
Equality and health inequalities statement
1. Promoting equality and addressing health inequalities are at the heart of NHS England’s values. Throughout the development of the service specifications and processes cited in this document, NHS England has:
- given due regard to the need to eliminate discrimination, harassment and victimisation, to advance equality of opportunity, and to foster good relations between people who share a relevant protected characteristic (as cited under the Equality Act 2010) and those who do not share it
- given regard to the need to reduce inequalities between patients in access to, and outcomes from healthcare services and to ensure services are provided in an integrated way where this might reduce health inequalities.
Introduction
2. This Methods: national clinical policies document outlines the approach and processes implemented in the development of clinical commissioning policies for specialised services. Methods: national clinical policies is accompanied by two documents: Service development policy and Methods: service specification which set out the processes in detail.
3. National clinical commissioning policies are initiated during the ‘clinical build’ phase of policy development, where a topic is proposed, a clinical evidence review is commissioned and completed, and the specialised services clinical panel confirms whether the policy proposition reflects the evidence review produced. The second phase is the ‘impact analysis’, managed and assured by the National Programme of Care (NPoC). The third and final phase is the ‘decision’, from the Clinical Priorities Advisory Group (CPAG), then the National Commissioning Group (NCG)/Delegated Commissioning Group (DCG), and finally the NHS England Board (or a subcommittee of the Board) for relative prioritisation items.
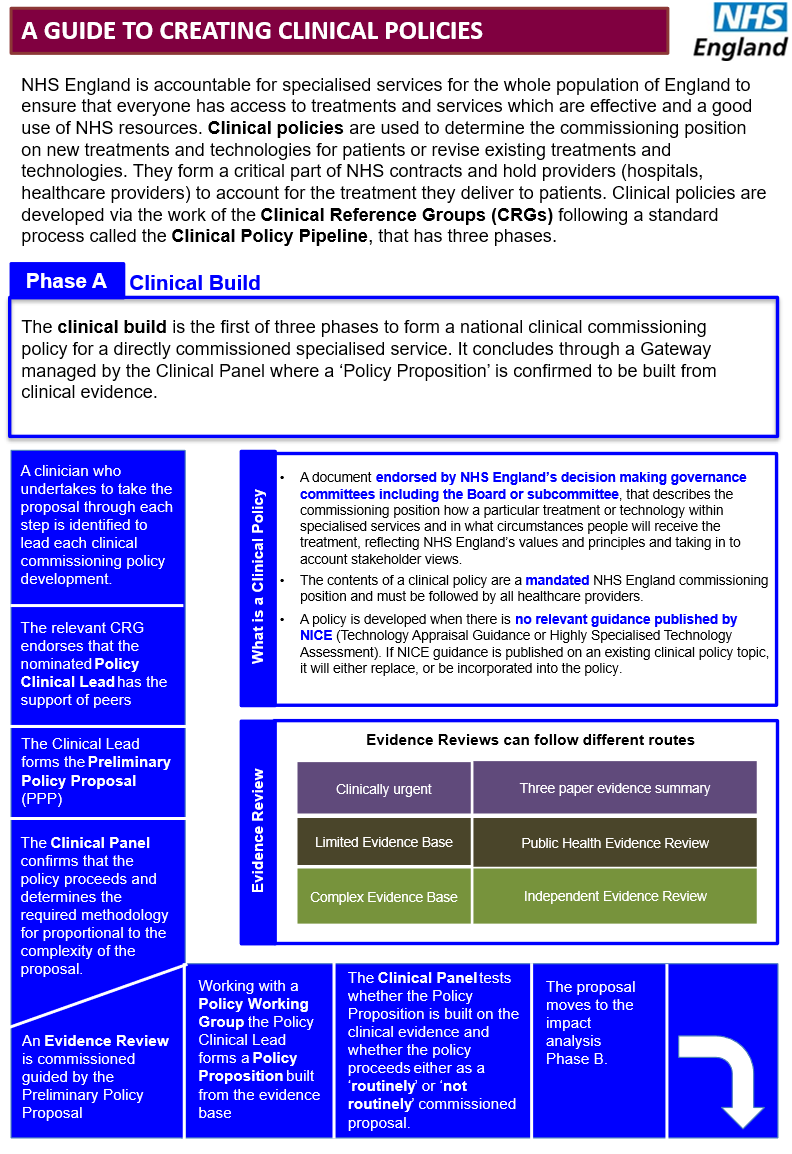
4. The clinical build is the first of the three phases to form a national clinical commissioning policy for a specialised service. It is co-ordinated and managed by the Specialised Commissioning Clinical Effectiveness Team (CET) and concludes through a gateway managed by the clinical panel. This phase also includes the assessment of the impact of the proposed policy on equality and health inequalities (EHIA).
