We've put some small files called cookies on your device to make our site work.
We'd also like to use analytics cookies. These send information about how our site is used to a service called Google Analytics. We use this information to improve our site.
Let us know if this is OK. We'll use a cookie to save your choice. You can read more about our cookies before you choose.
Maternity patient experience survey 2025: national qualitative report
1. Introduction and methodology
The NHS Patient Survey Programme is delivered by the Care Quality Commission (CQC) on behalf of NHS England and the Department of Health and Social Care. The Survey Coordination Centre at Picker, coordinates the NHS Patient Survey Programme on behalf of CQC. There are five surveys within the Programme: Adult Inpatient, Maternity, Children and Young People, Community Mental Health and Urgent and Emergency Care Surveys.
This report has been produced by Solutions Strategy Research Facilitation Ltd (Solutions Research) and NHS England to share national insights from qualitative thematic analysis of written responses provided by patients that took park in the NHS Patient Survey Programme. The aim of this endeavour is to identify opportunities for learning and improvement through an in-depth understanding of experiences of care.
The focus of this report is on the 2025 NHS Maternity survey, which gathers feedback from patients about their experiences of care provided before giving birth (antenatal care), during labour and delivery, and up to 8 weeks following birth (postnatal care).
Further information on the survey is available on the CQC website.
Qualitative data analysis
One open question was included in the survey which allowed patients to use their own words to respond. This question was positioned at the end of the survey and included the instructions as follows:
‘If there is anything else you would like to tell us about your maternity care, please do so here.’
To ensure a robust approach a purposive sampling method was used for qualitative analysis:
675 comments were analysed as a sample from 9,545 viable comments.
Once the sample of 675 comments had been analysed it was seen that data saturation had been reached i.e. no new themes were emerging from the data. Had this not been achieved, additional comments would have been added to the sample as necessary, in line with best practice in qualitative analysis.
Throughout the report, quotes are included to illustrate patients’ experiences in their own words and substantiate the findings. Please note that except for the partial censoring of profanities and very specific details of medical history, the data is not edited in the interests of correct spelling and punctuation, to stay as true to the words of patients as possible.
Certain information from the qualitative comments used in the report has been redacted to protect the identity of survey patients and any other individuals referenced. Information that has been removed includes:
names of patients or staff replaced with “[name]”
names of wards, units or hospitals replaced with “[location name]”
names of specific services replaced with “[service name]”
specific dates replaced with “[date]”
There is a degree of duplication in the use of quotes in this report to substantiate insights. This reflects that written feedback is often complex in that it is rich in detail and spans several parts of patients’ care journey, providing a depth of insight as to several themes and/or sub-themes.
Use of quantitative data
Where possible in the findings section, themes are presented in context of the most relevant quantitative survey data. This allows for insights to be considered more holistically and to provide a greater opportunity for reflection and learning. There is a degree of duplication in the use of statistics in this report.
Context to support interpretation
Many responses to the open questions were very detailed and complex. This contributes to the length of the report and extensive thematic framework, as well as the duplication of quotes.
While detailed responses provided opportunity for insight, asking patients to reflect on their experience across their entire maternity journey could create long and complicated feedback. Further, as outlined below it is of most use where the findings can be aligned with stages of the maternity care pathway but this was not always stated or obvious.
To support interpretation and use of the insight, the findings, where possible, have been structured to signal which stage of the maternity care pathway the feedback speaks to. There are seven sections: overarching themes; prior to labour; early labour; labour and delivery; soon after delivery; discharge; and follow-up care.
Feedback that cannot be attributed to a specific stage, either explicitly or through context, is presented under ‘Overarching themes.’ The ‘Overarching themes’ also includes feedback relevant across multiple stages of the pathway to avoid duplication across sections.
While this structure allows for navigation to specific parts of the pathway which may be of particular interest to readers, we recommend reading the entirety of the results chapter given the complexity of experience and how interwoven we observed many of the key themes and sub-themes to be. Keep in mind that the feedback often describes several stages and aspects of care within a single response and themes and sub-themes are not mutually exclusive but often overlapping and interconnected. Indeed, this qualitative dataset is best described as both rich and complex.
2. Headline findings
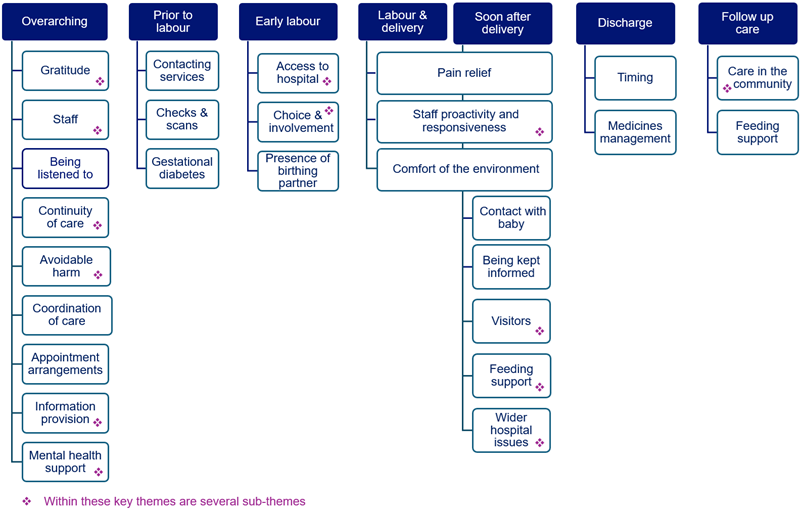
This diagram summarises the key themes and sub-themes identified across the maternity care pathway, from before labour through to follow-up care.
The themes are grouped by stage of care:
Overarching themes apply across all stages and include gratitude, staff, being listened to, continuity of care, avoidable harm, coordination of care, appointment arrangements, information provision, and mental health support. Several of these themes include multiple sub-themes.
Prior to labour, key themes include contacting services, checks and scans, and gestational diabetes.
Early labour themes focus on access to hospital, choice and involvement, and the presence of a birthing partner.
During labour and delivery, themes include pain relief, staff proactivity and responsiveness, and comfort of the environment.
Soon after delivery, themes include contact with the baby, being kept informed, visitors, feeding support, and wider hospital issues. Some of these themes include multiple sub-themes.
Discharge themes cover the timing of discharge and medicines management.
Follow-up care focuses on care in the community and feeding support.
The diagram also highlights that several of the key themes contain multiple sub-themes.
3. Thematic analysis findings
3.1 Key themes
There were 30 key themes identified from the thematic analysis. Within 13 of these key themes are sub-themes totalling 36 overall, which support interpretation and use of the insights. Key themes which include sub-themes are noted in the list below, e.g. *2 means there are two sub-themes within the key theme. Note the unique reference to each key theme and sub-theme is shared in the list to support with navigating the findings.
3.2 Overarching themes 3.2.1 Gratitude *3 3.2.2 Staff *4 3.2.3 Being listened to 3.2.4 Continuity of care *2 3.2.5 Avoidable harm *5 3.2.6 Coordination of care 3.2.7 Appointment arrangements 3.2.8 Information provision *6 3.2.9 Mental health support *3
3.3 Prior to labour 3.3.1 Contacting services 3.3.2 Checks and scans 3.3.3 Gestational diabetes
3.4 Early labour 3.4.1 Access to hospital *2 3.4.2 Choice and involvement *2 3.4.3 Presence of birthing partner
3.5 Labour and delivery 3.5.1 Pain relief 3.5.2 Staff proactivity and responsiveness *1 3.5.3 Comfort of the environment
3.6 Soon after delivery 3.6.1 Pain relief 3.6.2 Staff proactivity and responsiveness 3.6.3 Comfort of the environment 3.6.4 Contact with baby 3.6.5 Being kept informed 3.6.6 Visitors *2 3.6.7 Feeding support *2 3.6.8 Wider hospital issues *2
3.8 Follow up care and support 3.8.1 Care in the community *2 3.8.2 Feeding support
3.9 Other observations
This section of the report contains the detail of each theme with a range of quotations shared to substantiate and exemplify the experience of patients using their own words.
3.2 Overarching themes
This section includes findings which have relevance either across the maternity pathway or are not easily attributable to specific parts of the pathway.
3.2.1 Gratitude
A prevalent finding in the feedback overall was gratitude, most often thanks were for the maternity care received broadly though some comments related to a specific element of the pathway.
General
These comments tended to be brief and typically described the care as ‘great’ or ‘amazing’. Most of the comments were not specific to a part of the pathway.
“Thank you for great care that you are provided to me. I really appreciated.”
“Five stars thank you.”
“Everything is 10/10 , thank you so much for everything:)”
“I am very happy and thank you very much.”
“I had an amazing experience at [location name] Hospital with both my planned c-sections for both babies. Couldn’t fault anything!”
“I have anything else to say, but I must say, I’m happy to experience every thing during my pregnancy and labour.”
“I was very happy with the service I receive from all the NHS staff.”
Staff
Often feedback expressing appreciation referenced specific teams or individual members of staff, highlighting how the staff influenced their positive experience. Expressions of gratitude about staff links to the ‘Staff manner, attitudes and attributes’ sub-theme later in this report, though comments were less detailed about specific qualities that drove positive interactions.
“I had a great pregnancy and birth experience with the midwives. Thank you to all of the midwives who involved me and my baby’s care.”
“I would like to thank the entire health care team and the NHS.”
“Each of those ladies is an absolute angel. They helped my baby to breathe in his most vulnerable first moments. I could cry when I think of what they’ve done for our family! Thank you will never be enough!”
“My experience at [location name] was magical and I will remember every single midwife involved in our care, they clearly have passion and love their job and I would feel very comfortable being treated by the same team in the future. Thank-you everyone.”
“I appreciated the care given by the [location name] team.”
“The care i received during birth and antenatal was absolutely outstanding. each person treated you with such compassion , i would have expected the same treatment if paying privately.”
Specific
A few patients specified their comment related to the antenatal care they received, reporting ‘good’ care from staff but without further details.
“Antenatal care (at triage) was good, always seen and looked after.”
“Antenatal care – Overall recieved good care from all midwives I met, however it was a mix of different midwives every time.”
“I was under [location name] for my care initially, antenatal appointments were brilliant, I cannot put into words how amazing they were. I cant thank them enough.”
Other expressions of gratitude explicitly related to care during early labour and/or labour and delivery. Typically, these comments highlighted positive experiences with staff who were described as ‘amazing’ or ‘fantastic’ with some patients reporting that staff had exceeded their expectations.
“The level of care was outstanding. Three individuals that stood out for me on [location name] were [Name], [Name] and [Name]. [Name] treated me when I first arrived and was kind and patient even though she was busy. [Name] was a trainee but she must have had more experience or worked in midwifery before as her bedside manner was impeccable… I’m so grateful.”
“I was really happy with choosing this hospital again. Everything was perfect. Great and so kind staff, doctors, midwives, nurses, all were helpful and super caring. I wouldn’t change anything. Thank you for bringing my son to the world in such a great atmosphere.”
“I cannot fault the care I received at [location name], especially during labour + birth. All midwives I dealt with were amazing + very supportive [name, name, name + name]. I can’t thank them enough for making what was a nervous first time experience into a safe and calm one.”
“I wish my partner could have stayed overnight during my induction as it was quite frightening when my waters broke but the midwives were fantastic and called my partner back in when I wasn’t in a position to.”
“I must highlight that the care I received by the midwives at [location name] Hospital was outstanding. The 2 midwives assigned to me communicated with me throughout, were very knowledgeable and helped me to remain calm during a fast active labour. They worked intuitively with my circumstances and followed my lead during the birth. I have praised them to everyone I have spoken to about my birth.”
Experiences with neonatal care were also singled out for gratitude by patients. Appreciation for the support patients received were made, with references to the comfort and reassurance given by staff.
“Our baby had to go to NICU when he was 8 hours old and I was so upset. The midwife I had was brilliant at helping me get up for the first time and brought down to NICU. The nurse we had in NICU was amazing.”
“We are eternally grateful for helping us so well during pregnancy and labour and delivery and especially for the fantastic support we received in NICU. Thank you to the wonderful NICU psychologist, nurses, midwives, doctors, feeding consultant, and all the people in the background who make the hospital run around and offer such incredible support to people when they really need it.”
“[Name] was a trainee but she must have had more experience or worked in midwifery before as her bedside manner was impeccable. When I found out my son had to go to SCBU, she fed him and comforted me. All these women stood out to me as exceptional. [Name] was fantastic and the other doctors ([Name], [Name]. [Name], Name), [Name]) provided amazing care. In SCBU, the nurses who took care of my son were phenomenal (Name], [Name]. [Name], Name), [Name], [Name]). These ladies made a hugely positive impact on me and taught me so much about feeding. I’m so grateful.”
“We are so lucky. In particular, I owe everything to the incredible ladies in SCBU [location name] for looking after my baby boy [Name] in the first week of his life.”
3.2.2 Staff
What does the quantitative data tell us?
88% said they were ‘always’ treated with dignity and respect during antenatal care (b14)
83% said they were ‘always’ treated with kindness and compassion during labour and birth (c21)
84% said ‘all of the staff’ introduced themselves during labour and birth (c10)
Of those who stayed in hospital after the birth or required hospital care after a home birth, 73% said they were ‘always’ treated with kindness and understanding in hospital (d5)
Staff were demonstrated to play a very critical role in how patients experienced maternity care across the entire pathway.
Staff manner, attributes and attitudes
Staff communication and attitudes were key to how many patients experienced their maternity care. There was wide variation in how patients described individuals or groups of staff, including comments which shared both positive and negative examples from across their maternity journey.
Key words used to describe staff shown below demonstrate how polarised experiences could be:
Positive descriptions of staff
kind
caring
approachable
friendly
professional
supportive
considerate
informative
helpful
knowledgeable
Negative descriptions of staff
dismissive
cold
patronising
uncaring
unsympathetic
condescending
rude
abrupt
pushy
Within positive feedback, patients highlighted personal and professional staff attributes that they appreciated. This was noted across all stages of care and, when specific roles were mentioned, included midwives, doctors, consultants, and other healthcare professionals. When patients felt staff demonstrated the positive attributes highlighted in the diagram above, where detail was shared this had made them feel comfortable, relaxed and calm.
“I had such a positive pregnancy, labour and birth thanks to the [location name] team of midwives. [name] in particular was incredibly supportive.”
“My (antenatal) midwife was very approachable and I felt comfortable discussing my wishes with her.”
“I was looked after by [name] as my community midwife and [name] who delivered my baby. Could not speak highly enough about them both. Amazing midwives. All the nhs staff who worked with me they were kind, considerate, informative and really helped me as further complications arose towards the end of my pregnancy.”
“My experience at [location name] was magical and I will remember every single midwife involved in our care, they clearly have passion and love their job and I would feel very comfortable being treated by the same team in the future.”
“I’m so grateful for the care I received while I was hospitalised for 5 days from midwives and doctors who did my cesarean. All your dedication to my health has been truly inspiring, and I always feel like I was in good hands with you all.”
“I had a short and straight forward labour, but I must highlight that the care I received by the midwives at [location name] Hospital was outstanding. The 2 midwives assigned to me communicated with me throughout, were very knowledgeable and helped me to remain calm during a fast active labour. They worked intuitively with my circumstances and followed my lead during the birth. I have praised them to everyone I have spoken to about my birth.”
“My midwife (community) [name] was amazing, very supportive & caring. The team in the antenatal assessment unit were patient & couldn’t do enough for us. My C-section team midwife [name], anesthetist [name] & surgeon [name] were incredible, very professional, caring, made me feel at ease & comfortable. I couldn’t have asked for a better team.”
“I felt extremely supported during my whole pregnancy by my midwife. My birthing team were beyond helpful and kind. I felt so at ease and supported. I had an experienced midwife and a training midwife team (x2 as it was shift change time) they were very professional, very kind and made the whole experience seamless and as relaxing as birth can be. I honestly couldn’t praise them enough.”
“While I was in labour the student midwife I had called [name] was amazing, she did everything in her power to make sure I was comfortable & knew what was happening.”
“During my inductions all of the midwives were kind and compassionate and the team who carried out my c section were also very kind and made me feel safe during and after the procedure.”
“The midwives after the birth looked after me and my baby so well. I can’t thank them enough, they gave me confidence in my mothering skills, helped with breastfeeding and supported me with pain so that I could concentrate on learning to be a mother.”
In contrast, comments which described negative staff manner shared the emotional distress that this created for them. Negative experiences spanned all stages of care and were seen across a range of roles including doctors, midwives, and other healthcare professionals.
“At one point in the postnatal ward, I felt really upset by a staff member’s behaviour. I felt that she was being rude and didn’t consider how I was feeling. As a patient, she could have treated me with more kindness.”
“One negative experience at hospital clinic where the doctor was rude, unhelpful and extremely abrupt. Made a complaint about this and did not see him again however remain worried about this doctor, who was a locum, seeing other families as his attitude was appalling.”
“The lady that came in to tell us we was being transferred to the ward was very abrupt and stand off!”
