
Summary
The 10 Year Health Plan sets out an ambition to build a truly modern NHS that delivers better treatment for patients and better value for taxpayers. To realise this vision, we must deliver services in new ways that better meet patients’ needs, and provide care as close to home as possible, in a way that is most convenient for them and gives them what they need when they need it. As set out in the Neighbourhood Health Framework, this will mean improving routine healthcare services, moving to a more proactive care model for people with multiple long-term conditions and delivering better alternatives to hospital care.
Commissioning reform and development will support integrated care boards (ICBs) to become more expert strategic commissioners, moving to a population health approach that aligns incentives, reduces fragmentation and addresses the imbalance of resources. Commissioners will increasingly use population-based contract models to enable providers to work together to deliver joined-up care. Delivering this vision does not require disruptive organisational change.
This publication sets out new population health delivery models to facilitate this change, supporting ICBs to commission providers around the needs of defined populations. ICBs – working with partners, including local authorities and health and wellbeing boards – will agree neighbourhood footprints that form clearly defined populations. Single neighbourhood, multi-neighbourhood and integrated health organisation contracts will be commissioned around these populations.
- Single neighbourhood providers (SNPs) will deliver services, through integrated neighbourhood teams, within a defined single neighbourhood, enabling primary care to take on new neighbourhood services that are not contracted through today’s general practice contracts – General Medical Services (GMS), Personal Medical Services (PMS) or Alternative Provider Medical Services (APMS) – which will continue to be determined nationally and commissioned locally.
- Multi-neighbourhood providers (MNPs) will co-ordinate the consistent delivery of services across multiple neighbourhoods. This may include delivering services directly at a larger scale than a neighbourhood or by ‘filling in’ services where an SNP is not willing or able to.
- Integrated health organisation (IHO) contracts will give providers a whole population health budget for a geographically defined population, underpinned by a contract. The model will empower highly capable providers to lead change through their understanding of local population need, knowledge of activity and costs, and ability to engage frontline clinicians in service redesign. IHOs will undo needless NHS fragmentation and create incentives to invest in community-based preventative care.
Purpose
Most patients’ experience of the NHS happens outside the walls of their local hospital, and they rightly expect services to be designed in a way that meets their needs and is delivered as close to where they live as possible.
Yet too frequently the services provided through primary, community, mental health and acute care can be disjointed and poorly co-ordinated, creating frustration for both the communities they serve and the staff that deliver them.
This is not a new problem. For too long, the NHS has piloted and tested new ways of creating greater cohesion between services both inside and outside of hospital, yet the conditions to support local leaders to create more efficient and effective joined-up care – whether that’s the policy environment or the financial incentives to drive a sustainable change – have all too often been lacking.
The 10 Year Health Plan marks a genuine and welcome departure from this; it sets out an ambition to build a truly modern NHS that delivers better treatment for patients and offers better value for taxpayers. It describes a care model that is personalised, preventative and proactive, and convenes professionals into patient-centred integrated neighbourhood teams. This model will deliver better outcomes for people by cutting waiting times and improving performance against constitutional standards.
The 10 Year Health Plan builds upon ambitious approaches to developing neighbourhood services that have been trialled in the NHS over the last few years.
To create the conditions for local leaders to systematise those examples in a way that best suits their local community, we committed through the Medium Term Planning Framework to work with them to:
- create a blueprint to describe the new delivery models to support both commissioners and providers to develop their system architecture locally
- work with system leaders to create new funding flows that incentivise joined-up, preventative care and empower capable providers to lead service redesign
- support commissioners to ensure these new arrangements can be underpinned by effective contracts, with clear outcomes set by ICBs as strategic commissioners
Importantly, this is not about costly or disruptive re-organisation of the provider landscape; it is about creating opportunities to use existing resources and capability differently. Our approach is to enable commissioners and providers to build on existing innovative local practices where they are working and provide clear alternatives where they are not.
Since the publication of the 10 Year Health Plan, NHS leaders have demonstrated real ambition in everything from accelerated recovery waiting times to returning to financial discipline. This blueprint is purposefully light touch: designed to amplify and support local ambition, not direct it from the centre.
This document sets out a description of the new delivery models that underpin the implementation of the 10 Year Health Plan, guiderails for local planning and next steps.