Step A1: propose policy clinical lead
5. A clinician who undertakes to lead the proposal through each step will lead each clinical commissioning policy development stage.
A1.1 All clinical commissioning policy proposals will have a policy clinical lead. Any NHS clinician can nominate themselves and propose the development of a clinical policy. The clinical lead must have detailed clinical understanding of the policy proposal and must not have a conflict of interest associated with the technology.
A1.2 Patient organisations, royal colleges, industry and other organisations can initiate the formation of a clinical policy proposal, but they must identify a clinical lead who does not have a conflict of interest to make the proposal.
A1.3 Some clinical commissioning policy proposals will be initiated by NHS England either to introduce new interventions or to decommission existing interventions. In circumstances where an appropriate clinician willing to lead the proposal development cannot be identified, a public health consultant or other NHS England employed clinician will be identified as the policy clinical lead. In addition, the Specialised Commissioning Public Health Network may lead policies that have a wider public health benefit.
A.1.4 A copy of the clinical lead proposal form can be obtained by contacting the CET (at england.CET@nhs.net). Once the clinical lead proposal form has been completed and sent to the CET who will confirm its receipt.
Step A2: Clinical Reference Group endorses the clinical lead
6. The relevant Clinical Reference Group (CRG) endorses that the nominated policy clinical lead has the support of peers to lead the development of a proposal.
A2.1 The CET emails the policy clinical lead proposal form to the relevant CRG chair.
A2.2 The CRG chair completes a CRG preliminary policy proposal (PPP) checklist confirming whether the CRG supports the policy clinical lead, having discussed this with the CRG members. The form is returned to the CET.
A2.3 Where a lead is nominated by NHS England, the CRG members are informed and are asked to provide assistance in building clinical involvement in the Policy Working Group (PWG).
A2.4 The CET confirms endorsement with the policy clinical lead, supplying the online PPP form link, a guide for completing the form and a policy proposal reference number.
Step A3: production of the preliminary policy proposal
A. Clinical build
A3.1 The policy clinical lead completes the PPP form. This can take some time if the issue is complex, and the lead may need assistance to complete all elements of the proposal. Where the PPP proposes development of an urgent clinical commissioning policy, this should be indicated on the form with a clear explanation of the rationale.
A3.2 The policy clinical lead submits the PPP form to the CET by an online submission.
A3.3 The CET confirms receipt of the PPP.
Step A4: The NHS England Specialised Services clinical panel reviews the preliminary policy proposal
7. The clinical panel (with the NPoC Senior Managers) confirms that the policy proposal should proceed into the work programme on the basis of core qualifying criteria, and determines the required approach for a fully independent evidence review proportional to the complexity of the proposal.
A4.1 The CET submits the PPP to the next available clinical panel meeting, having received confirmation from the clinical policy team that:
- the proposal is for a specialised commissioned service
- the National Institute for Health and Care Excellence (NICE) is not undertaking an appraisal in the Technology Appraisal (TA), Highly Specialised Technology (HST) or Cancer Drugs Fund (CDF) programmes unless an urgent policy is being considered to allow for more timely access
- the intervention is not included in tariff (unless there is a specific reason to consider an in-tariff intervention, e.g. to support shared care)
- the relevant NPoC senior manager (NPoCSM) has identified initial considerations regarding the equality and health inequalities issues pertaining to the new proposal.
A4.2 For PPPs proposing the development of a clinical commissioning policy, the clinical panel confirms that the policy proposal should proceed into the work programme. The clinical panel can exclude a PPP in the following circumstances:
- the PPP has failed to identify any qualifying evidence for the proposed intervention’s benefit
- the clinical utility of implementing the intervention through a national clinical commissioning policy is not well defined.
For PPPs proposing the development of an urgent clinical commissioning policy, the clinical panel will determine:
- whether the topic will be added to the work programme to provide an urgent commissioning position
- the commissioning position of the urgent clinical commissioning policy, based on the three evidence papers provided by the clinical lead with the PPP.