“I had to ask a care assistant to help me put my baby in the cot and she was very rude to me and told me my partner couldn’t be here he need to leave now… She was not supportive, aggressive in her tone, patronising and unhelpful. She made me feel extremely anxious and like I was failing!”
“There was a head midwife in which didn’t seem to listen to my partner over a concern we had, when I wasn’t able to speak. She seemed very rude towards him.”
“As it was my first child I had relied on the midwives to help me, most (not all) were cold, and not interested in taking care nor listening to me.”
“I had midwives have a go at me whilst I was in active labour and in a lot of pain.”
“I was treated awfully by one doctor in particular and was in a lot of pain and all she seemed to care for was the health of my baby. I was made to feel like I did not matter.”
“During pregnancy I did speak to a diabetic nurse called [name] based at [location name] hospital. I found her to be quite condescending, and even laughed when I asked questions.”
Staff availability and capacity
What does the quantitative data tell us?
74% stated they were ‘always’ given the help they needed if they contacted their midwifery team during pregnancy (b9)
66% stated they were ‘always’ able to get a member of staff when needed during labour and birth (c13)
57% stated they were ‘always’ able to get a member of staff when needed when in the hospital after the birth (d3)
75% stated they were ‘always’ given the help needed if they contacted a midwife / midwifery team after leaving hospital (g2)
Staff capacity and a lack of availability was an overarching theme that appeared in feedback across the maternity pathway. Observations often included acknowledgement that staff were doing their best in the circumstances, noting the issues to be systemic and could highlight the negative impact this could have on staff.
While not always stated, the comments included several areas where patients held the belief that insufficient staff contributed to their poor experience, including:
waits for induction and transfer to labour and delivery areas
waits for assessment / triage
delays to postnatal midwife visit
not being able to give birth at a preferred location, including home births
“Spent 3 days in hospital waiting for induction after my waters broke to start contractions however due to lack of staff I was unable to go to the delivery suite for this to happen. I then ended up classed as an emergency c section which took 3 days before being able to have this done. Midwife’s and delivery team amazing but lack of staff is disgusting.”
“The midwife who first came to visit us, came a day later due to the service being overstretched. There was also no advance warning and she just showed up.”
“The planned home birth didn’t go ahead due team unavailable once on established labour. The Trust still not providing enough staff for the home birth service.”
“There’s only 1 women that does tongue ties in [location name] and she was on holiday so I was unable rectify it for 2 weeks. The procedure is quick, why can’t these be done in the ward on the day or within a few days of birth to avoid the stress I endured later down the line? More people should be trained to do it.”
“The only negative I have is waiting for a hospital bed due to lack of staff and not being assessed regularly during labor again due to staff shortages but over all the midwives did all they could to ensure I was comfortable and did a fantastic job with such staff shortages, they were absolutely fantastic!”
Feedback included observations from patients that staff were under pressure due to there not being enough of them, while some patients reported staff commenting to them about workforce shortages. This could result in patients not getting timely assistance or feeling unsafe.
“The midwives were rushed off their feet and with no doctors to carry out assessments it was just mayhem. It felt like the hospital was being let down by the fact that the doctors were spread so thin across multiple departments and heavily pregnant and worried women in triage were just left to sit on uncomfortable chairs for an unknown period of time.”
“It is clear to see that women are not able to be adequately cared for in a system which is so stretched. Pregnancy needs to be respected as a big event in a woman’s life, continuity of care is essential but lacking.”
“The department was exceptionally short of beds during 1st week of Feb so this made my inpatient induction more drawn out due to lack of doctors to examine me and emergencies understandably taking priority.”
“I felt that despite challenging circumstances, they were all trying to do their very best and keep to professional standards. However, it was clear a lack of resources meant it was difficult for staff to do their jobs properly.”
“Some midwifery staff/nurses were absolutely fantastic however some were extremely rude and very dismissive of pain and I kept getting comments about how they’re short staff.”
“You could tell the hospital was short staffed on the wards but all the midwives and team did all they could.”
“The shortage of staff in triage at the time was concerning the midwife or health assistance I saw was rushing because she was on her own. This is how mistakes happen.”
Privacy and dignity
There was mixed feedback from a small number of patients regarding their privacy and dignity. Some patients felt their privacy and dignity had not been maintained while they were in hospital due to being in shared spaces. Other patients shared positive experiences of their privacy being upheld by staff who handled their information with ‘discretion’.
“During my labour, a midwife called [Name], wasn’t very sympathetic when I expressed my concerns of being in labour. I had to ask several times to have a bit of privacy as I felt I was in labour. Finally she gave me a side room but I was told there was absolutely no reason for me to be in that room.”
“Facilities at [location name] for post natal not fit for purpose, small bays and lack of privacy in shared bays.”
“I work for the NHS so I am acutely aware of the national pressures on bedspaces, however the lack of space and privacy truly did impact the dignity of myself and other new parents.”
“felt genuinely cared for throughout my time on the maternity ward. The staff were respectful, attentive, and ensured my privacy and dignity were maintained at all times. I appreciate the way sensitive information was handled with professionalism and discretion. It gave me confidence that both my personal and medical details were treated with the highest level of confidentiality.”
Discrimination
A few patients reported discrimination relating to ethnicity, age or sexuality. Patients described feeling that their treatment was inferior or that health concerns had not been picked up due to not being listened to by staff, echoing the insights in the sub-theme ‘Being listened to’ explored later in this report.
Regarding ethnicity, some patients questioned whether their negative experiences of staff manner and attitude could be due to racism while others felt it was clearly the case.
“I had multiple visits to the maternity unit after birth as I has pain and discomfort and raised blood pressure. My last time there was were there (plus my husband and baby) for 6 hours with no one helping until my white husband complained, saying we can see why black women have such awful outcomes through pregnancy and birth and said he was taking us home despite no help. That incident led to a scan being requested which identified a large haematoma for which I was not given any pain medication or assistance.”
“All of the staff were very friendly and helping except one midwife or healthcare that was on night duty. She was being racist and not looking on us, didn’t provide us any information on feeding. It was our first nights with the baby, my husband stayed on a very sturdy chair whole night, although I could see other parents and babies were getting more care and attention when we were left out there.”
“I have myself been mistreated and while waiting seen a huge number of patients being mistreated especially when english is not there first language. In average 3/5 midwives on shift displayed these behaviours, this is based on numerous visits not just one. You also have an elderly Caucasian gynacologist displaying racist characteristics. I was unable to get her name, however she treated me this last time of using triage, reviewed my reason for being at triage and did not even allow me to talk or tell her why I was there and in her 2nd sentence said it’s anxiety it’s your 1st baby. I said to her about 3 words before she cut me off talking and told me it was anxiety. I am a professional myself working in the medical field and never spoken to my patients in this manner, she did not even ask why I was there. Same thing for the next patient!”
“I feel like Asian people are looked after and treated differently by certain staff.”
Age discrimination was highlighted by patients in the youngest age groups. These patients wondered if negative experiences with staff were due to their age.
“During pushing i said to one of the midwifes i could not push anymore and my baby’s heartrate was dropping, she said things such as ‘its called labour for a reason’ ‘you need to push because her heartrate is dropping’ Making me feel like i was failing my baby and she did not take me seriously, presumably because i am young. I demanded a c-section which they didnt want to do at first but eventually a doctor came in and checked me, i have a curve in my spine which must have led to a lack of curve in my pelvis, my baby was stuck like i said. My epidural failed so i was in agony, i was screaming not being able to do anything about it as i couldnt push, i was taken in for a cat.1 c-section but they ended up using forceps instead as my baby was low enough. I could have lost my baby due to not being taken seriously at my most vulnerable.”
“I felt and believe that the [location name] maternity hospital staff where neglectful in a sense due to I only saw them maybe twice every 13 hours the only staff member I actually thought was amazing and was good at her job and that wasn’t rude was a student midwife named [name]. A male doctor examined me vaginally which I stated at the beginning of me going into hospital that as I was a 17 year old female I didn’t want a male doctor to examine me. I was spoken to with judgment and rudely which I believe was due to my age. I had asked for pain relief multiple times and was forgotten about every time. They took over 12 hours to put me on the hormone drip which at that point I had been in labour for at least 48 hours. My baby had a permanent scar on his forehead from where one of the nurses had roughly without care nor trying to be gentle had tried but failed to break my forewaters. My overall care was not up to a standard that it should have been.”
“No one was listening to me or taking me serious because they didn’t believe I was in labour like I did.”
An example of discrimination based on sexuality was also found in feedback, with several occasions shared where assumptions were vocalised by staff despite being in the patients notes.
“Follow up visits at home we had 2 negative experiences. Firstly a midwife support worker assumed my partner (female) was baby’s grandma. This is offensive to my partner and showed that she had not had even a cursory look at the notes before entering my home. She did not introduce herself and just said “is it through here”, which was very rude again as new parents care could have been much better. Another midwife also made the same assumption. Please look at the notes.”
3.2.3 Being listened to
What does the quantitative data tell us?
84% said their midwives ‘always’ listened to them during antenatal check-ups (b6)
88% said that if they raised a concern during antenatal care, they felt it was taken seriously (b15)
82% said if they raised a concern during labour and birth, they felt that it was taken seriously (c12)
78% who attended triage face-to-face said the midwife or doctor ‘definitely’ listened to them (f3)
77% who saw or spoke to a midwife after the birth said the midwife or midwifery team that they saw or spoke to ‘always’ listened to them (g6)
Being listened to and feeling heard stretched across all points in the maternity pathway and was a prevalent theme in the data. While predominantly negative feedback, positive experiences were also shared that further demonstrated how valued being listened to is to patients. The findings in this report identify multiple areas where it was suggested that not being listened to had contributed to poor experiences, these included:
antenatal concerns were dismissed/ignored, impacting health of mum and/or baby
staff making poor triage decisions, and admission to hospital to give birth not happening early enough
lack of checks by staff around how labour was progressing
not receiving timely pain relief
postnatal concerns were dismissed/ignored, impacting health of mum and/or baby
requests for delayed cord clamping not adhered to
In cases where concerns had been raised antenatally or postnatally, patients often felt that they hadn’t been sufficiently listened to, staff had been dismissive, and that their concerns should have been given more attention which could have impacted on outcomes and/or resulted in treatment or action being taken sooner. There were patterns observed regarding pre-eclampsia in pregnancy and jaundice or tongue tie in babies following delivery.
“My debilitating nausea during pregnancy was not taken seriously by my GP, and was refused medication other than one that I already knew didn’t work. I was told any other medication would be too risky for my pregnancy, but I know that many other women are given help via medication.”
“During my antenatal care, I had to be persistent with my midwife to get her to do swab tests to investigate my concerns. I sometimes felt like this was an administrative burden to her at my appointments.”
“Every time l went to my scans it felt like they were always negative about my baby’s growth and l tried to explain it so many times that l carry small babies, but they wouldn’t listen.”
“Diagnosed with pre-eclampsia after raising numerous concerns. Returned to the hospital to then be told by a different doctor he didn’t agree with this diagnosis and it wasn’t pre-eclampsia. I returned for daily monitoring the following day to be told again it was pre-eclampsia, medication was required.”
“I feel I was not taken seriously when calling triage in early labour, most likely due to being first pregnancy, which led to an emergency home birth.”
“When I went to hospital in labour, I didn’t feel they believed me with ‘how much’ labour I was in. They wrote on the screen not in active labour before examining me and when they (eventually) examined me, I was 5 cm and hadn’t had any pain relief. (they then believed me and gave me pain relief).”
“Dismissed our concerns about baby jaundice and then looked at her again 10mins later and told us to go straight to a+e (we did, and she was jaundiced)!”
“My son had a tongue tie which wasn’t picked up on until his day 5 check. I thought he had during our stay in hospital but only one member of staff in the ward could diagnose it and because I was desperate to leave the hospital the day we got discharged I didn’t have time to get it checked.”
“My only gripe would be that my baby wasn’t picked up for having a tongue tie – this was noticed on day 3 after feeding problems. By that point, my baby had lost weight and blood sugars were low, so we ended up bottle feeding. I think this should be checked in hospital and follow up care given. I feel this greatly contributed to me not being able to successfully breast feed.”
“My wish to not have cord clamped even after ‘2mins’ was not communicated to theatre team during my emergency C-section, I forgot to mention it and the theatre team never asked, it should be included in the surgical checklist in theatre before starting procedure.”
“I also asked for delayed cord clamping and was only clamped for 1 minute.”
Positive feedback relating to being listened to was given by those who had experienced a home birth, along with patients who delivered in hospital and felt that their choices had been both heard and respected. While positive comments were made by a few patients, these were noteworthy exceptions against the backdrop of mainly negative experiences shared.
“The home birth midwife team were absolutely outstanding and made it a special and empowering experience. I felt completely trusted and respected to make safe informed decisions. I am very grateful for the quality of care I received.”
“The care we received at [location name] was exceptional… We felt safe, heard and respected.”
“My community midwife was amazing throughout and listened to my concerns and made me feel heard. The labour midwives who were on shift whilst I gave birth were just as amazing, they listened to my wishes of a water birth and followed through with this immediately. They respected my space and offered support when needed.”
“Huge thank you to the [location name] team. Their care, work ethic and consideration for my birth choices enabled me to have a very positive birth experience. We chose a ‘hands off’ approach, where I birthed my daughter myself in the pool at home.”
“I was a surrogate and gave birth to a little X on [date], after a planned induction. The care we received from start to finish was faultless. I was always treated as the pregnant person and my friends were always treated as the parents, as I requested. Our midwife care was fantastic throughout the pregnancy. The birth experience was amazing and the [location name] were incredibly accommodating of the extra people in the room. The midwives even thanked us for letting them be part of it. Post birth, baby had to be observed for 12hrs. They took parents and baby up to the ward and I was discharged straight from the delivery room. This allowed me to get home to rest and them to be respected as his parents from the very beginning. Thank you to everyone involved.”
3.2.4 Continuity of care
What does the quantitative data tell us?
25% said they saw or spoke to the same midwife ‘all of the time’ at antenatal check-ups (b3)
17% who saw or spoke to a midwife after the birth said they saw or spoke to the same midwife ‘all of the time’ at their postnatal check-ups (g3)
13% said midwives who had cared for them postnatally had also been involved in their labour and antenatal care (g9)
There was a strong theme found across the maternity pathway that patients would like continuity of care in terms of seeing the same midwife or consultant consistently. For clarity, most patients wanted consistency within each stage of the pathway, i.e. having the same person provide all of their care antenatally, accepting then a different person would provide their care for labour and delivery though importantly this person would be consistent throughout this part of the journey, and so on. There was variation across individual experiences as to whether this had been the case or not.
Midwifery
While patients who received care from multiple midwives during a stage of their care often praised individual midwives, they also described how the lack of consistency had led or could lead to care feeling disorganised and even withholding questions or concerns. In some cases, it also meant that differing advice had been received.
“I saw 17 different midwives in the 40 hours I was in hospital across the assessment unit, induction ward, labour ward and postnatal care. 13 of those were during my labour which was only 2 hours long and this was very unsettling in an already difficult time.”
“My midwifery team was very good but I did request to see the same midwife and I did not get a lot of appointments with her and even booked my appointments with her to ensure I seen my named midwife but on the day find out she was not there for unknown reasons.”
“During this recent pregnancy I never saw the same midwife more than once and this was difficult because I felt like I was having to repeat myself all of the time.”
“All of the midwives I came across (antenatal, triage, delivery, postnatal) were very helpful and friendly I would have preferred the same midwife throughout antenatal and postnatal care.”
“I was seen by many different people during my antenatal and postnatal check-ups. My assigned midwife didn’t see me once postnatally and antenatally always seemed to be on leave.”
“My husband who saw how much I suffered to he made midwives to take me to labour ward and only then they checked on the baby and realized I won’t be about to deliver the baby without getting specialist help. All im saying all suffering I went through could be avoided if I would be taken care of as I should and if I would have one midwife not 10 of them.”
“I was also lucky enough to have a pleasant pregnancy without any issues and each antenatal appointment was informative. However, I did not see the same midwife throughout my pregnancy, it didn’t bother me, although there wasn’t any consistency in the information and results being published in badger notes.”
“While I appreciate the effort of all staff and the quality of care provided, I’d have loved to have at least 2 or 3 antenatal sessions with the same midwife. Going every day and seeing different faces makes me not (at most of the times) have that freedom to express myself to the fullest, in terms of how I was feeling, which I would say made me keep lot of things to myself and figured them out myself.”
Patients who had experienced care from a consistent midwife described this very positively, focussing on the benefits of relational continuity whereby they felt they had a more personal and meaningful relationship which then facilitated individualised care.
“I have had 2 babies with the trust now, the first a hospital unassisted vaginal and the second a home water birth. Both times the staff have been amazing and I’ve had really great experiences. However the second time I had continuity of care with the same midwife and that made such a difference! When she called to say she was in her way when I went into labour at home, I felt so relived and at ease.”
