We've put some small files called cookies on your device to make our site work.
We'd also like to use analytics cookies. These send information about how our site is used to a service called Google Analytics. We use this information to improve our site.
Let us know if this is OK. We'll use a cookie to save your choice. You can read more about our cookies before you choose.
Community Mental Health Survey 2024: National qualitative report
1. Introduction and methodology
The NHS Patient Survey Programme is delivered by the Care Quality Commission (CQC) on behalf of NHS England and the Department of Health and Social Care. The Survey Coordination Centre at Picker, coordinates the NHS Patient Survey Programme on behalf of the CQC. There are five surveys within the Programme: Adult Inpatient, Maternity, Children and Young People, Community Mental Health and Urgent and Emergency Care Surveys.
This report has been produced by Solutions Strategy Research Facilitation Ltd (Solutions Research) and NHS England to share national insights from qualitative thematic analysis of written responses provided by respondents that took part in the NHS Patient Survey Programme. The aim of this endeavour is to identify opportunities for learning and improvement through an in-depth understanding of experiences of care.
The focus of this report is on the Community Mental Health Survey 2024, which captured feedback from 14,619 patients aged 16 and over who received treatment for a mental health condition between 1 April and 31 May 2024.
Further information on the survey is available on the CQC website.
Qualitative data analysis
Three open questions were included in the survey which allowed respondents to use their own words to respond. The questions were positioned at the end of the survey and included the instructions as follows: ‘If there is anything else you would like to tell us about your experiences of mental health care in the last 12 months, please do so here.’
Respondents were then invited to write into a box about their experience, with the following questions posed:
QA: ‘Was there anything particularly good about your care?’
QB: ‘Was there anything that could be improved?’
QC: ‘Any other comments?’
To ensure a robust approach a purposive sampling method was used for thematic qualitative analysis:
QA: 658 comments were analysed as a sample from 7,537 viable comments.
QB: 641 comments were analysed as a sample from 6,510 viable comments.
QC: 644 comments were analysed as a sample from 4,186 viable comments.
Once the total sample of 1,943 comments had been analysed it was seen that data saturation had been reached i.e. no new themes were emerging from the data. Had this not been achieved, additional comments would have been added to the sample as necessary, in line with best practice in qualitative analysis. Further detail can be found in Appendix 5: Methodology and Appendix 6: Sampling Approach.
Use of illustrative quotes
Throughout the report, quotes are included to illustrate respondents’ experiences in their own words and substantiate the findings. Please note that the data is not edited in the interests of correct spelling and punctuation for example, to stay as true to the words of respondents as possible.
Certain information from the qualitative comments used in the report has been redacted to protect the identity of survey respondents and any other individuals referenced. Information that has been removed includes:
names of patients or staff replaced with “[name]”
names of wards, units or hospitals replaced with “[location]”
names of specific services replaced with “[service name]” or “[mental health service]”
names of county replaced with “[county]”
Where acronyms were used in comments, the full wording has been provided in the Appendix 7: Glossary.
There is a degree of duplication in the use of quotes in this report to substantiate insights. This reflects that written feedback is often complex in that it is rich in detail and spans several parts of patients’ care journey, providing a depth of insight as to several themes and/or sub-themes.
Use of quantitative data
Where possible in the findings section, themes are presented in context of the most relevant quantitative survey data. This allows for insights to be considered more holistically and to provide a greater opportunity for reflection and learning.
Context to support interpretation
Content warning: This report includes references to experiences of mental health, including mentions of suicide, which some readers may find distressing.
Further information about safeguarding procedures during data collection is available via patient.survey@cqc.org.uk.
Some responses in the analysis were very brief and lacked detail, which limited the insights that could be drawn. For example, answers such as “everything” or “nothing” suggested strong sentiment about what was good, while comments like “too much to list” indicated strong feelings about what could be improved. Although these responses were useful in showing the intensity of feeling, they did not provide enough detail to identify good practice or areas for improvement. For this reason, they were not included as insights in the main report but are presented here as contextual information.
A small number of respondents focussed on details of their mental health as opposed to the care that they received. It is unclear from the comments why this was the case, and helpful to note that this detail was out of scope for analysis. A further small number of comments could not be analysed due to the meaning being unclear.
In a few cases it was clear from the responses that the questionnaire had been completed by a partner or relative on behalf of the person who had received care.
There is evidence that some respondents were describing experiences of care beyond the NHS Community Mental Health services focussed upon in the survey. While some respondents stated they had been inpatients in mental health settings, the specific types of care, treatment or settings were not always specified. Similarly, some respondents were not always commenting on the recent experience they were asked about in the survey. Some patients would share their full story, which could include multiple interactions with mental health services and/or wider NHS access over periods of time not explicitly stated though inferred to stretch beyond the scope of the survey.
Comments reveal varied reasons for accessing mental health services, for example there is feedback from patients experiencing dementia, PTSD, ADHD and conditions requiring antipsychotics. Significant diversity in prior experience was also observed. These factors shaped how patients responded to their care, creating a challenging environment for delivery. Themes are closely interwoven and often interlink, and this report highlights these connections throughout. For instance, feeling confident in the care being received was influenced by multiple factors spanning the themes of ‘Access’, ‘Staff,’ ‘Treatment’ and ‘Communication.’
2. Headline findings
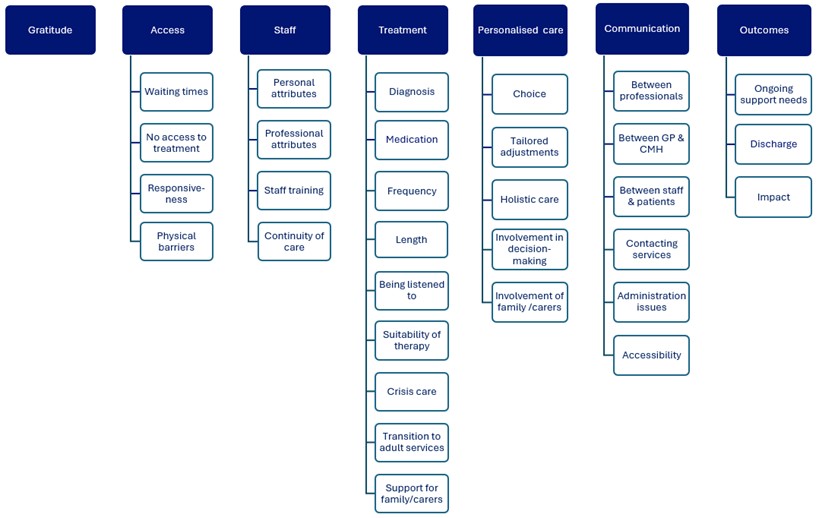
Thematic analysis of the qualitative data revealed the following key themes:
This image is a visual diagram showing seven themes related to patient experiences in mental health services. Each theme appears as a dark blue header with a column of light blue boxes beneath it listing specific subtopics.
Gratitude – no subtopics listed.
Access – includes waiting times, lack of access to treatment, responsiveness, and physical barriers.
Staff – includes personal attributes, professional attributes, staff training, and continuity of care.
Treatment – includes diagnosis, medication, treatment frequency and length, being listened to, suitability of therapy, crisis care, transition to adult services, and support for family or carers.
Personalised care – includes choice, tailored adjustments, holistic care, involvement in decision‑making, and involvement of family or carers.
Communication – includes communication between professionals, between GPs and community mental health teams, between staff and patients, contacting services, administration issues, and accessibility.
Outcomes – includes ongoing support needs, discharge, and impact.
The layout is a horizontal row of themes, each with vertically stacked subtopics, presenting a structured overview of key feedback areas.
3. Thematic analysis findings
Key themes
Seven key themes were identified from the thematic analysis, listed below. Within each key theme are several sub-themes which support interpretation and use of the insights. There are 31 sub-themes in total.
Gratitude
Access
Staff
Treatment
Personalised care
Communication
Outcomes
This section of the report contains the detail of each theme with a range of quotations shared to substantiate and exemplify the experience of respondents using their own words.
Theme: Gratitude
What does the quantitative survey data tell us?
Of all respondents who answered this question, 33% rated their overall experience a 9 or 10 where a score of 0 represented a ‘very poor experience’ and a 10 a ‘very good experience’ (Q39).
Of respondents who left a viable comment, 33% rated their overall experience a 9 or 10 (Q39).
Many comments made across the three questions were expressions of gratitude for the care patients had received. While there was a substantive volume of gratitude the feedback largely lacked detail or specifics about what created a good experience, with patients simply saying they were happy or that everything was ‘good’.
“I am very pleased with my care and am grateful for it.”
“Myself and my family have been so impressed and will be forever grateful for helping me get back to who I am!”
“Were do I start I can honestly say without their support I wouldn’t be here they saved my life. Thank you so much.”
“I want to say personally Thanks NHS for providing such a nice strong mental health support team.”
“I have always been happy with your good care. Thank you.”
“Always been excellent, cannot fault the care my husband has been given.”
“I’ve always received good care from my MH team.”
“Great service.”
“Nine out of ten.”
“We couldn’t have asked for more support. Our experience of mental health services has been superb in all areas.”
Theme: Access
What does the quantitative survey data tell us?
33% reported waiting 3 months or more between their assessment with the NHS mental health team and their first appointment for treatment (Q3).
84% felt their mental health either got worse or remained the same while waiting (Q5).
While there was a range of feedback about accessing community mental health services, from experiences of waiting through to physical access, the sentiment was predominantly negative with a focus on what could be improved about their experience. There were opportunities identified for improvement from very first contact through to treatment.
