
Introduction
This framework for proactive and sustained oral health care delivery across the later stages of life represents a change of approach. It does not propose new services; instead, with a focus on prevention regardless of care setting, it takes needs- and evidence-based proactive approaches to oral health service provision, inclusive of primary care and public health.
Most current models of oral care focus on care settings. Transformation of care delivery arrangements is needed to address the challenge of the evolving epidemiology of oral diseases and health combined with demographic changes. This includes integration of oral health into wider health and social care, training the workforce in gerodontology and flexibility in dental service provision. Central to this is partnership working across dental, health and social care systems and co-producing clinical care pathways relevant to local contexts and communities.
In England, the number of people aged 65 and over has almost doubled in the last 40 years (by over 3.5 million) and in the next 40 years the number aged 80 and over is set to more than double to over 6 million. As well as these demographic changes, there has been a shift toward patients wanting to retain their dentition for longer and undertaking complex and costly restorative treatment that can be difficult to maintain long term. The 2021 adult dental health survey suggests half (52%) of adults in England aged 75 years and over have 21 or more natural teeth.
Therefore, we now have a growing population of older people who are retaining their often heavily restored teeth for longer and who need support with effective oral care. Many older adults live independently without any need for formal or informal support, including to maintain good oral health. However, many others experience increasing physical, sensory and cognitive decline that can contribute to rapid deterioration in their oral health from inability to self-care and reliance on others, difficulty in expressing pain and dysfunction, and increasing challenges in accessing and accepting dental care. They need support for effective daily mouth care and access to appropriate dental services for their needs, which with ageing can become more difficult and complex to manage.
National oral care programmes focused in care homes in Scotland (Caring for Smiles) and Wales (Gwên am byth) and in hospitals in England (Mouth Care Matters) have demonstrated good outcomes and learning. However, there is no national programme in England for care settings or hospital settings.
Who is this framework for?
It is for dental systems: dental service providers and commissioners of oral health and dental services, including local authorities.
Local authorities, dental commissioners and dental leads within integrated care systems (ICS) will find the guidance useful given their responsibilities for delivering and monitoring dental public health initiatives and dental services. Clinicians and providers of services, including dental teams from the general, community and hospital dental services, will be able to draw on several aspects of this framework, however, the absence of clear guidance on pragmatic management of the ageing dentition is recognised.
Defining ageing and older person
Ageing is complex with biological, social and psychological changes presenting in an unsynchronised order. In line with the World Health Organization (WHO) framework for healthy ageing, this framework considers dependency rather than numerical years.
There are 3 categories of older person in the WHO framework and ICSs should explore the needs of each of these within their population when planning oral health improvement activities and dental services:
- A functionally independent older person who can live independently although they have some chronic diseases.
- An older person living with frailty who needs some assistance and may be living independently or in a care setting.
- A functionally dependent older person who needs assistance and will be living in a care setting or in their own homes with 24-hour care.
We strongly recommend that oral health programmes and services embrace the whole ageing life course to reduce the risk of inadvertently increasing oral health inequalities.
General health, oral health and ageing
There is strong evidence for a bilateral link between a person’s general health and oral health.
Good oral health is central to ensuring people can eat a well-balanced diet and avoid under or malnutrition. In turn, adequate nutrition and hydration are essential for the maintenance of oral tissues, saliva flow, ability to chew and the prevention of dental caries and periodontal diseases, as well as overall wellbeing. Loss of dental function and aesthetics or pain may also affect quality of life and self-confidence.
Risk of dental diseases is compounded in people with:
- cognitive decline: inadequate toothbrushing, changes in eating habits and dry mouth (related to polypharmacy) all increase plaque accumulation and consequently risk of dental caries and periodontal diseases
- frailty: linked to missing natural teeth and need for dentures, and the ability to chew food
- multimorbidity: linked to the oral impacts of polypharmacy
Over time, older adults can find access to professional dental care increasingly difficult and they may present with unique complexities (cognitive and physical decline) that make it harder for them to comply with routine mouth care and dental interventions. Patients may also have fluctuating capacity or lack the capacity to consent to dental treatment. When a need for dental treatment is identified, the range of deliverable treatments may need to be modified and decisions made in the best interest of the individual.
