
A critical aspect of providing effective care and treatment to people with mental health needs is understanding the likelihood of harms occurring to the person or others in context of their mental ill health. This includes working with the person, their family and support network to put plans in place to reduce the likelihood of the harm or mitigate its impact.
The most important strategy to reduce risk of harm is to provide effective personalised care and evidence-based treatment.
Thus, safety assessment, formulation and management planning is integral to each principle and action in the Mental health personalised care framework. It must not be seen as a separate task and activity to planning and delivering care and needs to be directly linked to from or part of a person’s care and support plan.
Personalisation, continuity of care, prioritisation of a therapeutic relationship and engagement are key enablers of safety. Professional curiosity, investment of time in developing trusted relationships, understanding the person and their strengths, collaboration across care settings, partners and agencies and consistently involving the person and their support network are all fundamental for effective safety management and planning.
Safety assessment and management are carried out within several legal, statutory and governance frameworks which are signposted throughout this guidance. Professional should be aware of these, operate within them and access the relevant expertise and advice when needed.
Throughout this guidance we use the term ‘safety’ in line with recent suicide prevention guidance, but recognise that other relevant resources may use the term ‘risk’.
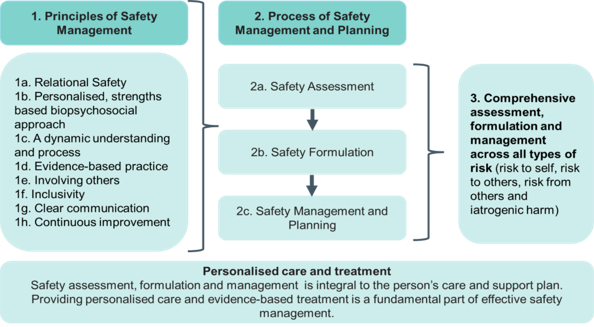
Developing safety assessments, formulations and management plans across all types of risk
Safety management requires the development of an assessment, formulation and safety management plan that considers risk to self, to others, from others and from iatrogenic harm together and applies key principles of safety management. This process and the principles that inform safety management are set out in this annex and illustrated in figure 1 below.
Figure 1: The process and principles that inform safety management
Principles of safety management
The principles below apply across all settings and types of risk and inform how comprehensive safety assessment, formulation and management is carried out with consideration of all risks of harms together.
Relational safety
A relational approach to safety should be prioritised to improve clinical outcomes. This includes focus on building and maintaining a trusting, collaborative relationship, supporting engagement and continuity of care.
When people feel heard and that their views are valued, they are more likely to trust and engage with mental health services. Co-production supports relational safety. The process of understanding relevant risks, formulating when related harms may occur and creating a plan to mitigate them must be co-produced with the person and their chosen support network.
Acknowledging and working with any difference in views about risk between the person, their support network and practitioners is important. Balancing the development of a therapeutic relationship with the need to support the person’s safety and potentially that of others is nuanced. It requires time and sufficiently skilled and culturally competent teams.
If the person is too unwell to meaningfully co-produce their safety plan, this should be noted and ongoing efforts made to promote their voice and involvement in all aspects of their care and safety-related decisions.
There will be times when care and treatment decisions to manage safety go against the wishes and views of the person, particularly when a symptom of their mental health condition is no awareness of when they are unwell and because of this they do not want treatment. It is particularly important to communicate clearly and transparently to the person why the decision was taken and record the different views to maintain a trusted relationship, including authenticity, empathy and curiosity about the person’s perspective.
Personalised, strengths-based biopsychosocial approach
Management of safety must be personalised. It should build on the person’s strengths and be part of a broad biopsychosocial approach aimed at improving overall wellbeing by considering biological, psychological and social aspects of needs and care together.
Formulation can take time to bring together an understanding of the interaction between illness, a person, their life and the environment in which they live. To help the person best manage and mitigate any risks, professionals need to get to know them, understand what factors could lead to them being unsafe and put in place strategies to reduce the likelihood of them becoming unsafe or to mitigate potential harms to themselves or others. A strengths-based approach throughout formulation and management that considers how the person’s strengths can best be supported is essential.
