&E [location] visit and another painful and distressing blood test that the doctor ran a culture test and it came back positive for paratyphoid – a disease that can be fatal if left untreated. it’s a pity it took us reaching out to her ourselves to get our daughter the right treatment.” (parent/carer of child aged 0-7)
Cannulation
Cannulation was a specific area of concern for parents/carers, with a range of difficulties shared relating to the process.
“My daughter had a cannula for 3 days and when we removed the cannula she had a pressure sore on her hand.” (parent/carer of child aged 0-7)
“When a toddler (2 yrs) old is required to have a ‘Tv’ cannula fitted, after 2 failed attempts, why was the vein detector used on the 4th attempt by a doctor be – not before. Vein detectors should be used on all paediatric wards with all patients in my opinion.” (parent/carer of child aged 0-7)
“My only concern was that I was really shocked that the Trust routinely cannulate a child in their hand and then routinely PUSH IV antibiotics in such a small vein still?? I did a bit of reading and I understand there was a shortage of giving sets at a point in the past, but I had to really stand my ground and ask the nurses to stop pushing them into her vein on the third dose. She was screaming out in pain.” (parent/carer of child aged 8-11)
“The gel before making the cannula was applied too late by the nurse on the ward and did not work on time.” (child aged 12-15)
Blood sampling
Intravenous blood tests were raised by children and young people as an area to improve. Most comments related to the distress of having multiple blood tests or when there were problems finding a vein. Evident also in the sub-theme ‘cannulation’, feedback about blood sampling links back to insight detailed earlier in the report on ‘training needs’ for staff.
“Due to not drinking/ eating it was difficult for the doctors and consultant to find my veins. They tried at least 8x to gain entry when all they needed to do after the 3rd attend was use the ultrasound machine to locate it.” (CYP aged 8-11)
“I had to have my blood taken 7times.” (CYP aged 8-11)
“I had a blood test but the thing was but my nerves were very thin and I had to do it in 3 different places.” (CYP aged 8-11)
“Play therapists should be offered every time you need a blood test.” (CYP aged 8-11)
“I had to have a blood test and before this i was fine with needles but when it happened blood when all over my arm and all over the bed in the room. The nurse was not any help because I hate blood and it was every where I was tired and she just carried on saying “calm down, calm down” basically trying to shut me up in a way and now I am a lot more hesitant about needles.” (CYP aged 8-11)
“Staff not trained enough to do simple procedures. blood tests painful. Support worker took Cana out of arm wrong by pulling it upwards.. awful experience wouldn’t go back unless I was desperate.” (CYP aged 12-15)
Medication
Some respondents highlighted the need for different forms of medication when the patient was unable to take tablets orally. A few parents/carers, along with a young person themselves, described their concerns at being ignored when expressing this need and the resulting distress of being ‘forced’ to take medication in a particular form.
“One of Drs would listen when I said I couldn’t take tablets and came to give me big anti biotics I am unable to swallow tablets after an hour and half my mum managed to get me liquid the Dr said it won’t work as well but I can’t swallow tablets I didn’t feel listened to then.” (CYP aged 12-15)
“He will not take medicine orally and I said this many times however he will take it at home mixed in a yoghurt but would only eat this in a familiar surrounding. I was extremely distressed when we was made to try force antibiotics down his throat and this made him extremely heightened.” (parent/carer of child aged 0-7)
“Please can children be asked routinely if they want it in tablet or liquid form?” (parent/carer of child aged 8-11)
“(name) struggles with most treatments. She cannot take oral medication (except for Movicol and Gaviscon, which she has been on since infancy). Despite explaining this multiple times, we encountered significant resistance…(name) cannot tolerate oral medication. Even so, the doctors insisted on following their ‘process,’ repeatedly trying to administer oral medication and subjecting (name) to further trauma.” (parent/carer of child aged 8-11)
Errors in treatment
In a small number of cases parents/carers described what they experienced to be serious errors in aspects of the patient’s treatment that had significant consequences for the child/young person, such as infection. Note there is an example of an NHS Never Event shared below.
“A mistake happened in the A&E where my child was given an adult instead of a child dose of a medication to stop seizure which led to respiratory failure and required the resuscitation team to intervene.” (parent/carer of child aged 0-7)
“My daughter was discharged with a stitch still in place (which we had been told was dissolvable). I called the ward a week or so later saying it was looking infected and I suspected a stitch has been missed but was advised over the phone to go the GP for antibiotics and assured she only had dissolvable stitches in place. … Another week or 2 later and we ended back in A&E and there is was confirmed there was a stitch that needed removing and the stitch site needed cauterizing to aid the healing.” (parent/carer of child aged 8-11)
“The only concern was she was not provided with any antibiotics on discharge and that’s how she was readmitted for post surgery infection.” (parent/carer of child aged 8-11)
“My child ended up with an infection due to a swab or similar being left inside the incision site.” (parent/carer of child aged 12-15)
Theme: Communication
Feedback on communication ties closely to the ‘staff’ and ‘treatment’ earlier in this report, with comments demonstrating the importance of involving patients alongside parents/carers. Elements highlighted as valuable and which created good communication for both parents/carers, and children and young people, included:
- clear information about diagnosis, treatment or care
- giving timely updates
- explaining what was going to happen
- making information understandable
- talking openly with both parents/carers and CYP
- having time to ask questions
Between staff and CYP
What does the quantitative survey data tell us?
- 74% of parents/carers of 0 to 7-year-olds said staff ‘always’ communicated with their child in a way they could understand (Qp37).
- Among CYP aged 8 to 15, 73% said staff ‘always’ talked to them in a way they understood (Qc13).
- Among parents/carers of 0 to 7-year-olds, 59% said staff ‘always’ took the time to listen to their child’s fears or worries (Qp47).
- Among CYP aged 8 to 15, 71% said staff ‘always’ took the time to listen to their fears or worries (Qc17).
- 72% of 8 to 15-year-olds said staff ‘always’ listened to what they had to say (Qc15).
- 79% of 8 to 11-year-olds said they were involved in decisions about their care and treatment (Qc9i).
- 87% of 12 to 15-year-olds said they were involved in decisions about their care and treatment as much as they wanted to be (Qc9ii).
Comments from children and young people themselves made clear how much they valued being included in conversations about their treatment and care. They described how staff taking the time to speak and listen to them helped them to feel less anxious.
“talked me through everything that was happening and made sure I was ok throughout my stay.” (CYP aged 8-11)
“The staff were really good and told me what was happening very well they were also very kind I don’t think there is anything that could be improved.” (CYP aged 8-11)
“I felt safe in the hospital, but better to get back out again! The nurses were very kind and tried to be cheerful. They were honest though about what was happening.” (CYP aged 8-11)
“The best appointments are when the doctors talk to me and explain things for me.” (CYP aged 12-15)
“Everything was very good and as a patient I was handled with care and was always in the loop knowing what was going to happen going forward.” (CYP aged 12-15)
“I was happy with everything and was not as frightened as I thought I would be, because the staff looked after me and explained things to me.” (CYP aged 12-15)
“The surgeon who saw me and operated on me was very good and explained what was going to happen to me very well. He didn’t rush me or talk over me. I was really scared but he made me feel much better.” (CYP aged 12-15)
“I was very nervous about being in hospital, but they made me feel very comfortable and took the time to listen to any worries I had, and did as much as they could to help.” (CYP aged 12-15)
“I was treated very well all the staff was friendly and they explained everything to me in a way that I understood and they made my stay very comfortable.” (CYP aged 12-15)
“They were very friendly and spoke to me in a language I understood and when explaining what I was going through, if I didn’t understand or if I had questions they explained everything.” (CYP aged 12-15)
Parents and carers observed the positive impact when staff provided reassurance to their child by talking to them and involved the patient in what was happening with their care.