The lead commissioner will then lead the development of the urgent clinical commissioning policy. A rapid impact assessment will be completed. The final documentation will proceed for a decision on final investment.
In general, PPPs for all policies follow a similar clinical panel review process. If the nature of the product to be produced changes during the course of its development, then this will be approved by clinical panel and the appropriate steps will apply.
A4.3 A commissioning policy (CP) or a commissioning position (CoP) are developed to address service issues for commissioned specialised services. The need for a statement may arise when there is requirement for a decision to address a service need, for example, regarding capacity, access, implementation or equity. The Specialised Commissioning Senior Management team (SMT) assures the development these.
The deputy director of the relevant NPoC or the NPoCSM submits the request form to CET.
The CET allocate a proposal reference number (PRN) to the request and forward the form to the Head of Programme Support for review by the Clinical Policy Team (CPT) and, if required, the contents are clarified with the submitter. The CET will assure this form.
The CET will then submit the form to the Medical Director Specialised Services and the Director of Clinical Commissioning for a decision on whether and how the proposal should proceed.
If the proposal is not approved, CPT will return to the deputy director of the relevant programme to discuss the next steps. CET will record the outcome of the decision. If the proposal is approved, it is then submitted to a SMT meeting for approval. CET are notified of the SMT meeting outcome.
CET allocate a Unique Reference Number (URN), informs the Head of Programme Support and notify the submitter that the proposal has been added to the work programme.
If a CP is to be developed, it will be based on a 3 paper evidence summary and formal clinical consensus, where needed.
If a CS is to be developed, it will normally be based on formal clinical consensus.
Thereafter, the CP or CS will follow the urgent policy proposition process post clinical panel Gateway 1.
A4.4 The clinical panel determines the required approach for an evidence review:
- very small number of publications and top three selected publications clearly define efficacy (or lack of efficacy). The clinical panel can state there is no need for a further clinical evidence review
- the intervention is a device
- the clinical panel can refer the proposal to the recognised independent provider (procured by NHS England for this work) or to NICE for a rapid evidence review.
A4.5 The clinical panel defines the clinical urgency of the requirement of the policy proposal by reviewing the clinical problem, the degree to which the intervention meets clinical need and the number and outcomes of individual funding request (IFR) applications. The CET will provide information on IFR activity relevant to the PPP. The outcome will be:
- inclusion in the work programme for proposals of high clinical urgency to be considered outside the relative prioritisation process. Any such proposals will need to satisfy specific criteria for this to happen
- the need to form an urgent clinical commissioning policy for proposals considered to be clinically urgent (to be considered outside the relative prioritisation process).
Step A5: Evidence review commissioned
8. The CET commissions an evidence review guided by the PPP.
A5.1 The lead commissioner from the relevant NPoC with support from the clinical policy team (where it is involved) establishes the PWG, to include the policy clinical lead. The PWG is formed, in line with the terms of reference. Dates are defined for receipt of the evidence review and meetings to build the policy proposition. The PWG should work via a virtual conferencing platform.
A5.2 The NHS England Specialised Services Public Health Network identifies a lead to form the PICO (population, interventions, comparators and outcomes) framework for the commissioning of the evidence review. Where involved, the clinical policy team will work with the Public Health lead to draft the PICO document. This is built from the information in the PPP and is tested with the policy clinical lead and all available members of the PWG. The CET quality assures the PICO document. In parallel, the PWG completes an initial draft of the EHIA and the patient impact assessment (PIA) template, informed by previous NPoC comment at PPP stage and PWG considerations based on sources of evidence.
A5.4 The CET commissions the evidence review and CPAG summary report for the clinical panel from an external provider, and co-ordinates its completion.
A5.5 The CET establishes communication between the evidence review team and the policy clinical lead to clarify elements of the evidence review and CPAG summary report for the clinical panel.
A5.6 The CET receives the evidence review and circulates it to the PWG for comment over five working days. The CET quality assures the evidence review and CPAG summary report during this period.
Step A6: Policy proposition formed
9. Working with the PWG, the policy clinical lead forms a policy proposition from the evidence base.
A6.1 All members of the PWG are asked to undertake online training and an assessment, led by the CET, which includes the fundamentals of an evidence review and clinical policy formation.
A6.2 On receipt, from the CET, of the evidence review and CPAG summary report for the clinical panel, the PWG proceeds to form a policy proposition and Evidence to Decision (EtD) document.