“My midwife [name] at [location name] centre was amazing throughout my pregnancy, I’m very grateful I was able to see the same midwife throughout my pregnancy, she gave my all the information I needed, I was never left with any questions, she was kind and really put me at ease.”
Consultants
A similar pattern was seen in feedback around continuity of care where patients were on a consultant-led antenatal pathway, or where paediatricians were involved after delivery. Patients described how the lack of consistency had led to them having to repeatedly explain their situation and, for some, differing advice had been received which created anxiety or was seen as the cause of delayed diagnosis.
“At first the scan and consultant team didn’t know my history, I had to tell them. But once they knew it was a fairly good continued conversation and care. I barely saw the same consultant twice but they were all good.”
“i would have liked to have seen the same medical professionals for appointments instead of someone different every time. but i can understand the service is very busy and that isn’t always practical.”
“During pregnancy, I was under consultant-led care with weekly scans nearing the end due to issues with slow growth, but saw a different consultant each time, all with slightly different views on way forward. This lack of consistency was stressful.”
“I generally had a great experience but I found as I was under consultant led care the midwife appointments became pointless and I was passed around the consultants.”
“The care from the paediatricians following birth was difficult as each change of shift brought a different perspective and treatment plan so there was no consistency and jaundice was missed.”
3.2.5 Avoidable harm
There is a range of examples in which patients described harm they believed to have been avoidable, which had resulted in health complications for them and/or their newborn(s) across the maternity pathway. Where possible from the feedback shared, the causes and reasons that patients believed contributed to these events have been highlighted within sub-themes. This includes links to issues discussed earlier in the ‘Staff’ sub-theme of staff capacity and availability, as well as broader aspects of the working culture.
Prior to delivery
Patients highlighted issues during pregnancy, particularly being misdiagnosed or diagnosis being missed. This included an example of a misdiagnosis of miscarriage in early pregnancy, notable for the impact this had on the patient and their assertion that this could have significant negative impacts if it happened to other patients.
“Not sure if this applies to maternity care, as this was prior to speaking to a midwife. But at around 5 weeks pregnant I started bleeding, 111 sent me to A&E which I was then sent to SDEC gynaecology, I was examined by a male doctor who told me I had miscarried, told me to retest in 3 weeks to ensure the test comes back negative. I was obviously very upset about this as I was sent home to just deal with a miscarriage, 2 hours after I got home the same doctor phoned me to tell me to come in the following day for a scan, it turned out I did not miscarry and was in fact still pregnant. I feel as though he should not be giving out a diagnosis unless 100% sure as this could have been very traumatic for someone else if they weren’t coping well in the first place.”
A common thread was observed where patients felt that opportunities had been missed before a diagnosis of pre-eclampsia was made and could question whether this had resulted in them being less informed.
“I had all pre-eclampsia symptoms except protein in the urine, so it was missed. My BP was measured against typical ranges rather than at the baseline from my booking appointment, so my hypertension was missed. I was not given advice about postnatal impacts of pre-eclampsia.”
“Diagnosed with pre-eclampsia after raising numerous concerns. Returned to the hospital to then be told by a different doctor he didn’t agree with this diagnosis and it wasn’t pre-eclampsia. I returned for daily monitoring the following day to be told again it was pre-eclampsia, medication was required.”
“Pre-eclampsia was not picked up during my pregnancy until I was 38 weeks, even though I had high blood pressure throughout that was always dismissed as white coat syndrome.”
Clinical care including procedures
Patients highlighted issues with the quality of clinical care and/or procedures that they had received and how this had led to health complications such as infections and ongoing pain. Please note that feedback typically is attributable to care soon after labour and delivery, though in some cases the experience in labour and delivery is what led to the complications/impact described once their baby was born. For example, stitching required after delivery may have been described as poor which led to infection, highlighting that improved stitching could have prevented this outcome. What is unclear is whether the need for stitching itself might have been avoidable, representing another potential means of preventing the harm experienced by patients.
The following areas were specifically mentioned:
lack of care when using cannulas, catheters, epidurals, injections or when taking blood
poor quality stitching following tears, episiotomy and caesarean sections
poor wound, scar or tear care following episiotomy and caesarean sections
retained placentas
“The junior surgeon who sliced through a large fibroid causing me to haemorrhage X.X litres of blood should not be able to operate until she has obtained further training. If it was not for the swift actions of the consultant, my baby and I could be dead.”
“I had emergency surgery X days post-portum due to retained placenta I contacted the hospital where I delivered to let them know of this oversight which caused significant emotional & physical distress but have not heard back.”
“I had to be readmitted for another three days due to infection and hematoma that was visible on my abdomen and missed by all doctors and midwives who checked my scar.”
“I had retained placenta in place for X weeks and had multiple infections during this time (one requiring hospitalisation for IV antibiotics), but did not receive an ultrasound until I insisted because I had passed a piece of placenta at X weeks and X days after the birth.”
“I contracted a serious infection X days post delivery which resulted in a large hole opening up on my stomach (seperate to my c-section scar). This led to re-admission to HDU for X days.”
“During the delivery, forceps were used, resulting in significant blood loss (almost X.X liters) due to the cuts made. My hemoglobin levels dropped dramatically from X to X and I became extremely unwell. To make matters worse, it was later discovered that Xcm of pregnancy tissue was left inside me.”
“When I give birth I had to have a few stitches and they lost a needle for X hours, they almost had to send me for a x-ray.”
“In labour my epidural didn’t work. It took me getting up and walking before staff believed me.”
“Anestesiologist took X attempts to put a spinal in before another doctor stepped in and did it first time, each attempt caused me pain and distress at what was already a stressful time having a c section – also his communication skills were horrific.”
“The midwifes who came to put the epidural had no idea how to put it because they kept putting the needle in and out and my back still hurts.”
Newborns
There were examples of health concerns for newborns being missed or minimised by staff, some of which resulted in the re-admission of the baby for treatment. Concerns were raised that babies were not getting the medical attention that was needed from staff following delivery, alongside patients feeling they were not being listened to. This echoes the insights shared earlier in the report within the ‘Being listened to’ sub-theme.
“Baby had sticky eyes, swab taken on day X check up, no results communicated with myself, I was told to continue cleaning them as probably blocked tear duct. Baby ended up in a&e with ?sepsis at X weeks old which was suspected spread if the infection from the eye. The swab came came positive for Moraxella. I feel this should have been actively raised as an abnormal result and communicated to me and feel there is a gap in follow up care becuase of this.”
“When I was getting discharged I mentioned baby not eating Xhrs after its first feed and was told “he just might not be hungry” Xhrs later I had to take baby to a+e because he still wasn’t eating n would throw up if I tried. He spent the next X days being treated with antibiotics on the children’s ward.”
“A couple of hours after I gave birth, I raised a concern about my baby looking yellow with the midwife, which she didn’t give me a satisfactory answer for and wasn’t acted upon until the night-shift midwife came on and she did her preliminary checks and confirmed that the neonatal doctors should have looked at my baby as he was quite yellow. Things moved fast after that and my baby had to be admitted in the Special Care Unit to receive phototherapy and antibiotics.”
“The [location name] midwifery team do not have the correct training when dealing with babies born with a cleft. Treating parents like they’re doing something wrong because they don’t have any idea of what they’re doing in this situation is very belittling. They need adequate training to suite all babies and families.”
Tongue-tie checks and treatment
In relation to babies’ health, there was a distinct theme in the data around the need for improved service provision regarding how tongue-tie was identified and treated. Across the feedback, there was a strong sense that more thorough checks were needed before discharge from hospital, as well as quicker referrals. Where tongue-tie was not picked up in a timely way this had impacted patients’ ability to breastfeed and led to babies not gaining weight.
“I feel that tongue ties should be sorted and cut before leaving the hospital as my appointment took 9 weeks. External referrals were unnecessary when such a quick procedure could have been done then and there.”
“There’s only 1 women that does tongue ties in [location name] and she was on holiday so I was unable rectify it for 2 weeks. The procedure is quick, why can’t these be done in the ward on the day or within a few days of birth to avoid the stress I endured later down the line? More people should be trained to do it.”
“My son had a tongue tie which wasn’t picked up on until his day 5 check. I thought he had during our stay in hospital but only one member of staff in the ward could diagnose it and because I was desperate to leave the hospital the day we got discharged I didn’t have time to get it checked.”
“My only gripe would be that my baby wasn’t picked up for having a tongue tie – this was noticed on day 3 after feeding problems. By that point, my baby had lost weight and blood sugars were low, so we ended up bottle feeding. I think this should be checked in hospital and follow up care given. I feel this greatly contributed to me not being able to successfully breast feed.”
“There was delay in seeing the lady who does the full assessment on baby which was done at home. Which caused delay in diagnosing my baby tongue tie.”
“My son also had a tongue tie which was 100% restricted and if this has been assessed sooner than day 3 this could have improved my breastfeeding journey. Also, the 6 week wait for tongue tie to be cut also impacted my breastfeeding journey.”
In some cases, patients reported that they had paid for private treatment because of the issues encountered.
“It wasn’t till after several visits one midwife suggested a tounge tie. No one not even in the hospital had discussed tongue tie with us. We later decided to investigate and have this done privately.”
“After birth, my baby wouldn’t breastfeed. A pediatrician mentioned a ‘mild’ tongue tie before discharge. I was discharged 24 hours post C-section without established feeding, he had only taken 1ml via syringe in 24hrs. His referral was rejected for tongue tie so I paid privately to have the tongue tie assessed and treated at 8 days old. It was actually 80% tied-one of the worst they’d seen. They also noted severe jaundice during this private appt, which midwives who visited had said they thought seemed ok. I requested a blood test for bilirubin at the birth centre; he was admitted for treatment on Childrens ward as his levels were over treatment line.”
“Tongue tie stopped him from being able to latch… I booked to get it done privately.”
“His referral was rejected for tongue tie so I paid privately to have the tongue tie assessed and treated at 8 days old.”
“My baby attended [location name] to address a tongue tie at 4 weeks but it was not completely divided so had to take my baby through this again privately.”
Inexperienced staff
Several patients felt that the healthcare staff, particularly midwives, did not have enough experience and this had contributed to sub-standard care. While this feedback could be very general, when specific tasks were mentioned, this was often related to stitching after delivery.
“Midwife’s in hospital were very young and inexperienced. Care received from these midwife’s was worrying.”
“I had forceps delivery and episiotomy – the registrar who did this was amazing but he didn’t know the female anatomy as he said I needed an injection in my clitoris but it wasn’t. The consultant even said that he doesn’t know the female anatomy!”
“I had a student midwife throughout my antenatal and postnatal care. I do think this affected my experience because she was a bit forgetful, took a long time to do things, was terrible at taking my blood and she was the only midwife I saw after my baby was born. Although she was very kind, I did not fully trust that she always knew what she was talking about.”
“When I was getting sewn up after birth, the midwife [name] from [location name] was not professional. She didn’t numb me properly. I was told if it was too painful she would stop, she didn’t.”
“I had to really fight to be checked for progress I felt I wasn’t being listened to I have done this 3 times previously and I know my body. Once finally checked and allowed to move I had the baby within 15 mins. When I was in pushing stage midwife left student alone. She panicked when head came out, calling my partner to pull the emergency cord – was distressing after what happened earlier.”
“My labour and birth was overseen by a student midwife (which isn’t a problem, I believe everyone needs the opportunity to get hands on experience). She at one point left the room whilst I was contracting/pushing. My wife had to leave me to call for help as the baby’s heart rate monitor started beeping. After my birth she stitched me up following a cut and a tear, she took so long (which isn’t a problem as I’d rather it was done properly and with care) but towards the end the numbing had wore off… I was still using gas and air at this point, and it was only when another midwife came in to offer tea and toast, who seen my painful expression, then told the student to use more numbing…. her response was ‘I only have 3 left to do’. Overall my experience is good, I just feel the student work should have been checked or overseen by someone more senior… I developed 2 hemetomas the next day and I’m unsure whether these could have been recognised or diagnosed at the stitching stage.”
3.2.6 Coordination of care
What does the quantitative data tell us?
53% said during their antenatal check-ups, their midwives or doctor ‘always’ appeared to be aware of their medical history (b4)
65% said during labour and birth, their midwives or doctor ‘always’ appeared to be aware of their medical history (c20)
77% who saw or spoke to a midwife after the birth said the midwife or midwifery team appeared to be aware of their and their babies’ medical history (g5)
Issues of coordination within and between services across the pathway were typically noticed by patients in the context of poor communication or information sharing across a wide range of scenarios, staff and services named. The impact of poor coordination of care was that treatment didn’t happen in a timely way; care felt disjointed and impersonal; and patients had to themselves play an active role to have their needs met. For some, the issues of coordination were exacerbated by care spanning different geographical areas.
“My diabetes doctor didn’t know my medical/pregnancy history when in appointments made me feel like a number.”
“I found antenatal appointments with the doctor to be very superficial. There wasn’t enough attention to my long-term health condition and a lack of coordination between the antenatal team and the specialist looking after my condition. As a result, I had to be rushed to the hospital for an emergency IV and had to stay overnight in the corridor waiting to complete treatment even though I’ve flagged it to the team well in advance.”
“It would be great to improve communication between doctors/midwifes. My baby needed hepatitis B vaccination in the first 24 hours and this was not communicated properly and it was delayed as there was a lot of confusion between the Teams in hospital.”
“Bad communication from junior paediatric staff and ultimately we self discharged (we are doctors) after 4 days because of several delays and poor communication (and knowing our baby was not unwell).”
“I received care during my pregnancy and labour in [location], but once discharged I received care from the [location] health visitor service. If we had received post natal care from the [location] team I believe it would have been smoother and I would have seen by the same team.”
As indicated in some of the quotes already shared within this sub-theme, there was a pattern in feedback of patients’ records being poor quality or being lost. There was frustration for patients when staff did not have access to accurate information which was felt to affect decisions about their and/or their babies’ care.
“She also input my ethnicity incorrectly resulting in an incorrect Down syndrome test result. Some of this incorrect information remained on my record through pregnancy resulting in my baby being offered tests he did not need.”
“My baby’s weight appears to have been incorrectly measured at birth. This caused knock on effects as by day 5 it appeared he had gained 5lbs. This resulted in concern around baby and kids of monitoring from midwives, making us feel overwhelmed.”
“During visits to the hospital, I was told they did not know how far I was during my pregnancy even though I had a 6 week and a 9 week scan. I was made to feel like I was going to be birthed early without a valid reason, other than the hospital losing record of my scans.”
“One of the nights, the night nurse wrote my sons information about the amount of milk that went in his feeding tube wrong so we were almost forced to stay another night even though my son was eating perfectly without throwing up.”
3.2.7 Appointment arrangements
Patients shared negative experiences around appointment arrangements which spanned antenatal and postnatal care and referenced a range of different healthcare professionals, e.g. midwives, consultants, nurses.
Common issues identified were:
appointments not happening
appointments being rushed
appointments not lasting long enough
appointments not being frequent enough
delays
missed appointments
difficulties booking appointments
a lack of expected contact from services
“The only poor experience I had was at my initial VBAC appointment – the appointment was one hour late (which was not an issue in itself I appreciate often these things are beyond anyone’s control) however my appointment still went ahead, it was rushed, impersonal and I did not feel I was fully listened to, or my thoughts, opinions and previous experiences were taken into consideration.”
“Throughout the pregnancy, had multiple last minute cancellations or changes to routine appointments from the same midwife. Not good for making me feel like my pregnancy was important.”
“Admin error meant c section & pre op were showing as booked on badgernotes, but when I attended, they had no record on their side. I appreciate things go wrong, and they organised a c section the next morning for me which was brilliant, but for approximately 2 hours, no one spoke to me to tell me this had occurred/ that they were trying to sort out a new date so think communication could have been better.”
“Delays with antenatal appointments should be identified and communicated on arrival. Some appointments were delayed by 1-2 hours.”
“A mistake was made about my due date and this meant that my appointments were booked for the wrong dates. It took a long time to get this cleared up, it caused me lots of issues as I was repeatedly told there were no appointments available.”
“I turned up for my booking appointment on a Saturday morning and the clinic was completely closed. I made an official complaint about this.”
“My midwifery team was very good but I did request to see the same midwife and I did not get a lot of appointments with her and even booked my appointments with her to ensure I seen my named midwife but on the day find out she was not there for unknown reasons, my named midwife also knew that I had this complaint.”
“When I was pregnant last time I seen a midwife was 30 weeks and 4 days pregnant and never seen a midwife after that till I was giving birth as I never got contact for anything.”
“I really struggled getting vaccines I needed in pregnancy. Apparently the midwives couldn’t do them at my appointments which meant additional appointments with nurses which were a pain. I imagine this would put a lot of people off.”
3.2.8 Information provision
Across the maternity pathway were multiple examples shared whereby patients felt ill prepared. In this feedback patients often inferred or explicitly noted a lack of information provision and/or confusing/contradictory information having been received. This spanned information to support with pregnancy; birth planning; preparation for induction; feeding decisions; how to care for a baby; and how to care for oneself after delivery, particularly after c-section or episiotomy.