“Everything was explained and all staff involved came to meet my son. Walking to the theatre the staff were brilliant and put my son at ease.” (parent/carer of child aged 0-7)
“I felt the team (lady) who delt with explaining the procedure to my daughter did a fantastic job and picked up on my child’s needs and communicated this information to the theatre staff and myself so I could be more involved with her in this time of stress to help it go smoothly for all involved.” (parent/carer of child aged 0-7)
“My child’s appointment with their paediatric consultant was excellent. She was kind, interacting with our child, caring, clear on the care plan, explaining complex details without medical jargon and compassionate.” (parent/carer of child aged 0-7)
“The play therapist in children’s A & E was absolutely wonderful, really making my child feel at ease & explaining everything in a way that my child understood before cannula insertion which was his first experience ever.” (parent/carer of child aged 8-11)
“The member of staff who did the EEG put my daughter at ease straight away by chatting to her and explaining everything.” (parent/carer of child aged 12-15)
Between staff and parents/carers
What does the quantitative survey data tell us?
- 81% of parents/carers of 0 to 15-year-olds said staff ‘definitely’ gave them information about their child’s care and treatment in a way they could understand (Qp38).
- 92% of parents/carers said they were involved in decisions about their child’s care and treatment as much as they wanted to be (Qp49).
Staff taking care to communicate well was important to parents/carers, with a common thread through feedback being parents/carers who felt listened to. This reflects insights shared earlier in sub-themes on ‘medication’ and ‘missed or late diagnosis’.
“My daughters symptoms were treated and she was prescribed antibiotics but no one administered it because we moved from the emergency room up to waiting on the ward, I highlighted this several times and no one gave it to her.” (parent/carer of child aged 0-7)
“The care my son received was exceptional. The staff were kind and really listened to my concerns. They did everything they could to help him get the tests needed quickly. My only concern was A&E, where there was a long wait and my child was sent home initially despite having a life threatening infection. I brought him back in when I started to have doubts and then he was admitted.” (parent/carer of child aged 8-11)
There was feedback shared as to how valued it was to have someone to ask questions of and discuss any concerns.
“We felt well looked after we was explained about the whole process my daughter was going to be having done and there was always staff to talk to or ask questions this was undoubtedly the best service we could of received and the best experience we could of hoped for.” (parent/carer of child aged 0-7)
“At all times we were informed about what was going to happen and asked if we had any questions.” (parent/carer of child aged 12-15)
Another indicator of good communication for parents/carers was staff ensuring they understood and felt reassured about what came next for the patient.
“It was quite a scary situation but myself and my son but the staff took time to explain everything to me. They were amazing!” (parent/carer of child aged 0-7)
“The registrar and consultant who cared for my child were exceptional. They kept me informed and were open and honest with me about my daughter’s Illness/treatment.” (parent/carer of child aged 0-7)
“Overall, his care was good. The communication was good, in the operating room before my son was put under, the entire team engaged with us. They were very child-friendly and provided me, as a mom, with comfort and supportive words.” (parent/carer of child aged 8-11)
“The child’s diabetic team in hospital were amazing and invaluable. In a very distressing time they were there to help us understand and learn.” (parent/carer of child aged 12-15)
Reflecting the earlier feedback on involving children and young people, parents/carers emphasised that involving both them and their child in conversations about treatment and care in a way that they could all understand was a positive experience. One parent welcomed their non-verbal child being included.
“Even though my daughter is non verbal staff still explained everything to us both so it felt like she was still included in her care.” (parent/carer of child aged 0-7)
“At all times the staff informed us what was happening & any concerns they had. The staff spoke to us & my son, everything was explained & any concerns answered.” (parent/carer of child aged 12-15)
“The way they explained things to both of us made the experience much less frightening. The doctors were thorough and took the time to answer all of my questions, ensuring that I understood everything about my child’s treatment.” (parent/carer of child aged 12-15)
“Everything that was going to happen to him was explained to us both in a way that we could understand.” (parent/carer of child aged 12-15)
Continuity of care
What does the quantitative data tell us?
- 32% of parents/carers said staff gave them conflicting information ‘a lot’ or ‘a little’ (Qp42.
Feedback demonstrated that communication was a fundamental part of care continuity. There were indications picked up by parents/carers through communication, that there lacked continuity of care, such as being asked repetitive questions and staff not holding the same information about the patient as others. A range of factors were observed in the feedback as to signs of issues with continuity visible through the lens of communication, and/or reasons it was believed to have occurred:
- lack of handover
- staff not reading patient notes
- departments not communicating with each other
- staff not communicating with each other
- repetitive questions
- no point of contact with overarching view
- conflicting information
A range of more negative examples were shared of communication issues relating to continuity of care. The impact included delays to treatment, parents having to repeat information, and tests having to be re-done.
“I think the doctors can be a bit more joined up as it felt there was not much communication. People doing there thing but not looking at the overall picture.” (CYP aged 12-15)
“We were in hospital for 5 days. Every day a new doctor would come round and every day I had to repeat my son’s history, stressing that this was an issue he has had for a long time, have to say what sort of tests he had. It was like day to day there was no handover.” (parent/carer of child aged 0-7)
“Communication between all major members of staff could have been better. We was told our son had to fast from 9pm to the next morning until he had the 1st wee of the day. This was quite distressing with a 2 year old. 1st attempt they didn’t even test it for Diabetes Insipidus which is what he was in for and the second time a trainee nurse threw it away without getting tested so he ended up having had one tested that wasn’t fasted so we wasted a full week and we didn’t get accurate results.” (parent/carer of child aged 0-7)
“We spent several hours sitting in the hallway with a sick child because we were sent back to the emergency room, even though we had a referral to paediatrics.” (parent/carer of child aged 0-7)
“11 doctors seem my daughter pocked prodded and asked the same questions over and over. None of the doctors seemed to read any of the notes from the previous doctors.” (parent/carer of child aged 12-15)
“Our experience was very poor in A&E – getting my daughter taken seriously and too a ward also took time – she was left for hours and hours – the situation was awful I could not even find a doctor or staff member to help we were just left in a corner in A&E. when she was eventually admitted and passed to surgical team things were a bit better but there were still delays and cock ups with tests / she did a urine sample in A&E – we were told it was lost and another was required – she could not stand at this point as the pain was so bad – she managed to do another one then they found the first test!” (parent/carer of child aged 12-15)
Feedback indicated how a lack of continuity due to communication issues was experienced as distressing for the patient and their parent/carer. It was of particular concern when there was disagreement between professionals or where conflicting information had been received. It was suggested that having greater continuity of staff involved would help to improve the situation.