Waiting times
Experience of waiting times being lengthy for assessment and/or treatment stood out as the most prevalent theme in responses to the question asked about improvements. Please note, there are additional insights about waiting detailed within sub-themes later in this report regarding ‘Crisis care’ and ‘Contacting services.’
Where patients described the impact of waiting for support this often included a significant worsening of their mental health. Patients also described how deteriorating mental health had negative impacts on other aspects of their lives. Some made the point that earlier intervention would have led, in their view, to better outcomes.
“Quicker access to counselling on NHS. I am still waiting.”
“Time, it’s taken far too long and has had a detrimental effect on my longer term health.”
“The waiting times for both peer support and DBT are extremely long and I felt these two particular things strongly need and felt very unsupported.”
“I’ve had to save up to go privately because during the wait time I deteriorated rapidly.”
“Everything is taking so long and every week that goes by my mum deteriorates mentally.”
“I have been trying to access psychology/counselling services for 18 months, and have only very recently got on a waiting list. The situation I have been needing to resolve has had a great impact on my thinking/life, and as it has involved suicidal thoughts.”
“I was left to fester for 2 years until I had a breakdown and my symptoms became severe enough to treat.”
“The waiting time from when the referral was sent from the GP to adult ADHD team was around 18 months. I had already gone to the doctor at crisis point. During the waiting time, my life fell completely apart and resulting in self medicating with illegal substances, losing my partner and my children. The basics of life became unmanagable, I nearly died a few times.”
Some patients suggested that having clearer information about waiting times for treatment and where they were on the waiting list would be improvements that help manage expectations and reduce the anxiety attached to not knowing how soon treatment would begin.
“Only thing I will say is it should be made clearly before going for an assessment, how long the expected wait would then be before starting theory, if offered. I went for an assessment, then was told it would be 6 – 9 months before theory would take place. This actually had a very negative effect on my mental heath, and made zero sense to me.”
“However, I am an adult on the waiting list to be assessed for autism and it’s a very long wait. I have been waiting over a year and a half (and I know it will still be longer) but I have had no communication in regards to how much longer I need to wait and it is something that I am struggling with. I don’t know how long my wait is and it causes a great deal of stress often.”
Patients rarely mentioned being offered and/or accessing support while waiting which could indicate that it was not commonplace. Amongst those who referenced interim support there was mixed feedback as to how beneficial it was while waiting.
“The wait times are not okay! And there is not enough support offered during the waiting times.”
“The timescale of waiting to receive is 18 months; I have been fortunate to receive interim and low level intervention, which is a bonus.”
“Waiting for treatment calls are an absolute joke, it’s not helpful, it’s just a kick in the teeth every month and time spent doing those calls could be time spent on actually therapizing people.”
In contrast to comments about long waits, there were noteworthy exceptions sharing positive feedback about how quickly patients had been seen. While some cases related to emergency care, in other feedback it was not always clear whether being seen quickly related to treatment or an assessment.
“Getting seen really quickly.”
“I was given medical psychotherapy by a junior doctor and did not have to wait long at all.”
“When absolutely crisis situation, I got help quite fast.”
“The speed from initial referral by my GP to my first appointment with the mental health team was remarkable.”
No access to treatment
Some patients commented that they had been unable to access any treatment or a particular type of treatment that had been recommended. Feedback did not always clearly state why treatment was not received. When this was shared, some patients understood they had been refused care because they were already receiving support from another team.
“I had referrals rejected 4 times due to being under the eating disorder service in [Location] and the mental health team said I could only access one service, despite the eating disorder service making the referrals because the ED service said they couldn’t meet my needs for my PTSD, ASD, GAD and depression.”
“I was denied therapy for my anxiety because I am seeing someone from the ADHD team but these are not connected and it should not have impacted care for other conditions.”
In other cases, patients shared they had been told there was nothing the mental health service could offer them. The subsequent impact was that patients could be left feeling dismissed and this reduced the likelihood of them asking for help in the future.
“The team in [location] I was initially seen by after my suicide attempt told me they couldn’t help me. They sent me away with no resources. I felt helpless and not worthy of help, it was really unpleasant experience and made me not want to keep fighting for help.”
“I was referred to [service] by a member of the care team at [service]. They thought that Talking therapy my be of help. I had a very full assessment by F2F and completed questionnaire. The result was a very polite “I don’t think we can offer anything for you”, so a waste of time for me and the [service] staff.”
In other comments patients suggested the lack of access they experienced could be linked either to long waiting times or capacity issues.
“Access to appropriate services. (1) Whilst under the care of the Crisis Team, they recommended inpatient admission. Unfortunately no beds were available – this continued for some time. Eventually they discharged me to the community team. I never received the inpatient care that was needed. Care provided during this period (by the Crisis Team) was not adequate / equivalent to the care that I really needed at the time.”
“When [name] and I were out of our depth (I am retired and was having suicidal thoughts), she sought consultant psychiatrist advice and an appointment has never been delivered. Fortunately, I am now improved but if I had taken my life, I wonder how HM Coroner would have viewed appalling lack of provision.”
“Being able to access CMHT in the first place and not having to go private would have helped.”
Responsiveness
A theme with mixed sentiment was the responsiveness of services – that is, the extent to which care and support was provided when needed and adjusted to the changing needs of individuals. Positive comments focused on there always being a source of help available if needed.
“I always get quick response from my team.”
“My nursing associate is very on the ball and responsive to my needs.”
“The responsiveness and quick to be seen by crisis team was amazing.”
“Never felt abandoned by the team, always a number to ring.”
“I also have regular visits by CPNs who always ask if I need more frequent visits and advise if I need help to phone immediately.”
Lack of responsiveness when trying to access services due to changing symptoms or circumstances was a clear theme in feedback on areas to improve. The difficulty contacting a clinician, particularly those who could handle prescriptions, was also mentioned by several patients. There is related insight shared later in the report within the sub-theme ‘Contacting services.’
“Better access to psychiatrist when needed – not random annual check up.”
“I spoke to someone who was meant to call me a week later. They cancelled the appointment and never called again. That was 5 weeks ago, my condition has not changed but no support, it’s disgusting and unacceptable.”
“Trying to contact a psychiatrist for an appointment – as he is the only person who can prescribe / alter medication.”
“Please have more staff who understand people with the illness and staff that we can call when needed.”
“I’ve had zero support when I’ve tried coming off antipsychotic medication with the agreement of my psychiatrist. He agreed that I could do it but when actively trying to come off it the CMHT was hands off, save for my next psychiatrist appointment in 4 months time. I have previously called up the CMHT via the crisis number, they said they’d get back in the next day and they simply forgot to note this task.”
Physical barriers
What does the quantitative survey data tell us?
56% had not been asked by their NHS mental health team if they needed support to access their care and treatment (Q35).
35% reported that they need support to access care and treatment (Q36).
Of those respondents that required support, 74% required emotional support and 30% required support in accessing online appointments (Q37).
Some patients highlighted physical barriers to them being able to access in-person treatment and services. Feedback covered travel distance to services, the importance of help with transport to appointments, and in one case a building not being wheelchair accessible.
“Hospital care nearer to home (not over 100 miles away).”
“I have some mobility problems so I struggle sometimes to get to some appointments. I think maybe you should put on a transport service for these.”
“…the therapist I was assigned to was in an inaccessible building meaning I had to get out of my wheelchair to get in (door was not wide enough, no ramp) so I was in lots of pain the entirety of my therapy which I had to attend in order to access medicine at all.”
“Lots of help with transport and trying their best to make sure there was an appointment even when transport wasn’t available.”
Theme: Staff
What does the quantitative survey data tell us?
65% felt they were ‘always’ treated with care and compassion by their NHS mental health team (Q13).
51% reported they were ‘definitely’ given enough time to discuss their needs and treatment (Q8).
Staff clearly played a critical role in shaping the patient experience. Feedback covered a wide range of roles demonstrating the impact all individuals in the workforce can have. The evidence suggests that continuity of care is critical but systemic pressures and evolving patient needs create a challenging context to achieve this.
Personal attributes
A strong theme in the positive feedback was references to individual staff members or teams. A wide range of roles were singled out for praise, from clinicians such as therapists, psychiatrists, and nurses to care co-ordinators, and receptionists.
“My current therapist is really lovely and patient with me.”
“My CPN was very supportive and helpful.”
“GP mental health nurse helpful. Everyone I spoke with was very kind and helpful.”
“The perinatal mental health team are superb. I will be so sad to leave this service. I have been offered so much support and therapy.”
“When I called the office, the lady there always very kind and patient with me, she always asked do I need to talk to anyone, how am I feeling and I only called them to check my appointments.”
“[Name] is an excellent care coordinator. He is always ready to listen and is very approachable.”
“Reception staff made you feel welcome before your appointment, they would chat to you.”
“My therapist is the most kind, considerate, non-judgmental, supporting person and has been a very strong and positive influence on me. I have confronted some of the worst experiences and trauma in my life which were locked away for years. All of the staff are simply lovely, from the receptionist, my therapist and the consultants. I can’t praise them enough.”
A few patients reported that individuals had gone ‘above and beyond’ what was expected.
“Finally, the therapist was calming and very patient, listened attentively, showing empathy, kindness, care and compassion. Also, a willingness to go above and beyond to help and support me with my anxiety and OCD.”
“I now see Dr [Name] who goes the extra mile and makes a real effort to get to know me.”
The importance of staff demonstrating kindness and a caring attitude in particular came through strongly. There were many descriptions of staff being friendly, compassionate, non-judgemental, empathetic and supportive.