A6.3 The clinical lead (or clinical policy team) secures consensus agreement to the policy proposition from members of the PWG. The clinical lead shares and agrees the policy proposition with the PWG.
A6.4. A prior approval form should be drafted at this point and included in the audit requirements section of the policy proposition.
A6.5 The deputy director of clinical effectiveness submits the previous clinical panel report, evidence review, an EtD document, CPAG summary report for the clinical panel, draft EHIA report, draft PIA, draft prior approval form, and policy proposition to the next available clinical panel meeting.
A6.6 Where there is no consensus in the PWG, a short summary of the points of difference is prepared and submitted to the clinical panel.
Step A7: clinical panel
10. The clinical panel tests whether the policy proposition is built on the clinical evidence and whether it should proceed into the impact analysis phase as either a ‘routine’ or ‘not for routine’ commissioning proposition.
A7.1 The clinical panel receives the previous clinical panel report, evidence review, CPAG summary report for clinical panel, draft EHIA report, draft PIA, draft prior approval form, final EtD document, and policy proposition.
A7.2 The clinical panel determines:
- whether the eligible population is adequately defined
- whether any eligible subpopulations are adequately defined
- that the policy proposition is built on the evidence base as defined in the evidence summary
- that the evidence presented supports the proposed commissioning position.
- whether any eligibility criteria are adequately defined.
A7.3 If the clinical panel supports the policy proposition, the CET passes the proposition to the relevant NPoC (and CPT where applicable) to move to the second phase – ‘impact analysis’.
For urgent clinical commissioning policy proposals supported by the clinical panel, the proposition will be drafted by the clinical lead (or CPT on their behalf) in conjunction with the lead commissioner, and submitted to the NCG / DCG for approval, and then will progress to Step C6.2.
A7.4 The clinical lead will receive a written report of the clinical panel’s decision. If the clinical panel does not support the policy proposition, the clinical lead will report back to the PWG. The PWG may agree that it (a) needs to work up the proposition further before re-submission to the clinical panel or (b) has demonstrably valid grounds for disputing the findings of the clinical panel. The clinical lead will discuss this with the CRG chair who considers the preferred course of action and may need to discuss this with CRG members. The PWG will receive a detailed clinical panel report outlining the clinical panel’s debate and reasons for its recommendation. If the CRG chair agrees the PWG has grounds for dispute, a formal letter will be written to the NPoC for consideration. It is for the NPoC to then decide the course of action, and whether the clinical panel should be formally requested to review its recommendation.
B. Impact analysis
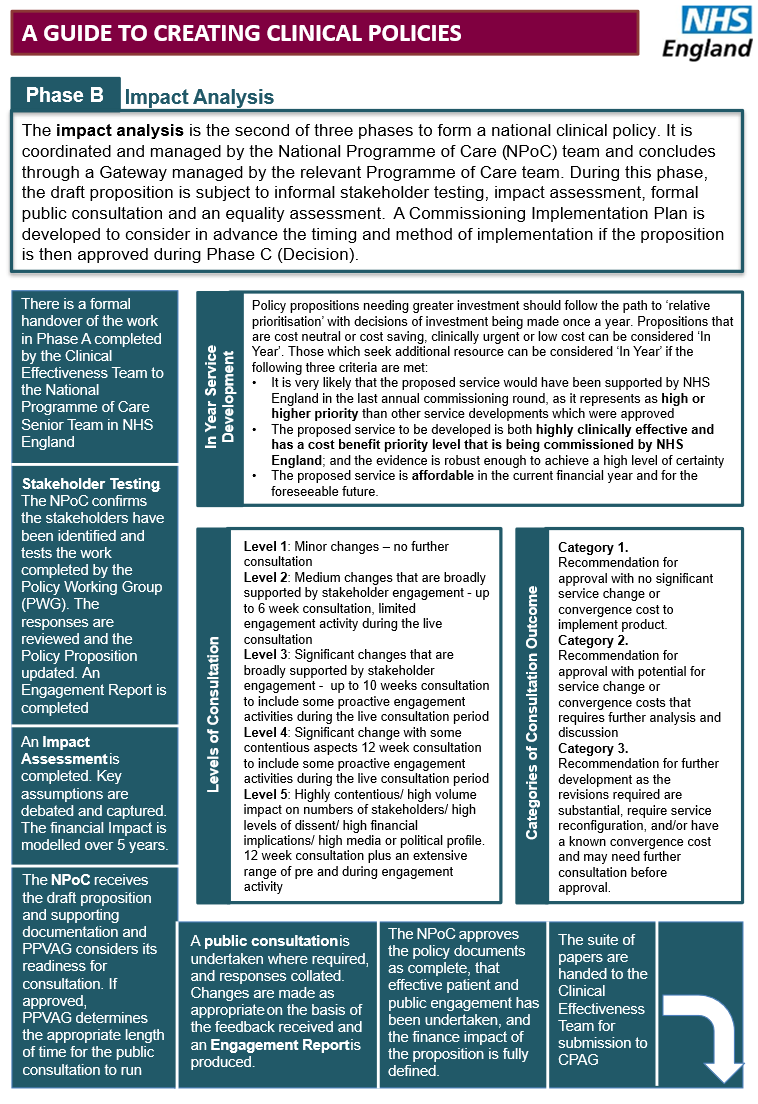
11. The impact analysis is the second of the three phases to form a national clinical commissioning policy. It is co-ordinated, managed and assured by the NPoC.