Birth plans
A pattern was observed in feedback on information provision during pregnancy as to how staff presented information, particularly around delivery options, with patients feeling that they had not received all the information or perspectives that they could have. There are links to the earlier ‘Being listened to’ sub-theme with patients feeling that their opinions were not accounted for when providing information about choices. Some felt they had been pressured into decisions and shared a reduced sense of choice during labour and delivery as a result.
“I also felt I wasn’t given sufficient reasons for why they wanted my baby out by x time due to being IVF – genetics didn’t seem explanation enough.”
“Their rhetoric was fear-based in a bid to gain my consent for various interventions – this is not the definition of informed consent. When consultants use sentences such as ‘I absolutely will not let you birth this way’, and ‘the trauma of a birth that didn’t go as you expected is easier to get over than the trauma of a dead baby’.”
“I think conversations about c-sections were (understandably) very serious and outlined risks. We went through this process several times. However, I do think that this was (unfairly) not compared to vaginal birth, and the risks also associated therewith, particularly in relation to my condition (epilepsy).”
“I was lectured endlessly on gestational diabetes and threatened with statistics about still birth due to my age if I refused induction. The consultants were defensive and patronising in their discussions and had no time or interest in listening to my concerns or different strategies.”
“My experience of community midwife was also excellent. However, most of the antenatal doctors in both hospitals were extremely poor at communicating birth options, risks, and treating me with respect. When I asked questions to establish the evidence base for recommendations, I was treated like an emotional person who wasn’t capable of being rational. I was almost never provided with an evidence base for decisions. I was told by at least 3 doctors that if I didn’t go with their recommendation then my baby could die (exact words). No other risks were described, and no percentages of possible death could be provided. Phrases used by doctors included ‘we would not allow you to do that’, ‘that’s not allowed’ etc. which shows a very poor understanding of the rights of women during pregnancy and birth.”
“The only negative experiences I had during my maternity journey were with doctors at the hospital. One was during an antenatal phonecall where we were discussing induction and my gestational diabetes. I expressed that I didn’t want to be induced yet and that this was supported by the midwives and I understood the risks. The doctor in question said that if I didn’t induce, my baby could die, in those exact words. I found her very blunt, unsympathetic and felt she was overdramatising the risks involved with choosing not to induce in my particular circumstances.”
Types of birth
What does the quantitative data tell us?
42% said their labour was induced (c3)
of those who said they were induced, 76% said before they were induced, they were given appropriate information and advice on the risks associated with an induced labour (c4)
Within the context of labour and delivery, feedback highlighted gaps in information provision specifically around caesarean sections and induction. There were indications this information could/should be provided antenatally as well as just prior to labour and/or during labour and delivery.
Examples prior to or during c-sections were given where there was not enough information which led to patients feeling unsure of what was happening or would happen next.
“No one told me why I needed a CAT 1 section.”
“Due to several emergencies, I wasn’t seen until much later than expected. Whilst this couldn’t be avoided, it triggered my anxiety and there was very little information given to us to when I would be having the baby.”
“I was sent to birth suite and prepared for a c-section without being told what was going to happen, why it was happening by the triage staff or the birth suite staff. I had to figure that out by myself with no support as I was there alone and no one was communicating with me.”
“When taken into the theatre for the planned C-section the anaesthetist team were great and talked me and my husband through each stage but after that there was no communication with me or my husband to say they were about to cut me open, about to birth our child, it was like I was on a factory conveyor belt. I also had tubal ligation and there was no confirmation during or after that this had actually been done and was successful.”
Where patients shared examples of there being an issue with information provision, induction was a common area highlighted as needing improvement. Predominantly the examples were about a lack of information prior to induction starting which meant patients felt they had made an uninformed decision that they wouldn’t make again.
“Induction information was poor especially around the syntocin drip – feel this was terrible procedure and would never opt for this again.”
“The induction process was never fully explained both pre birth and even when I was admitted for an induction. Timescales need to be more explicitly explained, alongside more information about what happens or what to expect once induction has been initiated.”
“I was not informed fully about the induction process and that this would mean I would be stuck in bed unable to move.”
“I felt the induction process and risks could have been explained more fully.”
“The induction process should have been more clearly explained. I was given a leaflet but no one explained the process to me until the day of my induction.”
“I wish someone had explained in more detail the risks of induction, what to expect etc. the only reason why I got one was because the midwife mentioned risk of still born which scared me so I said yes to one but I wouldn’t have one again.”
“My waters broke and I did not go in to natural labour so was booked into the consultant ward for an induction. When I arrived I was taken to a private room and left alone with my partner for an hour. We were not given any information on arrival – plus reading posters about the added pain and risks of induction whilst waiting alone added to anxiety.”
“Thursday evening they had started the induction process and I was in the queue to move onto the labour ward and have my waters broken. This didn’t happen until Saturday night. In this time I had no updates and was left waiting whilst the midwives tried to help with the pain of the contractions. It was frustrating and upsetting.”
Feeding
What does the quantitative data tell us?
59% said during their pregnancy, midwives ‘definitely’ provided relevant information about feeding their baby (b12)
53% said after the birth, if during evenings, nights or weekends they needed support or advice about feeding their baby they ‘always’ got this (g15)
When information on feeding featured in feedback it was consistently raised in negative terms, and examples were shared from across the whole pathway of maternity care. Patients highlighted the importance of good quality advice and guidance, including antenatally, as this had an impact on how they experienced feeding. Some patients experienced a lack of consistent information or had received conflicting advice about feeding. It was evident that patients required accurate, up-to-date information that was consistent across all staff.
“Didn’t receive anywhere near enough info antenatally on feeding, particularly after c section so feeding was a disaster.”
“There were many things particularly with baby feeding and sleep that could have been explained better before leaving the hospital. I didn’t have the knowledge on breastfeeding and tongue tie which led to increased mental health issues.”
“During pregnancy i feel as though i didnt not recieve enough information on breast feeding. I wanted to breast feed but was not aware my milk would take time to come in.”
“In hospital, midwifes kept giving differing advice on things like feeding. Made to feel bad for having a hungry baby then made to feel bad for giving baby too much formula.”
“Breastfeeding frequency wasn’t explained properly at the hospital and there were conflicting advice from different midwives. One told us to feed every 3-4 hrs and not demand feed which wasn’t correct.”
Caring for baby
What does the quantitative data tell us?
65% said in the four weeks after the birth of their baby they ‘definitely’ received help and advice from health professionals about their baby’s health and progress (g16)
When this topic was raised in feedback it was predominantly by patients who felt improvements could be made. Patients indicated that they would have liked more information around how to look after/monitor the health of their baby. Specific examples included a lack of information about changing nappies, feeding and burping, and postnatal classes.
“I felt as a first time mum I could’ve really benefited from 10 minutes with a midwife to show me how to feed, burp and change our baby.”
“As it was my first child I had relied on the midwives to help me, most (not all) were cold, and not interested in taking care nor listening to me.”
“One thing that surprised me as a first time mum was that I was allowed to leave the hospital with no real evidence that I could look after my twins. To ensure mums are equipped a demo of how to look after baby should be carried out before being allowed to leave the hospital.”
“We had no tips or anything on how to care for our new baby, being our first, we had no idea how to change a nappy or anything yet had no help from midwives or doctors.”
“It was not discussed about any ante natal or post natal classes e.g baby rhyme time, baby massage etc throughout my journey which was disappointing and I had to find this information out myself.”
Wound care
What does the quantitative data tell us?
26% said they had pelvic health problems during pregnancy or after birth (h7)
51% said they were ‘definitely’ given information about their own physical recovery after the birth (g13)
A specific area identified where more advice and information were required was in relation to those who had a c-section or perinatal tear, with patients commenting that gaps in information provision had meant they had been left not knowing what to expect and how to care for their wounds. It was suggested that this information would have been best provided before discharge from hospital.
“During childbirth i had a third degree tear and required surgery. The extent of my injury wasn’t fully explained neither was i told how to care for this at home or shown/told how to self inject with the Tinziparin. I went home where a GP later discovered i had MRSA in the surgery wound. Noone told me i would receive an appointment with Gynaecology and Physio which left me very confused when an appointment letter came through a month later. The staff on the post natal unit never checked on me as a patient or the baby, offered to help or provide the necessary information.”
“I also feel that more information should be provided regarding how to look after your c section wound as I was not given any advice before I went home. 10 weeks post c section I ended up in A&E as I had to get some stitches removed which had not dissolved and was stopping my wound from healing and causing me pain.”
“However the amount of care I received for my c section recovery was shocking, I was only checked when the dressing was removed. My scar came open and I had to sort myself with little knowledge. There needs to be more care for after c section, my recovery took a very long time and I was still in a lot of pain with no checks from professionals. I had to call my doctors and get information myself. This all should have been explained to me, with how to look after scar, and expectations of recovery!”
“There needs to be more care for after c section, my recovery took a very long time and I was still in a lot of pain with no checks from professionals. I had to call my doctors and get information myself. This all should have been explained to me, with how to look after scar, and expectations of recovery!”
“During my postnatal time on the ward I felt I didn’t get much information about my healing process with a caesarean. I got lots of leaflets on feeding baby but I was not given any about what to expect or how to take care of my wound or aftercare.”
“No antenatal care prepares you for an emergency c-section either, everything is tailored towards a textbook birth. I had to ring for pain relief when I had gone way passed due it as I’d been too busy trying to feed my baby and recover. I was left to work things out for myself a lot and I felt totally alone and unsure following my birth.”
Post-birth debrief / reflection
Another thread observed was patients who felt that they were missing information about what had happened during their labour and delivery. Patients who had been asked if they would like a conversation to review what had happened shared that this had not materialised, often due to staff shortages. Both these patients, and others who reflected that a post-birth debrief/reflection would have been welcomed, were looking to fully understand what had happened and to have support to process what was often referred to as a traumatic experience.
“I have emailed [location name] Maternity regarding a meeting but have not heard back. I emailed in Feb. I want to understand my surgery.”
“It would be helpful to have a debrief after birth giving birth as I do not remember everything that happened. I have questions about my birth and I have no one to contact. I would have liked to speak to the person that delivered my baby and had a debrief of the steps taken.”
“I would like to talk to someone about my birth. I was told I would get a referral to this by a few people and never got one.”
“I was asked if I wanted a debrief to discuss my c section as it was quite traumatic as I lost a lot of blood but the doctor never got back to me in the end so I didn’t get to have a debrief.”
“I asked for a post birth review/debrief at every postnatal check with midwives and they told me one would be booked it at a later date (around 8-12 weeks) however I had never heard anything from them/had an appointment and my baby is now over 4 months old.”
“Quite traumatic birth, was suggested to do birth after thoughts, I requested this and got a bounceback saying the person who does it is on maternity leave and the service has been suspended.”
“It would be helpful to have a debrief after birth giving birth as I do not remember everything that happened. I have questions about my birth and I have no one to contact.”
A small number of comments shared appreciation when time had been taken by staff to explain what had happened during labour and delivery as a post-birth debrief/reflection. Note that the timing as to when this took place was unclear.
“I have had a birth reflection since and it opened up a lot to me about how we were treated, how my care was handled and how it now effects me and my mental health. I have struggled a lot and I am disappointed with some of the care I received at [location name].”
“All staff were very good recently requested debrief and spoke to [name] regarding the following feedback: Pain relief didn’t work rather than increase, offer other options. Offer gas & air in theatre whilst setting up. Offer support to transfer onto operating table. Discuss how to self refer for a debrief after birth.”
3.2.9 Mental health support
What does the quantitative data tell us?
90% said they were given enough support for their mental health during pregnancy (b8)
77% said during their antenatal check-ups, midwives ‘definitely’ asked about their mental health (b7)
94% said after the birth, a midwife or health visitor asked about their mental health (g10)
61% said they were ‘definitely’ given information about any changes they might experience to their mental health after having their baby (g11)
83% were told who they could contact if they needed advice about any changes they might experience to their mental health after the birth (g12)
45% said at the postnatal check-up (around 6-8 weeks after the birth), the GP ‘definitely’ spent enough time talking about their mental health (g18)
Amongst patients that had a need for mental health support during maternity care, there was predominantly negative feedback.
Birth experience
A term used across this dataset is ‘trauma’ / ‘traumatic’ and while for some patients this is not articulated in the context of mental health needs or experiences specifically, for a noteworthy proportion of patients it is explicitly stated their experience of maternity care has resulted in mental health support being required for Post Traumatic Stress Disorder (PTSD). Examples describing care as traumatic are shared below alongside mentions of PTSD, some of which feature elsewhere in this report.
“I have received counselling as a result of my labour as I was traumatised significantly by it.”
“My requests weren’t listened too. Overall this has left me with a huge amount of trauma around my birth and it ruined an experience I will never get back.”
“Was not checked thoroughly enough pre c-section for pain relief. Could still feel and was incredibly traumatic. I ended up opting for being put to sleep. Recently had an assessment for health in mind and I am on the CISP for PTSD on the trauma scale.”
“I cried in triage because of how the midwife was treating me. In response, the midwife raised a concern about my mental health to my community midwife team, thus relinquishing herself of any accountability for her behaviour being the reason I was so upset and blaming my mental health for my upset.”
“I am extremely traumatised still from my birth experience. I had an emergency c section… I was discharged with an infection to then be re-admitted to another hospital 24 hours later. I tried to get support for all of this like a talking therapy, but was offered CBT which is not suitable for the trauma I went through. I am deeply impacted by this experience.”
“It was upsetting hearing the nurses come in and talk to all the other patients in the room and often ignore me completely. I think this may have slightly contributed to my severe decline in mental health following discharge – where two weeks later I was diagnosed with PPD.”
“The delivery team were amazing but sadly as soon as I was put on the ward for 5 days due to complications of my babys birth it wasnt a great experience which has gave me slight ptsd about going back in a hospital, even when my c section opened up I didnt go in as I was terrified due to my experience with some of the midwives on the ward after the birth.”
“My labour however was unfortunately not a good experience for me. Despite having a flagged specialist care plan, highlighting a need to feel listened to, and to have a compassionate approach due to PTSD from a previous birth, the experience was cold and clinical. This affected me intensely.”
Bereavement
Also evident in the feedback were suggestions that services need to be more proactive in supporting mental health needs where patients had previously experienced miscarriage and/or neonatal baby loss. There was frustration for patients when they had to repeatedly explain their situation, which felt avoidable through using patient notes more effectively, if not also through delivering continuity of care. Where patients felt that their previous losses were not accounted for during this maternity journey, this left care feeling impersonal and could exacerbate their need for mental health support.
“I also feel the trust could improve communication between staff in regards to previous pregnancy losses. If my appointment was not with [name] I had to explain on multiple occasions this was not my first baby and that my other two babies had died as a result of pre term labour and neonatal death.”
“Haematology support was wildly different between the 2 hospitals which was confusing. Scan technicians were unaware of previous pregnancy loss. Had to explain previous blood clot to doctors whilst screaming through contractions – isn’t this information available on my NHS record?”
“Midwife did not refer me to bereavement or mental health midwife until 7 months pregnant, even though I requested this at my booking appointment at 9 weeks due to previous loss. Midwife said ‘everyone wants support so you’ll have to wait’ and made out like I was an inconvenience for requesting mental health supports!”
“This is my 4th pregnancy. My 3rd resulted in a neonatal death. People were not aware of this throughout my pregnancy and birth. Every appointment tended to be a different doctor at clinic meaning I had to explain the trauma we had been through.”
Notable exceptions
While rare, patients with positive experience mentioned access to specialist staff such as a “mental health midwife” or highlighted members of staff who had been particularly helpful in supporting their mental health. These comments demonstrate how valued this support is when it goes well.
“I cannot fault the care I received during my pregnancy and after the birth. It was a traumatic delivery and I suffered a severe PPH due to placenta praevia, my son also spent some time in SCBU. Every single midwife was so caring, kind and supportive during our stay. It was a very challenging time both physically and mentally and the team made everything we went through that much easier.”
“I ended up having a meltdown halfway through pregnancy of which I had to reach out for help which resulted in my midwife team referring me to the mental health midwifery team.”
3.3 Prior to labour
Where possible, insight within this section is shared in an order of what is anticipated to be chronological, e.g. confirming a pregnancy is shared before mentions of gestational diabetes testing. That said, it is not always explicitly clear in the feedback exactly when or where the care took place.
3.3.1 Contacting services
What does the quantitative data tell us?
of those who contacted a midwifery team during pregnancy, 74% said they were ‘always’ given the help they needed (b9)
Patients who mentioned contacting services during their antenatal care primarily shared negative experiences. Not being able to get through to services on the telephone was the main issue shared, and ultimately not being able to get in touch with a midwife when needed. The reason for contact was rarely given.
“When I called the antenatal department, no one answered the phone. This happened several times.”
“Tried to ring triage over and over again to ask about my symptoms. I got stuck in an endless loop of ‘press 1’ type menus and if it did get through to triage the phone hung up.”