The process is strengthened by trusted relationships, the involvement of the person’s support network and collaboration between all those involved in their care.
A dynamic and understanding process
How safe a person is at any time will be influenced by a range of factors and these factors will likely change over time. Therefore, the process of formulating and planning how to best support the person’s safety (and that of others where relevant) needs to be dynamic and ongoing. Safety assessment should be regularly revisited and a person’s formulation and safety plan must be updated to reflect changes in their needs and circumstances. This includes when the person’s circumstances or their mental health needs change and, importantly, when an incident of harm occurs. Review is an opportunity to reflect with the person and those involved in their care about what precipitated the incident, what did and did not help in that context and how any learning can be used to better support the person in future.
Evidence-based practice
Approaches to safety management and planning should be informed by the latest research including intelligence on population-level risk trends. Practitioners need to be supported to stay up to date with changing patterns and trends in the populations they work with including intelligence and learning from research, reports, safety incidents and networks. This should be part of their ongoing continuing professional development.
Relevant research could include changes in trends or modes of self-harm, risks from illegal drugs and local supply patterns, research about risks and how they may present in specific populations, for example autistic people, older adults and men.
Given the known risk of poor outcomes for people with co-occurring substance use, all practitioners should be competent in identifying co-occurring substance use and working with partner agencies to manage the related risks. They also need to be competent in responding to changes in societal factors that can impact on risk. For example, they need to understand the ways in which digital cultures and technologies and social media can impact on safety, both positively and negatively, and take reasonable measures to educate the person and their support network about relevant risks.
Involving others
Listening to the person and involving trusted others, such as family, carers and the person’s chosen support network, is a core part of safety management and planning. Effective multidisciplinary and multi-agency working is essential; the multidisciplinary team should support decision-making around who to involve.
Wherever possible, who the person wishes to be involved in their safety management plan and how should be discussed with them when they are not in crisis or acutely unwell.
Family, carer and support network involvement can support safer and more person-centred care. These individuals often know the person best, may notice early and important signs of relapse, and are often best placed to raise concerns about risks to the person or others. They may also be the ones most impacted by changes in the person’s safety. However, their involvement must be balanced against the person’s rights to confidentiality and choice. Caldicott principles should be followed to ensure people’s information is kept confidential and used appropriately. In balancing involvement and information sharing practitioners should refer to:
- Information sharing and suicide prevention: consensus statement
- Sharing information with the police
- Confidentiality: good practice in handling patient information
Services should adopt a trauma informed approach, remain alert to safeguarding, including domestic violence and coercion, and recognise that in some cases family members may present risks or be at risk.
Inclusivity
Inclusivity requires cultural competence, attention to potential bias and ensuring practices are inclusive and adaptable (see Patient and carer race equality framework and Advancing mental health equality), particularly for marginalised groups and those with particular needs, such as autistic people and those with dementia, with reasonable adjustments made as appropriate. National guidance on meeting the needs of autistic adults in mental health services is available.
Clear communication
All communication with people should be in simple, straightforward language, avoiding jargon and complex terminology, and tailored to their individual use of additional supports, including advocacy, interpreters and reasonable adjustments.
Continuous improvement
Formulations and safety management plans should be refined and updated based on outcomes and feedback to reflect any learning. The constant focus should be how to help the person to be and feel safe.
Process of safety management and planning
Safety assessment, formulation and management should be holistic and consider all the different types of risk – to self, to others, from others and from iatrogenic harm – and how to mitigate or reduce the likelihood of harms. No one type of risk and related harm should dominate consideration at the risk of not responding to other types. For example, people who present a risk to others may also be vulnerable to self-harm, self-neglect, retaliation or exploitation by others. The section comprehensive assessment across all types of risk considers this further (see also The Royal College of Psychiatrists’ CR201: Rethinking risk to others in mental health services (2016, pending revision).