Step B1: Stakeholder testing
12. The NPoC confirms the stakeholders that have been identified and tests the work completed by the PWG.
B1.1 The PWG prepares to test the policy proposition, EHIA report, and PIA with stakeholders, including those that have already registered as having an interest in the work of the host CRG.
B1.2 The PWG considers any additional stakeholders they would wish to contribute views at this stage, forwarding details to the Communications and Engagement Team. The PWG should identify any other CRGs to which the policy proposition may be relevant and that should test the documents.
B1.3 The draft policy proposition, EHIA report, and PIA is sent to the complete list of stakeholders (with evidence review-related documentation, if one has been undertaken), together with a response form.
B1.4 The PWG considers, particularly for more contentious topics, whether a formal stakeholder event should be arranged to supplement testing by email. Otherwise, responses are received via a generic email and acknowledged. Collated responses are sent to the lead commissioner.
B1.5 The PWG reviews the responses and updates the policy proposition and EHIA report as appropriate based on the feedback.
B1.6 If the stakeholder testing raises the issue that the evidence review may not have evaluated the full evidence base, the public health lead will review whether the evidence identified was considered and excluded from the evidence review (e.g. because the study did not meet the PICO) and if not, whether there has been an omission that materially affects and alters the proposition. An evidence report should be completed to identify whether there has been an omission or to outline the reason for the exclusion. If they determine the full evidence base has not been evaluated, the policy process will be returned to Step A5 and handed back to the CET.
B1.7 An engagement report is completed. For policy propositions not progressing to public consultation, on completion of stakeholder testing, the proposition will progress to Step B6, for sign off by the NPoC and progression to the decision phase.
B1.8 Once the outcome of the stakeholder testing has been reviewed, the PWG will complete the Specialised Commissioning 13Q Assessment Form Part A for the proposition to determine whether public consultation is required. The assessment is reviewed and confirmed by the relevant NPoCSM in consultation with the deputy director of the relevant NPoC and the Communications and Engagement Team.
The 13Q Assessment Form is discussed at the next Patient and Public Voice Assurance Group (PPVAG) meeting, unless urgent and then Chair’s action may be required. PPVAG will provide assurance on the decision on the requirement to undertake public consultation or not and, if considered required, the length of that consultation. If public consultation is not required then the proposition will proceed to PoC assurance and then CPAG.
Step B2: Completion of impact analysis reports
13. An impact assessment is completed with advice from a finance specialist. Key assumptions are debated and captured in a supporting spreadsheet. The NPoCSM establishes the work programme to complete the impact analyses.
B2.1 The lead commissioner confirms to the NPoC that stakeholder testing is complete and receives its agreement to process the impact assessment.
B2.2 The NPoCSM with the NPoC finance lead identifies the finance support to complete the finance impact report.
B2.3 The impact assessment is undertaken, identifying the impact of moving from current pathways of care to the one(s) proposed in the draft policy proposition. The finance lead works with the lead commissioner, the clinical lead and public health lead to agree assumptions. A supporting spreadsheet is produced to capture the financial workings included in and assumptions made in the assessment.
B2.4 Impact is modelled over five years, or by exception over 10 years; for example, if significant demographic changes are expected over an extended period.