It should be read alongside the Model ICB Blueprint and Strategic commissioning framework, and sits alongside the Neighbourhood Health Framework and the forthcoming Integrated Health Organisation Blueprint.
Introduction to population-based delivery models
As set out in the Model ICB Blueprint and Strategic commissioning framework, we are developing ICBs as strategic commissioners. Over the next 3 years, they are modernising how they work to enable them to lead the change to new population-based contract models much more effectively and ensure maximum value for the money spent on behalf of local populations. ICBs will support high-performing providers to take on more responsibility where they are well placed to do so.
As ICBs become more expert strategic commissioners, they will increasingly commission providers to be responsible for meeting the needs of populations, rather than contracting individual providers in a reactive, activity-based ‘receive and treat’ model. ICBs – working with partners, including local authorities and health and wellbeing boards – will agree neighbourhood footprints that form clearly defined populations. Single neighbourhood, multi-neighbourhood and integrated health organisation contracts will be commissioned around these consistent populations.
Commissioning providers on a population basis aligns objectives across providers and incentivises the shift of care into the community and towards prevention. In setting these contracts and the underlying payment mechanisms, the commissioning approach should address how existing resources will shift to enable more efficient, neighbourhood-based care.
In achieving this, we will see providers holding population-based contracts to work in new ways, looking beyond their organisational boundaries, with a strong focus on primary prevention and neighbourhood care, underpinned by new partnerships and collaborations.
Why are we moving to population-based delivery models?
In the past, the way NHS services have been contracted for and provided has acted as an obstacle to achieving the 3 shifts in the 10 Year Health Plan, in particular:
- multiple organisations delivering care along the same pathway – in many areas, services are fragmented across multiple contracts. These contracts often cover different population footprints, use different outcome measures and are provided by multiple teams working to various strategies. This fragmentation is a barrier to understanding activity and cost data within and between providers and, as a result, makes it harder to move activity, staff and money between organisational boundaries to deliver integrated models of care
- misalignment of incentives – spend incurred in one area leads to savings accrued in another. Contracting, payment and oversight mechanisms lead to organisations focusing on their own part of the picture at the expense of best efficiency for the NHS pound. This disincentivises individual providers from implementing changes that would benefit patients and the local population and from engaging frontline clinical teams in transformation of a whole pathway
- imbalance of resources – there have been systematic increases in resources in acute care despite strategies to invest in primary and community care, which has limited primary and community services’ ability to adapt to an at-scale shift of activity
To overcome this, the 10 Year Health Plan sets out an ambition for a new value-based approach that focuses on getting better outcomes for the money we spend. This will be delivered through 3 complementary, population-based contracts commissioned by ICBs that will enable most effective use of resources and integrate care locally: single neighbourhood provider (SNP), multi-neighbourhood provider (MNP) and integrated health organisation (IHO) contracts.
Commissioning population-based delivery models
The shift to population-based contracts will require organisations that can effectively embrace new ways of using population insight and intelligence to identify population health need, set outcomes and inform commissioning decisions. To do this, they will need to:
- understand the needs and drivers of risk within their defined population, as well as current activity and associated costs. This will include using joined-up, person-level data and intelligence (including user feedback, partner insight, outcomes data, public health resource and insight) to develop a deep and dynamic understanding of their local population and their needs now and in the future, and the biological, psychological and social drivers of risk and demand, proactively identifying underserved communities and assessing quality, performance and productivity of all existing provision
- understand health utilisation and optimal costs of delivery to optimise resources
- use detailed activity and cost data to inform medium-term tactical planning, including identifying interventions that increase value and minimise risks, informing workforce and skill mix design to use the available capitated budget to optimise models of care
- use real-time data to identify individuals at rising risk or who may respond to support to stay well at home
- use national modern service frameworks to create the evidence base for new integrated models of neighbourhood care that maximise value, guiding the development of population health improvement plans
- deliver through payer functions and resource allocation by holding the budget for and subcontracting and commissioning acute, mental health and neighbourhood services through an appropriate mix of direct delivery and co-ordination of the onward delivery chain and brokering the distribution of savings and losses across providers to where resource delivers the most value for patients.