“The people involved were always caring and nice to me.”
“Non judgemental, empathy, compassion, respect.”
“The CPN comes regularly, she understands me and exudes care and compassion.”
“Respectful, compassionate, empathetic, helping with therapy, listening to solve your problems, approaching without stigma.”
“I cannot believe that the standard of care I have received is within the NHS, it has been fantastic. I have never met so many kind, professional, caring, genuine people. Absolutely fabulous. Please don’t stop this service. Thank you.”
While there were fewer negative comments about staff personal attributes, lack of care and lack of kindness was highlighted in feedback. Some patients described staff as unsympathetic, dismissive, and patronising.
“Lack of empathy from the team psychiatrist has been a negative experience.”
“Nurses could show more compassion and more time to talk to you.”
“To be treated with respect and dignity. Not to be shouted at as they thought I had understanding English; at times treated like a child.”
“Staff attitude, listening skills, lying.”
Professional attributes
Many patients highlighted the professional behaviour of staff. This included positive comments on staff being competent, polite, respectful and treating patients with dignity.
“All the psychiatrists were polite, professional and listened to me carefully.”
“Yes how professional and considerate the team members were in your dignity matters.”
“Always professional, caring and informative. Couldn’t be more helpful. Made me feel reassured that someone was finally there for me.”
“I would just add that the therapist I have been working with, [name], has been outstanding in relation to his patience and professionalism and practical tips he has given me.”
“I would personally like to request that the [service] and [service] staff members are recognised for their professionalism, dedication and exceptional standards of care. It can be very overwhelming and difficult to build positive and trusting relationships with clinicians when starting treatement. However, both individuals have such brilliant individualised approaches and insight, that it’s enabled me to build that trust and honesty. This has then in turn ensured I receive the right care quickly, which is always vital during the first stages of treatment.”
“A really good team, who kept up to date and let each other know how I was doing. A very professional and conscientious group of people.”
A few patients highlighted the competence and specialist knowledge of staff who supported them having a positive effect on their care.
“I had therapy with a dietician who was able to help me with my many menopause symptoms. She was so knowledgeable. The sessions were brilliant.”
“Yes, I saw a brilliant psychiatrist who was very informative. She listened to my needs and was extremely knowledgeable in how best to support me.”
“I was continually given options about how best to improve my mental health while my therapist was still fully in control with the knowledge of how best to recover from my eating disorder.”
In contrast, some patients described unprofessional behaviours of staff, a few of which were described as serious incidents. These included being significantly late for appointments, breaking patient confidentiality, and making inappropriate comments that could cause harm.
“I had a doctor turn up at my home, who I didn’t even know. He hadn’t read any of my notes and was 4 hours late. I never saw him again, he left!”
“Community mental health nurse said in reference to my bulimia ‘as long as you lose weight it doesn’t matter how you do it’ I raised a complaint at the time.”
“A student nurse brought out my medical notes meant not to be taken out from the ward, to my home.”
Staff training
Responses included calls for better staff knowledge or training, including on specific types of mental illness and neurodiversity. Feedback highlighted a mix of training needs for both specialist mental health staff and other healthcare professionals. Some patients held a view that staff had lacked necessary expertise or were underqualified.
“Overall, I felt the NHS staff want to help but are unable due to a lack of knowledge/training and resources.”
“Better understanding of mental (ill) health.”
“Training of psychiatrists to improve “bedside manner””
“Some nurses are not too good at ECGs as they are only learning, we get a result in the end.”
“At the very beginning of my eating disorder care a consultant “nutritionist” questioned why my family and I why we thought I was underweight (several doctors thought I was) – this was very unhelpful, all NHS staff should be taught more sensitivity around different conditions.”
“Training of what OCD actually is for all mental health staff.”
“Better awareness of neurodiverse conditions and adapting their approach to therapy.”
“Neurodiversity training must be incorporated into mental health services as a matter of urgency.”
Continuity of care
What does the quantitative survey data tell us?
36% said they ‘often’ had to repeat their mental health history to their NHS mental health team (Q12).
Patients described the importance of having the same clinician or support worker over an extended period. Feedback demonstrated that this could be affected by staff being off sick or unavailable as well as high staff turnover. Changing therapist or consultant was often described as stressful. A few patients described clinicians or support staff leaving and not being replaced, the consequences of which were a lack of support for periods of time.
“Twice, my treatment has abruptly come to an end when therapists left the service. This isn’t helpful.”
“I had several changes in care worker which increased my anxiety at initial appointments and took me time to readjust.”
“Given a worker that I got to know and finally open up to to work with me 3 months, then leave; make sure staff can complete plans with people and not walk out and leave you with the feeling of no one cares all over again.”
“Permanent psychiatrists instead of constantly changing temporary ones.”
“Cancellations of appointments. My therapist always cancelled and then went off sick so I had to go back on the waiting list.”
“The communication was dire. The psychiatrist was suddenly changed which had a big detrimental effect on [Name]. I had to complain several times about the temporary psychiatrist who made several mistakes which led to [Name] not getting the help she needed both with her mental health and her education. She was left with no therapy several times during her time with CAMHS… The constant change of staff was difficult for [Name] people with mental health problems need consistency and good clear communication which didn’t happen.”
One of the impacts of not having continuity of care was reported as creating a need to repeat their story – which could be described as re-traumatising. Outside of situations where staff changed, being asked to repeat information made patients feel unimportant, and was felt to be a waste of time. Feedback demonstrated how crucial it is to patients that staff are aware of personal details and their previous history, whether this was from memory or reading notes. Something as simple as remembering someone’s name made a positive difference.
“For my CBT, I had 2 separate phone calls about the same initial assessment – I’m not sure if they just didn’t keep notes on my last conversation but I did feel like I was repeating myself loads.”
“Try to read any notes before meeting the person, because having to retell everything is a huge trigger.”
“To have the people doing the assessments look at your notes. I had to repeat my entire mental health history. She didn’t listen to me.”
“They make me repeat the same issues over and over again. It is physically exhausting talking to them. They don’t listen to me anyway.”
“Would be great if the people I see have had the time and opportunity to read my notes. There is a lot of history, which would be useful for them to understand. However, I typically have to repeat this on every visit.”
Positive comments where continuity had been experienced make it clear how important this is to the patient experience including how it helps patients feel cared for, safe and removes the need to repeat themselves and relive their personal journey.
“We are very pleased that we see the same mental health nurse at each review.”
“Consistent person supporting me. Same person to talk to helps.”
“Having continuity of care is vital to me feeling safe. Without continuity l would find it hard to be honest about how l am feeling, especially when feeling suicidal or feeling in crisis.”
“There was one young lady at the reception area at [location] that was always pleasant towards me and she remembered my name and knew where to find my information easily.”
“My therapist made me feel very seen. Even if it was because she read our notes or because she actually remembered me and what we spoke about. I felt that she actually paid attention and cared about my progress.”
“…when I called the home care service they knew I exactly who I was and what I was going through when I just said my name, so I didn’t have to relieve everything each time I called.”
Theme: Treatment
What does the quantitative survey data tell us?
48% stated that the support was ‘completely’ appropriate for their mental health needs (Q7).
Feedback demonstrated a lack of confidence some patients had in their treatment, particularly when they felt unclear on their diagnosis, their care plan and/or feeling listened to about their needs. Further, there was evidence that difficulties in accessing therapy or other treatment they felt was appropriate and timely, contributed to a lack of trust in the service overall.
Diagnosis
Where patients mentioned diagnosis this was most often to highlight its importance at both practical and emotional levels – including helping them to move forwards. Those who shared that they had received a diagnosis indicated that this was helpful to them. Others expressed frustration and sometimes suspicion at not getting a diagnosis or not having the opportunity to explore and treat the underlying causes of their mental health problems rather than just the symptoms. For a few, receiving a diagnosis had been important in unlocking access to treatment, understanding themselves better, or securing additional support such as reasonable adjustments at work.
“Managed to get a diagnosis so I could better understand myself.”
“The care I received from the first appointment and there after has been very good. It has helped me understand who I am and how I work how my mind works and how to make it work and look after it. How can you fix something if you don’t know what’s broken or how it works. There is still some tweaking to be done with the medication side of things and coping strategies at home but I have faith that I will get there.”
“There is a lack of diagnosis with the emphasis on treat and release with no clear follow up for diagnosis which might be helpful in the patient taking ownership of their illness to prevent relapses.”
“I was hoping to get a diagnosis so I can accept it and start improving my life but it seems nobody can tell me what is wrong.”
“…also not wanting to give a reason or a name to my condition is unhelpful. And I eventually told them I had PTSD and psychosis from a known previous event, this helps me to understand what is going on.”
“…they were basically reluctant to move me on to getting a diagnosis cus they didn’t want me to have a label. But my job were asking me for a formal diagnosis so that they could follow through on my reasonable adjustments.”
“Diagnosis of dementia was delayed until any options for “Treatment” were long gone. Mum was clearly suffering from the early stages of dementia a year before the crisis that resulted in her being sectioned. I am a [job role] with basic psychiatric training and [name] is a trained psychoanalytical therapist but we were unable to “convince” the GP that success in performing serial 7s tests does not rule out dementia. I am not a conspiracy theorist but the resistance we experienced in order to get a diagnosis made feel as though there was a budget driven agenda. If treatments are available then there needs to be proper early assessment, diagnosis and provision while they might still be beneficial.”
Medication
What does the quantitative survey data tell us?
83% reported that they had received medication for their mental health needs in the last 12 months (Q20).