Safety assessment
Safety assessment should be carried out with authenticity, active listening, curiosity, validation, compassion and acceptance, and with the person and their support network consider:
- the person’s strengths
- historic factors, including past risk events
- changeable and current risk factors
- potential future risk factors, including specific upcoming events or circumstances
- situations in which risk may increase or decrease
- protective or mitigating factors
- what harms could occur
Safety formulation
Safety formulation is the process of bringing together insights about potential harms that could occur, the likelihood of them occurring and factors that could increase or decrease this likelihood and/or mitigate its impact.
The safety formulation maps and creates a shared understanding of the current safety concerns for the person and the changeable factors that may impact on their safety. It makes sense of the safety assessment and forms the foundation for the safety management plan.
It should be co-produced with the person and bring together the person’s insights into what makes them feel and be unsafe with those from their family, support network and other agencies (as relevant), as well as learning from historical incidents and evidence-based knowledge of factors likely to impact on safety. Importantly, it should build on the person’s strengths.
Frameworks such as the Three Ps or Five Ps formulation support safety formulation. The Three Ps considers the presenting problem, protective factors and precipitating factors and the Five Ps considers predisposing and perpetuating factors in addition. Critical to whichever approach is taken is that it is personalised and undertaken with the person and their support network.
Safety management and planning
A person’s assessment and safety formulation are only meaningful if they are used to develop a clear, specific and personalised plan to support the person’s safety and that of others. The plan considers what actions are needed including any immediate actions needed to reduce the risk of harm.
Safety management plans should include signs that a person may be becoming unwell/struggling, what helps and does not help in this context, what harms could occur if relapse is not effectively addressed in a timely manner and what can be done about them. The plan should include a summary of the risk of harms identified, the situations in which they may occur, actions to be taken by practitioner, the person and any others and in what timeframe.
The plan should set out:
- what helps the person to feel and be safe from the identified potential harms
- what factors might cause them to become unsafe
- what might be the warning signs they are feeling or becoming less safe
- what action will the person take if they begin to feel unsafe or notice the warning signs
- what action will mental health services take if the person begins to feel or become less safe
- what actions will any other agencies or people take including the person’s family and support network as relevant.
- what strengths of the person the plan will draw upon
The identified actions should be context specific and realistic.
Safety management plans may also consider advance care planning and, where relevant, will link to advance choice documents.
The person’s safety management plan must be made available to them and, in accordance with the person’s wishes, their support network, and be accessible to the care team for the purposes of direct care.
Using interoperable systems and consistent terminology to describe plans and the structure of their content or template may improve meaningful use of safety management plans especially when being referred to outside of normal service hours or when people move between services and care.
Where data sharing rules support the sharing of relevant information for direct clinical care, the person should be made aware of how local clinical records systems enable other providers and agencies to access their plan (for example, ambulance services, primary care, acute trusts on local integrated care records). If due to legislative or public protection reasons, the plan needs to be shared with other agencies without the person’s consent, they should be told and the rationale for sharing explained to them.
Services should have systems in place to receive feedback so the person’s plan can be updated with them after they have had a clinical contact outside their immediate care team.
Comprehensive assessment across all types of risk
The term ‘comprehensive assessment’ has been used specifically in the context of safety following an episode of self-harm. The National Institute for Health and Care Excellence (NICE) defines psychosocial assessment following self-harm as “a comprehensive assessment including an evaluation of the person’s needs, safety considerations and vulnerabilities that is designed to identify those personal psychological and environmental (social) factors that might explain an act of self-harm”.
However, when considering the safety of an individual, comprehensive assessment should be taken to mean that all types of risk of harm are considered together – to self, to others, from others and from iatrogenic harm – in the context of the person’s strengths. This requires that insight is sought from a range of sources to inform the formulation and management plan.
Approaches will vary according to the context and individual history of the person. The assessment may need to focus on the ‘here and now’ and be appropriately tailored to the person’s current situation. Priority may need to be given to understanding and responding to the most immediate, severe and higher likelihood harms.
Clinical judgement will be needed to determine what information may be needed now to support the person’s safety and what may be better explored later (for example, in relation to past events or less immediate risks).