This will require new population health capability and infrastructure. The Strategic commissioning framework sets out how we should begin consolidating and building this capability. In the first instance, ICBs will lead this work. ICBs are increasingly working at a larger scale to enable sufficient consolidation of expertise.
As integrated health organisation (IHO) contracts are established, ICBs will work with IHO hosts to determine where this capability best sits. Once these new contract models are in place and providers take on more responsibility for planning care and resource allocation, ICBs will need to continue to oversee these contracts – setting population health outcomes, monitoring delivery against agreed outputs and ensuring quality, choice and waiting lists are maintained through their contractual levers.
Population-level delivery models
Single neighbourhood provider (SNP) contracts and multi-neighbourhood provider (MNP) contracts aim to strengthen the infrastructure and capability to design and deliver integrated services within and across neighbourhoods, with the potential for more incentive and outcomes-based contracts at greater scale. Further detail on neighbourhood care is set out in the Neighbourhood Health Framework.
a) Single neighbourhood providers (SNPs) will deliver new services, through integrated neighbourhood teams, within a defined single neighbourhood.
- SNPs will enable primary care to take on new neighbourhood services that are not contracted for through today’s general practice contracts (General Medical Services (GMS), Personal Medical Services (PMS) or Alternative Provider Medical Services (APMS) which will continue to be determined nationally and commissioned locally.
- The SNP contract holder will need to work closely with practices that cover the neighbourhood population to ensure they can deliver services to the registered patient lists in that population. We will consult on how this collaboration might work in the coming months.
b) Multi-neighbourhood providers (MNPs) will co-ordinate the consistent delivery of services across multiple neighbourhoods.
- MNPs will have a clear relationship with SNPs and practices, so they too can deliver services to the registered population list across the neighbourhoods they serve. This will allow commissioners to set consistent outcomes for aligned populations. We will consult on how this collaboration might work in the coming months.
- MNPs will use their scale to design and co-ordinate neighbourhood health services within their footprint, which may include delivering services directly at a larger scale than a neighbourhood or by ‘filling in’ services where an SNP is not willing or able to deliver.
- New risk-sharing approaches will incentivise neighbourhood providers to deliver effective preventative care that reduces avoidable non-elective admissions, focusing on high priority cohorts.
c) Integrated health organisation (IHO) contracts give providers a whole population health budget for a geographically defined population, underpinned by a contract.
- IHO contract holders will take on responsibility for resource allocation and service planning across the whole care pathway, holding responsibility for effectively meeting the needs of that population using available resources. Models where providers do not take on the whole population risk for a geography, for example, by taking on funding for a set of services, pathways or cohorts, are lead provider arrangements rather than an IHO.
- The model will empower highly capable providers to lead change through their understanding of local population need, knowledge of activity and costs, and ability to engage frontline clinicians in service redesign. IHOs will undo needless NHS fragmentation and create incentives to invest in community-based preventative care.
- IHO contract holders will allocate resources and design services to support the implementation of new models of person-centred care – including the shift to neighbourhoods – that will improve health outcomes, patient and staff experience and the quality of care. This will require the designated host provider to work and contract with other providers to deliver services, including multi-neighbourhood providers.
- The IHO contract holder will develop decision-making infrastructure to shift the balance of care and existing spend out of the acute sector into the community, demonstrating a strong understanding of cost-effectiveness, healthcare value and the relationship between cost and outcomes.
- The defined population covered by an IHO contract should be coterminous with one or more MNP footprints to create an aligned delivery chain for the local population and to enable commissioners to set consistent outcomes.
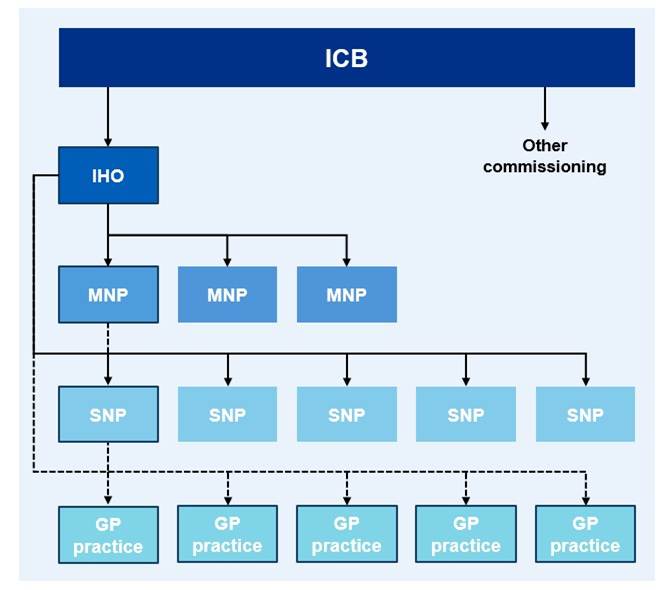
Figure 1: The IHO, MNP and SNP (and GMS, PMS and APMS) are all population-based contracts. The populations should be nested to ensure commissioners can set aligned outcome objectives.