Feedback about medication was mainly negative, with a variety of issues shared including:
lack of information on side effects
unable to find medication that works for them
desire for therapy or other support as well
lack of support for side effects
lack of support when changing dose
infrequent medication reviews
“Medications given to be suitable and not simply put me to sleep as this is not the solution.”
“I do not think I have had enough support in reducing/ tapering off from my medication, nor have had the chance to develop a clear (timed) plan as to how I can be supported with this. My current medication has adverse side effects which cause me distress.”
“I would like to explore alternative therapies other than just taking medication to help contain my mental health. I would like this to be available to me.”
“I’ve had zero support when I’ve tried coming off antipsychotic medication with the agreement of my psychiatrist. He agreed that I could do it but when actively trying to come off it the CMHT was hands off, save for my next psychiatrist appointment in 4 months time.”
“Being listened to more. People only seem to understand from their own perspective, which is not what I am telling them. I’d like more control over what medications I take without being ignored. I’d like to be heard when I say I am experiencing ill health mentally.”
“I wasn’t listened to when I kept telling them I
Length
In the same way as intervals between appointments, the length of each appointment had mixed feedback. Positive feedback included patients who did not feel rushed, which made them feel more confident and that they had the ability to ask questions.
“Length of appointment is good and doesn’t rush me going through the things I need to talk about. I’m able to ask a lot of questions about my care.”
“Very good care coordinator with monthly appointments of up to an hour.”
“Everything the psychologist did. Going beyond one hour. Being flexible when I had no energy.”
“These appointments were never rushed or cut short at any time. Considering the precious commodity of ‘time’ that was afforded to me on these, rather (for me) traumatic occasions I can honestly say that the mental health care team went above and beyond their duty of care.”
The opposite was found in comments where this was flagged as an area for improvement, with patients sharing they felt rushed and unheard.
“In a realistic world, more time would be wonderful. An hour flies by.”
“Wish I have a bit longer with her.”
“30 minute review appointments are generally 3 minute appointments. It feels like the NHS is being ripped off.”
“Increase the length of appointments (often feel rushed or pressured to ‘perform’ in short space of time).”
“The psychiatrists are too busy trying to get next person in, rather than listening to what the patient in front of them are saying. They aren’t bothered at all. There is never enough time for an appointment – 10 minutes only, this is not enough.”
Being listened to
What does the quantitative survey data tell us?
52% felt they were ‘always’ listened to by their NHS mental health team (Q9).
Feeling listened to was a thread in feedback, most notably relating to therapy sessions though other examples were shared. Patients highlighted that when they felt heard, this made them feel safe, relaxed and that they could be honest.
“I felt really listened to and understood.”
“My therapist is fantastic. He listens, doesn’t judge or make me feel bad and takes time to understand the complexities of my mental health issues.”
“I have been working with the same clinical psychiatrist over the past 3 years, who has always been a consummate professional. From this consultant, we have discussed and they have directed me to additional support (e.g. EMDR, counselling), which has overall helped. I feel heard, understood and consulted about my welfare.”
“I had the most amazing therapist, she was kind listened to me and I was able to open up to her about my entire life from childhood trauma to most recent experiences. Not everyone can relate and adapt to assist someone in overcoming PTSD trauma but her dedication to helping me take charge of my life was impeccable here was a therapist that went above and beyond for her patients.”
“The health visiting practitioners were very good at listening to my concerns and given me valuable suggestions.”
“Health professionals I spoke to took the time to understand my issues and problems, due to listening so attentively they were able to make the right recommendations in helping me through my troubles.”
“All the people I have met whilst involved in mental health services, whether support staff e.g. receptionists, or clinical staff, e.g. CPNs, psychiatrists, have treated me with the utmost respect and trusted me enough to listen to me, even when I was obviously having a delusional episode. This makes a big difference to being able to be honest with them and thus receive appropriate care.”
Conversely, when patients did not feel heard or did not feel that they were being ‘taken seriously’, it was harder for them to trust and engage with support. Impacts shared by patients who did not feel they were listened to were feeling they were a ‘problem/burden’ or that they were not being treated as an individual but as a number. This links strongly to the insights on attributes captured earlier within the ‘Staff’ theme, demonstrating the value of feeling important and being treated as an individual.
“Please take my concerns as the patient in to account, and don’t just follow a pre-defined flowchart for how my mental health should be treated. I’m not a problem to be solved, I am a person.”
“You get the impression no one gives a damn and you’re just a number in a long waiting list.”
“The contact I’ve had from my care coordinator has been very minimal and I don’t feel I am listened to and am treated as a number.”
“I mistrusted the environment immediately, it seemed I was a problem to be dealt with rather than someone to be helped. That extent to which I was considering extreme harm to myself and others was missed.”
“I feel like I’m a burden to them and that I don’t bring enough money in for them to care about me or do there job properly. I have absolutly no faith in the mental health team at all.”
Further, some patients reported feeling frustrated that their views were not heard which could have detrimental impacts on their mental health.
“More care, actually take the time to listen and not just interrupt and guess what you’re feeling, because then it’s hard to share so the docs don’t even know all the issues.”
“Yes, I was scared and worried when I left hospital that I may harm someone or myself. I was not listened to and subsequently took an overdose.”
“Listen to the patient and don’t assume or think you know whatever the patient is talking about. That will screw their head up, just like they screwed mine up.”
“Being listened to more. People only seem to understand from their own perspective, which is not what I am telling them. I’d like more control over what medications I take without being ignored. I’d like to be heard when I say I am experiencing ill health mentally.”
Suitability of therapy
What does the quantitative survey data tell us?
61% reported that they had received any therapies for their mental health needs in the last 12 months (Q24).
A positive theme that emerged was how receiving specific therapies were helpful and made a positive difference to mental health and quality of life.
“I am receiving group therapy and one to one therapy as part of the [Name] Programme and cannot say enough positive things about it. Without it I would no longer be here. They have improved the quality of my life and even though I have a way to go it’s a journey I feel fully supported on.”
“Occupational therapy, music therapy, gym, counselling, art, pets therapy they are a great benefit. Counselling and psychology are good.”
“EMDR was extremely helpful.”
A very small number of patients highlighted types of therapy that they felt had been unhelpful for them personally, inferring their needs may not have been assessed sufficiently to provide effective treatment.
“I think the therapy wasn’t appropriate for my issues.”
“It became clear quite early on that CBT was not going to work for me.”
Crisis care
Some respondents made specific reference to crisis care provision, with largely negative feedback evident. Many of the comments reflected sub-themes elsewhere in this report, including but not limited to ‘Choice’, ‘Waiting times’, ‘Contacting services’, and communication ‘Between staff and patients.’ A summary of the feedback shared pertaining to crisis care is as follows:
unsympathetic staff
no one answered or no one called back
uncertainty about which number to call for access
need for access on behalf of patients who are unable to seek help themselves
lack of communication between crisis care and other CMHT teams
positive experiences described services as quick and caring
Patients could be scathing about the quality of crisis care, describing the experience from the service or staff as unsympathetic, reporting not receiving any help or feeling worse after calling the crisis line.
“The person I spoke to on the crisis line didn’t seem very sympathetic.”
“Crisis team – often felt like a number or chore.”
“Crisis team. I did not feel able to contact the crisis team. Because the few times I have they belittled me and made me feel totally worthless, and I was just wasting their time.”
“Same with the Crisis line where I was told to “stop shouting, ” (I was crying not shouting) and to “go and wash your face.” This was after I told them that I wanted to kill myself. Called 43 times in one day out of desperation and received no help.”
“About 18 months ago, I rang the Crisis Line one weekend. I was told he could not speak to me and I needed to call a mental health charity. It took a lot for me to call the crisis line and to be so unsupported meant I could not call the other charity and I would not call the crisis line again.”
“Crisis team needs to be better. Too many times where they’d ended the conversation and I was more suicidal than before.”
Negative feedback often related to the difficulty in contacting crisis teams or emergency helplines. Patients describe being unable to get through, long waits, and calls not being promptly returned. Some patients had called what they believed were crisis helplines only to be directed elsewhere or to call back. There also appeared to be a lack of understanding as to the role of NHS 111 in relation to mental health crises, including within the service itself.
“The mental health system is broken across the UK and [Location]. The crisis line needs sorting out as waiting 7 hours is not right and could be too late.”
“On one occasion I tried to contact the emergency NHS [Regional Mental Health service] 24/7 hotline. It went to voicemail and I didn’t hear back for 2 hours. By then I was already at hospital. I find that pretty appalling.”
“Accessing the crisis team – the number changed recently to the national 111 number. It would have been good to have received a letter, or even a text message about this. Reason being that I had a need to try and call them out of hours recently on the number I had been given (which was the old number, not 111), and was sent from pillar to post trying to get put through to the correct number.”
“The crisis team in [Location] is not fit for purpose. It takes 5 minutes for someone to answer and when they do, especially if it’s at night, they seem not interested and tell you to phone your team in the morning. There is no point to having this crisis team service as it does not do anything and benefits no one.”
“It seems that the people providing out-of-hours support, whether on 111 or whatever number is the right number, need to be updated on what it is they are supposed to be doing, and the care they are meant to be providing. As it is, after this event I was advised to contact the duty team in hours if I needed crisis care. Which means I now feel like genuine crisis support is only available Monday to Friday 9am-5pm.”
“When I was having a personal crisis I called the number issued to me. It took me through to an admin team that said nobody was there to take my call. After I asked what to do they said hold the line. They put me through to a male nurse in the hospital wing for prisoners. Of course, he couldn’t help me and just stated that the system is a mess. I emailed my MH nurse but she was not working that day, so I had to go it alone.”