“The consultants seemed to vary on what they thought the issue was and so from shift to shift they took different approaches and gave different information depending on their viewpoint. This was not at all reassuring and meant that we kept having to explain things over and over again.” (CYP aged 8-11)
“The Doctor removed my neck brace to examine me before I had the results of my MRI scan. Even though the doctors the previous day said it should not be removed until they have seen the MRI results.” (CYP aged 12-15)
“There was no communication between the Drs and consultants and we were constantly given conflicted information as to treatment and diagnosis which was incredibly frustrating and stressful. The lack of continuity between Drs and consultants was also very stressful.” (parent/carer of child aged 0-7)
“I had very conflicting advice about my daughters Condition whilst at [Location]. We went in not knowing what was wrong with her. The A&E doctor seemed very concerned and told us that we would need to be admitted daughter would need bloods and an EEG. When we got to the ward we were forgotten about entirely and then were discharged the next morning without any tests being done.” (parent/carer of child aged 0-7)
“High Infection markers showed on child’s blood tests and no beds on ward. Dr said as no beds we could go home at 5 am in the morning and said she was confident infection markers were high due to viral infection therefore did not require any antibiotics. However, the next morning I got a call of a different dr in paediatrics A&E and they asked me to take my child back to reassess him due to his infection markers.” (parent/carer of child aged 0-7)
“1st paediatric we saw was fantastic and he made it sound like our process would be done within a few days yet a week later and 4 doctors we was told to go on our way with no answers.” (parent/carer of child aged 0-7)
A related area for improvement was shared through questions relating to the accuracy of patient records and suggestions were made for greater transparency of notes for parents/carers to feel more informed.
“It will be great [location] hospital have up to date records of patient, even though I’m being treated in [location] hospital, this help to speed up the activities for remediation.” (CYP aged 8-11)
“I didn’t like the way my discharged summary was done, it wasn’t detailed enough for me.” (CYP aged 8-11)
“It was very difficult to get access to my child’s notes when I requested them.” (parent/carer of child aged 0-7)
“I’d love a transparent patient record that we could look at together so I can look up eg previous drugs or advice that worked.” (parent/carer of child aged 8-11)
“My son had a reaction to something after surgery I am concerned this wasn’t documented on his discharge notes or medical records.” (parent/carer of child aged 8-11)
Theme: Hospital food
Food was frequently raised by children and young people, indicating it played a significant role in their experience of care in hospital. Feedback was largely negative, with the comments indicating areas for improvement to include choice and quality, meeting dietary requirements, and provision of food for parents.
Choice and quality
What does the quantitative survey data tell us?
- 49% of parents/carers of 0 to 11-year-olds said there was ‘always’ enough choice of hospital food for their child (Qp54)
- 43% of young people aged 12 to 15 years said there was ‘always’ enough choice of hospital food (Qc5)
- 40% of parents/carers of 0 to 11-year-olds said there was ‘always’ hospital food available for their child outside of mealtimes (Qp55)
- 43% of young people aged 12 to 15 years said they were ‘always’ able to get hospital food when it wasn’t a mealtime (Qc6)
There were comments, mainly from children and young people, expressing dissatisfaction with the food available during their stay in hospital. Both choice and quality were often commented upon together. In some cases, options were highlighted as inappropriate due to age. The examples demonstrated how subjective the concept of age suitability for food was across respondents.
“The food was disgusting and it felt like the people who made it didn’t put much effort into what they were cooking.” (CYP aged 8-11)
“I didn’t like the food in hospital, there was I of curry and grown up food, and then after 10 days they finally offered me food I like such as jacket potato or chips or beans.” (CYP aged 8-11)
“I think they should have a spicy Caribbean menu because that’s what I mostly eat at home.” (CYP aged 12-15)
“The quality of food could be a bit better, it would be nice to have more choices but better quality of the current menu would be good.” (CYP aged 12-15)
“The hospital food needs to be way better that stuff made me even more sick. Basically starved myself mate.” (CYP aged 12-15)
“It was a bit difficult to eat after my surgery and therefore some of the stodgy foods were harder to eat. It would be nice if there were some light snacks that were easy to eat such as cucumber and fruits etc.” (CYP aged 12-15)
“The food options I was given were very limited, I got a ham sandwich but it was very dry and tasteless.” (CYP aged 12-15)
“Hospital food was poor – no proper meal choices for child – assumption my child would only eat pizza + fish fingers/chicken nuggets. No snack options available for in between meals.” (parent/carer of child aged 0-7)
“I then asked for food for him and they said they could get him a jacket potato, yes you read that correctly, an 11 month old baby a jacket potato.” (parent/carer of child aged 0-7)
Dietary requirements
Limited food options were highlighted by respondents where there were dietary requirements, such as patients with intolerances/allergies, who were vegan, and those observing religious diets. Examples indicated information on food suitability for specific dietary needs, including allergens, wasn’t always provided, made accessible or easily understood.
“Lack of knowledge by nursing staff about gluten-free menu options. As I recall, there were limited options, but the staff weren’t aware of what, if anything, was available. It would be helpful if they knew what dietary options are available.” (CYP aged 12-15)
“There could have been more vegan options for food although the jackfruit curry I did have was good.” (CYP aged 12-15)
“There was no real options for vegan and I just ended up with plain jacket potato.” (CYP aged 12-15)
“Also more food options for Muslims as when I was there I was only allowed to eat jacket potatoes.” (CYP aged 12-15)
“My son who is 9 months, with allergies to egg, peanuts, tree nuts and soy, was offered dinner but the staff member was only ‘pretty sure’ the fish fingers didn’t have egg. She also wasn’t certain about if the food was safe from the other allergens.” (parent/carer of child aged 0-7)
“All children were offered food after surgery; my daughter was offered a cheese sandwich even though she is unable to eat dairy. Better care of dietary requirements would be good.” (parent/carer of child aged 0-7)
“I think there should be a better food option for children with “beige diets”. My son could only eat quavers as the hot food he would not eat due to his autism he diet is extremely restricted.” (parent/carer of child aged 0-7)
Bringing food from home
Feedback included examples where parents/carers brought food into hospital for their child/young person. While not always clear, some indicated this was due to perceptions of hospital food being poor quality or there being a lack of options that met patient dietary requirements.
“The quality of provided on the children’s ward was extremely poor. Ended up locking our own meals.” (parent/carer of child aged 12-15)
“The food was dry and not very good so my parents bought me food in.” (child aged 12-15)
“I am vegan and there were only limited options for me and these then repeated themselves a lot throughout my stay. My parents had to bring in food for me.” (child aged 8-11)
“I am allergic to cows milk and soya. The hospital had no food at all that did not contain either of these and even though I told them this when I was checking in, no one seemed to get it or be prepared. I was offered cheese crisps, a cookie and even a white ham sandwich but the nurse didn’t know if they contained my allergens and asked my mam to check. I was not allowed to leave without eating but luckily my mam had brought food I could eat.” (child aged 12-15)
Provision for parents/carers
What does the quantitative survey data tell us?
- 27% of parents/carers said they had ‘very good’ access to food in hospital (Qp57)
- 35% of parents/carers said they had ‘very good’ access to hot drinks (Qp58)
The main feedback relating to food from parents/carers was the lack of access for them when they were with the patient. Shops and cafes were not always open or had limited offerings, and leaving the child/young person to get food was not always possible.