Diagram description:
This diagram shows how population-based contracts fit together across an ICB area.
- The ICB contracts a single integrated health organisation (IHO) for an area.
- The IHO then contracts a number of multi-neighbourhood providers (MNPs)
- Each MNP works with multiple single neighbourhood providers (SNPs).
- Each SNP works closely with all local GP practices in the neighbourhood. The dotted line shows how GP contracts remain nationally determined.
The bold outline on the providers highlights one neighbourhood as an illustrative example. The diagram illustrates how these contract types nest within one another so outcomes can be aligned from system level through to individual neighbourhoods.
NHS trusts will be designated by NHS England and the Department of Health and Social Care as eligible to hold IHO contracts. Designation will provide assurance that these trusts have the capability to work in partnership across systems and to manage the additional risk and subcontracting requirements of holding an IHO contract. Initially, these will be high-performing and highly capable advanced foundation trusts. Designated trusts will be commissioned by ICBs using a newly developed IHO contract. We anticipate that community, mental health and acute trusts could all be eligible to be designated as IHO contract holders.
NHS England will work alongside the first wave of IHO contract holders to test the model and develop a pipeline for wider rollout, including to areas where there is compelling evidence that an IHO approach can solve entrenched problems in a health system.
We expect all IHO contract holders to think carefully about how they build and sustain mature partnerships with their local communities, including local authorities and third sector organisations, both as they develop their proposals and in their future governance. In particular, primary care clinical leadership in IHOs will bring local insight, clinical leadership and patient-centred design right to the heart of decision-making. This will enable communities to design care that works for them, integrating primary, community and specialist services into one seamless system.
IHO contracts will only ever be able to be held by NHS organisations. However, we will develop routes for mature neighbourhood providers to lead an IHO either by partnering with a statutory NHS organisation (through an alliance or joint ventures), by working within an NHS organisation, or by forming a new NHS organisation themselves. This approach blends the agility of general practice with the scale and accountability of the NHS.
What the future can look like
Achieving the ambitions set out in this publication will deliver a radically reformed NHS – a culture where highly capable, empowered providers take on greater responsibility for leading the planning and delivery of end to end pathways, and where decision-making is underpinned by shared data and strong actuarial analysis. Our aim is for all trusts to achieve advanced foundation trust status, and for all areas of the country to be covered by an IHO contract. We will design financial and regulatory reforms so that there is an incentive to move to the IHO model as the status quo of fragmented and episodic care will be unaffordable
ICBs will continue to play an important role as strategic commissioners, working closely with health and wellbeing boards (HWB), local authorities and other partners to determine the outcomes that its contract holders must deliver.
IHO contract holders will subcontract neighbourhood services, most likely through multi-neighbourhood providers (MNP), and take on local contract management responsibility for GMS (or PMS or APMS) general practice contracts, as well as pharmacy, optometry and dentistry, all of which will continue to be determined nationally. They will – of course – need to work with partners across health, local authorities, social care and the voluntary sector, among others, to discharge their responsibilities.
IHO contract holders will either directly deliver or subcontract the remaining acute, mental health and community services from a range of providers, including trusts and independent and third sector providers. IHO contract holders may choose to contract some community services via MNPs where there are particular benefits to consolidating services and improving integration. IHO contract holders may also use lead provider arrangements for specific services, for example, mental health, learning disability and autism pathways or ophthalmology, where there is another provider in the area well placed to lead resource allocation for a specific pathway.