A few patients highlighted the problems of crisis help being available by telephone as they could struggle to make the call themselves. This could lead to suggestions that crisis phone numbers should be accessible to family or carers of patients to make a call on their behalf.
“One massive issue for me is getting help when I am in crisis. I cannot call a number. I just can’t do it. I find it very hard to pick up the phone when I am feeling that way, so email or text system would be useful, even if its something that gets picked up the next day.”
“Crisis team to open phone lines to public (i.e. family or friend of registered patient for initial contact), during daytime hours so that people can get the help when they need it. Instead of having to wait either to see their GP or wait until the evening.”
Other comments demonstrated the high value placed on in-person assessments when in crisis and included examples of the positive impact this could have on experiences with the service.
“Crisis care was inadequate, it would have been helpful to be assessed by a practitioner in person as I did not feel I could keep myself safe, however there was no in person crisis care offered even when I asked a member of the crisis team over the phone when I had things I could seriously hurt myself with.”
“Crisis support in person is extremely hard to find.”
“The responsiveness and quick to be seen by crisis team was amazing. Everyone I met was incredible and it was great to have them visit me at home. I feel very lucky to live in a place that offers this.”
Better communication between crisis care and other mental health teams was also occasionally recommended.
“I also think my psychiatrist should be notified when I have contacted the crisis team so he can know how much I have been struggling.”
“The communication between crisis team, CMHT and home treatment team … As a person who attempted suicide the care I received immediately was not followed through with as promised”
Some patients reported positive interactions with crisis services and praised the quick and caring support they received.
“The crisis team were excellent.”
“Crisis team and doctors were very good.”
“Crisis team were fast and understanding.”
“When absolutely crisis situation, I got help quite fast.”
“When in crisis I was supported by the crisis team and they were good. The care since crisis team ended has been limited and inconsistent.”
Transition to adult services
Individuals aged 16-35 consistently identified the transition between child and adult mental health services as an area requiring improvement. Descriptions included the experience of ‘losing’ support once aged 18 alongside a lack of handover being described as disruptive.
“It’s really tough just losing support at 18 when there is so much else going on. Although there was not a need for an adult MH referral, I was still struggling. I think there should be more support from the transition from CAMHS into adulthood.” (aged 16-35)
“The continuance of care from Child Mental Health to Adult Mental Health is extremely poor, although this is more an issue with Child Mental Health discharging patients.” (aged 16-35)
“My transition period was pretty awful. Firstly I was rushed through that transition. As an autistic person I need to look around the area, have multiple meetings to get to know and trust the new person. It was more like get this over with because we have paper work and more important things so do. When they time came to be with my new care coordinator, we had one session and then she went to hospital and left the service. CAMHS said it wasn’t there problem and that it was up to adult mental health to sort it.” (aged 16-35)
Support for family/carers
Feedback suggests that when offered, support for family and/or carers could be very valuable. Other feedback highlighted this as an area for improvement, including calls for more education for families/carers on mental health to reduce stigma. Some comments interlinked support with involvement which is detailed further in the ‘Involvement of family/carer’ sub-theme within ‘Personalised care.’
“The [Region] mental health team have provided outstanding support to my husband with his complex needs; they have been extremely professional, supportive and responsive to his needs. They have also provided excellent supportive for me as his full time carer. Couldn’t have managed without them. Thank you so much.”
“Yes when I had my breakdown my family had no support they were left which caused them to have anxiety worrying about me there should have been someone for them to talk to about any concerns they had.”
“The only other point would be that I didn’t know/wasn’t told that when I was discharged my husband would be discharged from the partners support group. This was a shame. He accessed his support a lot later than me … so when I was discharged it was a little early for him. Perhaps some communication early on about this would be helpful – it came as a surprise to my husband and I.”
“More parent sessions. Parents of the past generation view mental health as a stigma and are hesitant towards mental health care. More education would help them understand why this current generation values mental heath so much than dealing with it silently.”
Theme: Personalised care
This theme demonstrates the high value patients place on receiving personalised care. This included being offered greater choice and the ability to engage with support for other parts of their lives which influenced mental health as well as treating specific symptoms.
Choice
What does the quantitative survey data tell us?
64% said they were given a choice on how their care and treatment would be delivered (Q16).
Feedback included several areas where patients would welcome greater choice in whether they had therapy as part of their treatment, and how their therapeutic care was delivered including:
method
location
mode
practitioner
Some patients commented that they had a desire to access a specific type of therapy but indicated they were not given a choice. Often this related to individual talking therapy, with some sharing that not being able to access the approach they would choose for themselves left them feeling dismissed.
“I would like talking therapy’s.”
“I wanted to work with a psychologist or psychiatrist to understand why I get recurring suicidal depression, but this was not available.”
“I found it impossible to access CBT or DBT, which would have been life-changing for me, I will never be truly stable without it and there just wasn’t the funding for it/availability, which is a real shame, and makes me more likely to need to access mental health services again in the future.”
“I was diagnosed with BPD. I take quetiapine. I feel as though I was diagnosed and just left to it. I really would have appreciated some therapy or some help other than just medication.”
“I wanted to access trauma therapy after my group work due to childhood sexual abuse but was told I wasn’t traumatised enough.”
Positive feedback was notable when patients had home visits, particularly when this enabled individuals to access care when they might otherwise have struggled to attend an appointment.
“The home visits are very helpful.”
“Flexibility of appointments, team visit me at home which is helpful with a baby.”
“[Name] from the mental health team was amazing. Having her able to visit me at home was particularly helpful as it’s really difficult for me to get out as I have an energy limiting condition and I’m severely anxious outside the house.”
A strong desire for face-to-face rather than telephone or video contact emerged as an area for improvement. However, choice and flexibility were key as the evidence suggested that what might be the preference of one person would not work for someone else.
“Offering video call.”
“Regular check-ins. Variety of appointment types – in person, at home visits, online.”
“Yes, face to face appointments. Video or phone isn’t what I expected.”
“Psychiatrist appointments are sometimes on the phone but this was not something I wanted. I preferred face to face but these weren’t always offered.”
“My first appt with [Name] was at a library/contact centre. At that point my son was still very young (approx 5/6 weeks) and the appt was early in the day. It may have been better for that to be at home.”
“A continuation of contact by phone (COVID turned me into an agoraphobic regarding contact with people (not special).”
Finding a therapist or support worker whose style worked for the patient was also an important element where patients were looking to make a choice for themselves. Some patients described getting on better with one therapist than another, and where they had been able to express a preference or change therapist, this was appreciated.
“Initial psychiatrist I saw (before Dr [Name]) I do not feel like he listened to me. I do not feel like he treated me with respect and increased my stress levels during pregnancy. However when expressing this to nurse [Name], she was able to get me an appointment with a different psychiatrist. Meaning I felt like I had options and could be involved in my care.”
“Being able to choose who gave me therapy, the people, especially [Name], have been exceptionally good.”
Tailored adjustments
Where support was flexible and could be tailored to the individual, this was reported as making a positive difference. Patients appreciated when staff took time and effort to get to know them, and when adjustments to accommodate individual preferences and circumstances were made.
“Yes! I don’t like sitting in a room with my CPN, so all my appointments are walking ones, like around the park, I talk better with her when I’m out in nature, I love that the MH manager allows me and my CPN to do this.”
“My care has been individualised, the team have made every effort to work with me to enable me to stay in the community working on my eating disorder.”
“Throughout my mental health care, I always felt that it was tailored to fit just ‘me’ and the differing changings that were happening in my life at that time and from my past. Whenever something challenging happened during the days that I didn’t see anybody from the mental health care, the help and guidance I received was invaluable to my mental health.”
“I had a very patient and compassionate CPN. I felt he adapted to the communication style I needed once he got to know me.”
“Yes, I had practical sessions with the therapist, outside and at my house and surrounding area, which were tailored to me and my specific needs. I learn best, by physically doing things, so this was a great way to help me to understand how to relate CBT techniques to me and my obsessive thoughts, rituals and behaviours in my everyday life. I just wish that I had been given these tailored practical sessions years ago. Also, the Therapist adapted the techniques, to help me to understand how to relate them to me and my OCD, by making them individual and quirky. This was a great help.”
In contrast, when care was not tailored to needs or preferences this was highlighted as an area to improve as it undermined confidence for patients in their treatment.
“My recent session was for my claustrophobia which I have been suffering from for over 20 years. The young lady didn’t sound very confident from the beginning, I had to constantly ask her to speak up. She then followed what seemed like a script. Not helpful when you are trying to battle something like claustrophobia. I didn’t finish the sessions as they would be no use to me. Please individualise your approach.”
“Have a proper conversation and not just a medical one and you may learn more about the person and the things they are struggling with. If it’s only medical, people like me only discuss that and not the things they would like to do and what help they can give them to help achieve it.”
“Stop thinking one size fits all. If it isn’t textbook they never know what to do. You can’t just treat all mental health types the same because that’s what you’ve been trained to do. Different things work for different people and there needs to be more advanced training on that.”
Holistic care
Feedback was mixed about support for patients outside of clinical support for mental health. Where this had been experienced it was reported to enhance both the experience of care and the impact of treatment for the individual.
What does the quantitative survey data tell us?
46% said their NHS mental health team ‘definitely’ considered how areas of their life impacted their mental health (Q11).
29% felt their NHS mental health team ‘definitely’ supported them with their physical health needs (Q32).