“It is very hard to contact the midwife during pregnancy.”
“My community midwife was wonderful and I had weekly blood pressure checks with her. However, as she took over from another, I don’t think the correct mobile number was given to me as I rang the number three times over the course of my pregnancy and the phone was never answered and I was never called back – by her and the original number.”
3.3.2 Checks and scans
What does the quantitative data tell us?
81% said they were ‘always’ given enough time to ask questions or discuss their pregnancy in antenatal check-ups (b5)
Comments that referred to antenatal appointments focused on ‘check-ups’ (mainly those with midwives) and scans that needed to happen during this stage of care. A pattern observed in feedback was expectations not being met regarding being equipped to make an informed decision and/or the ability to discuss questions. This indicates a need for clarity prior to appointments on what to expect and signpost to support should patients have questions.
“more information/reassurance when referred for growth scans.”
“When I had growth scans there was little time to discuss concerns and a delivery plan.”
“I had a previous emergency C section, so was expecting to have appointments arranged to discuss birth plan with consultant/Dr. However, I didn’t have any specific appointments for this. I did have additional scans due to an anomaly flagged at 20 week scan, so met consultant at these appointments and discussed births plan. However it was unclear if this would happen at these appointments beforehand. I called my midwives [location name] and [location name] to try to understand if I should expect a specific appointment with consultant to discuss birth plan but no one could tell me if I would have a specific appointment and if so, when this would be. Although in my case this wasn’t a problem as I had the additional scans so had the opportunity to talk to a consultant, I felt frustrated with lack of clarity on this and if I would have had the right appointment if I hadn’t needed the scans.”
Feedback highlighted ‘long’ wait times for antenatal appointments, although it is unclear what would be an acceptable waiting time there were comments which suggested two hours was too long.
“Clinics overbooked, wait times > 2 hours per antenatal appointment.”
“The antenatal check up waiting times are horrendous but the care is great.”
“I have raised these directly but I had concerns with the waiting times for consultant clinic at [location name] (often 2 hour delays).”
“I turned up for my booking appointment on a Saturday morning and the clinic was completely closed. I made an official complaint about this.”
3.3.3 Gestational diabetes
While the data referencing gestational diabetes was sparse, it highlighted variation in individuals’ experiences as to the extent it was managed during pregnancy. Feedback included that for some, they felt diagnosis came late and/or was not adequately managed, whereas others felt they received good support once diagnosed.
“I had gestational diabetes and the care I received from the diabetes team was outstanding.”
“I had a terrible experience with the Gestational Diabetes team. I was not told for 2 weeks that my GTT had raised concerns appointments were made for me that I had no knowledge of… Nothing else suggested I had gestational diabetes besides the initial GTT test.”
“Triage at [location name] was awful, I had gestational diabetes and they didn’t tell me and also hypertension. They were bringing me in every day for monitoring to sit all day then send me home, they eventually gave me medication after a week.”
There was no detail in the data as to why these disparities in experiences existed and no patterns observed by demographic groups sampled for.
3.4 Early labour
Within this section, feedback was attributable to the experience of early labour and most typically shared in the context of an acute hospital setting as opposed to community and/or home. This was explicit in some of the feedback and/or inferred in others.
3.4.1 Access to hospital
Where patients spoke of accessing a hospital to give birth, predominantly negative experiences were shared.
Delays to admission
What does the quantitative data tell us?
85% of those who had a labour said they were given appropriate advice and support when they contacted a midwife or the hospital at the start of labour (c6)
9% of those who had a labour said they were sent home during labour when they were worried about themselves or their baby (c7)
Patients reported negative experiences of decisions made and advice given by healthcare staff in relation to when they should arrive and be admitted to hospital to give birth. In these cases, it was felt that the decisions were not always correct. The impact of what were considered by patients to have been incorrect decisions made about their care resulted in being sent home; gaining access to hospital only once very or fully dilated; almost not making it to hospital to give birth; and births happening very quickly after arrival at the hospital. The impact on patients was clear as to the stress and anxiety observed in the data.
“Throughout my pregnancy I was reassured that I could come in as soon as I started having contractions even if it would be a while before the baby was born. However when I phoned, with very strong contractions, the person I spoke to on the phone asked if I should stay at home for an hour to see how I get on – if I had done that the baby would have been born at home!”
“I rang triage and said I was having cramps and discharge, they told me to ring back in an hour and they’ll have a look if there was anymore. So I rang back an hour and explained I had more and I spoke to a different women on the phone said to me not to bother coming in and it’s nothing, I explained I was really worried and I felt completely belittled by her saying ‘it’ll be nothing, just mucus plug.’ Luckily I went in and my baby had pooped in me and was induced within half hour.”
“Appalling care from agency midwife day of labour. I went into triage after waters breaking and there was no beds available on the ward so I was put in a delivery room. I was in a lot of pain and the midwife lacked empathy. My husband was helping to open packets of testing material to check if my waters had gone. There was no second midwife. She led me to believe my waters hadn’t gone when I later found out they had. My cervix was checked and she said it was closed. I said it was 2cm last time and she said ‘2cm is nothing’. I was sent home in pain and made to believe my pain was not bad enough to be in labour. Arrived back at triage hours later and was 10cm dilated.”
“I followed every advice and I attended every appointment only to end up having an emergency c-section at the last minute. A day before I gave birth I was at the hospital because I had called to tell them I was having contractions every 2 to 3 minutes, I came in and I was accessed by the midwife who concluded I wasn’t ready to give birth yet, but I was ready because the contractions were strong and I wasn’t feeling like myself but of course because I wasn’t rolling on the floor in pain they concluded I wasn’t ready. I was giving a membrane sweep & sent home at about 2am in the morning, although they mentioned we could stay back but neither I nor my partner could rest so we headed home. At around 11am in the morning my water broke, I called the clinic & they told me to come in, we hurried to the hospital. By the time we got there the baby had poo & I was told about the emergency c-section. This could have been handled better & they should have listened to me about the pain I was feeling.”
Waiting times
Patients reported negative experiences of having to wait, sometimes days, to be induced, have c-sections and access the labour and delivery wards in hospital. Extended waits were sometimes said to have left patients in pain for lengthy periods of time. They could also cause emotional distress for those waiting and undermined confidence in the care they received. The commonly cited understanding for why they were having to wait were a lack of bed availability and lack of staff, along with emergencies taking precedence.
“I was diagnosed with gestational diabetes and had a planned c section. The day I had my c section booked there were multiple emergencies which took priority of course. I was told mid morning to eat as they were worried I would get low blood sugar and that my c section would be that afternoon instead, I trusted the staff and did this. A few hours later the emergencies were done quicker than they thought but I could not go in as I had eaten so got bumped down the list. My c section ended up being cancelled at 5pm after being sat on the ward since 7am. I understood the emergencies could not be helped, they checked my sugar before I left which was now low as I had waited so long without food.”
“Whilst waiting for my c-section I had a similar thing where they told us to get there for 7am and we’d be taken down by 11am. We were in a waiting room and I had to lie on the floor, at 11am they said it may not happen today. I was starving and in agony, at 1pm they said okay let’s go down.”
“I had a planned c-section, but was last on the ‘list’ for that day. Due to several emergencies, I wasn’t seen until much later than expected. Whilst this couldn’t be avoided, it triggered my anxiety and there was very little information given to us to when I would be having the baby.”
“From when my water broke they kept me waiting over 24 hours that led to my baby had an infection when born. Next time they should induce me straight away.”
“Spent 3 days in hospital waiting for induction after my waters broke to start contractions however due to lack of staff I was unable to go to the delivery suite for this to happen. I then ended up classed as an emergency c section which took 3 days before being able to have this done.”
“The triage however is utterly lacking – in all bar my last visit it was an 8/9 hour + day and there were simply no doctors. How you could be expected to go into spontaneous labour while sat in that awful [location name] triage waiting room (where at times there were no seats available) I don’t know.”
“The only negative I have is waiting for a hospital bed due to lack of staff and not being assessed regularly during labor again due to staff shortages.”
“I was admitted as my baby had stopped growing at 38 weeks and was not given a bed for 24 hours despite being told rather worryingly that the baby needed to be born for their safety.”
“I was called in Thursday morning once a bed was available. Thursday evening they had started the induction process and I was in the queue to move onto the labour ward and have my waters broken. This didn’t happen until Saturday night. Induction process was equally badly managed. I was asked to arrive to the hospital while there were still no beds available and the process wasn’t going to start for another 24hrs.”
“The only hiccup I can think of now was that I was booked for induction on Monday at 08:30 however wasn’t able to be transferred to delivery suite until Tuesday 16:00 as they were so busy.”
3.4.2 Choice and involvement
What does the quantitative data tell us?
82% said they were always involved in decisions about their antenatal care (b11)
of those who said they were induced, 76% said before they were induced, they were given appropriate information and advice on the risks associated with an induced labour (c4)
77% said during labour and birth, they were always involved in decisions about their care (c16)
75% said during postnatal care, they were always involved in decisions about their care (g1)
Having a role and feeling involved in decision-making was very important to patients. When this was experienced, it was very positively described by patients who gave high praise to individual and sometimes named staff members. When it was not experienced, it had significant negative impacts.
Care/birth plans
What does the quantitative data tell us?
79% of those who were induced were given information about induction of labour (c5)
25% of those who were induced were given information about increased monitoring without an induction (c5)
20% of those who were induced were given information about planned caesarean birth (c5)
Patients shared both positive and negative experiences on the extent to which they had choice and involvement in early labour and plans for delivery. This incorporated whether plans put in place antenatally were followed, but also decisions being made in the moment. Patients were very appreciative when they had positive experiences. In these cases, it was noteworthy that they often named specific members of staff, singling them out for praise, indicating that a relationship of personalised care had been built with them. This reflects the positive descriptions outlined earlier in the ‘Staff manner, attitudes and attributes’ sub-theme. The following common characteristics underpinned these positive experiences, which suggests that services should work to ensure that they are consistently in place:
patients being listened to
staff being familiar with and acknowledging the care plan
patients being provided with enough information to make informed choices
patients feeling their choices were respected
staff empowering patients and offering support when required
“My midwife [name] who is part of the [location name] team was amazing. She got to know me, respected my wishes and really took her time to make my care feel personal and not just another mum to be.”
“The midwife’s who helped me during labour and birth was absolutely amazing! I’m very lucky to say I had the birth that I wanted! Calm and positive. They were very reassuring and helpful.”
“I had a really positive birth in the birth centre and had a water birth which is exactly what I wanted. The midwives supporting me were amazing particularly [name] who really helped to calm me down and was able to support me exactly how I needed whilst also giving me the space to do it on my own.”
“The ongoing care and support myself, my baby and partner received from day one of my pregnancy and after I had given birth was second to none. My community midwife was amazing throughout and listened to my concerns and made me feel heard. The labour midwives who were on shift whilst I gave birth were just as amazing, they listened to my wishes of a water birth and followed through with this immediately. They respected my space and offered support when needed.”
“The consultant I spoke to was extremely supportive of this decision and gave me all of the information to make sure I was making the right decision, without influencing my thoughts.”
In contrast to positive experiences, feedback that spoke to areas for improvement referred to a birth plan not being respected. Patients could feel pushed into choices which were not in line with their preferences, or that they had to be insistent to have these considered. There were also instances where patients were simply not told what was happening, which could lead to them feeling traumatised by their experiences. This strongly links to the findings in the ‘Mental health support’ sub-theme earlier in this report.
“Felt staff pushed for vaginal birth too much. My first two babies were vaginal delivery, this time opted for c section given my past difficulties (and this baby was breach…). Regardless, on multiple occasions the staff pushed for vaginal delivery again.”
“The doctor at the point of my birth when deciding to go for c-section or assisted birth, when I chose c-section, they tried to talk me out of it and did not make me feel supported.”
“My preference was always to have a home birth; at no point was I offered this choice. I had to continually push for this to happen.”
“He wanted me to accept the only option he gave me, which was an instrumental delivery. I never wanted an instrumental delivery and I asked for a C-section based on my own knowledge because the doctor did not give me that option… I’m sure they never read the birth plan that the midwife filled out during my prenatal care where I said that I never wanted an instrumental birth.”
“My main issue was that when I went into hospital for checks after 42 weeks it was very clear the pressure I was under for induction. This is a very narrow minded way to approach a woman in my position.”
Issues were particularly evident in relation to patients being able to have the type of birth they preferred (e.g. a water birth, a home birth or a c-section); or having a say in whether they were induced. Reflecting the earlier ‘Information provision’ and ‘Staff manner, attitudes and attributes’ sub-themes, patients described feeling patronised, a sense they were not being presented with all the information and that their views were not respected.
“Stop pushing people towards inducement.”
“There is a pressure to book inductions in which isn’t presented as a choice.”
“I wasnt happy with the approach of the obgyn that was appointed to me, [name], he made me feel uncomfortable most of times and made unnecessary comments. My baby was measuring on the smaller side but everything else was great with me and my pregnancy and she was still growing after every scan. I was pushed to give birth at 37 weeks even if i insisted as i trusted my body that everything is okay and i can carry her without risks at least 38 weeks. My decision was not supported but instead the risks were pointed out in a very scary way.”
“My only negative; during my antenatal care was that I felt pressured into having an induction, despite having gone overdue with my previous two + no birth complications.”
“Antenatal care at [location name] was average especially when trying to persuade me not to have a C section when I had already made up my mind.”
“The consultants were defensive and patronising in their discussions and had no time or interest in listening to my concerns or different strategies. As a result of being endlessly misunderstood i opted to trust myself and my body and gave birth naturally and safely at home alone.”
“However, when it came to my choice of a home birth ‘outside of guidelines’, she didn’t fill me with confidence and expressed how she hoped I wouldn’t go into labour when she was on call. I also found one particular consultant to be very patronising, condescending and dismissive when I expressed my desire for a home birth.”
Choice of birth location
What does the quantitative data tell us?
59% said they were offered a choice of hospitals to have their baby (b1)
29% said they were offered a choice of birth centres to have their baby (b1)
18% said they were offered a choice to have their baby at home (b1)
12% said they were not offered any choices about where to have their baby (b1)
58% said they ‘definitely’ got enough information from either a midwife or doctor to help them decide where to have their baby (b2)
Patients not being able to give birth at their preferred location was another sub-theme relating to choice and involvement. This was highlighted for home births and not being able to give birth at an alternative to the delivery unit at their chosen hospital. A lack of staff was pointed to as a reason for this by several patients which is why it arose during early labour as opposed to prior to labour, as it was not anticipated and planned for.
“We were accepted at the delivery unit first, despite planning to give birth at the birth centre. On the phone we were told that in the birth centre there were no free rooms and that it was a chaotic night in the hospital so we were offered the delivery unit as the only option.”
“The planned home birth didn’t go ahead due team unavailable once on established labour. The Trust still not providing enough staff for the home birth service.”
“I was told all along I had a low risk pregnancy and could give birth in the midwife led unit. As my due date approached, I began to hear that delivery in a midwife led unit was statistically unlikely (see [location name] stats on midwife led vs delivery suite deliveries). I was told staffing of the midwife led unit is often the issue so women are sent to the delivery suite regardless. I think it’s important to better set the expectations for women who are keen, as I was, for a midwife led delivery. It seems disingenuous to offer it all along if in reality it’s unlikely to be where the baby is ultimately delivered.”
“The only negative I experienced was in regards to the midwife led unit at [location name]. I had really wanted to give birth in the [location name] birth centre after the information I had been given from my midwife and what I had seen on the tour of the hospital that we had joined our antenatal classes. I have been told that the number of people that were able to use the [location name] birth centre was very low due to staff levels and the information that the midwife gave us during the tour seemed consistent with this. I had spoken to the community midwife about it and she had said that a lot of people didn’t get to use the [location name]. I do feel that this added a lot of stress to the later stage of my pregnancy.”
3.4.3 Presence of birthing partner
What does the quantitative data tell us?
95% said if their partner or someone else close to them was involved in their care during labour and birth, they were able to be involved as much as they wanted (c9)
For some patients, birthing partners had not been allowed to stay with them once they were experiencing contractions and this feedback included an example of a partner missing the birth consequently. Patients emphasised how the absence of their birthing partner caused them distress. Please note references to someone accompanying the patients during labour are interpreted as ‘birthing partner.’
“My partner missed the birth of our child due to staff not listening to how I was feeling. Visiting hours need to be scrapped.”
“The biggest issue I faced was my partner being sent home when I went into early labour. I had to stay on the ward but he was not allowed to stay with me and I was really distressed. I have really bad anxiety around being in hospital and this made things so hard.”
“I was told my partner was unable to stay with me in hospital both during and after labour despite telling them I was too anxious to be on my own in labour.”
“I had an emergency c section and was put to sleep and understand some of the reasons why. But when my partner got told to say goodbye, removed from theatre and was left to sit in the delivery suit in the dark (where all our stuff had been removed) alone for half an hour or so with no one explaining what was happening or comfort, it was very traumatic for him.”