Fundamental to the dental team’s approach is early intervention and continual prevention throughout ageing, adapting to patient needs. A shared care approach may be appropriate when a patient’s care increases in complexity. This may be within a shared care model between general, community and hospital dental services and should work across routine and urgent dental care.
A systems-wide approach
ICSs should understand the local oral health needs for the older people residing in their area and how well these are being met by public health approaches and access to dental care. As older adults are treated across dental care settings, planning should be considered a partnership with local dental committees, local dental networks, oral health promotion services, workforce training and education and other experts under the clinical leadership of a special care dentistry managed clinical network (MCN).
Public health and oral health promotion
This section highlights the need to:
- focus on a preventative approach
- work with health and social care partners
- consider local workforce, training and education needs
Embedding a preventative approach
The public health approach for our ageing population’s oral health involves acting earlier in the life course.
Local authorities hold statutory responsibility for improvement in the oral health of their population. Local systems should work together to understand what public health measures are and should be in place to improve the oral health of their older population.
Fundamental to preventing dental diseases and slowing their progression are regular removal of dental plaque from teeth and the gum line, advice on management of dry mouth and fluoride interventions, together with avoiding tobacco, enjoying a healthy diet and drinking alcohol within safe limits. Care homes should adopt healthy food policies and healthy diets should be encouraged for those living in their own homes. Oral diseases are largely preventable. As some older adults will rely on carers for support, it is essential that informal and formal carers are given appropriate oral care training. All preventive advice should be evidence based and align with Delivering better oral health. Those living in care or nursing homes should have support with their mouth care routines in line with NICE guideline NG48 Oral health for adults in care homes.
Collaborating with wider health and social care
The anticipatory care approach focuses on intervention before deterioration. For oral health this means understanding a person’s priorities and pragmatic care and treatment planning to ensure maintenance and function. Working with health and social care colleagues, namely dieticians, pharmacists and general medical practice teams , offers the opportunity for oral health to be supported from point of diagnosis of a general health condition as part of a collaborative and multidisciplinary approach to patient care.
Evidence-based resources, such as the Mouth Care Matters toolkit for hospital care and Dementia Friendly Dentistry guidelines, as well as evidence from the academic literature can be valuable in designing oral health programmes and dental services locally.
ICSs should consider local opportunities for oral health integration through primary care networks, voluntary sector organisations and social care providers, including to ensure those on complex care lists, such as frailty or dementia, are directed to the right dental services for maintenance of their oral function and comfort. Integration of data across health, social and dental care should be prioritised, such as access to the summary care record to facilitate appropriate, holistic, safe and patient centred dental care planning.
Local workforce, training and education
Service planning for clinical care at different points in the ageing life course, be it for prevention and early intervention, maintenance and function or comfort, and in various settings must consider the oral health workforce and the opportunities around skills mix. There has been a focus on training of formal carers, in particular in care homes (NICE guideline NG48, CQC Smiling Matters), but with many older adults residing in their own homes, training and education of informal carers as well as care agency staff is needed. Training should be continuous to ensure carers can adapt as a person’s care needs and ability to accept oral hygiene practices change.
Additionally, oral health training of wider health care team care staff (dieticians, pharmacists and general medical practice teams) is needed to widen awareness of the factors that impact on oral health. Delivery in local training centres, general practice training hubs and social care training centres present opportunities to raise awareness of the impact of poor oral health and importance of taking a collaborative approach to make every contact count.
NHS England Workforce, Training and Education (WTE) teams hold the remit for health and social care staff education and development and local authorities have statutory responsibilities for oral health improvement. Therefore, a joint approach with NHS commissioners that encompasses training and service design should be sought to ensure a whole system approach.
Caring for vulnerable, complex older adults requires specific skills. Dental teams need to be upskilled in gerodontology and managing the older patient, education that should start in undergraduate programmes, and dental care professionals should be facilitated to work to their full scope of practice in both preventative programmes and clinical care delivery. Clinically, this will be driven by partnership working across the special care dentistry MCN, restorative dentistry MCN and NHS England WTE teams.