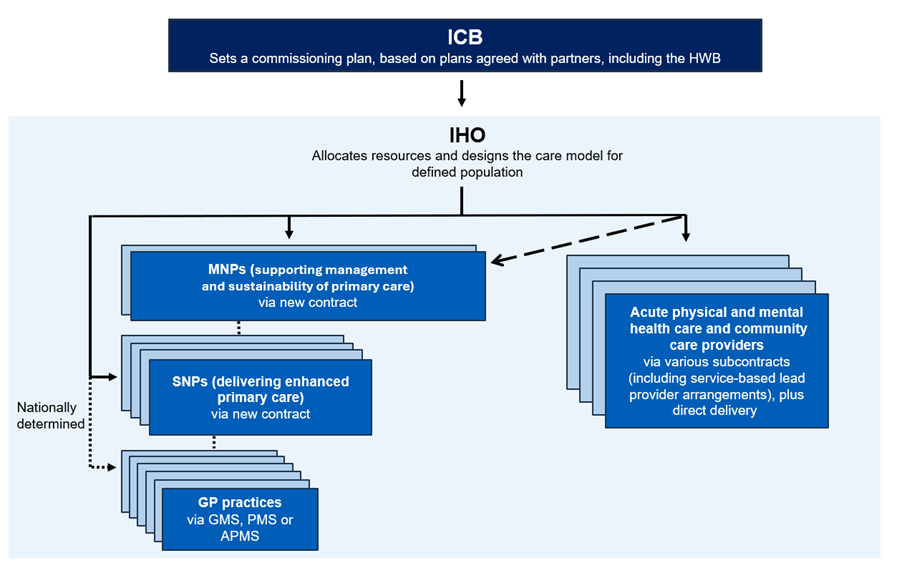
Figure 2: ICB commissions an IHO to lead on resource allocation, the IHO makes decisions around delivery and onward subcontracting, working through neighbourhood and non-neighbourhood providers.
Diagram description:
This diagram shows how an integrated health organisation (IHO) allocates resources and designs the care model for a defined population.
- The ICB sits at the top and sets a commissioning plan based on plans agreed with partners, including the health and wellbeing board (HWB).
- The IHO then sits below this and contracts delivery across different types of providers.
The diagram shows that this will involve multiple multi neighbourhood providers (MNPs), single neighbourhood providers (SNPs) and GP practices.
- MNPs (shown in the top stack) support the management and sustainability of primary care and are contracted via a new MNP contract.
- SNPs (shown in the second stack) deliver enhanced primary care through a new SNP contract.
- GP practices (shown in the third stack) continue to hold GMS, PMS or APMS contracts. These are connected via a dotted line as the contracts remain nationally determined.
A broken diagonal line highlights the shift towards more neighbourhood level models, indicating that more services will be delivered through MNPs and SNPs rather than through traditional acute or community provider subcontracting.
On the right hand side, a stack of rectangles represents acute physical and mental health care and community care providers, which the IHO may subcontract through service based lead provider arrangements, plus direct delivery.
Overall, the diagram illustrates how the IHO co-ordinates a mix of neighbourhood based and wider acute and community services, signalling a growing emphasis on neighbourhood models.
Delivering this change together: Guiderails for local planning
Our new operating model describes the return to locally led ambition. There is no one-size-fits-all approach for navigating the transition to the models outlined above; local leaders will best understand the route to the end state architecture.
Nevertheless, it is important that we avoid unwarranted complexity in the system and confusion around roles and responsibilities. Therefore, we have set out guiderails to support strategic commissioners and providers around the core expectations:
Purpose and roles
These new delivery models will drive the move to a neighbourhood health service while ensuring resources are also used effectively so that day-to-day performance and delivery is improved.
In all circumstances, the ICB will retain its role as strategic commissioner, but some responsibilities will shift when an area moves to an IHO model.
Providers will retain their role in delivering high-quality care but also have the opportunity to take on an enhanced role in allocating resources and co-ordinating the onward delivery chain.
Many providers will continue as now to hold multiple contracts; for example, a provider commissioned to hold an IHO contract for a particular population may continue to deliver services under the NHS Standard Contract for people outside of that population. Similarly, in transition, ICBs will also continue to commission via existing contract methods and/ or lead provider models for a subset of the local population, pending full IHO coverage.