3.5 Labour and delivery
Within this section, feedback was typically shared in the context of a hospital setting as opposed to home. This was explicit in some feedback and/or inferred in others.
3.5.1 Pain relief
What does the quantitative data tell us?
of those who had a labour, 65% said during labour and birth, they thought that their healthcare professionals ‘definitely’ did everything they could to help manage their pain (c8)
Patients reported being in excessive and avoidable levels of pain during labour and delivery. Feedback frequently explained patients had asked for pain relief but that this had not been acted on. Below shows the wide range of overlapping reasons given as to why adequate pain relief was not received when patients felt it was needed.
lack of clarity around pain relief options
staff not proactively offering pain relief
not being listened to or believed about the level of pain
lack of monitoring, with labour progressing too far
staff being too busy or unavailable to administer pain relief
poor administration of epidural pain relief, leaving patients without pain relief
“I did not have proper pain management during my labour.”
“I feel my contractions were not taken seriously during my induction. And I was not proactively offered any pain relief.”
“I feel the 4 hour checks should be reduced to two as I had to labour on just paracetamol while not being able to physically stand due to pain and pressure.”
“Pain relief was only given if I asked for it, there was no regular check in with me to offer pain relief. I wasn’t really sure what was available to me.”
“When in labour it would have been nice to have a few more check ins from staff as I had to ring a couple of times (once which was that I was due my pain relief).”
“The medical team could have helped me with the pain; I was not offered an epidural as discussed in the childbirth planning consultation, nor any other type of medication to relieve my pain except for the gas, which did absolutely nothing. I had to go through a very uncomfortable and painful natural birth because the midwives claimed there was “no time left”.”
“When I asked for pain relief I was told no doctors were available due to demand of other patients. I was left with only gas and air, was told to keep pushing despite no more strength to do so.”
“There were similar delays with getting pain relief during labour because of the need for someone to sign off the meds. I get that procedures need to be followed but the delay really needs to be addressed.”
It is noteworthy that comments which mentioned being disbelieved in relation to how much pain they were in, highlighted the speed of their delivery and expressed concerns that the lack of earlier action had contributed to the need for a c-section.
“I was happy with my care, except for being unable to have an epidural. I was in pain but only dilated 1cm so was denied the epidural, but then the baby arrived within the hour.”
“I was in pain I was being induced and it was like they didn’t believe me and minutes after that I was in active labour and had to have a c section. I was in so much pain and had no help or didn’t believe I was as I dilated really fast.”
“I was given pain medication close to giving birth that should not have happened and caused my baby’s heart rate to drop thus leading to an emergency c section. I strongly believe if I was examined more frequently this pain medication would not have been offered and a strong chance I would have not resulted in a emergency c section.”
Where patients commented that pain relief had not worked, this was usually in relation to an epidural. These comments typically also mention that staff did not listen to their concerns about the epidural not being effective.
“In labour my epidural didn’t work. It took me getting up and walking before staff believed me.”
“During labor, I was administered an epidural, which was supposed to alleviate my pain. However, due to a leak, the epidural only affected half of my body, leaving me in severe pain for an extended period.”
“I had an emergency c section the man who delivered my baby kept repeating he was going to start cutting me open when I was still awake with NO epidural, this box isn’t big enough to write about that s*** show!”
It is important to highlight that a small number of experiences were shared that detailed staff attempting to insist on pain relief against patient wishes.
“During my labour, there was a lovely midwife who kept insisting to me that I should have an epidural while I understand her good intentions, I think if a mother wants to push through it and have no medication then that should be respected. I heard afterwards (after birth) from my mum and sister that she told them to convince me to take the epidural. A bit frustrating but it’s okay.”
3.5.2 Staff proactivity and responsiveness
What does the quantitative data tell us?
12% said they (and/or their partner or a companion) were left alone ‘during early labour’ at a time when it worried them (c11)
7% said they (and/or their partner or a companion) were left alone ‘during the later stages of labour’ at a time when it worried them (c11)
3% said they (and/or their partner or a companion) were left alone ‘during the birth’ at a time when it worried them (c11)
76% said they (and/or their partner or a companion) were not at all left alone during labour and birth at a time when it worried them (c11)
66% said during labour and birth, they were ‘always’ able to get a member of staff to help when they needed it (c13)
As described within ‘Early labour’, patients reported that once admitted to hospital, staff did not carry out checks frequently enough to monitor how labour was progressing. This was said to have implications in terms of increased pain; being rushed to delivery areas; and health risks. Several comments inferred that a root cause was staff not listening to, believing, or having confidence in patients’ knowledge of their own bodies. Please note the link back to the sub-theme ‘Being listened to’ for further examples of how a lack of listening to patients impacted experiences of care.
“When I arrived at the birthing centre nothing was ready even though I had a history of quick deliveries and the midwives didn’t seem to know what they were doing. They did not get the birthing pool ready or even set up a bed so I had to give birth to my son on the floor as there was no where else to go. It was an incredibly traumatic experience and I did not feel well looked after there.”
“I had an awful experience from when I was admitted in to be induced. My heart rate and my baby’s heart rate went very high so I decided on a c section where I was left for 3 days constant ill of mouth alongside I had an infection and could barely get out of the bed. I waited hours and hours for doctors and I feel deeply neglected with the whole situation it was the first birth I had and the treatment was awful. I was left attached onto a drip that had finished for 2 hours after and asked to get it removed several times and asked for anti sickness several times and had to wait 2-3 hours.”
“I gave birth in 3hrs 50mins at 19:52 hours after having my waters broken. I was not administered the hormone drip. I asked for an epidural around 18:30 but was told by the initial midwife he would not be checking me until 20:00hrs – at approximately 19:00hrs I told him I felt like I needed to push. Again I was told he would not be checking me until 20:00hrs. He then handed over to the next midwife, I repeated to her I felt like I needed to push so she checked me and I was in fact 10cm dilated. Looking back it just felt like the initial midwife wanted to clock off shift and didn’t want to get involved in the labour.”
“I wasn’t allowed pain relief as they couldn’t confirm active labour as they wouldn’t examine. I had bite marks in my hand and was pulling out my hair in sheer agony. They saw the pain I was in and ignored me, then congratulated me for going through labour on two paracetamol. I didn’t feel like a hero – I felt violated and traumatised.”
“When I went into labour, I called the maternity ward. I said I felt I needed to be seen and they said my contractions weren’t close enough, so I had to lie and say I couldn’t feel my baby to get them to take me seriously. I got there and my baby was delivered only 30 minutes later. When I got there, the midwife did a cervical check and said I was 4cm dilated. I explained this wasn’t 4cm pain as this was my second child. I was so scared and said to them I think something is seriously wrong and that if I was only 4cm I think I’m dying. The midwife kept laughing at me. I got angry because I was in so much pain and she turned to my husband and sarcastically said ‘good luck’. Furthermore, I told the midwife my baby’s head was coming out to which she laughed and said ‘no it’s not’. She didn’t check, my husband had to look to confirm that yes, this was a very quick birth and my daughter’s head was in fact coming out.”
Consent
An issue of consent was evident in the feedback about labour and delivery experiences with several patients describing they did not consent explicitly, or wanted someone else to have the ability to consent for them, to procedures carried out.
“I did not consent to an episiotomy but was given one.”
“And also I was given an injection immediately after my baby came out on my right thighs and I was not told what the injection was for, and have been having slight pain when I stretch my leg.”
“Please involve partner or someone else who is carer for pregnant women to take consent and specific type of birth decision at the moment.”
“I have only one concern. During labor, when the medical team decided they needed to use forceps and transfer me to another room, I was asked to sign a document. I was told that if I didn’t sign it, they wouldn’t be able to proceed. I was in severe pain, using gas, and had no idea what the document was about. I asked if my husband could sign it, but I was told it had to be my signature. It is unacceptable to force a patient in such a condition to sign anything. To this day, I still don’t know what I signed.”
3.5.3 Comfort of the environment
Where the comfort of furniture was raised in feedback and the context was labour and delivery, it was discussed largely in relation to the needs of birthing partners. A prominent suggestion was that chairs needed to be comfortable enough for birthing partners to sleep on.
“Whilst it was lovely that my husband could stay the night, the facilities for him were terrible. He only had what I would describe as a plastic school chair to sleep on, which isn’t adequate for a new father.”
“One thing that I think could be better but I understand it’s not possible based on budgets is the seat / bed setup for partners / family. It was a really uncomfy chair.”
“When being unable to go home after birth due to complications, make partners as comfortable as possible if staying overnight beds available sooner. I spent 7 days in hospital & my husband slept on a chair for 2 days.”
“The only thing that would have made the whole experience better for us would have been for my husband to have had access to a comfortable reclining chair or somewhere to lay down. It just meant that we were equally as sleep deprived as each other almost and when this became more of an issue for me he could have been more rested to look out for both me and the baby instead of also being quite exhausted as well.”
“I think partners should be provided with reclining chair to assist in their rest as they are essential in care and recovery.”
3.6 Soon after delivery
Within this section feedback was typically shared in the context of a hospital setting as opposed to home. This was explicit in some feedback and/or inferred in others.
3.6.1 Pain relief
What does the quantitative data tell us?
of those who said they stayed in hospital after the birth or required hospital care after a home birth, 66% said their healthcare professional ‘definitely’ did everything they could to help manage their pain in hospital (d7)
Patients reported delays receiving pain relief after they had given birth, experiencing unnecessary and avoidable pain because of this. In these instances, staff were not proactively providing pain relief, patients had to chase up requests for pain relief, and medication could be missed. Delays in receiving pain relief were often attributed to a lack of staff and/or staff not listening to patients.
“Aftercare on the ward wasn’t as good [as labour ward]. Longer wait times for pain killers.”
“When I told the hospital staff for pain killer, then every time I was waiting for long hours.”
“The only issue I had in hospital was with pain meds. I went all night without them because I kept thinking they would bring them around and they didn’t.”
“On ward told by midwife that paracetamol & ibuprofen would be enough for post c-section pain despite asking for oral medication, before I mobilised for the first time. It was not & I fainted in the shower due to the pain.”
“When I had asked for pain medication (was only paracetamol!) one of the nurses said she would get me some, came back some hours later because she had forgot, said she’d get it for me in a sec when the changeover happened. I asked for my pain meds, they couldn’t give any to me because she wrote down that I had received some!”
“Not even 24 hours after my cesarean I was left 7 hours with no pain relief. When I asked the midwife on shift when I would be having it she said I didn’t have any as I needed to ask for it. By this point I couldn’t get myself up off the bed and got so upset (I already struggle with mental health). The midwife I had that night was an angel and made sure I had stronger pain relief, and kept on top of it for me.”
“The lack of pain relief post c-section was horrendous given that it is major surgery, I was left hours without anyone attending when I pressed emergency buzzer.”
“The after birth care in the hospital ward is embarrassing and impacts negatively the perception about [location name]. I spent the first night with no painkillers even when I requested them repeatedly (with an episiotomy and 2 stitches) — really stressful and dangerous for an epileptic patient. When I asked any questions, the midwife would read the answer from the pamphlet they gave us the first day. They didn’t know the answers or had further information. I arrived there after a 21 hours labour with almost no sleeping and I was concerned I could have a seizure. No one cared. The neurology clinic was very concerned when I told them my experience. Shameful.”
3.6.2 Staff proactivity and responsiveness
What does the quantitative data tell us?
9% said they (and/or their partner or a companion) were left alone ‘shortly after the birth’ at a time when it worried them (c11).
Of those who said they stayed in hospital after the birth or required hospital care after a home birth, 57% said while in hospital they were ‘always’ able to get a member of staff to help when they needed it (d3).
The need for responsive care soon after delivery was highlighted by a range of patients, most commonly for those experiencing mobility issues following a c-section. Assistance from hospital staff was also needed to care for newborn babies in these instances for some. Other responsive care needs reported as unmet for some patients included assistance with mobility to access what they needed. A lack of response to requests for help using a call button were also shared, although there was not always detail on what help was needed.
“I felt uncomfortable with some staff so I wouldn’t press buzzer for anything and had to clean up and walk to a water machine after having C-section.”
“Asked a midwife to help me lift my nearly 10 pound baby out of the next to me as my incision was hurting when I twisted and she said ‘that’s the whole point of a next to me that you do it yourself’ which made me feel terrible and left me crying.”
“Aftercare was virtually non-existent — didn’t change my pads, didn’t check my c section scar / bandage once, wanted to discharge me the next day when I told several staff members I wasn’t ready. I was in a lot of pain, could hardly walk, didn’t have support at home — all fell on deaf ears and I was kicked out of an empty ward so it wasn’t like they needed the bed.”
“I felt and believe that the [location name] hospital staff were neglectful in a sense due to I only saw them maybe twice every 13 hours. The only staff member I actually thought was amazing and was good at her job and wasn’t rude was a student midwife named [name].”
“I struggled mostly post-birth with the care/lack of care that I received. It was like a third world hospital ward.”
“I would like to mention that during handover times, no staff were available and responsive to the call bell. The call bell rang for over 30 minutes before I was checked on. I was still unable to walk independently at this stage (post c-section) and my partner was not there.”
Some patients described being left in blood or that they experienced an inability to take care of their personal hygiene. Staff were found to not be proactive or responsive when support was requested for these situations. Across examples were concerns raised about staff attitude as well as capacity levels.
“I was disappointed with the length of time it took to get me cleaned up and moved to the room I would be staying in at the birth centre.”
“I asked for new sheets as they were covered in blood from where I was bleeding post birth, they never got round to changing them. So was sat in my bloody sheets for over 12 hours.”
“I was given no care post birth and left covered in blood to clean myself up which was very bad and really affected my first hour where I should have been bonding with the baby.”
“I had to ask for my sheets to be changed. I also had to ask for help with washing when the support staff just put all the stuff on the bed expecting me to do it myself when I could barely move or bend post c section.”
“No care at all for personal hygiene after the C-section even when I stayed with my baby for a week in intensive care and I couldn’t bend to wash myself properly.”
There were also concerns that babies were not being monitored following birth as closely as patients believed was necessary, and this was seen to have delayed diagnosis.
“After the birth of my baby, I was left by my midwife — she said she should be 5 minutes, she didn’t come back for at least an hour. A new midwife came in and said the previous midwife had gone to their dinner and they switched shifts. During this time I had no idea that my baby was hypothermic and he had problems with his gut. I believe if I was seen to earlier or had the same midwife with me this could’ve been caught right after birth not 2-3 hrs later.”
“Also, a couple of hours after I gave birth, I raised a concern about my baby looking yellow with the midwife, which she didn’t give me a satisfactory answer for and wasn’t acted upon until the night-shift midwife came on and she did her preliminary checks and confirmed that the neonatal doctors should have looked at my baby as he was quite yellow. Things moved fast after that and my baby had to be admitted in the Special Care Unit to receive phototherapy and antibiotics.”
“After having a C-section, I feel there’s not enough support to care for baby. My baby needed light therapy and it was extremely difficult attending to my baby, getting him in and out the incubator myself for a feed when recovering from a C-section. I feel I wasn’t listened to when expressing concerns about my baby not feeding well. The midwife was happy to discharge me even though my baby hadn’t fed well through the night. He was on the hypoglycaemia pathway, so as blood was being taken the doctor ran a bilirubin test and it was picked up that his bilirubin levels were high which explained why he wasn’t feeding well.”
Across multiple comments comparisons were drawn by patients between postnatal care and earlier care in the maternity journey. There was an inference in this feedback that there was a decline in quality of care once the baby was delivered, particularly in terms of staff being both proactively attentive and responsive to explicit needs.
“The delivery team were amazing but sadly as soon as I was put on the ward for 5 days due to complications of my baby’s birth it wasn’t a great experience which has given me slight PTSD about going back in a hospital. Even when my c section opened up I didn’t go in as I was terrified due to my experience with some of the midwives on the ward after the birth. Some of the midwives were not nice at all, unsupportive and didn’t listen to me which resulted in my anxiety (which I wasn’t able to get my medication for until towards the end of my stay) being really bad and feeling very stressed and emotional. I could not wait to get home where I felt safe.”
“Was shocked and appalled by my awful post birth experience at [location name]. Felt forgotten about in the delivery suite for 7 hours after the birth. Postnatal ward experience was terrible, midwives had little to no empathy, shockingly brash and rude considering how vulnerable women are post birth.”
3.6.3 Comfort of the environment
Comfort of the environment was raised in the context of post-birth experiences on postnatal wards. Negative feedback included a lack of space; sensory issues including temperature and lighting; noise from machinery and other patients; lack of accessible shower facilities; and feeling disrupted by staff. The environment was reported to have a negative impact on their babies and partners, along with concerns raised that their own ability to recover after delivery was inhibited by the environment.
“The postnatal ward was the most unrelaxed environment and did not aid recovery and recuperation — I couldn’t wait to leave.”
“Also way too many interruptions too many times a day and night on PN ward – rest basically impossible.”
“I found the maternity recovery ward to be a really challenging environment. Space was incredibly limited on the ward, meaning certain elements of my recovery and breastfeeding journey were complicated.”