“Would be good to after food to parents as some cannot leave ward to get food.” (parent/carer of child aged 0-7)
“There were not enough food I as parent was hungry all the night as in dinner time the staff for food just give me one peace of chicken wings.” (parent/carer of child aged 0-7)
“Food for parents was limited. The [name removed] was mainly sandwiches and the canteen was closed on the weekend. Hard to go out for food when have a very young child in the hospital.” (parent/carer of child aged 0-7)
“Sometimes parents arrive in an emergency and don’t have food with them. Staff try their best with spare sandwiches but this is not always available and it isn’t practical to leave children and go out to shops away from the hospital.” (parent/carer of child aged 8-11)
Some children and young people also mentioned that there was no food available for their parents/carers in their feedback, highlighting the impact that this can have on the overall experience for the patient. Note that some examples also mention access to drinks for parents/carers being a concern also.
“Being able to have some food as the cafe was shut and Mum couldn’t get much from the vending machine.” (CYP aged 8-11)
“Food should be provided for the parent who stays with the child too.” (CYP aged 12-15)
“My mum wasn’t offered any food even though she stayed in hospital with me for 4 days.” (CYP aged 12-15)
“Access to any sort of vending machine or near by food/drink kiosk would have been good as the only one we were made aware of was some distance away and would have meant my Mam leaving me or us both going to get something which we felt we couldn’t do as we might miss our time to be seen by the doctor. Once we had stayed overnight, we were offered food then but my Mam hadn’t eaten before she took me in and so went without anything for most of the day before.” (CYP aged 12-15)
Three parents/carers of children aged 0 to 7 commented on the provisions made for breastfeeding mothers. Feedback spanned breastfeeding mothers not being given any provision; and mothers not exclusively breastfeeding, observing that they were not provided for and treated differently and unfairly as such.
“When staff saw me breastfeeding, I was fed 3 meals a day and very well looked after with nourishment in that sense. It felt nice when we were obviously going through a tough time…When a formula bottle was seen, all meals were immediately ceased without any conversation. Luckily I have a wonderful family that bought me food and kept me well nourished and hydrated.” (parent/carer of child aged 0-7)
“I was told that breastfeeding mothers are offered a meal (which I don’t agree with, I think all parents should be offered food) however I was not offered any food or drinks.” (parent/carer of child aged 0-7)
“I think it would have also been good if we could have been directed to or provided hot drinks and food. Particularly for me who was breastfeeding and very recently postnatal following a caesarean section.” (parent/carer of child aged 0-7).
Noteworthy exceptions
A very small number of positive comments were shared about hospital food.
“I liked the food.” (CYP aged 8-11)
“Staff are very supportive attentive and provided special halal level 4 pureed out of meal of hours.” (CYP aged 12-15)
“He cited the fact he was provided with extra ice cream and jelly after operation, and that there was little kitchen nearby to make toast while we wait to be discharged.” (parent/carer of child aged 0-7)
Theme: Hospital environment and facilities
Feedback on the hospital environment and facilities was predominantly negative, with lots of improvement suggestions made to meet both the children or young person’s needs and that of their parents/carers. There are interconnections between the sub-themes shared in this section, along with linking to the themes of ‘Hospital food’ and ‘Things to do in hospital’. For example, a lack of accessible or age-appropriate facilities can contribute to feelings of being unsafe within the hospital environment.
Comfort
What does the quantitative survey data tell us?
- 66% of CYP aged 8 to 15 years who stayed overnight were stopped from sleeping by at least one factor. The most common factors were: noise from other people (42%), noise from medical equipment (31%) and hospital lighting (16%) (Qc3)
Children and young people reported that they struggled to get comfortable in the ward or room they had used. Sensory issues were described, with the brightness, temperature and noise being problematic for some, along with bedding or even beds being uncomfortable. While not always stated explicitly this appeared to impact on patients’ ability to sleep.
“The pull out beds were extremely uncomfortable and some broke and it was cold In the room at night.” (CYP aged 8-11)
“I had to lay upside down on my bed to get to sleep, but when I was in my own room it was okay because I could turn all the lights off.” (CYP aged 12-15)
“The bedding didn’t feel comfortable but I really liked the lights and padding in the sensory room.” (CYP aged 12-15)
“It was cold at night.” (CYP aged 12-15)
“The temperature of the room I was staying in was either too cold or too hot.” (CYP aged 12-15)
Privacy
What does the quantitative survey data tell us?
- 83% of parents/carers of 0 to 7-year-olds said their child was ‘always’ given enough privacy when receiving care and treatment (Qp48)
- 83% of CYP aged 8 to 15 years said they were ‘always’ given enough privacy when receiving care and treatment (Qc10)
Lack of privacy was only mentioned by children and young people, particularly ages 12 to 15. The language used demonstrates an issue that was keenly felt and could lead to embarrassment. Lack of privacy could be due to a lack of private spaces or perceived insensitivity of staff.
“I think I could have been in a treatment room when ward was full to have things done.” (CYP aged 8-11)
“I was asked lots of embarrassing questions and everyone in the ward could hear.” (CYP aged 12-15)
“As a female teenager I think that there should be teenager wards or private wards for girls during their menstruation as this is very private and can be embarrassing if leaks happen.” (CYP aged 12-15)
“The only thing I hated was the cleaner lady just comes and opens your curtains and leaves them open. I was in a lot of pain and wasn’t wearing any knickers because I had a catheter and when my mom came back from the loo anyone passing could see my bare bottom cause the cleaner didn’t care I was embarrassed about that.” (CYP aged 12-15)
Age-appropriate
What does the quantitative survey data tell us?
- 72% of parents/carers of 0 to 7-year-olds said the ward was ‘very’ suitable for their child’s age (Qp33)
- 64% of children aged 8 to 11 said the ward was ‘very’ suitable for someone of their age (Qc4)
- 50% of young people aged 12 to 15 said the ward was ‘very’ suitable for someone of their age (Qc4)
Related to sub-themes on ‘Comfort’ and ‘Privacy’ was feedback on whether hospital provision was age appropriate. Both children aged 8 to 11 and parents/carers of 0 to 11-year-olds commented on the difficulties they experienced when accommodated alongside older children. Parents/carers highlighted how young children could be disturbed by noise and exposed to inappropriate language.
“The ward was amazing for older children – my son was two so in between being too little for the children’s ward and too big for the baby ward.” (parent/carer of child aged 0-7)
“My only criticism was being put into a ward with a 12 year old. My son was 17 months old at the time and in a cot and we were not even given our own room like we was on the normal paediatrics wards… 12 year old and her family were playing loud music until gone 10pm, not really age appropriate for our 17 month old.” (parent/carer of child aged 0-7)
“A negative was that we were on a ward with a <1yr old and a suicidal adolescent which wasn’t appropriate. The language, noise and drama caused by this individual ruined a calm, safe environment for children.” (parent/carer of child aged 0-7)
“(Name) Ward was extremely noisy and the staff were so busy. We were put in a shared room with a teenage boy, not that appropriate as his language wasn’t good and he stayed up later than us.” (parent/carer of child aged 8-11)
Young people aged 12 to 15 and their parents/carers, commented negatively when accommodated alongside much younger children or when on adult wards. This was due to feelings of discomfort or the feeling that it wasn’t ‘right’ to mix with a different age group.