The success of these models will be judged by the delivery of locally determined objectives, as well as Medium Term Planning Framework objectives, and by improvements in performance against the National Oversight Framework.
Local actions
ICBs and their partners, supported by regional teams, should begin developing plans for adoption of population health delivery and contracting models locally. We will expect ICBs to be able to set out how they will have begun implementing some outcome-based contracts within 3 years, with a view to IHO contracts becoming the norm.
As set out in the Neighbourhood Health Framework, we expect all ICBs, working with partners in primary care and local government, to agree neighbourhood footprints.
We expect to see a rapid shift towards commissioning care on a population basis using these agreed neighbourhood footprints.
To drive the shift to prevention and to neighbourhoods, commissioners should move towards new nationally developed financial flows and locally developed variants that increase resources invested in care out of hospital. This may include risk-gain sharing arrangements, initially on an upside basis, that incentivise and reward the shift of activity into community-based, preventative care.
Next steps
The NHS is undergoing the biggest change process since its inception: moving away from an era where unparalleled levels of bureaucracy, complicated rules and unnecessary processes have constrained and restricted transformation to a new way of working where local leaders are empowered to drive the change their patients, communities and staff want and need to see.
This blueprint for population health delivery models is a key building block in creating the conditions for that new way of working to take root and really support accelerated, locally driven change.
The approach we need to take collectively to successfully seize the opportunity set out in this blueprint is to continue working hard together, avoid organisational self-interest at all costs and focus relentlessly on using the new models to dramatically improve local services.
NHS England’s commitment is to support the local development of the capabilities required to use novel contractual models more effectively through the Strategic Commissioning Development programme.
The programme will provide a range of support to ICBs and their partners to work through how they adapt the necessary levers to change the investment pattern and contract for novel lead provider models (such as MNPs and IHOs). This will include three main areas: (1) specialist analytics and actuarial support from partners, (2) Board development and accredited training, and (3) a programme of action learning on how contract differently, including baselining risk and cost, setting outcomes, market assessment and development, capitated payment models, and contract management. The programme will benefit from significant national investment over the next two years to secure a range of subject matter expertise to help local teams adapt their approaches. The programme will be available to both ICBs and their key partners, such as designate IHOs, who will need to develop core strategic commissioning skills.
We all should recognise that 2026/27 will be a developmental year for all 3 new contracts (SNP, MNP and IHO). The Department of Health and Social Care and NHS England will work closely with the first new SNPs and MNPs to develop the neighbourhood care model. NHS England is also working with some ICBs to develop new payment models to support neighbourhood services, including for the high-priority cohorts (those with moderate to severe frailty, who are in care homes or housebound, or at end of life) with the aim of reducing avoidable non-elective admissions. We will outline the co-designed payment approaches for all ICBs to consider shortly.
We will also continue to work closely alongside providers and commissioners to provide further technical guidance for consultation on the implementation of novel SNP and MNP contracts. We will test out the different ways MNPs can be established and how the wider partnership of primary, community and social providers and an MNP relates to each other. We will consult on how MNPs, SNPs, GMS and the Primary Care Network Directed Enhanced Service (PCN DES) will work together, including how PCNs might evolve into SNPs.
NHS England will designate the first wave of providers eligible to hold IHO contracts in Spring 2026. Last November we published for consultation a draft Advanced Foundation Trust Programme – guide for applicants. This sets out expectations of how newly authorised advanced foundation trusts can apply to become designated as capable of holding an IHO contract. The final version of the guide will be published in Spring. We will also issue further detailed guidance in an IHO blueprint document in the coming months.
Through an Integrated Health Organisation Implementation Programme, we will work with IHO designates and their commissioners during 2026/27 to co-develop service scope, contract objectives and new financial flows to support the shift of resources into neighbourhoods, bringing in relevant thought leaders and international experts. We will learn from this to refine the implementation approach and develop a pipeline to ensure IHOs can become the norm.
We think provider group models also have a role to play in the future system architecture, particularly in capturing the benefits of scale and sharing best practice to support improvement. To support the continued development of effective provider group models, we will work with system leaders to learn from existing models so we can publish good-practice guidance later this summer.
Please direct any questions to england.systemdevelopment@nhs.net – we’ll use them to inform next steps.
Publications reference: PRN02244