The following percentage reported ‘definitely’ receiving help or advice from their NHS mental health team with finding support in the last 12 months for: 29% joining a group or taking part in an activity; 14% finding or keeping work; 17% financial advice or benefits; 11% cost of living (Q33).
Patients highlighted positive experiences of care when they felt their needs as a whole were addressed, including getting help with welfare benefits and addiction for example.
“The occupational therapist is extremely good and helped me get the things I needed to allow me to live at home still, she also recommended someone to help me receive the Attendance Allowance that I had not been claiming.”
“[Name] from the mental health team was amazing. Having her able to visit me at home was particularly helpful as it’s really difficult for me to get out as I have an energy limiting condition and I’m severely anxious outside the house. She was also really good at looking at my life holistically and very differently and this meant she noticed things that other people haven’t and thanks to her I’m now embracing the fact that I’m autistic and getting the right help.”
“My care coordinator managed to access some help for me from an occupational therapy service.”
“[name] put me in touch with [Service name], concerning my alcohol addiction. I have now had a detox and no longer drink alcohol thanks to [name].”
The importance of attending to other aspects of patients’ lives, such as physical health, was raised as an area to improve. Comments included requests for support around housing, finances, employment and benefits, with improvements suggested in signposting to social and leisure activities.
“Physical health problems are not taken seriously by the mental health team. They need to realise that both affects the other.”
“I was given no advice on support e.g. groups to get involved with, access to a befriend for example. The main approach was on continuing to take the medication I am prescribed.”
“More communication between different services (doctors, carer) to help tackle needs which affect mental health which aren’t necessarily connected (but are in carers belief).”
“Still need support, emotional, financial help with food and bills which are increasing all the time!”
“Yes, an art class or a woodwork class, a group to talk to about anything just to get a friend.”
Involvement in decision-making
What does the quantitative survey data tell us?
Of those with a care plan, 71% said they were involved to ‘a large’ or ‘very large extent’ in agreeing their care plan with their NHS mental health team (Q15).
Of those who wanted to be in control of their care, 29% said they ‘definitely’ felt in control (Q19).
There were both positive and negative experiences shared about the level of involvement patients felt they had in decisions about their care. Positive examples from patients described how care plans and decisions were developed collaboratively between patient and clinician.
“I did not feel rushed and was listened to by MH professional. Was generally treated with respect. Was given opportunity to be involved in care plan.”
“I was continually given options about how best to improve my mental health while my therapist was still fully in control with the knowledge of how best to recover from my eating disorder.”
“I don’t feel they take control in my care it is very much led by more [of] a joint approach. Which through the traumas I have experienced in my life control was taken away so the fact none of them do this is hugely important.”
In contrast, some patients highlighted a lack of involvement in decision-making about care plans or treatment options.
“Have a say in my care plan or at least have a copy of it.”
“The lip service that is paid to client empowerment is only lip service.”
“Ask me if I want something rather than just sign me up and expect me to be happy when I get a phone call from a service I have neither asked for nor did I want.”
Involvement of family/carers
What does the quantitative survey data tell us?
45% said that NHS mental health services ‘definitely’ involved a member of their family or someone else close as much as they would like (Q34).
Patients and carers highlighted the importance of involving family/carers in decisions, noting a thread in this feedback was the context of patients having a diagnosis of dementia.
“My consultant Dr [Name] is exceptional. He involves my family in my care.”
“Yes. Contacting me or my brother (power of attorney) to be present when examining or interviewing my mother who has vascular dementia and aphasia caused by 2 strokes and is unable to answer any questions with any certainty of accuracy.”
“Living with dementia and bipolar, I feel more help and support should be given to my carer/ wife.”
“It is 39 years since my last stroke and I lost my short term memory, and dementia began. My wife has supported me throughout. She has not had any support which she would have received had the stroke affected me physically.”
Theme: Communication
Feedback on communication was predominantly negative and highlights the important role it has in building trust and confidence. In turn, positive communication experiences encourage patients to engage and support self-management.
Between professionals
There was mixed feedback on experiences of communication between professionals, with comments not always clear whether this was within teams or between teams and/or organisations. Most feedback highlighted this as an area for improvement, with patients describing a lack of, or minimal, communication between professionals leading to frustration and delays in accessing treatment.
“More communication and joined up thinking between different teams and professionals.”
“To have a more cohesive conversation between staff and not just quick meetings as too much is missed and things getting missed is the difference between life and death for many individuals.”
“I think there needs to be more communication between different professionals within the same mental health team in particular. I was seeing a support worker but my psychiatrist didn’t seem to know anything about it. I also think my psychiatrist should be notified when I have contacted the crisis team so he can know how much I have been struggling.”
“I was transferred to North Team from South Team due to moving house. I was told I could not see a psychiatrist, even though my previous psychiatrist had written to say I needed to be seen within three months. [Name] rejected three requests from waiting list coordinators who talked to me, for me to be allowed to see a psychiatrist. It was only after I put in a formal complaint with the support of the admissions prevention team that I was referred to a psychiatrist.”
Positive feedback included examples of effective co-ordination across different professionals and services.
“I am very grateful to be under the [service]. I find it very beneficial that all the professionals involved in her care at the hospital work as a team and are in contact with my daughters special needs school as well as other medical professionals from other hospitals who are involved in her care.”
“Things that I loved – different people came to visit me and support so I got different point of views, saw different people, not just only one every time. I could tell they discussed my care after each time I saw them and they always were up to date with my mental [health]. I never needed to explain again or repeat myself. It felt we are a “Big family”, it was a good feeling that they “Know me well”.”
“Good to see services becoming more integrated, different agencies working together more.”
Between GP and CMH
The communication between GPs and community mental health services was identified as an area for improvement when feedback about communication between professionals was attributed clearly to specific services. Examples of impact shared included a lack of clarity on who was responsible for the next steps in treatment and delays to treatment.
“For a long time, it has concerned me that the quality of communication between my GP and CMHT is poor. A lack of mutual access to electronic records means all communication seems to go by mail, and a delay of 6–8 weeks is not uncommon. This can cause problems if my treatment regime is rapidly changing, and neither party can keep fully up to date with my MH and physical health treatment.”
“There’s a breakdown in communication between my GP and [service] as my GP says I’ve not been discharged but [service] says I have.”
“Housebound due to anxiety and I have depression which is untreated due to GP refusal to issue medication that [Service name] mental health prescribed.”
Between staff and patients
There was mixed feedback from patients about their communication with staff. Although predominantly this was raised as an area for improvement, there were also positive examples shared. There were links to insights detailed within the ‘Between professionals’ and ‘Contacting services’ sub-themes.
Patients shared a range of communication issues between staff and patients as follows:
lack of clear explanation, such as diagnosis or care plan
not checking patient understanding
not tailoring information to the individual
lack of explanation for the purpose of therapy and/or medication
not keeping patients informed of changes
not explaining potential side effects of medication
Where patients shared detailed examples, the impact of communication issues was often that patients were left feeling concerned or that they were missing important information.
“I would like to see the mental health team to keep you informed of what’s actually going on with my care and if we’re putting a care plan in place.”
“I was discharged without being personally notified.”
“I felt overloaded with information and I found it difficult to digest all that was being said to me.”
“More explanations would be beneficial.”
“My previous CPN did not keep her appointments with me (for injections), nor return my phone calls. This is particularly worrying as I was on CTO.”
“Would appreciate knowing if my mental health aide can’t make it to an appointment to see me.”
“Communications are not always good. Not always told about changes to my lead practitioner.”
“Communication wasn’t great. The hub team pass messages on to clinicians, also some clinicians never let me know they hadn’t accepted my referral. An easier way to contact, communicate would be easier.”
Further evidence of the importance of clear explanations and feeling fully informed about the purpose of treatment was evident in the positive feedback. Patients placed importance on transparency from staff involved in their care, linking to the positive examples shared in earlier sub-themes on ‘Personal attributes’ and ‘Professional attributes’ within the ‘Staff’ theme.
“Yes, I saw a brilliant psychiatrist who was very informative. She listened to my needs and was extremely knowledgeable in how best to support me. I was put on medication by her recommendation, even though I was reluctant at first; she explained in great detail on the medication, its purpose, and side effects.”
“The Head of MHSOP is really good very firm but fair and in our meetings clearly explains what is happening e.g. medications etc.”
Contacting services
What does the quantitative survey data tell us?
78% said they knew who to contact out of office hours within the NHS if they had a crisis (Q27).
Of those who knew who to contact out of office hours, 45% said they had done so in the last 12 months (Q28).
Of those who had contacted out of office hours, 40% said they ‘definitely’ got the help they needed (Q29).
Having the ability to contact services was highlighted as an area to improve, adding weight to the earlier sub-themes on ‘Waiting times’ and ‘Crisis care’ which further evidenced difficulties patients had experienced. A range of issues were raised in the feedback relating to contacting services, including:
not knowing who to call
multiple contact details causing confusion
inability to contact services outside office hours
unsure which team or organisation to contact
calls not returned
long waits for calls to be answered
“I tried not to pester the team so refrained from contacting but I was ignored when told some one would return my call.”
“Need a direct number for mental health professional, not waiting for days for a call back after contacting office.”
“Answering the phone should not take 2 hours on hold. If you are told someone will call you back, waiting a week is not good enough. If you relay a message, then it should be passed on.”
“On my discharge from hospital I was told to get in touch with the Mental Health Team immediately as I would then have some support. I was discharged on a Friday at about 7pm. Metal Health Team can only be contacted Mon-Fri 9am-5pm and not at all on Public Holidays. Those needing support should be made aware of this availability.”