“I’m 15 and was put in a ward with 2-5 year old which was slightly strange.” (CYP aged 12-15)
“I don’t think sixteen years old should be in the adults area until they are lease seventeen or eighteen years old.” (CYP aged 12-15)
“I had to go to the adults women only ward which wasn’t suitable for me, i was also placed on my own away from others because my dad was with me.” (CYP aged 12-15)
“As a teenager, my son wasn’t too impressed with initially being on the day ward with very young children.” (parent/carer of child aged 12-15)
“As an almost 16 year old my son felt uncomfortable sitting in the children’s area. It would be great to have a more age appropriate area for teens.” (parent/carer of child aged 12-15)
Children and young people aged 8 to 15 and their parents/carers particularly highlighted the disruption of being accommodated alongside babies or very young children, whose crying would often keep them awake.
“I am 10 and I was in a room with 2 and 3 year olds They cry alot in the night and I wasn’t able to sleep.” (CYP aged 8-11)
“There was a small child who as soon as he woke up made a lot of noise and cried, after which he was hospitalized in the same room as a boy older than me and I felt a bit uncomfortable.” (CYP aged 8-11)
“I struggle with noise and there were a lot of crying babies and children.” (CYP aged 12-15)
“It would have been nice if he had been with just older children as very young child kept them up all night crying.” (parent/carer of child aged 12-15)
A&E environment
Parents/carers of all ages and children and young people aged 8 to 15 shared negative experiences of A&E environments. Primarily this covered the lack of comfortable or appropriate seating for patients or their parent/carer, particularly where they had extended periods waiting which links to the sub-theme of ‘Wait time’ detailed earlier in the report. Feedback also included a lack of cleanliness, noisy and overcrowded spaces, and a lack of things for children to do.
“I am disabled and can’t sit in my wheel chair for a long time. So waiting to be attended to unless I come in by Ambulance is really difficult for me.” (CYP aged 8-11)
“Please kindly think of getting better seating in the children’s A&E waiting area, thank you.” (CYP aged 12-15)
“We were placed in a tiny waiting room that was being used as a storage facility.” (CYP aged 12-15)
“I do think that cots should be available for babies in children’s A&E we were waiting for reviews and OBS for several hours and could have done with somewhere other than a car seat to put her.” (parent/carer of child aged 0-7)
“The waiting room in children’s A&E at the (location name) is appalling. It is always completely overcrowded, it’s too small, there is no adequate ventilation and there are barely any toys or activities for children. It is always full with children who are very poorly and have no space, some families have to sit on the floor.” (parent/carer of child aged 0-7)
“Children’s A&E waiting area was very dirty with blood on the floor for some time. (parent/carer of child aged 8-11)
“A far far less important part of our feedback is that after 3 nights without sleep, the plastic seats in A and E next to our daughter were extremely uncomfortable and we couldn’t even doze off!” (parent/carer of child aged 12-15)
Accessibility
Some feedback gave examples of hospital facilities that were not considered suitable for the patient’s needs. This included disabled children who did not have beds or washing facilities that were accessible. Some comments indicated that experiences such as this, left the patient feeling unsafe.
“When in hospital I did not have an appropriate hospital bed, for my needs. I felt unsafe and could not settle in the bed I was given. I felt very overwhelmed.” (CYP aged 8-11)
“I am a 10 years old, with lots of health problems. I am also a wheelchair user and the ward is not suitable for me, the rooms are very small so my carer can’t use the mobile hoist in the room. As it is not enough space to use it safely. Also there is not a bath or shower suitable for me. So when I’m in hospital. I can’t have a clean and sometimes I’m staying for more than a week.” (CYP aged 8-11)
“My child’s disability is absolutely not catered for in hospital. We have to bring cushions and blankets from home to try and make the beds safe and comfortable for him. I have to transfer him to the toilet every time he needs it, throughout every hospital stay, as staff can’t or won’t.” (parent/carer of child aged 12-15)
A noteworthy exception came from a parent/carer who described how having a side-room allowed them to better support their child’s needs.
“It was very helpful that he was put in to a side room to help keep him calm and I was allowed to keep another adult with me to be able to help with my son’s needs. When he becomes overwhelmed he can become aggressive and start to scream, so being moved made it so much easier for treatment.” (parent/carer of child aged 8-11)
Provision for parents/carers
What does the quantitative survey data tell us?
- 64% of parents/carers of 0 to 15-year-olds who stayed overnight rated the facilities for parents/carers as ‘very good’ or ‘good’ (Qp60).
In the same way that parents/carers commented on a lack of food and drink provision for themselves, some responses highlighted how impactful better facilities for parents/carers would be. There were calls for specific spaces for adults who are facing extended stays with their child/young person and examples also shared of insufficient storage for clothes in current facilities.
“Private area for parents to have a shower, comfier facilities for them also.” (parent/carer of child aged 0-7)
“Could do with somewhere for parents to have a shower / change as I had to have a baby wipe wash in the tiny loo.” (parent/carer of child aged 0-7)
“Poor provisions in parents room, no basics such as cutlery and plates and fridge is small.” (parent/carer of child aged 0-7)
“There should be a kitchen for parents to access to be able to make a hot drink maybe sandwiches for parents. After a whole night in A&E – you need this as a parent.” (parent/carer of child aged 8-11)
“The toilet availability is a bit poor for such a large ward and there was no parents kitchen.” (parent/carer of child aged 8-11)
“Please improve the parents rooms. There are lots of cupboards with people’s clothing instead of cups and cutlery for parents to use. And it could use some cleaning as well the microwaves and the fridge.” (parent/carer of child aged 12-15)
One noteworthy exception further demonstrated the positive impact kitchen facilities can have for parents/carers.
“The family room was brilliant though for cups of tea and fridge space.” (parent/carer of child aged 0-7)
Equipment availability
A few parents/carers highlighted a lack or scarcity of equipment that they would have expected in a hospital. This ranged from basic medical supplies to wheelchairs.
“It was shocking to see the staff had no basic equipment like thermometers and tongue depressors.” (parent/carer of child aged 12-15)
“My daughter has had to be examined by a doctor in the corridor because no cubicles were free, they have used wooden spoons to check the back of her throat because there was no other equipment.” (parent/carer of child aged 0-7)
“The IV was inadequately stocked so she had to leave and go to adult day and to get some more piece of equipment so she could insert the IV cannula.” (parent/carer of child aged 8-11)
“My child struggled to walk from the children’s ward the length of the hospital to the car park. This was die to the nature of his operation. I had bags to carry and I feel we needed help I.e a wheelchair.” (parent/carer of child aged 12-15)
Children aged 8 to 11 also highlighted where medical equipment or patient clothing were not available in appropriate sizes for them.
“They should have children’s grippy socks, I had to use adult ones and they kept falling off my feet and made it hard to walk.” (CYP aged 8-11)
“There was no children’s neck brace so used a small adults, which was not the right size for me.” (CYP aged 8-11)
“I wish there were more sizes of gowns because I had a too big gown as the small size was too small for me.” (CYP aged 8-11)
A few parents or carers of 0 to 7-year-olds asked for cots to be made available, as they had struggled to look after very young children without one and had safety concerns regarding the risk of falling off the bed.
“I do think that cots should be available for babies in children’s A&E we were waiting for reviews and OBS for several hours and could have done with somewhere other than a car seat to put her.” (parent/carer of child aged 0-7)
“There were no cots available and I was asked to co-sleep with my 11 month old in a bed – this was ok in this instance but not ideal, and did not feel very safe.” (parent/carer of child aged 0-7)
“Because my child was so poorly and little I had to permanently stay with her. She was also not in a cot but on a bed which she preferred. Staff seemed annoyed when I asked if they could watch her (on breathing machine) so she didn’t fall off the bed if I needed the toilet/ drink.” (parent/carer of child aged 0-7)
Parking
Difficulties finding a parking space and parking charges were raised by parents/carers and some children and young people. Parking passes were requested or highlighted as helpful and extended to family members broadly.