All dental team members should be up to date with current relevant guidance and training, such as safeguarding, obtaining consent and management of patients taking certain medication. However, more bespoke training on the management of an older complex patient and their dentition should be a feature of any commissioned care as it lends to the development of shared care models.
Primary care and care pathway considerations
This section highlights the need to:
- assess current provision as a baseline to service planning
- adopt a shared care approach
- commission complex care
- embed quality and outcome measures
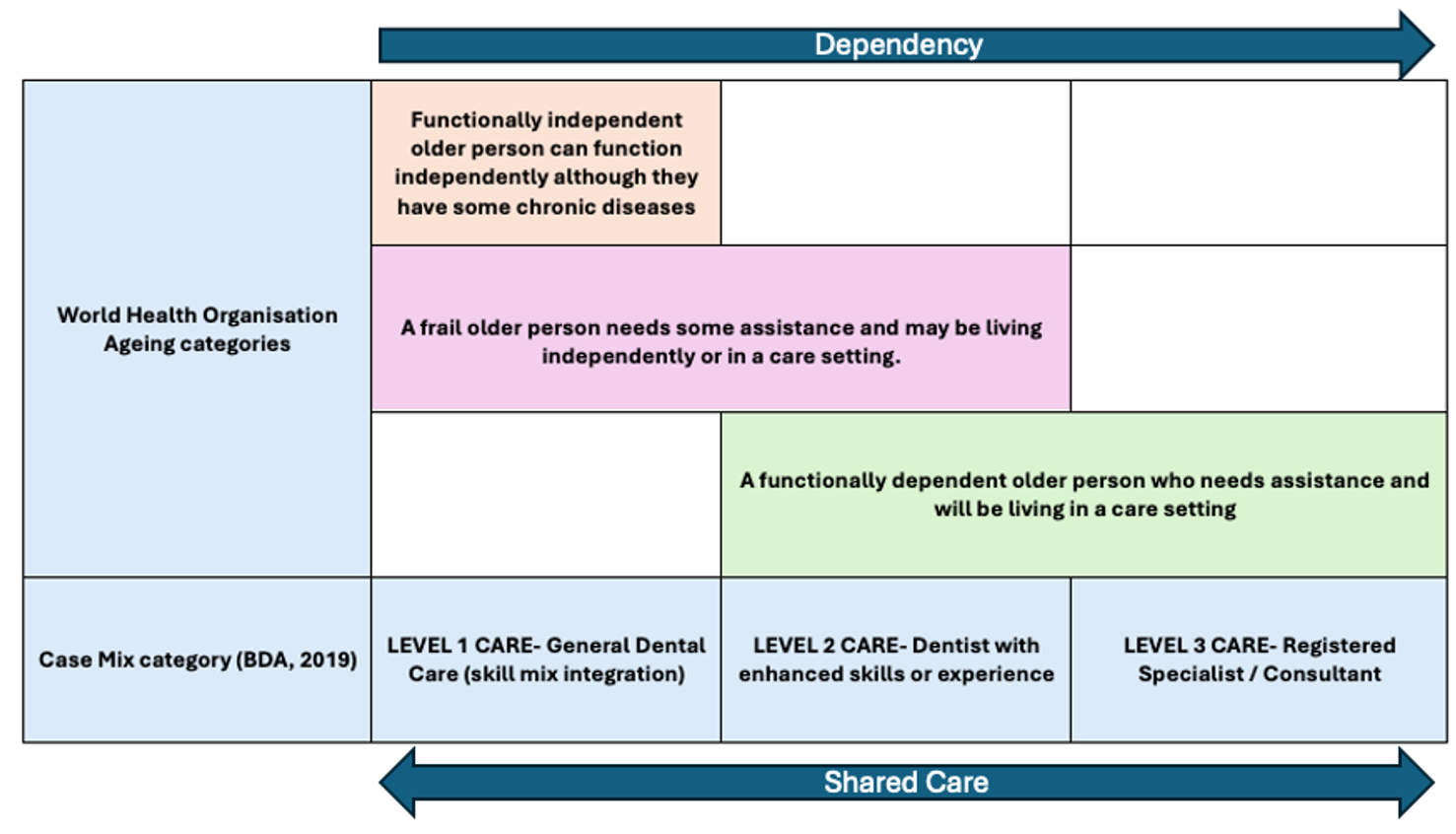
A shared and flexible approach to patient care should be standard, whereby patients may access specialised services for specific treatment and move between services as with any other patient group. This should include skill mix integration in all settings to allow a patient to move between level 1, 2 and 3 of care (see Figure 1 below) based on the dental treatment they need and their changing behavioural, social and physical care needs.