Clinical guidance on psychosocial assessment advises practitioners on how to set the scene for and carry out psychosocial assessments, and the additional considerations for particular groups, including the relevance of past trauma to the approach taken.
In initial assessments practitioners will still be developing an understanding of the person and establishing a trusted relationship with them, and information will be incomplete. The safety formulation from these assessments may then inevitably have limitations. Noting how, when and by whom any limitations should be addressed (for example, more information sought or further assessment time needed) supports the iterative development of the safety formulation and management plan.
Risk of harm to self including from self-neglect
The 2022 NICE guideline Self-harm: assessment, management and preventing recurrence recommends clinical services stop the following practices:
- using risk assessment tools and scales to:
- predict future suicide or repetition of self-harm
- determine who should and should not be offered treatment or who should be discharged
- using global risk stratification into low, medium or high risk to:
- predict future suicide or repetition of self-harm
- determine who should be offered treatment or who should be discharged
The Staying safe from suicide guidance reinforces this shift from risk stratification to a more personalised approach to safety assessment that considers the person’s strengths. This along with the NICE guideline NG225: Self-harm: assessment, management and preventing recurrence and Psychosocial assessment following self-harm: a clinician’s guide support practitioners when carrying out risk assessment, formulation and safety planning following self-harm.
Self-neglect can lead to significant harm and have both life threatening and limiting impact. For example, neglect of physical health is known to contribute to the mortality gap for people living with a severe mental illness. Risks from neglect of preventable physical health conditions should not be inadvertently discounted because they lack immediacy or are accumulating slowly over time. Screening and interventions in physical health should be a core component of personalised care and support safety management planning (see Improving the physical health of people living with severe mental illness and the Positive cardiometabolic health resource).
Essential to managing self-harm, including from self-neglect, is ensuring that the person and their support network are fully informed about these harms, the evidence base for effective interventions is used and that they are considered within the safety formulation and management plan.
Risk of harm to others
Some people who experience severe mental health problems may pose a risk of harm and serious violence to others when unwell. Risk of violence is elevated in untreated psychosis, with that risk increasing when there are concurrent other factors such as concurrent substance misuse.
Where serious violence has occurred the evidence emphasises the necessity for all safety assessment, formulation and management plans to address all factors contributing to the relationship between mental health and risk of harms, including co-occurring problems such as substance misuse. Critically, early treatment of amenable clinical risk factors and the assertive use of approaches to engage the person and their support network in treatment should be central to the person’s care and support plan. Guidance on assertive engagement approaches for adults and older adults and guidance on the management of co-occurring substance use is available.
While the guidance above for the assessment, formulation and management of harm applies to all types of harm, there are specific additional considerations for potential harm to others:
Safety assessment
The purpose of assessing risk to others is not to predict risk. It is to identify factors that contribute to the potential for harm to occur, to build an understanding of the likelihood of harms and to develop a risk formulation to inform a plan to mitigate them.
Risk of harm to others may be conceptualised as both occurring over the longer term and acutely. No one is ‘high risk’ or ‘low risk’. Risk is always dynamic and can change with circumstances, both internal and external to the person, over the briefest of timeframes. Therefore, risk assessment needs to include a short-term perspective and frequent review. A safety assessment should identify key factors that indicate a pattern or that risk is increasing.
Understanding any historical risk to others, particularly in relation to violence, is critical. A detailed history of events and the context in which they occurred is required. Some risks may have identifiable potential victims and these will need specific safety management plans.
Specific risk assessment tools such as OxMIV are validated for use in general adult community and inpatient populations, and may be used to identify those with heightened risk for additional intervention. Advice or input may need to be sought from forensic services including on the use of specific risk assessment tools. Those such as HCR20, SVR20 and RSVP must only be used with appropriate training and in populations on whom they have been validated. If clinical history and presentation suggests they are indicated, input from forensic services should be sought.
Safety formulation
A safety formulation will be derived from considering:
- historical risk factors – which will not change but will need to be kept up to date
- clinical risk factors related to the person’s mental health – which are usually amenable to change with treatment
- circumstances external to the person such as environmental factors
- the needs and strengths of the individual
It should detail the magnitude of the potential risk, its likelihood and the circumstances that may increase or decrease the likelihood, imminence and frequency of the risk and associated harm.