“Car parking is an issue in hospital.” (CYP aged 8-11)
“Mummy says parking was a nightmare.” (CYP aged 8-11)
“We were given a parking permit which really helped us.” (CYP aged 12-15)
“Parking pass for extended family such as grandparents would have been useful especially when they have come to help with childcare.” (parent/carer of child aged 0-7)
“Parking! Very very deceptive. It lets you leave without paying whereas in other hospitals it checks gone registration with whether you’ve paid or not. Cost me dear!” (parent/carer of child aged 12-15)
“Parking charges could be waived off for patient in care.” (parent/carer of child aged 12-15)
“Parking was very difficult. Took almost an hour to find a parking space, luckily we are a 2 parent family so I could take my daughter in whilst my husband parked. It would have been a nightmare if I was on my own.” (parent/carer of child aged 8-11)
Theme: Things to do in hospital
There were both positive and negative comments about things to do, with feedback emphasising how important it was to have activities while spending time in hospital.
Play
What does the quantitative survey data tell us?
- 53% of parents/carers of 0 to 7-year-olds said staff played or did activities with their child ‘as much as my child wanted’ (Qp46)
- 53% of CYP aged 8 to 15 said staff played or did activities with them while they were in hospital ‘as much as I wanted’ (Qc7)
Parents/carers of 0 to 7-year-olds commented on how beneficial access to playrooms and toys were, both for the patient and for their wider family such as siblings, as these facilities could ease an anxious time for all involved.
“My daughter enjoyed using the playroom and the outside space when she felt better and actually said she’d like to go back.” (parent/carer of child aged 0-7)
“There were a range of toys and play areas my child could access. All of these things made a worrying time a little easier.” (parent/carer of child aged 0-7)
“The playroom, play kitchen and interactive lights etc were great for my toddler. These areas are really special!” (parent/carer of child aged 0-7)
“The children’s ward was great and there was plenty of toys, puzzles and activities for her to do whilst waiting and post-op.” (parent/carer of child aged 0-7)
“The play room was a great bonus when in with our baby. The staff had her on portable oxygen so we could visit and when her older brother came to see her he was equally occupied!” (parent/carer of child aged 0-7)
“The playroom was an amazing addition plus the thoughtfulness of the charities to deliver food.” (parent/carer of child aged 0-7)
Children aged 8 to 11 particularly relished having access to games consoles.
“Was lucky enough to have an Xbox.” (CYP aged 8-11)
“The doctors and nurses were kind and helpful and the play team brought an xbox which was amazing.” (CYP aged 8-11)
“The staff let me use a gaming gadget to help pass time while I stayed for a couple of days in hospital.” (CYP aged 8-11)
“The entertainment was really good, I got to play Crash Bandicoot on the PlayStation!” (CYP aged 8-11)
Negative comments generally related to a lack of entertainment, descriptions of books and toys being in poor condition, and broken equipment such as televisions. This feedback predominantly came from parents/carers, providing further evidence of the positive impact having things to do can have on the experience for the whole family.
“The PlayStation could be be working that would have made my room better.” (CYP aged 8-11)
“I know toys can be a hygiene risk but maybe something to play with or a tv she could have watched would have been helpful.” (parent/carer of child aged 0-7)
“It was incredibly difficult to keep a walking 1.5 year old occupied when there were little activities on the ward and it was a stressful experience overall.” (parent/carer of child aged 0-7)
“The toys and books in the department all looked sad/ shabby and maybe not the cleanest.” (parent/carer of child aged 0-7)
“Some toys and books were quite battered and old but I wouldn’t know how to donate to a hospital children’s ward. Might be worth some way of advertising that donating to a hospital can be an alternative to donating toys and books to charity shops or binning them.” (parent/carer of child aged 0-7)
“Most of the TV’s are broken on the assessment unit and the ward which again makes things difficult for young children.” (parent/carer of child aged 0-7)
“I felt the wards play room was not big enough. Toys tired.” (parent/carer of child aged 8-11)
Children and young people aged 8 to 15 flagged toys and entertainment not being age appropriate as an area for improvement.
“More things to do (there were things for little children, but not older children) e.g. television, books puzzles, comics, tablets to take their mind off what is going on.” (CYP aged 8-11)
“The toys on the children’s ward were quite babyish, all I could do was colouring.” (CYP aged 8-11)
“It would be nice if there were some books to read or magazines for teenagers. There were only toys for young children.” (CYP aged 12-15)
“The waiting room in children’s emergency had an adult programme showing all night that was very triggering.” (CYP aged 12-15)
“Would be nice if they could get things for older children to do while in hospital I like sensory toys an lot of time could fine any think like that.” (CYP aged 12-15)
Wi-Fi
What does the quantitative survey data tell us?
- 43% of CYP aged 8 to 15 who used the hospital Wi-Fi said it was ‘always’ good enough to do what they wanted (Qc1)
Predominantly young people aged 12 to 15 mentioned access to Wi-Fi as an area to improve. Examples spanned poor signal, intermittent connectivity, and Wi-Fi not working. This was a source of frustration for young people, with indications that it had a negative impact on their overall experience.
“WiFi isn’t working every time we visit.” (CYP aged 8-11)
“Wi-Fi was hit and miss.” (CYP aged 12-15)
“Better WiFi.” (CYP aged 12-15)
“Better WiFi would have made things a lot easier.” (CYP aged 12-15)
“Also the internet kept cutting out, then when I was on the ward I had no internet at all.” (CYP aged 12-15)
“Wifi in children’s hospital is poor – kids depend on it especially during long stays. We eventually had t buy our own wifi box to get better signal in his room.” (parent/carer of child aged 12-15)
Theme: Discharge and aftercare
Feedback relating to discharge through to aftercare indicated areas for improvement to ensure patients and their parents/carers are clear on what would happen next. Clarity on next steps links this theme to ‘Treatment’ and ‘Communication’ outlined earlier in this report.
What does the quantitative survey data tell us?
- 66% of parents/carers of 0 to 15-year-olds said they ‘definitely’ knew what was going to happen next with their child’s care and treatment when they left hospital (Qp69)
- 90% of parents/carers of 0 to 7-year-olds said staff told them who to contact if they were worried about their child when they got home (Qp68)
- 53% of CYP aged 8 to 15 said staff told them who to talk to if they were worried about anything when they got home (Qc25)
Discharge
Several children and young people, along with a few parents/carers, shared negative experiences of discharge. For some, they described a long wait before discharge, while for others discharge came as a surprise with patients sharing they felt it was too soon for them to leave. Other examples included those who felt they had insufficient information on next steps following discharge.