In a shared care approach most older adults should be seen in general dental practice. Patients can be referred to community or specialist care for a particular treatment or course of treatment and then return to their general dental service for their continual care once the treatment episode has been completed. For those unable to attend a clinic, domiciliary dental care (DDC) will need to be factored into commissioning models for both community dental services (CDS) and general dental services (GDS), but with specific, clear and standardised referral criteria in place to avoid unnecessary DDC.
To date, the focus in dental service design for older people has been dental care provision for those living in care homes, which overlooks the carer training, dental access and prevention needs of those continuing to live in their own homes. Service design needs to consider early intervention for all older adults regardless of setting. Different dental service models may need to be offered depending on specific barriers to accessing clinic-based care, including clinic-based care with transport facilities and domiciliary care.
It is reasonable to consider that those residing in a care setting or in receipt of supported care in their own home will have an elevated level of dependency, be it behavioural, social or physical. Higher dependency may indicate complex oral health care needs, which need to be reflected in service design and workforce expertise. This should include oral care for older patients who are hospitalised or in rehab facilities as this is often when they are at their most vulnerable.
The clinical care pathway should begin with assessment of the older person’s need (functionally independent, frail or functionally dependent) and whether they are living independently. This preliminary assessment will determine the appropriate clinical care pathway for the patient’s overall needs.
Where appropriate, an older person’s family and carers should be facilitated to be involved in important care decisions and how to do this should be explored as part of service delivery design.
Figure 1 maps the dependency needs of the 3 categories of older person in the WHO framework (WHO, 2020) to the British Dental Association (BDA) Case Mix level of care. The BDA Case mix tool provides a framework for the provision of care that can be provided within the scope of practice of a general dental practitioner (GDP), dentist with enhanced skills or a registered specialist or consultant in primary or secondary care.
Figure 1: Dependency needs of the WHO framework categories of older person mapped against the BDA Case Mix level of care
Assessment of current provision
The commissioning of any services should be informed by an oral health needs assessment. Under the remit of the special care dentistry MCN, this may be completed in partnership with consultants in dental public health and the local professional network. It should cover access to general and community dental services as well as secondary care and DDC, but the focus should be on need through the ageing life course rather than setting.
Data by inclusion group on prevalence of general health conditions, dependency and care may be useful as a predictor of unmet need alongside activity data. Also, as detailed activity data for specific inclusion groups is lacking, commissioners should explore the use of proxy data with local authority and NHS analytics teams, such as using dementia lists or lists of those who have home social care visits.
Disability does not imply need. For many older people with disability, treatment can and should be provided within the general dental practice setting. Only those meeting the criteria should be referred to specialised care for a specific routine or urgent course of care, in a shared care model with their GDP. The need for DDC can be modelled using wider health and social care services data, and where possible the required level should be commissioned to an appropriately skilled provider in the context of a wider care pathway for clinic referral.
Commissioning complex care
Securing excellence in commissioning NHS dental services directs a care pathway approach for dental services, whereby care pathways apply consistent, nationally agreed descriptors of case complexity across all levels of care. The levels of care (1, 2 and 3) patient descriptors reflect the workforce skills and environmental requirements to deliver each level of care complexity.
A clinical guideline is needed on pragmatic treatment planning for older adults with a consensus on criteria of care that is evidence informed but also practical. This needs to be delivered in partnership with special care dentistry and restorative dentistry experts and should underpin the standards of expected clinical care for all dental professionals. It should be noted that caring for vulnerable, complex older adults requires specific skills.
Most older adults should be seen in primary care dental services. However, as their care needs and complexity change over time, they may need other specialised services through a shared care approach for specific treatment. This approach should also apply to DDC if they can no longer access clinic care because they become dependent while continuing to live at home, are hospitalised or move into a care home. All services should adopt a standardised approach to triage using the BDA Case Mix tool for all older people (see table 1 below).