“The postnatal ward is absolutely boiling. Someone next to me had a room thermometer — 28 degrees!”
“My experience on the post labour ward was very poor; how this environment is conducive to recovery is beyond me. It was incredibly hot, loud and uncomfortable. The postnatal wards are horrible — from the somewhat calm and peaceful labour ward to the noisy and flustering postnatal ward is shocking. Babies screaming, extremely cramped spaces.”
“Facilities at [location name] for postnatal not fit for purpose — small bays and lack of privacy in shared bays. Overnight lighting is intrusive and space is limited. Postnatal experience was awful based on other patient behaviour. Facilities for birth partner are awful especially given the level of support they provide to take pressure off clinical staff.”
“I found the ward extremely hot and the baby was put in a woolly hat — the room was much hotter than the recommended room temperature for babies, especially with hats on. I questioned this but was dismissed by the midwife.”
“If a woman needs to stay in hospital for more than 24 hours after the birth of their baby, they should be offered a private room to get them off the postnatal wards. They are far too noisy with new mums and babies, machines, bay lights, midwives checking on mums and babies etc. I had to stay in for 4 nights after the birth of my baby (I had already been in for 4 nights trying to be induced before my c-section) and I was left on the postnatal ward for the first 3 nights.”
“There was no seat in the shower — it was difficult to shower after having a C-section, I really struggled.”
“The hospital was disgustingly hot and made me feel really ill. The heating was on (with no thermostat) but the windows were open.”
“Ward rooms should be air conditioned.”
A small number of noteworthy comments highlighted how overwhelming the environment had been for neurodivergent patients and caused significant distress.
“Needs to be more understanding and awareness of the birthing and recovery process for an autistic person. The recovery ward was horrendous for me and despite asking many times for a separate room wasn’t given one, even when empty for most of my stay.”
“I told them I had ADHD and all of the other women and babies around me and monitors beeping were really over stimulating and causing me stress and I was ignored. I genuinely feel this horrific aftercare is what caused me to have postnatal depression.”
3.6.4 Contact with baby
Patients felt it important to have physical contact with their newborn baby and to be offered support with this. Where this did not happen and/or the support was not given, patients experienced distress, which could negatively affect their mental health.
“I was adamant that I wanted to have skin to skin as soon as my baby was born by C section but got told that they didn’t do that at [location name].”
“My biggest problem with everything was the 2 hours in theatre after my baby was born and I don’t have a complete answer as to why I missed the first 2 hours of my baby’s life. And it deeply upsets me that I missed it — I didn’t hold him first, feed him, change him first. And I haven’t ever been informed as to why.”
“One thing I didn’t like about the postnatal care straight after my c section — they never really allowed me to bond with the baby, they took me straight to the ICU.”
“I wasn’t offered skin-to-skin contact, despite it being explicitly stated in my birth plan. It was actually the anaesthetist who recognised my desire for skin-to-skin and communicated this to the midwives on my behalf.”
Other feedback focused on patients being unsure as to why staff were dismissive of, or had not facilitated, their wishes relating to contact with their baby. This left patients feeling disappointed that this first contact opportunity did not occur as expected.
“Every time a midwife saw me asleep with my baby next to me or on me asleep in the bed they would wake me up and move him to the cot where he would wake up and scream. The beds should allow bed sharing as that’s the only way my baby would sleep! Bedsharing is safe if done properly and midwives just need to give guidance on that.”
“Despite going in alone and having this amazing support during labour they decided to allow family members in without asking 5 minutes after. This action ruined my hour of bonding.”
“One of the nurses on the overnight shift had a terrible attitude which has left me feeling upset even now. As there was no room on the postnatal ward, I was placed in a premature ward (the ward which has a nursery). My baby was crying and needed to be handed to me from the next to me cot (I had had a c section so couldn’t move). After pressing the button for help, she came and asked ‘what do I want’ abruptly and proceeded to talk to me very patronisingly when trying to breastfeed and talking to me like I was stupid, which caused me to become very upset. I only wanted to hold, comfort and feed my baby and wanted to tell her to leave me alone but couldn’t as I needed assistance as I couldn’t move. It was like I was an inconvenience when I was told to buzz if I needed anything — this only made me feel like I couldn’t.”
3.6.5 Being kept informed
What does the quantitative data tell us?
51% said after their baby was born they ‘completely’ had the opportunity to ask questions about their labour and birth (c19)
of those who said they stayed in hospital after the birth or required hospital care after a home birth, 61% said in hospital they were ‘always’ given the information or explanations they needed (d4)
Numerous examples were given of patients feeling they were not informed following birth as to what had taken place during delivery. This was especially evident in cases involving complications, where patients expressed a desire to be promptly told what had happened and why. In some cases, patients had been completely unaware that there had been health concerns relating to themselves while they were in hospital until contact was made after discharge.
“After the C-section there was no communication between the doctors and me about the birth or the health condition of my baby. We didn’t even know that he had been born.”
“Wish the doctors/nurses would have explained in more detail why I needed what I needed. I wasn’t told how much blood I lost, was just told I needed 2 blood transfusions.”
“We had great maternity care at [location name] barring a couple of things — forceps were used during a planned C section but we weren’t told why, nor is it mentioned in our hospital notes. This has affected the shape of our baby’s head. Discharge was a long delayed process and the midwife was ready to discharge us in the middle of the night but we requested to delay by a day so we could travel back home with a newborn safely. We weren’t at the time advised that massive postpartum haemorrhage was a significant concern. Even though they kept me under monitoring and did an iron infusion, we were not clearly communicated as to why this had happened. Only a few weeks postpartum we received a letter about it stating they were looking into the learnings. We still have not heard back on the outcome of that review.”
“I also contacted the after birth team about my birth and they explained my birth very well. I only found out that my baby’s heart rate kept dropping because the cord was round his neck three times — I was never told this from doctors whilst I was in hospital.”
“I was not made aware my daughter was jaundiced despite it being written in my discharge notes.”
3.6.6 Visitors
What does the quantitative data tell us?
of those who said they stayed in hospital after the birth or required hospital care after a home birth, 72% said their partner or someone else close to them who was involved in their care were able to stay with them as much as they wanted (d6)
Feedback about visitors in hospital at this stage of the pathway highlights the challenge of meeting competing needs. On one hand, there is a strength of feedback that visiting restrictions should be relaxed, noting that greater flexibility would better support patients, particularly given reduced mobility and the impact on their mental health. On the other, there is evidence that other people’s visitors had negatively impacted patients’ ability to rest and recover after delivery, through disruptions such as noise.
Flexibility
Patients expressed a strong desire to have visitors with them while in hospital, usually stated to be partners or husbands. In a similar vein to the sub-theme ‘Presence of birthing partners,’ patients described partners/husbands having to leave the hospital soon after delivery due to visiting rules, with an example of a patient self-discharging as a result of feeling unsupported. Where partners were able to stay, patients highlighted the significant impact this had and reflected comments where it was felt this could have made a positive difference to their experience.
“My partner was unable to stay due to rules and as a result I self discharged 2 days post birth as I was receiving no help from the staff to care for my newborn.”
“I wish my husband was allowed to stay overnight which I think would have made a big difference.”
“We felt very supported and we appreciated that my husband could stay a couple of nights with me to support the feeding plan — this was so important to us and got us started on the right track.”
Patients struggling with mobility following birth felt their needs were heightened particularly at night times, when accessing support from staff was challenging. It is in this context that a need for visitors to be present more was shared, to compensate for the lack of staff support experienced at night. Note there are links between this feedback and insight shared within the sub-theme ‘Staff proactivity and responsiveness’ soon after delivery.
“A huge benefit was allowing partners to stay — without this it would have been horrific as no midwives were available for simple tasks.”
“It’s terrible partners can’t stay overnight. I really needed my husband after my c-section and struggled without him.”
“I think it would be better if arrangements were made for the guardians of caesarean mothers to stay close by at night after delivery.”
“The only thing I do think should change at my chosen hospital is partners being allowed to stay with you after a c section.”
“I felt difficult being on my own the first night after a c section especially because my baby was born at 4pm and it took me a while to be able to stand up. I would recommend letting the birth partner stay for the first night to support mum.”
Disruption
In contrast to requests for more flexible visiting, some feedback highlighted issues caused by visitors. There were mentions of noise but patients also described feeling unsafe due to the behaviour of other patients and their visitors. There were concerns raised about the ability of the setting to manage challenging situations, which could leave patients feeling less safe.
“After delivery, recovering in the ward was difficult due to antisocial behaviour from neighbouring patients. We were only asked how comfortable we were in the ward once we left but I wished we were asked during our stay if we felt safe by the people staying around us.”
“The wards were so loud and busy and none of the other patients had any respect for anyone around them. The midwives should be setting rules for this — e.g. don’t bring curry into the ward at 1am!”
“Antenatal and postnatal wards are inhumane. They are noisy, not clean enough and not restful enough considering the need for relaxation and rest in preparation for birth and for nurturing a newborn after a great physical feat. In particular for women who have had a traumatic birth.”
“Very glad to hear partners are no longer allowed to stay 24h at [location name]. I did not feel safe at night as the patient opposite was being verbally abused by her partner during the night. I informed the staff on 2 occasions and no one came in the room. Another night, I asked the patient’s partner to please keep the noise down — I had not slept for a few days as the ward is very noisy and my baby was unwell, it was 4am and he was on speakerphone laughing with friends. His response was ‘who the f*** are you talking to’.”
3.6.7 Feeding support
What does the quantitative data tell us?
84% said their decisions about how they wanted to feed their baby were ‘always’ respected by midwives (e2)
63% felt midwives ‘always’ gave them enough support and advice to feed their baby (e3)
57% said in the four weeks after the birth of their baby they ‘definitely’ received help and advice from a midwife about feeding their baby (g14)
Spanning examples of both breastfeeding and formula feeding, patients expressed unmet needs to feel supported, encouraged and given practical assistance to help with feeding their baby soon after delivery/before discharge.
Feeding choice
There was feedback from patients regarding support and encouragement received from staff, both in the context of choosing to breastfeed and formula feed. Irrespective of which feeding method was chosen or preferred, it was inferred that patients would appreciate staff supporting their preferences and being sympathetic to their individual circumstances.
“I completely understand why it happened, but I wished that my feeding preferences weren’t talked about every visit. I expressed from Day 1 that I wanted to exclusively bottle-feed, and being asked about it a few times at the beginning was fine. But being asked even at the very end felt annoying.”
“The midwives pushed me to use formula and then baby didn’t want to breast feed.”
“I was also accused of not feeding my baby enough whilst he was breast feeding and felt pressured to bottle feed when he had jaundice.”
“I can’t breast feed due to a mastectomy. I had no support to formula feed my baby. I had a few patronising looks from midwives when I said I was formula feeding.”
“More help and support after birth when asking for help with breast feeding.”
“I didn’t really know what to expect from the first 24 hours. My baby was quite sleepy therefore I didn’t breastfeed enough in the first 24 hours therefore she lost over 10% of her birth weight. I would have appreciated someone advising me to feed every 3 hours or so which no one said.”
“I feel once on the ward if you are bottle feeding, specially as a first time mum, you should be given advice on how often / how many ounces you should be feeding your child.”
Positive experiences with feeding support were shared by a few patients, although lacked detail as to what made this support particularly effective.
“The aftercare was excellent with lots of help and support with feeding when my baby was following the vulnerable baby pathway.”
“I was particularly impressed by the infant feeding team support this time around, much improved and very supportive.”
“The midwives on the post natal ward were sooooo helpful in helping me with feeding!”
Practical support to breastfeed
Patients felt that the practical help and support with feeding, particularly babies latching on for breastfeeding, was not always sufficient. Insufficient support with breastfeeding could also lead to patients switching to bottle and/or formula feeding or returning home from hospital without being able to breastfeed. The feedback also highlighted the need for feeding advice to be timely, which was not always the case.
“In hospital after my emergency c section, my baby wasn’t feeding well, and the staff were too busy to help, or spend time with us to assess her feeding.”
“When on the ward after giving birth, communication was poorer and I didn’t receive any support with breastfeeding as they assumed I was doing okay. By day three my baby was on a stage 2 feeding plan and these midwives offered a lot of support/tips which would have been good on day one.”
“Wanted to breastfeed but had no support in doing so so I had to use formula. After I gave birth I hadn’t been told how to position baby for breastfeeding, my baby had problems with latching. After a few days we asked the feeding team for help.”
“I wish I had more help with breastfeeding as I was struggling and I was just told to pump.”
“I requested breastfeeding support in the postnatal unit but was fobbed off, told they might not be working because it’s a weekend. My baby ended up losing 14% of her birthweight and was almost admitted and fed through an NG tube as a result.”
“I waited all day for someone to come and speak to me about feeding as I was formula feeding — no one came and I was sent away with a leaflet instead.”
“I feel I wasn’t listened to when expressing concerns about my baby not feeding well.”
“The midwife was happy to discharge me even though my baby hadn’t fed well through the night. He was on the hypoglycaemia pathway, so as blood was being taken the doctor ran a bilirubin test and it was picked up that his bilirubin levels were high which explained why he wasn’t feeding well.”
There were a small number of positive experiences where practical support had both enabled breastfeeding and built patient confidence. Even here, patients could still have outstanding questions which suggested information provision following assistance could be improved.
“I needed lots of support to start breastfeeding and [name], one of the team on the postnatal ward, helped me so much. If it wasn’t for her help I wouldn’t have had the confidence to continue trying to breastfeed as I wanted.”
“The support for feeding latch was very helpful — more info on quantities of milk would have been helpful.”
3.6.8 Wider hospital issues
Multiple examples were shared in feedback which pointed to issues with the hospital facilities, environment and provisions, beyond matters specific only to maternity care.
Cleanliness
Feedback about the cleanliness of the hospital environment was negative. Some patients reported that rooms, wards, and toilets were dirty. Issues echo insights shared within ‘Staff proactivity and responsiveness’ where patients were left with dirty bed linen.
“While in the post-natal ward the cleaners knocked over a bin with vomit in. The vomit came into our room and it took them a while to clean it up. I feel like this needs to be addressed as this was not hygienic especially when there are new born babies around.”
“My experience on the post labour ward was very poor; how this environment is conducive to recovery is beyond me. It was incredibly hot, loud and uncomfortable. Toilet/shower facilities were dirty.”
“The floors in the wards were disgustingly dirty!”
“Guest toilets were gross (forced to use it when the other toilets weren’t available). On the upside the ward itself was cleaned regularly (washrooms could do with a facelift but clean considering the traffic).”
Food and drink provision
Feedback on the quality and variety of food was mixed, with some patients reporting positive experiences, while others suggested improvements were needed including a need to improve confidence that dietary requirements were both understood and catered for.
“The only complaint is the food, it was absolutely shocking!”
“I’m gluten free and vegetarian and found it a nightmare to be able to eat anything properly on the post natal ward. The menus are confusing, staff were clueless on dietary requirements even though they were ordering and preparing the food for you.”
“Hospital food is not good — the rice is very hard and not fully cooked. You should improve the food please.”
“Great food choices and tasted nice.”
“I have coeliac disease and must follow a strict gluten free diet. I was very stressed about the possibility of gluten exposure during my induction/labour. I had to avoid eating anything I didn’t bring from home.”
3.7 Discharge
Within this section, feedback was shared in the context of a hospital setting as opposed to home. This was explicit in some feedback and/or inferred in others.
3.7.1 Timing
What does the quantitative data tell us?
of those who stayed in hospital after the birth or required hospital care after a home birth, 37% said the day they left hospital their discharge was delayed (d2)
Feedback contained contrasting experiences around hospital discharge. Some patients felt they had been delayed, while others were discharged earlier than they expected and/or before they felt ready. It could be inferred from the experiences shared that staff workload and/or the busyness of the hospital was believed to be a reason for either scenario.
Where discharge was delayed, patients described being given unreliable information around when they would be leaving or were left unaware of the reasons for the delay. Where reasons were provided, these typically indicated staff shortages or waits for paperwork to be completed.
“The discharge after birth was unnecessarily delayed and long. I was told this was staffing but the communication could have been better — i.e. I was told someone would come in a few hours, and 6 hours later I was still there struggling to get any update.”
“My discharge was delayed due to nurses not being available and them telling me a time and not turning up, and me having to keep asking.”
“Our discharge was delayed due to the doctors carrying out a ward round but not physically seeing patients (us) and medical plans not being communicated to the midwife looking after us.”
“The discharge process took 6 hours for paperwork to be ready!”
“I waited 10 hours for discharge and they wanted to discharge me finally at 1am after my husband had just gone home.”
“Was told I was being discharged so packed my bags and then told I had to stay another night.”
“I was told I’d be discharged following my final course of antibiotics at 3pm the day after my birth but was not discharged until 11pm and was left waiting still sat in the blood from my birth the previous day.”
Discharge could also be delayed by waits for medication.