“I was quite sick when I was sent home and didn’t feel quite ready to go home.” (CYP aged 8-11)
“when we were discharged we were not given clear answers of what should follow.” (CYP aged 8-11)
“It took a very long time to be discharged and wait for someone to tell us what had happened in the operation. They told my mum eventually how it went at midnight after a 2pm operation.” (CYP aged 8-11)
“Better discharge. We were thrown out at 11pm and had bo idea what the after care was! I ended up having to go back in.” (CYP aged 8-11)
“I didn’t feel well enough to be leaving hospital at 10pm when I was told I was staying over night . Felt very much like the ward wanted me out.” (CYP aged 12-15)
“I was waiting quite a while to be discharged and was ready for home.” (CYP aged 12-15)
“Was told she could go home in 1 hour, 2.5 hours later I had to chase someone up asking when she would be discharged and then finally someone sorted it out and we got out 3 hours later than they originally said we would.” (CYP aged 8-11- parent completion)
“We were unexpectedly told he could go home. Within 30 minutes we were expected to leave, without any assistance, pain relief or discharge info; it was appalling and very distressing for both my son and I. We were literally abandoned.” (parent/carer of child aged 12-15)
“when we were able to be discharged a doctor gave notes to someone else then it was left on the top no one dealt with it until after the doctor was back from lunch and half an hour after that seen we were still there.” (parent/carer of child aged 12-15)
Young people aged 12-15 also demonstrated a lack of confidence in the pain medication they had been given to take home after their hospital discharge.
“I would also like to have received stronger pain medication when I went home as I only received paracetamol, ibuprofen and another medication to prevent infections. All of these medications did nothing to help my pain and I was in a lot of pain.” (CYP aged 12-15)
“Don’t send me home without painkillers.” (CYP aged 12-15)
“I was given a very low dose of pain relief on my prescription when I left the hospital compared to what I had been given in the hospital.” (CYP aged 12-15)
Aftercare
Often discussed alongside feedback regarding discharge were negative comments relating to aftercare. While more prevalent among the parent/carer feedback, there were mentions among children and young people too. Experiences shared included a lack of, or incorrect, information about how to care for the patient after they left hospital.
“We weren’t given any information on discharge about how to care for my daughter at home with a plaster cast on – we had to ask about showering/washing, what position to keep her arm in etc.” (parent/carer of child aged 8-11)
“When sent home we had no paperwork on how to care for the huge brain surgery scar. I emailed a lot and had so many questions. A leaflet or email would have been very useful i.e. when we could wash hair, how long to wear a headband, how tight etc.” (parent/carer of child aged 8-11)
Some respondents focussed on follow-up appointments, with several examples shared where planned follow-ups did not happen in the expected timeframe, if at all. This included comments that indicated the parent/carer and patient were not clear on who was responsible for their care post hospital stay, and an example of feeling driven to private healthcare when support was not provided.
“After discharge, my mum has had to complain to get me reviewed. I’m not well and should have been reviewed after 3 months. It’s now 6 months and still haven’t been seen. I feel that nobody cares. My GP won’t see me because I’m under the consultant and the consultant says she’s too busy to see me.” (CYP aged 12-15)
“We still haven’t received an outpatient follow up appointment despite 6-8 weeks being the time frame stated in the discharge notes when we left hospital and it is now 5 months later.” (parent/carer of child aged 0-7)
“We weren’t sent a follow up appointment following the surgery and had to chase this few months later or this wouldn’t have been done.” (parent/carer of child aged 0-7)
“I met with an allegen consultant in the hospital for potential allergies, asthma. Once we were discharged that was it. Nothing more. No more conversations about the matter. I have had to go private to get this on going support.” (parent/carer of child aged 0-7)
“He was told he would have a 6 wk follow up appointment which he has not received.” (parent/carer of child aged 0-7)
“The information I was given for after his discharge was incorrect. I had to contact the consultant’s secretary to find the correct information about getting his pins removed post operation. (parent/carer of child aged 12-15)
Other observations
Below is a list of other topics commented upon in the data that were noted during the analysis process. There was a lack of volume of comments or depth and detail to inform themes and sub-themes but suggestions are noteworthy:
- dissatisfaction with young person signing consent form under Gillick Competencies
- mothers feeling ignored or dismissed when fathers were present
- descriptions of hospital décor as ‘dark’, ‘boring’ or in need of some ‘colour’
- children and young people unhappy to be on a mixed gender ward
- satisfaction that education materials or ‘schooling’ was provided
- patient not being offered food or unable to access food
4. Conclusions
This is the first national qualitative analysis delivered for the Children and Young People’s Patient Experience Survey, and the breadth and depth of the insights demonstrates the value of inviting respondents to share their experiences in their own words. This approach has enabled patients’ and their parents and carers voices to shape the focus of the findings, highlighting what is important to them and what impacts their experience of hospital care.
Overall, the report shows that children and young people tend to focus reflection on their experience in hospital on the interactions with staff along with hospital food, environment and things to do including play and Wi-Fi. The findings demonstrate that while there is appreciation and gratitude for care, there are significant challenges in delivery that can undermine experiences and confidence in care.
Reflecting on what constitutes high-quality children and young people’s hospital care, the analysis demonstrates the prerequisite that basic needs are met as common threads point to patients and their parents and carers experiencing difficulties relating to food, sleep and feelings of safety. Further, the analysis points to a gold standard for experience: involvement of both patients and their parents and carers were the foundation, with trust and confidence in care being created by staff who listen and communicate effectively with all parties involved. It is also pivotal that patients feel they are in an age-appropriate environment to feel calm and secure. The importance of staff listening appears across the themes, with indications that improvements in continuity of care and engaging with both patients and their parents and carers would significantly build trust in treatment and care.
The diversity of patients, their expectations and needs identified in this analysis demonstrate a challenging context. The findings demonstrate a level of complexity, for example the variation of needs across age cohorts run across multiple sub-themes and indicates that improvements in waiting, food, things to do and environment are required. Sitting alongside is consideration of the needs of children and young people who are more vulnerable, with signs that addressing their concerns around waiting, treatment and communication would be of benefit to all service users.
This report offers a comprehensive view of improvement opportunities but has limitations in determining which matter most. Where identified, sub-themes which only appeared in feedback from a specific age cohort are noted but the absence of mentions should not be seen as evidence that issues do not exist in other age groups. Triangulation with other datasets and targeted engagement activities are recommended to identify high-impact priorities both locally and nationally.
5. Appendix: Methodology
Survey methodology
In 2024, participants of the Children and Young People’s Patient Experience Survey were offered the choice of responding online or via a paper-based questionnaire.
The Children and Young People’s Survey asked children and young people and their parents and carers about their experiences of hospital care provided by NHS acute trusts. Trusts sampled patients aged 15 days to 15 years at the time of discharge and had received care in hospital during March, April and May 2024. The survey received feedback from 25,821 people – a response rate of 20%.
Qualitative analysis
Thematic analysis was undertaken to achieve a deep understanding of the findings from the open questions asked in the survey. This sought to facilitate reflection and learning across services delivering hospital care for children and young people in England.
To analyse qualitative data, the standard six steps of thematic analysis were used to identify patterns of meaning within the data and explore commonality and contrast – see Figure 1.