Once the episode of dental care or period ends, patients should be discharged back to their GDP for routine care and monitoring. A patient centred care approach should be taken, with unnecessary referrals avoided for the continuity of routine care and monitoring of the patient and to not overload community dental services. This may require upskilling of local dental teams to facilitate models that encompass urgent and routine care, where all members of the dental team can work to their full scope of practice.
Patients who require more specialised management for their dental treatment may need to be referred to an alternative service such as domiciliary care or services for those on a palliative care pathway.
Under the Equality Act 2010 all providers of NHS services are required to make reasonable adjustments for patients with additional needs and all patients should be treated with equality, respect and dignity. Reasonable adjustments may include extending the appointment time and supporting the interaction with particular equipment or facilities.
Table 1 describes the characteristics of patients requiring care at level 1, 2 and 3 and the factors affecting their eligibility. These are not exhaustive and intended as indicators of what is beyond the scope of reasonable adjustment from GDS providers and when onward referral of a patient should be deemed appropriate.
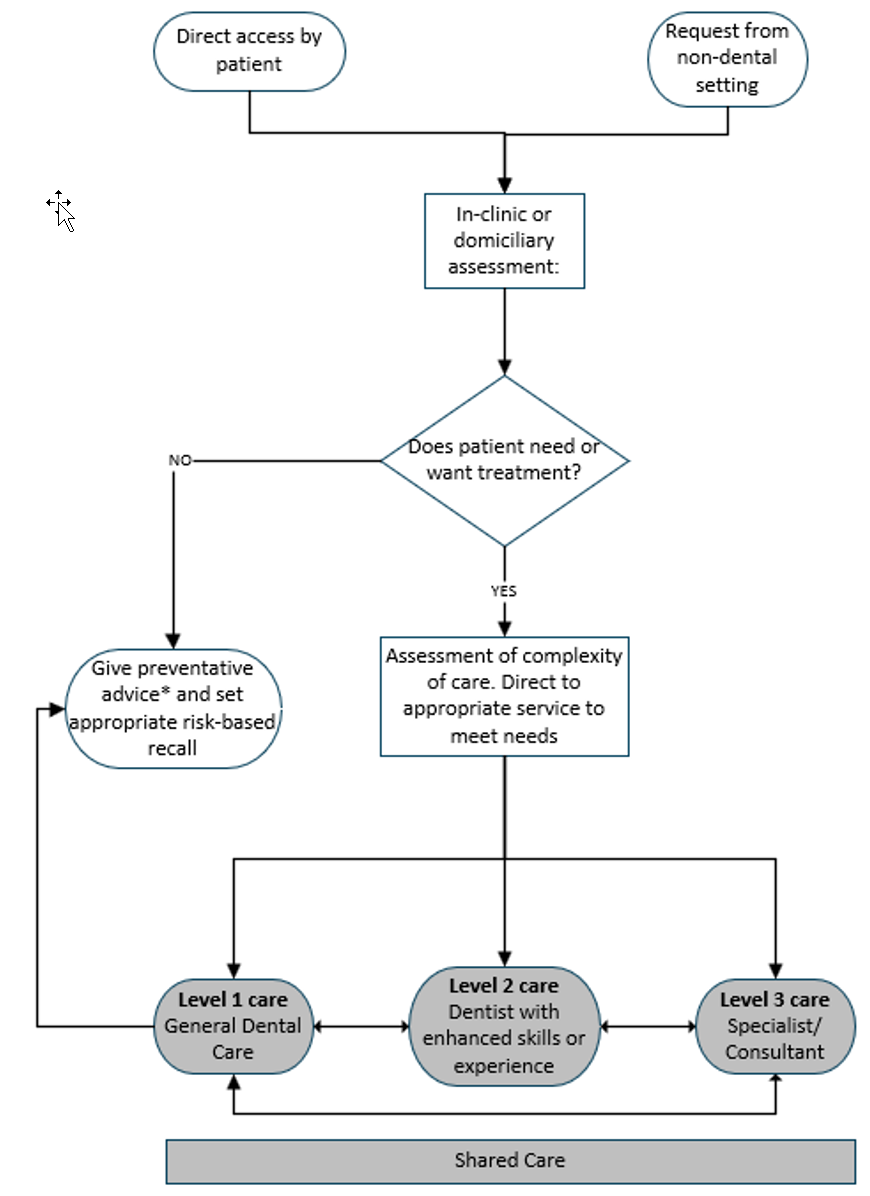
Figure 2 provides an illustrative patient pathway across level 1, 2 and 3 care.