“We weren’t discharged until late in the afternoon, despite being ready since 10am. It would have been nice if we could have been prioritised, given that we were fully ready to go, just waiting for medication.”
“My paperwork showed the discharge was approved at 10 but we couldn’t leave the hospital until around 1900 because of the incredible delay in getting antibiotics dispensed.”
“Discharge was delayed waiting for medications from pharmacy for baby.”
“Discharge should be done more smoothly. Medications are not always given when leaving. Pharmacy service and hospital don’t work together — very poor communication and they work extremely slowly.”
“Only negative is discharge took hours — waiting on pharmacy for meds.”
In other cases, patients were surprised that they were discharged early, feeling rushed and reflecting that this did not always feel safe or in their best medical interests. It is noteworthy that an example was shared of the impact being a quick return to hospital.
“I was also discharged from [location name] without carrying out assessments on the baby and I had to rush back the following day to carry out these checks.”
“We were discharged from the hospital after only 12 hours which was very early and stressful for us — we were not ready as first time parents yet.”
“I felt rushed to discharge.”
“Feel the discharge is very quick especially as a first time mum.”
“As a first time mother, it would have been less stressful if I stayed in the hospital longer after my planned c-section.”
“Wanted to discharge me the next day when I told several staff members I wasn’t ready — I was in a lot of pain, could hardly walk, didn’t have support at home. All fell on deaf ears and I was kicked out of an empty ward so it wasn’t like they needed the bed.”
3.7.2 Medicines management
Discharge from hospital following birth was a key point in care where issues receiving medication occurred. This included being sent home without pain relief; being sent home without other medication that patients deemed important; or lacking the relevant information needed regarding medication and side effects. The impact was not clear in several examples, though where it was observed this included avoidable pain and, for some, further health complications.
“I was not given adequate pain relief to take at home which led to 48 hours of suffering and poor ability to care for my new baby.”
“Sometimes medicines are not prescribed — they just tell us to buy them, so they are costly. If possible, prescribing all medicines would mean there are no worries for us to buy them.”
“I also was not given iron tablets which were needed — my doctor prescribed these at a later date when I got dizzy.”
“Following my c section I wasn’t given pain medication regularly as per the prescription. Again I had to advocate for myself to ensure I received the care I needed.”
“I was also severely constipated and wasn’t given any laxatives to go home with. I didn’t go to the toilet for 12 days after my c-section — nobody told me the painkillers they were giving me would make me severely constipated and cause severe pain.”
“After my C-Section I was discharged without any blood thinners, only stockings. I asked the discharge nurse why everyone else on the ward were prescribed anticoagulants and not me, and they said that I only needed stockings.”
3.8 Follow up care and support
This section of the report includes feedback about postnatal care experiences in the home and community, including primary care. Where possible, reference is made to the care setting to provide context and attribute feedback.
3.8.1 Care in the community
What does the quantitative data tell us?
of those who contacted a midwife/midwifery team after birth, 75% said they were ‘always’ given the help they needed (g2)
75% said they were ‘always’ involved in decisions about their postnatal care (g1)
61% said they ‘saw or spoke to a midwife as much as I wanted’ (g4)
33% said they would have liked to have seen or spoken to a midwife ‘more often’ (g4)
42% said at the postnatal check-up (around 6–8 weeks after the birth) the GP ‘definitely’ spent enough time talking to them about their own physical health (g17)
Care in the community following delivery was typically negative in sentiment when describing unmet needs in the context of home visits as well as postnatal checks at the GP.
Home visits
Patients conveyed a strong preference for postnatal appointments to be home visits. It was explained to be physically difficult to attend appointments outside of home after giving birth, particularly following c-sections, for example being unable to drive. Comments inferred that if home visits were not offered then care might not be accessed at all.
“The 3–4 day postnatal check and bloods — they wanted me to go to [location name] hospital from [location name]! But I had to complain and someone visited me instead as I could not drive 3 days postpartum. Ridiculous!”
“Two of the home visits were switched to the hospital due to understaffing which I didn’t necessarily like so soon after bringing the baby home.”
“I was told I could go to the midwife centre behind the [location name] Practice at any point. My scar was infected and my daughter was projectile vomiting. I pressed the door bell 5 times waiting for someone to come and help me. I waited for 40 minutes (I heard the door bell go off). I went outside and I could see them all looking at me so I went back in and pressed the bell. No one came to see me.”
“The only thing I would say is the aftercare could have been better — they wanted me to go to them when I don’t drive etc. I think those should have been home appointments.”
Some comments indicated that there had been a lack of clarity about what care would be provided after hospital discharge and that patients did not know who to contact if they had questions or concerns. As a result, patients described feeling unsupported.
“I thought I should have received a phone call at home after pregnancy about c section recovery. I did with my first child — to check on healing and pain symptoms.”
“The support of health visitors seems to vary from mother to mother. I only had 2 visits in the first few weeks of birth but others have regular visits months down the line and I’m not sure why.”
“After being discharged, I got no support — no midwives came until I rang up and they came out 5 days after. They said I’d been missed from a list. I felt so unsupported.”
“I got handed over to community midwives who were supposed to come and check my blood pressure every other day and I didn’t see anyone.”
“The support following birth on discharge from the ward wasn’t great — whilst at home, support was also poor. I had little information about midwives who would support initially and I was discharged whilst my son had several unresolved issues (which needed hospital visits).”
GP postnatal check
Patients gave feedback as to the focus of GP postnatal appointments. Comments typically described appointments as ‘rushed’ and that they felt this was a tick box exercise, with concerns that minimal attention was paid to both the patient and/or their baby’s health. This led to suggestions around what should be covered in GP postnatal appointments, for example a need for more focus on the person who gave birth.
“Postnatal check up at the GP wasn’t good at all — the GP didn’t care and was only there to tick boxes.”
“My 6 week follow up with the GP was a 2 minute telephone call which was extremely inadequate. If I didn’t have medical knowledge I would have been lost.”
“I would have liked the 6 week check up to be a bit more thorough as I felt like the GP was rushing through a checklist. Also postnatally I think there should be more checks on a woman’s physical health, as currently it feels like a very tick box exercise when discussing this at the 6 week check.”
“I still think the GP postnatal check is the poorest part of my care. Just felt literally tick boxy.”
“I did feel very rushed in my GP check up.”
“I also felt I was rushed in my 8 week checkup with the GP with her specifically stating she didn’t have enough time.”
“The GP check up was barely 5 minutes and didn’t cover any key areas expected. I would maybe have liked to have had a midwife check up or conversation at 6 weeks to check in on baby development and recovery.”
“I tried to discuss prolapse with my GP at the 9 week check but they didn’t have time.”
“My postnatal care was local to [location name] and my GP at [location name] medical centre is by far the worst GP surgery in the country, hence the negative feedback for the GP. They do not do a proper postnatal check up and they don’t listen to your concerns about women’s postnatal health at all.”
“GP 6–8 week checkup was not what I expected. No physical exam on me to check healing, and poor contraception support.”
“I felt the GP check up for me was very quick and minimal. They were unaware of the type of birth I had, which should have been on notes available. There was no offer to check my wound despite me saying ‘I think it is’ when they asked if it’s healing nicely. I felt my lack of confidence in my answer should have prompted them to check.”
Some patients shared more specific concerns about their GP’s lack of knowledge of postnatal health and felt that they had received incorrect information or guidance.
“I want to emphasise the lack of support available postpartum. In the first four weeks (when we are monitored by the professional team), everything went normally. The breastfeeding problem started later: mastitis. I want to highlight the lack of knowledge and support from the GP regarding this issue.”
“The GP is not reasonably informed on women’s health and postnatal care. I was refused a diastasis recti and pelvic floor check — in fact the doctor I saw advised I didn’t need to worry about pelvic floor health due to having a c-section, which is dangerously misinformed.”
“My only concern is about the GP not taking seriously the asymmetry issues of my baby. At the 8 week check up I was told it would resolve on its own but of course it hasn’t 1.5 months later. I wasn’t provided any advice on how to manage it or what to do if it doesn’t get better.”
Other comments shared experiences of delays to their GP postnatal check which caused concern for the patient and also had impacts on the health of their baby, for example late access to first vaccinations.
“My GP appointment was disappointing. We were not seen until my daughter was nearly 11 weeks old, which was not only late for her 6 week check but also meant her first jabs were 3 weeks late too.”
“My baby is nearly 12 weeks and we have not yet had our postnatal checks. I called the GP to raise my concerns when I got the appointment date at around 3 weeks postpartum. No one seemed to care — no apologies — and was pretty much told it is what it is. No appointments available, even though the surgery’s policy has always been that you cannot book an appointment more than 3 weeks in advance, so I was confused as to why I had a 9 week wait.”
3.8.2 Feeding support
There was variation in experience of feeding support postnatally. Feedback did not always specify where or how support had been accessed, although some mention was made of community midwives. Concerns were shared as to the expertise and knowledge of staff providing feeding support. Notably, feedback related to both breastfeeding and formula feeding.
“Breastfeeding advice in the hospital was great, but post leaving the hospital I did not get much help from the midwife or health visitor to help in my journey.”
“My feeding journey was and still is incredibly challenging and I have received no support or follow up regarding this.”
“Felt bullied by community midwife about not exclusively breastfeeding — totally unnecessary aggro for a sleep-deprived first time mum.”
“I was sent home with my baby with feeding problems — baby wouldn’t stay latched, home breast pump was useless — so I was left with my only option being to formula feed.”
“A volunteer at [location name] was called a feeding expert. She isn’t. That’s okay but just call her a volunteer and don’t advertise feeding support because for vulnerable mums she is in a position to actually cause damage. When you’re on the edge.”
“I was very nervous about being able to feed my baby postnatally. My community midwife was very reassuring.”
“[name], who came out to support me with feeding after my daughter was born, was a font of knowledge and solved my issues immediately as well as being amazing emotional support.”
3.9 Other observations
Below is a list of other topics commented upon in the data that were noted during the analysis process. There was a lack of volume of comments or depth and detail to inform themes and sub-themes, but the suggestions are noteworthy.
lack of information about pregnancy related conditions
receipt of c-section date allocation less than a week before allocated date
harvested colostrum misplaced by staff and no audit trail kept
report of being touched inappropriately by staff member
discharged from diabetes midwifery care without understanding why
satisfaction with extended skin-to-skin contact time post birth
lack of suitability of toilets in antenatal clinics related to pregnancy needs
difficulty understanding staff due to accent or poor English
4. Conclusions
This is the first national qualitative analysis published for the Maternity Survey, and this report demonstrates the value of inviting respondents to share their experiences in their own words across the maternity pathway. This approach has enabled respondents’ voices to shape the focus and depth of the findings, highlighting what truly matters to them and what impacts their experience of care.
Overall, the report shows that while there is a strong sense of appreciation and gratitude for NHS maternity care, significant variability exists. Systemic pressures and inconsistencies in care delivery undermine reliability and at times, safety. These insights underline the importance of addressing structural challenges alongside improving relational aspects of care.
Reflecting on what constitutes high-quality maternity care, the analysis points to a clear gold standard for experience: care that is compassionate, respectful, and responsive, delivered by staff who listen and communicate effectively. Continuity of care emerges as a cornerstone — building trust, supporting personalisation, and enabling shared decision-making. Equally critical are timely and safe clinical practices, consistent and accurate information provision, and proactive mental health support. High-quality care must also be equitable, tailored to individuals’ needs and free from discrimination.
The findings also highlight the need to alleviate systemic pressures on staff, as workforce shortages and capacity constraints directly impact care quality. Addressing these pressures is essential to enable staff to deliver the gold standard of experience of care described by respondents.
This report offers a comprehensive view of improvement opportunities though has limitations in determining which matter most and would make the biggest impact for patients. Triangulation with other datasets and targeted engagement activities are recommended to identify high-impact priorities. Ongoing listening and involvement of service users will be vital to ensure that national and local improvement efforts deliver the most meaningful gains.
5. Appendix: Methodology
Survey methodology
All NHS trusts providing maternity services that had at least 300 live births during the sample months were eligible to take part. Women who gave birth between 1 and 28 February 2025 (and 1 and 31 January 2025 if a trust did not have a minimum of 300 eligible births in February) were invited to take part in the survey. Trusts with fewer than 300 births were able to take part in the survey on a voluntary basis.
Fieldwork took place between April and July 2025. Responses were received from 16,755 people — an adjusted response rate of 39%.
Qualitative analysis
Thematic analysis was undertaken to achieve a deep understanding of the findings from the open questions asked in the survey. This sought to facilitate reflection and learning across services delivering maternity care across England.
To analyse qualitative data, the standard six steps of thematic analysis were used to identify patterns of meaning within the data and explore commonality and contrast — see Figure 1.
Figure 1: thematic analysis approach
This image shows a linear process diagram illustrating the stages of qualitative data analysis. The stages are presented from left to right within a long arrow, indicating progression through the analysis process.
The stages are:
Familiarisation – becoming familiar with the data
Initial coding – identifying and coding key features of the data
Generating themes – grouping codes into potential themes
Reviewing themes – checking and refining themes against the data
Defining themes – clearly defining and naming the final themes
Final analysis and report writing – producing the final analysis and written report
The arrow indicates that these stages follow a structured sequence from initial engagement with the data through to final reporting.
The results of the thematic analysis have been reviewed and are shared in context of the relevant quantitative survey findings. This exploits the value of both the quantitative results, which tells us the proportion of patients feeling a certain way, and the qualitative findings, which tells us why people feel that way. For example, where there is a high degree of agreement/positive experience evidenced in the survey data, the thematic findings offer an opportunity to understand why there was not 100% agreement/positive experience and therein, where the opportunities lie for reflection and learning.
Sub-group comparisons
Sub-group comparisons were not the focus of the analysis. Where variations were observed in the national sample, this has been included within commentary. It is recommended that further focused sampling would allow for in-depth exploration of how experiences of maternity care may vary for different groups. Observations included will unlikely be exhaustive due to the national sample and focus.
6. Appendix: Sampling approach
9,594 written responses were collected in total, meaning 57% respectively of the survey sample provided qualitative data in answering the open ended question.
Qualitative data cleaning
Before sampling, further data cleaning was carried out to identify and remove extremely short comments which were of no analytical value, for example those which simply stated ‘No’, ‘N/A’ or consisted of a single character.
50 comments were removed in this way, leaving 9,545 comments for the sample to be drawn from.
Sampling
It was decided to sample each of the surveys separately so that all patients with viable response to an open question had the potential to be included in the final sample for analysis.
To ensure a robust approach to sampling, a purposive sampling approach was taken. This is an established best practice technique when analysing qualitative data, as it ensures that the data has enough diversity across the most relevant criteria to allow the impact of the criteria to be explored and compared. For example, if age is a criteria, including responses from all the different age groups in sufficient volume means that differences in experiences between age groups can be explored.
The criteria chosen to sample on were the age, ethnicity, and deprivation level of patients, as these were key demographic groups recorded in the data. A sample matrix was drawn up to establish how many comments from each of the demographic groups were to be included in the analysis to allow for sufficient coverage.
In addition to the three key demographic groups a minimum of 30 comments were included on all other characteristics including sexual orientation and home births for instance. Please note that as there was a low volume of data from patients aged 16–18, all of this cohort were included in the sample. The breakdown of the volume of comments in the sample by these different criteria is provided below.
Once the original sample of 675 comments had been analysed it was seen that data saturation had been reached, i.e. no new themes were emerging from the data. Had this not been achieved, additional comments would have been added to the sample as necessary, in line with best practice in qualitative analysis.
Table 1: number of comments in analysed sample per characteristic
Characteristic
Sub-group
Number of comments analysed
% of comments analysed
% of comments overall
Age
16–18
13
2%
0.1%
19–24
39
6%
5%
25–29
124
18%
18%
30–34
255
38%
38%
35+
244
36%
39%
Ethnic background
White
453
67%
72%
Mixed
30
4%
2%
Asian
78
12%
11%
Black
35
5%
5%
Other
30
4%
1%
Not given
49
7%
9%
Deprivation level (IMD Quintile)
1 (most deprived)
114
17%
17%
2
144
21%
19%
3
153
23%
21%
4
128
19%
21%
5 (least deprived)
133
20%
21%
Blanks
3
0%
1%
Gender different as that assigned at birth
Yes
31
5%
1%
Sexual orientation
Heterosexual or Straight
574
85%
92%
Other
8
1%
1%
Gay or Lesbian
31
5%
1%
Bisexual
34
5%
2%
Prefer not to say
25
4%
3%
Not given
3
0%
1%
Birth type
A vaginal birth (no forceps or ventouse suction cup)
271
40%
41%
An assisted vaginal birth (e.g. with forceps or ventouse suction cup)
99
15%
12%
A planned caesarean birth
137
20%
22%
An emergency caesarean birth
163
24%
25%
Not given
5
1%
1%
Home birth
Yes
33
5%
3%
7. Glossary
BP Blood Pressure
C Section Caesarean Section
CAT 1 / Cat. 1 Category 1 Caesarean Section — performed when there is immediate risk to mother or baby