Figure 1: Thematic analysis approach
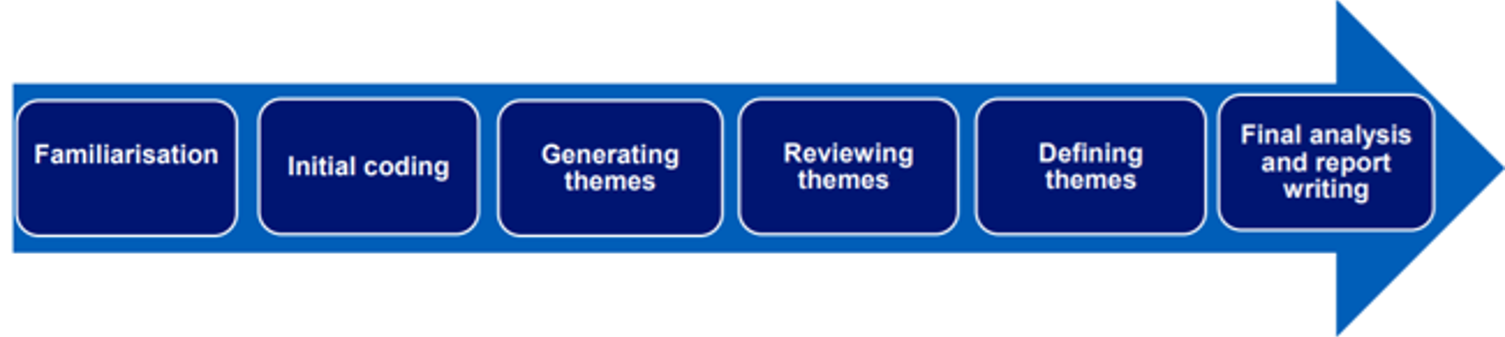
An inductive approach was undertaken for the data analysis of responses by both parent/carers and children and young people, which is a systematic method where themes emerge from the data without any pre-existing framework being used.
The results of the thematic analysis have been reviewed and are shared in context of the relevant quantitative survey findings. This exploits the value of both the quantitative results, which tells us the proportion of respondents feeling a certain way, and the qualitative findings, which tells us why people feel that way. For example, where there is a high degree of agreement / positive experience evidenced in the survey data, the thematic findings offer an opportunity to understand why there was not 100% agreement / positive experience and therein, where the opportunities lie for reflection and learning.
Sub-group comparisons
Sub-group comparisons were not the focus of the analysis. A small number of findings were specific to the age of the patients e.g. some issues were raised by children aged 8 to 11, which were not mentioned by the older age group. Where this was the case, it is stated in the findings. It is recommended that further focused sampling would allow for in-depth exploration of how experiences of care may vary for different groups. Observations included will unlikely be exhaustive due to the national sample and focus.
6. Appendix: Sampling approach
11,465 written responses were collected from parents/carers and 5,758 from children and young people aged 8 to 15, meaning 52% of participants who completed the survey provided qualitative data in answering the open-ended question.
Qualitative data cleaning
Before sampling, further data cleaning was carried out to identify and remove extremely short comments which were of no analytical value, for example those which simply stated ‘No’, ‘N/A’ or consisted of a single character.
For parents and carers, 362 comments were removed in this way, leaving 11,103 comments for the sample to be drawn from. For children and young people aged 8 to 15, 232 comments were removed in this way, leaving 5,526 comments for the sample to be drawn from. Table 1 below outlines the number of comments by survey version for parent/carers and for child/young person survey sections.
Table 1: Number of comments by survey section and in qualitative sample
| Survey version | Survey section | No. of comments overall | No. comments in sample |
|---|---|---|---|
| 0 to 7 (parent/carer only) | Parent/carer | 6,213 | 332 |
| 8 to 11 | CYP survey | 2,961 | 329 |
| Parent/carer | 2,640 | 145 | |
| 12 to 15 | CYP survey | 2,797 | 302 |
| Parent/carer | 2,612 | 153 |
Sampling
It was decided to sample parents/carers and CYP separately so that all respondents with a viable response to an open question had the potential to be included in the final sample for analysis.
To ensure a robust approach to sampling, a purposive sampling approach was taken. This is an established best practice technique when analysing qualitative data, as it ensures that the data has enough diversity across the most relevant criteria to allow the impact of the criteria to be explored and compared. For example, if age is a criteria, including responses from all the different age groups in sufficient volume means that differences in experiences between age groups can be explored.
The criteria chosen to sample on were the age, ethnicity, gender and deprivation level, as these were key demographic groups recorded in the data for the child who had received care in hospital. A sample matrix was drawn up to establish how many comments from each of the demographic groups were to be included in the analysis to allow for sufficient coverage.
In addition to the key demographic groups a minimum of 30 comments were included on all other characteristics including Arab or other ethnic group for instance. Please note that as there was a low volume of data from respondents identifying as ‘other’ gender identity, all of these cohorts were included in the sample. The breakdown of the volume of comments in the sample by these different criteria is provided below.
Once the original sample had been analysed it was seen that data saturation had been reached, i.e. no new themes were emerging from the data. Had this not been achieved, additional comments would have been added to the sample as necessary, in line with best practice in qualitative analysis.
Table 2: Number of parent/carer comments in the analysed sample, by CYP characteristic
| Characteristic | Sub-group | Number of comments analysed | % of comments analysed | % of comments overall |
|---|---|---|---|---|
| Age (based on survey version) | 0 to 7 | 332 | 52.7% | 54.5% |
| 8 to 11 | 145 | 23.0% | 22.8% | |
| 12 to 15 | 153 | 24.3% | 22.7% | |
| Ethnic background | White | 449 | 71.3% | 74.9% |
| Mixed | 42 | 6.7% | 6.6% | |
| Asian | 59 | 9.4% | 9.6% | |
| Black | 30 | 4.8% | 4.4% | |
| Other | 30 | 4.8% | 1.2% | |
| Not given | 20 | 3.2% | 3.3% | |
| Deprivation level (IMD Quintile) | 1 (most deprived) | 96 | 15.2% | 15.9% |
| 2 | 121 | 19.2% | 18.6% | |
| 3 | 124 | 19.7% | 20.5% | |
| 4 | 129 | 20.5% | 21.5% | |
| 5 (least deprived) | 154 | 24.4% | 22.9% | |
| Blanks | 6 | 1.0% | 0.6% | |
| Gender / sex | Female/Girl | 273 | 43.3% | 44.1% |
| Male/Boy | 332 | 52.7% | 55.0% | |
| Other | 19 | 3.0% | 0.2% | |
| Prefer not to say | 6 | 1.0% | 0.7% |
Table 3: Number of CYP comments in the analysed sample, by CYP characteristic
| Characteristic | Sub-group | Number of comments analysed | % of comments analysed | % of comments overall |
|---|---|---|---|---|
| Age (based on survey version) | 8 to 11 | 329 | 52.1% | 51.5% |
| 12 to 15 | 302 | 47.9% | 48.5% | |
| Ethnic background | White | 432 | 68.5% | 71.4% |
| Mixed | 42 | 6.7% | 6.8% | |
| Asian | 66 | 10.5% | 10.3% | |
| Black | 35 | 5.5% | 5.7% | |
| Other | 30 | 4.8% | 1.4% | |
| Not given | 26 | 4.1% | 4.3% | |
| Deprivation level (IMD Quintile) | 1 (most deprived) | 111 | 17.6% | 17.5% |
| 2 | 127 | 20.1% | 19.1% | |
| 3 | 127 | 20.1% | 20.6% | |
| 4 | 116 | 18.4% | 19.1% | |
| 5 (least deprived) | 146 | 23.1% | 23.0% | |
| Blanks | 4 | 0.6% | 0.7% | |
| Gender / sex | Female/Girl | 284 | 45.0% | 46.8% |
| Male/Boy | 317 | 50.2% | 52.2% | |
| Other | 16 | 2.5% | 0.3% | |
| Prefer not to say | 14 | 2.2% | 0.7% |