Feedback also drew attention to the complexity and difficulty of navigating the ‘system’ to access the care that they needed. Patients described feeling confused at having multiple staff or departments to contact, and frustration at being referred to services that did not exist or which they felt were inappropriate for their needs.
“There is still confusion about who to ring because of all the different numbers. The service that did provide a trained counsellor does not seem to be there anymore.”
“I saw too many people and was given too many contact numbers for different departments.”
“[service] has many teams with different roles, each with their own patient service integration and referral protocols. The service providers are unsure and the processes poorly defined. How is the service user expected to understand these protocols and outcomes. My point is, a patient could find themselves in checkmate – no way forward nor back.”
“The barrage of names organisations and telephone numbers with people with a rapid turnover of staff is overpowering when dealing with dementia. The system needs simplifying where departments inform others on the situation you’re living in. I’m at the stage where repeating myself is relentless and tiring.”
Administration issues
Patients shared a variety of examples in areas for improvement that evidenced administrative errors and their impact on the patient experience. This included referrals being sent to the wrong team or overlooked, causing delays in getting assessments and care. Other issues included letters which caused confusion and upset, and incorrect or incomplete record keeping.
“My referral was lost when CAMHS swapped to [county], [service provider], meaning from my assessment to my first appointment, for treatment took about 2 years.”
“Following through with referrals. I found out 2 years after I was ‘put on the waiting list’ for ADHD assessment that my psychiatrist had ‘dropped the ball’. I am now actually on the list but 2 years behind schedule. I was left hanging by this psychiatrist for over a year with no appointments scheduled for me. I gave up on my care only to be contacted by a person brought in to take over from her, and I was told that me and another person were left behind by the psychiatrist for no apparent reason.”
“Firstly addressing me as “Mr [Name]” when you send me letters and not my deadname as one of the main reasons I ended up needing support from the NHS was based around being transgender so for you to send me a letter addressed to name that no one calls me anymore is quite insulting.”
“Contact details should be checked at the start of any treatment to ensure messages are not left with the wrong person.”
“Additionally, poor note taking and incorrect information included in notes has been an ongoing problem.”
Accessibility
Feedback indicated that limited methods for communicating with services presented a barrier to accessing care for some patients. This includes feedback from patients who had difficulties using the telephone and requested other communication methods and for those needing interpreters.
“I am non-verbal and cannot ask about anything regarding myself as all communication is done by phone and I do not speak. Due to this, adult mental health did not try and reach out to me regarding the fact they haven’t heard from me, despite knowing I can be high risk to myself and others due to mental health. Instead they decide to discharge me until my care giver constantly reaches out to them on my behalf and keeps trying to let them know my current situation and the reason I haven’t been able to contact them. This is the second time that this has happened.”
“The language barrier, we can’t understand each other properly.”
“I feel like there should be multiply way contact someone not just try a couple phones call then close there file if they didn’t answer. I think sending letters and text to remind and help reinsure that still getting help”
“Accessible to have an interpreter (BSL).”
“Need book Interpreter BSL.”
Theme: Outcomes
What does the quantitative data tell us?
38% felt they ‘definitely’ got the help they needed (Q10).
Moving on from care was mainly raised as an area for improvement. Feedback suggests that patients need to have expectations about outcomes managed, and that it is important to ensure there is clarity on next steps before discharge.
Ongoing support needs
There was feedback that the time-limited nature of treatment was insufficient in addressing patients’ needs and left some feeling issues were unresolved when they reached the end of treatment. This echoes the ‘Frequency’ and ‘Length’ subthemes earlier in the report, which explored how the length and frequency of appointments could be insufficient in meeting the needs of patients for ongoing and/or longer-term care.
“More sessions – I don’t feel like I had enough time with just 10.”
“Having a more long term plan other than only working with people to get out of crisis. … Not limiting people with complexed PTSD to 5 sessions.”
“Long term (years, not 10-20 weeks) with the same expert person.”
“I was given 6 weeks with a psychologist and didn’t feel that I had started to get to know her.”
“My treatment also ended before I was able to restore my weight fully, meaning that I am still underweight. The treatment felt insufficient overall and I feel I am not at all recovered – I am still very much suffering from my eating disorder.”
Discharge
Patients shared feedback on their experiences of being discharged from treatment. Comments on discharge were often negative, with patients describing the experience of being discharged without notification or feeling that it was an abrupt ending. A few patients lacked clarity on why care had concluded, inferring they still had needs.
“Adult mental health has taken away my care coordinator without any explanation and my psychologist I was seeing every 3 weeks. I have no idea what is happening regarding my care and support and live in constant anxiety that one day I’ll wake to a letter that they going to discharge me again and I’ll have to battle to keep the support that I need.”
“I did not feel the psychologist who saw me initially took me seriously. I was discharged without being personally notified.”
“All the support came abruptly to an end when I reached age 65. A female nurse in a white uniform dress turned up unexpectedly on my doorstep. I didn’t know her and she didn’t introduce herself and practically the first words she said (before she even entered my house) were “I have come to talk about moving you on.) Later I was told by two different nurses that the service would no longer support me because I was not considered (due to the length of time I might have left to live) financially a good option!”
Patients also described being discharged without follow-up support, and that they felt abandoned. Examples of impact describe the worsening of patients’ mental health because of this experience.
“I did not feel I had the support I needed when I was discharged.”
“Was discharged from a month in hospital to literally no support.”
“Help and advice once the crisis team leave.”
“I was repeatedly discharged from hospital without a plan for my medication.”
“Longer more community based engagement after discharge.”
“Yes, I should of had support when I came out of residential treatment about 6 months ago. I should have a psychologist helping with my specific OCD doing some exposure and response prevention with me, especially as I had no treatment from Community Mental Health Team for 6 months, by which time my OCD got worse.”
“The sudden shocking end to DBT. This was cruel and left me alone and afraid. Suddenly my support network was removed and none of the DBT team would speak to me. They abandoned me knowing I was self-harming and suicidal. Their thoughtlessness left me extremely vulnerable.”
A few examples were shared by patients who were discharged because of non-attendance at appointments, despite still having mental health needs. Other comments indicated patients felt they had been ‘threatened’ with discharge for non-attendance or non-engagement, with suggestions that any difficulties in attending were not accounted for.
“There was no effort to accommodate the fact that in person appointments in a mental health hospital were triggering for me. No adjustments made for autism either. No offer of online or remote support. Threatened with discharge if I did not attend in person despite the aforementioned issues with this. Made my mental health worse because I attended in person. Missed university for a week because of it and wrecked my sleep for months.”
“Build better trust rather than threats. Actually help rather than “pass the problem” letters and dismissal from care with no help to access – Anxiety too high so left after so much panic / MH ACTS / hospitalisation left alone with no treatment again.”
“I started another online group which was exactly the same as my previous course. I asked why this was and that was all they could offer (pointless), but due to my physical health, I’m laid flat in my bed most of the time. I couldn’t attend some appointment as was in to much pain to thick about what I was doing and was discharged – this made no sense as I had done the course before within three months of doing this course; they knew I had mental health and physical health problems because I was laid down while doing these courses online. To then just to discharge me and leave me alone.”
“Please remember that you are caring for people with mental health conditions and the fact that they are attending your clinic means that they are engaging but it may take longer to see results than you would with a neurotypical patient. Please do not discharge on the basis of non-engagement.”
Impact
Responses included positive feedback from patients who felt that they had received the help and/or treatment they needed, even if it took a while.
“Finally got the help I needed.”
“I received the necessary care and treatment after experiencing a serious mental relapse, losing my job, and having a breakdown.”
“I get all the care to meet my needs from the mental health team and GP.”
“There method helped and worked for me.”
Many patients described the positive impacts their care had on them. Examples shared by patients included greater understanding of their condition; developing coping strategies; increased confidence and wellbeing; and getting back to their ‘usual selves.’ In some cases, the support was said to have been lifesaving.
“My psychologist really helped me understand my condition.”
“I received excellent care support and relevant talking therapy from the PTSD team. It’s twice that over 13 years that I have needed this excellent support. I truly believe that I have the tools to overcome any relapses in the future.”
“I always feel more positive after a session.”
“[Name] was so good at listening and made me feel like I had the confidence to do a college course.”
“I cannot thank enough the help what I received. The team was brilliant and I got the help what I needed to be able to process grief and postnatal depression, anxiety. Now I can fully take care of my baby, support my family and I am able to return back to work after the maternity leave.”
“They helped me to work out that I’m allowed to exist. Doesn’t sound much but is life changing for me.”
“Saved my life without a doubt thank you.”
A lack of positive impact was also shared, with some of these comments capturing how engagement with mental health services had in their view exacerbated anxiety and stress. Some patients expressed frustration that their situation had not been adequately addressed or improved.
“I’ve had a very poor experience and my mental health conditions have not improved at all.”
“Nobody listens to me and my mental health problem isn’t addressed. I’ve been severely ill since the first COVID lockdown and I’m getting worse, not better and now, because I can’t bring myself to leave the house or even my bed, my physical condition is really poor. I’m tired of my illness lasting so long without any sign of improvement.”
“They made me have physical health checks, they made me take like 50 different calls, attend like 50 different places but still never gave me any actual treatment, no therapy, no medication, no diagnosis even though they said what it was. It felt like it actually made my mental health worse because I wasted so much time trying to get the help then basically being abandoned even after attending and doing everything they asked.”
“the services have caused a lot of trauma.”