Safety management and planning
Once an assessment of safety and formulation have been completed, a plan must be developed with clear and specific actions and the named persons or agencies responsible for carrying out the actions. Some risks will be managed by clinical services; others will need multiple agencies to manage the risk.
Serious case reviews often find that poor multi-agency working is a reason that care, treatment, safeguarding and public protection arrangements have not kept the person and the public safe. Where someone poses a risk to others or has acted on that risk, it is critical for mental health services to work in partnership with other agencies, including the police, community forensic services, probation and prison community mental health teams, and multi-agency risk meetings (MARM) should be regularly held. multi-agency public protection arrangements (MAPPAs) are available for the assessment and management of the risks posed by sexual and violent offenders.
Good management of safety requires all parties and agencies to have proportionate necessary information. These include, where appropriate, the person, their family, carers and support network, as well as professional staff and the agencies listed above.
The use of legal frameworks such as the Mental Health Act 1983 must be considered where indicated. The Mental Capacity Act is not a legal vehicle for managing to manage the risk of harm to others.
Risk of harm from others
Professional curiosity and efforts to understand a person’s circumstances are necessary to ensure appropriate assessment, identification and management of any risk of harm from others.
The Care Act 2014 defines an adult at risk is someone who:
- is experiencing or is at risk of abuse or neglect
- has needs for care and support (whether or not the local authority is meeting any of those needs)
- as a result of those care and support needs is unable to protect themselves from the risk or experience of abuse or neglect
People who experience mental illness may be at increased risk of harm from others, including:
- abuse (physical, sexual, psychological, neglect, financial)
- exploitation (including from criminal gangs)
- financial exploitation
- domestic violence
- modern slavery
- discriminatory abuse, for example hate crimes
- organisational abuse
- risk of coercion
When providing care and treatment to vulnerable adults, staff have a duty of care to safeguard them from harm and follow the necessary steps to ensure this.
Risk of iatrogenic harm
Iatrogenic harm refers to the physical or psychological injury of a person as a result of their treatment. As with all healthcare, many of the treatments and interventions provided through mental health care carry the risk of iatrogenic harm – the physical or psychological injury of a person from their treatment, such as from a prescribed medication and restrictive practices respectively.
When assessing and formulating safety, consideration must be given to the possible unintended consequences of mental health treatment. In developing the personalised safety management plan the practitioner together with the person should weight the risks to form a balanced and personalised approach to managing multiple risks.
Decision-making can be difficult in some circumstances, such as where short-term restrictions or compulsory medication that could lead to iatrogenic harm are being considered with use of the Mental Health Act. There may be a need to balance the immediate and longer-term risks (for example, deterioration in physical health, social and vocational outcomes) against iatrogenic harm from restrictive practices. Involving the person and their support network as much as possible in decisions, seeking as much information as reasonably possible and involving multiprofessional perspectives in best interests decision-making can all help.
Teams can find it easier to recognise the potential for iatrogenic harm from prescribed treatments than to acknowledge the harm that may arise from the way staff and services interact with people. The language used to describe people who use services, the power imbalances inherent in care and the dismissal of a person’s own understanding of their experiences can all cause harm. A personalised, relational approach is essential to reducing this risk.
Health inequalities are often intertwined with iatrogenic harm. For example, failing to provide culturally competent care or care that is trauma and autism informed can contribute to poor outcomes and distress. Diagnostic overshadowing creates the potential for harm by overlooking physical health risks or allowing diagnostic labels to obscure attention to and appropriate curiosity about new risks, needs or co-morbidities. It can occur in multiple contexts such as the diagnosis of dementia, schizophrenia and co-occurring substance and in giving people the diagnosis of ‘personality disorder’.
Openness and transparency about any risk of longer-term harms related to treatment, interventions and illness can support the development of trust in relationships with services and ultimately may reduce the risk or impact of their occurrence.