Table 1: Description of patients requiring care at level 1, 2 and 3 and the factors affecting eligibility against BDA case mix tool
| Case mix category (BDA, 2019) | Level 1 care – general dental care (skill mix integration) | Level 2 care – dentist with enhanced skills or experience | Level 3 care – registered specialist or consultant |
|---|---|---|---|
| Communication | Free communication with adequate understanding between patient, carer and dental team. Patient can communicate for themselves without intervention of a third party. Some difficulty in communication but can be overcome. | Significant communication difficulties due to multisensory or cognitive impairment, | No ability to communicate due to impairment. |
| Co-operation | Patient will accept all restorative care and simple extractions with LA +/- routine behavioural management techniques. Some difficulty in co-operation. Full examination and simple treatment possible but requiring support or behaviour management techniques. | Presents with a disability or psychological or mental health state that means only limited examination is possible or significant treatment interruption due to inability to co-operate or tolerate procedure or inappropriate behaviour resulting in only a limited examination. | Presents with severe disability or mental health state that prevents patient from co-operating with dental examination or treatment. |
| Medical | Adequate medical history obtainable at appointment with no significant relevance to this course of treatment. No additional investigations required. Some treatment modification required. Medical history cannot be obtained at first appointment. Further information required to complete medical history. | ASA 3 moderately controlled medical condition(s). Progressive degenerative medical or disabling condition: intermediate stage where specialised service of risk assessment is required. | AS 3 unstable and ASA 4 medical condition. Progressive degenerative medical or disabling condition: advanced stage. |
| Access | Patient can access surgery without additional requirement. Patient requires support to access the surgery, for example carer attends, and may need positioning aids to self-transfer to dental chair. | Requires transport to access dental surgery or special equipment to transfer to dental chair (manual handling risk assessment, hoist). | Patients who require secondary care facilities for access. |
| Oral risk | Minimal risk factors: stable oral environment; teeth brushed twice a day with fluoride paste. Moderate risk factors: good oral hygiene hindered by manual dexterity; course of treatment following a period of neglect. | Severe risk factors: oral hygiene requires support of third party; altered salivation; access to oral cavity severely restricted. | Extreme risk factors: access to oral cavity for dental treatment severely restricted by major positioning difficulties, inability to open mouth or dysphagia problems; patient unable to tolerate home oral care provided by third party; requires multidisciplinary management of oral care with high risk factors for oral disease. |
| Legal and ethical barriers to care | No legal or ethical issues affecting care, for example no problems with consent. Some legal or ethical issues may arise. | Best interests require second clinical opinion. Doubtful capacity to consent, clinician required to make best interests decision and consult or correspond to do so. | Patients subject to Deprivation of Liberty safeguard or court decision regarding their oral care. Clinician required to make a non-intervention decision where there is extreme difficulty in providing care and it is not in the patient’s best interests to provide active treatment. |
Figure 2: Illustrative dental care pathway for older adults
Quality and outcome measures
Integrated care boards, under the special care dentistry MCN’s clinical leadership, should shape local arrangements for older adults and co-develop appropriate quality and outcome measures as part of the service design. In areas without a special care dentistry MCN, local expert working groups with special care dentistry and restorative dentistry clinical leadership and representatives from GDS and CDS should be put in place.
Key performance indicators (KPIs) are an integral part of the service specification. They should be co-developed with patient and health and social care representatives to ensure the care pathway operates as intended for vulnerable older patients and their carers, and an iterative quality improvement approach is taken.
In all ICS commissioned services, a uniform approach to data collection of the complexity of care delivered within services and the socio-demographics of patients accessing care is recommended. Not only for quality assurance, but also to inform ongoing improvements across services with a view to future standardised models of care.
Publication reference: PRN00783