“CBT at the Eating Disorders service was very focused on weight restoration and eating and did not address the underlying mental health difficulties (such as trauma/PTSD, emotional regulation difficulties, depression) that triggered the ED. This meant that it was extremely difficult to adhere to my treatment and my new eating pattern without returning the ED behaviours when I experienced heightened stress, depressive episodes, etc.”
Other observations
Below is a list of other topics commented upon in the data that were noted during the analysis process. There was a lack of volume of comments or depth and detail to inform themes and sub-themes but suggestions are noteworthy:
Observations from patients on staff shortages and suggestions to increase funding
Dissatisfaction in how formal complaints were handled
Experience of digital therapy platforms being unreliable
Mixed perceptions of involving students in therapy sessions
4. Conclusions
This is the first national qualitative analysis delivered for the Community Mental Health Survey, and the breadth and depth of the insights demonstrates the value of inviting respondents to share their experiences in their own words. This approach has enabled respondents’ voices to shape the focus of the findings, highlighting what is important to them and what impacts their experience of care.
Overall, the report demonstrates the height of the stakes in delivery of mental health care, whereby a positive experience can be life-changing if not lifesaving, and a negative experience can worsen patients mental health and in some cases, result in trauma. There are significant challenges in access and delivery that can undermine confidence in the service. Systemic pressures and inconsistencies in care delivery undermine reliability, quality and at times, patient safety. The insights underline the importance of addressing structural challenges alongside improving relational aspects of care.
From the patient perspective, high quality community mental health care should be timely – especially in crisis – easy to access, and delivered by staff who show kindness and consideration. Personalised care is fundamental: patients need to feel heard, have some agency over their care, be treated as individuals, and receive support that adapts to their needs. Treatment should be frequent and long enough to address underlying issues or help patients manage their condition. Clear information and regular updates are also essential about their condition, care plan, waiting times and medication. Continuity of care, avoiding repeated retelling of traumatic experiences, and effective coordination across services, all feature strongly. The findings also suggest improvements are needed both in pathways into services and within them to build trust and support navigation.
The diversity of patients, their expectations and needs identified in this analysis demonstrate a varied and challenging context. The findings highlight the need to alleviate systemic pressures on staff, as workforce shortages and capacity constraints directly impact on care quality and can be seen throughout, e.g. gaps in crisis care, waiting lists, handover issues, missed referrals, ‘early’ discharge. Addressing these pressures is essential to enable staff to deliver the standard of experience of care described by respondents.
This report offers a comprehensive view of improvement opportunities though has limitations in determining which matter most and would make the biggest impact for patients. Triangulation with other datasets and targeted engagement activities are recommended to identify high-impact priorities. Ongoing listening and involvement of service users will be vital to ensure that national and local improvement efforts deliver the most meaningful gains.
5. Appendix: Qualitative analysis
Survey methodology
In 2023, the Community Mental Health Survey underwent a large-scale redevelopment, revising both methodology and questionnaire design. The 2024 survey continued to use the push-to-web methodology, with the questionnaire available to be completed online as well as in paper format.
The Community Mental Health Survey looks at the experiences of people aged 16 and over who received treatment for a mental health condition between 1 April and 31 May 2024. The survey received feedback from 14,619 people – a response rate of 20%.
Qualitative analysis
Thematic analysis was undertaken to achieve a deep understanding of the findings from the open questions asked in the survey. This sought to facilitate reflection and learning across services delivering community mental health in England.
To analyse qualitative data, the standard six steps of thematic analysis were used to identify patterns of meaning within the data and explore commonality and contrast – see Figure 1.
Thematic analysis approach
Familiarisation
Initial coding
Generating themes
Reviewing themes
Defining themes
Final analysis and report writing
An inductive approach was undertaken for the data analysis of responses to QA and QB, which is a systematic method where themes emerge from the data without any pre-existing framework being used. As a high level of consistency was found between the themes that emerged and the responses to QC, a deductive approach was used for the analysis of QC comments. This means that the thematic codes created in the analysis of responses to QA and QB were used to analyse QC.
The results of the thematic analysis have been reviewed and are shared in context of the relevant quantitative survey findings. This exploits the value of both the quantitative results, which tells us the proportion of respondents feeling a certain way, and the qualitative findings, which tells us why people feel that way. For example, where there is a high degree of agreement / positive experience evidenced in the survey data, the thematic findings offer an opportunity to understand why there was not 100% agreement / positive experience and therein, where the opportunities lie for reflection and learning.
Sub-group comparisons
Sub-group comparisons were not the focus of the analysis. Where variations were observed in the national sample, this has been included within commentary. It is recommended that further focused sampling would allow for in-depth exploration of how experiences of community mental health may vary for different groups. Observations included will unlikely be exhaustive due to the national sample and focus.
6. Appendix: Sampling approach
9,090 individuals (62% of the survey sample) provided a written response to at least one of the three open ended questions.
Qualitative data cleaning
Before sampling, further data cleaning was carried out to identify and remove extremely short comments which were of no analytical value, for example those which simply stated ‘No’, ‘N/A’ or consisted of a single character.
For QA, 1,553 comments were removed in this way, leaving 7,537 comments for the sample to be drawn from. For QB, 2,580 comments were removed, leaving 6,510 comments for the sample to be drawn from. For QC, 4,904 comments were removed, leaving 4,186 comments for the sample to be drawn from.
Sampling
It was decided to sample each of the questions separately so that all respondents with viable response to each open question had the potential to be included in the final sample for analysis. A total sample of 1,943 responses (658 (QA), 641 (QB), 644 (QC)) were analysed.
To ensure a robust approach to sampling, a purposive sampling approach was taken. This is an established best practice technique when analysing qualitative data, as it ensures that the data has enough diversity across the most relevant criteria to allow the impact of the criteria to be explored and compared. For example, if age is a criteria, including responses from all the different age groups in sufficient volume means that differences in experiences between age groups can be explored.
The criteria chosen to sample on were the age, ethnicity, gender identity, and deprivation level of respondents, as these were key demographic groups recorded in the data. A sample matrix was drawn up to establish how many comments from each of the demographic groups were to be included in the analysis to allow for sufficient coverage.
In addition to the three key demographic groups a minimum of 30 comments were included on all other characteristics including sexual orientation for instance. Please note that as there was a low volume of data from respondents identifying as Intersex, all of this cohort were included in the sample. The breakdown of the volume of comments in the sample by these different criteria is provided below.
Once the original sample of 1,943 comments had been analysed it was seen that data saturation had been reached, i.e., no new themes were emerging from the data. Had this not been achieved, additional comments would have been added to the sample as necessary, in line with best practice in qualitative analysis.
The tables below show the number of comments in the analysed sample per question. The sampling approach ensured sufficient coverage across key demographic groups to allow for exploration of how experiences may vary.
Table 1: Number of comments in analysed sample per characteristic for QA
Characteristic
Sub-group
Number of comments analysed
% of comments analysed
% of comments overall
Age
16-35
183
27.8%
26.8%
36-50
160
24.3%
22.1%
51-65
175
26.6%
27.9%
66+
140
21.3%
23.2%
Ethnic background
White
512
77.8%
85.0%
Mixed
34
5.2%
3.8%
Asian
32
4.9%
3.9%
Black
47
7.1%
3.5%
Other
32
4.9%
0.8%
Not given
1
0.2%
3.0%
Deprivation level (IMD Quintile)
1 (most deprived)
152
23.1%
23.2%
2
141
21.4%
21.3%
3
122
18.5%
19.6%
4
117
17.8%
18.8%
5 (least deprived)
126
19.1%
17.1%
Blanks
0
0.0%
0.1%
Gender identity
Female
418
63.5%
63.8%
Male
227
34.5%
35.1%
Intersex
7
1.1%
0.1%
Prefer not to say
6
0.9%
1.1%
Gender different to assigned at birth
Yes
30
4.6%
2.3%
Sexual orientation
Heterosexual or Straight
517
78.6%
78.8%
Other
15
2.3%
2.0%
Gay or Lesbian
30
4.6%
4.0%
Bisexual
47
7.1%
6.8%
Prefer not to say
49
7.4%
6.3%
Table 2: Number of comments in analysed sample per characteristic for QB
Characteristic
Sub-group
Number of comments analysed
% of comments analysed
% of comments overall
Age
16-35
188
29.3%
26.8%
36-50
141
22.0%
22.1%
51-65
171
26.7%
27.9%
66+
141
22.0%
23.2%
Ethnic background
White
495
77.2%
84.6%
Mixed
33
5.1%
4.0%
Asian
36
5.6%
4.0%
Black
33
5.1%
3.4%
Other
31
4.8%
1.0%
Not given
13
2.0%
3.0%
Deprivation level (IMD Quintile)
1 (most deprived)
142
22.2%
22.9%
2
136
21.2%
22.0%
3
124
19.3%
19.2%
4
124
19.3%
18.7%
5 (least deprived)
115
17.9%
17.1%
Blanks
0
0.0%
0.1%
Gender identity
Female
403
62.9%
65.4%
Male
225
35.1%
33.1%
Intersex
8
1.2%
0.1%
Prefer not to say
5
0.8%
1.4%
Gender different to assigned at birth
Yes
30
4.7%
3.0%
Sexual orientation
Heterosexual or Straight
497
77.5%
75.5%
Other
19
3.0%
2.4%
Gay or Lesbian
32
5.0%
4.9%
Bisexual
51
8.0%
8.1%
Prefer not to say
42
6.6%
7.2%
Table 3: Number of comments in analysed sample per characteristic for QC