B2.5 The finance lead completes section II of the CPAG summary report containing the finance report, this includes the budget impact and the net cost per patient over five years (calculated as cost to NHS England over five years divided by the number of patients receiving treatment over five years). The NHS England Specialised Commissioning Finance Team approves the cost per patient information and budget impact and identifies and considers areas of uncertainty.
Step B3: NPoC receives the combined impact analysis report
14. The NPoC receives the draft policy proposition and supporting documentation, and considers its readiness for progression to the CPAG or public consultation.
B3.1 The NPoCSM with the lead commissioner supporting the PWG submits the following to the NPoC:
- clinical panel report
- policy proposition
- evidence review or three supporting evidence papers
- evidence report (where applicable)
- CPAG summary report for clinical panel
- EHIA report
- engagement report
- impact analysis report
- prior approval form
- EtD document
- PIA
B3.2 The NPoC approves the impact analysis report (or returns it to the finance lead for further work in conjunction with relevant PWG members).
B3.3 The financial model should be approved by the deputy director of Finance (Specialised Services) or nominated deputy before progression to the CPAG or public consultation.
B3.4 The NPoCSM or lead commissioner drafts the commissioning implementation plan.
Step B4: Public consultation
15. The public consultation is undertaken (if required) and responses collated for consideration by the PWG. Changes are made as appropriate on the basis of the feedback received, and the engagement report is updated.
B4.1 Documentation is prepared for consultation, actioning any amendments required by the NPoC.
B4.2 The following documents are prepared to be included in the consultation:
- policy proposition
- evidence review
- CPAG summary report for clinical panel
- clinical panel report
- EHIA report
- engagement report
- impact analysis report
- EtD document
- PIA
B4.3 At the end of the consultation period, the collated consultation responses are then forwarded to the lead commissioner. The PWG meets to consider these and amends the policy proposition, EHIA report, PIA, and impact assessment as appropriate, taking into account the consultation responses. The feedback is included in the engagement report.
B4.4 If any comments identify that the evidence review did not evaluate the full evidence base, the public health lead will review whether the evidence identified was excluded from the evidence review (e.g. because the study did not meet the PICO) and if not, whether there has been an omission that is material. The public health lead will complete an evidence report to identify whether there has been an omission or to outline the reason for the exclusion. If they determine this is the case, the CET will identify whether the evidence review can proceed with an addendum or whether the policy proposition should return to an earlier stage of the process.
B4.5 Should the policy proposition be paused or stopped at this stage, a status change report is completed.
B4.6 The NPoCSM or lead commissioner finalises the draft commissioning implementation plan, draft circular and provider letter, which will accompany the suite of documents for sign off by the NPoC (see Step B5) and may accompany the CPAG summary report to the NCG / DCG as required.
Step B5: National Programme of Care
16. The NPoC approves the policy proposition documents as complete and confirms that effective patient and public engagement has been undertaken, and the finance impact of the proposition is fully defined.
B5.1 The NPoCSM submits the following documents to the NPoC:
- policy proposition
- evidence review or three supporting evidence papers
- CPAG summary report (including sections 1 and 2 and the PIA)
- clinical panel report
- engagement report (includes consultation)
- impact analysis report
- EHIA report
- evidence report (where applicable)
- draft commissioning implementation plan, including draft circular and provider letter.
- prior approval form
- EtD document
B5.3 The NPoC determines whether the consultation materially affects the impact analysis report or the policy proposition. Further amendments are made if required and will be resubmitted for NPoC approval.
B5.4 For policy propositions developed with Highly Specialised Services (HSS) involvement, the HSS Team will submit the proposition to the Rare Diseases Advisory Group (RDAG) to consider endorsement prior to Step B6. This is an additional gateway step for policy propositions developed with HSS involvement.
Step B6: Handover to CET
17. The suite of papers is handed to the CET for submission to the CPAG.
B6.1 The NPoCSM hands the documents back to the deputy director of Clinical Effectiveness. These include:
- final draft policy proposition
- evidence review or three supporting evidence papers (
- CPAG summary report (with sections 1 and 2 completed and PIA included)
- engagement report (includes consultation)
- impact analysis report
- EHIA report
- finance model spreadsheet
- evidence report completed by public health lead (where applicable)
- draft commissioning implementation plan, draft circular and provider letter
- any comment that the NPoC would want the CPAG to be aware of during the decision-making phase
- prior approval form
- EtD document
C. Decision
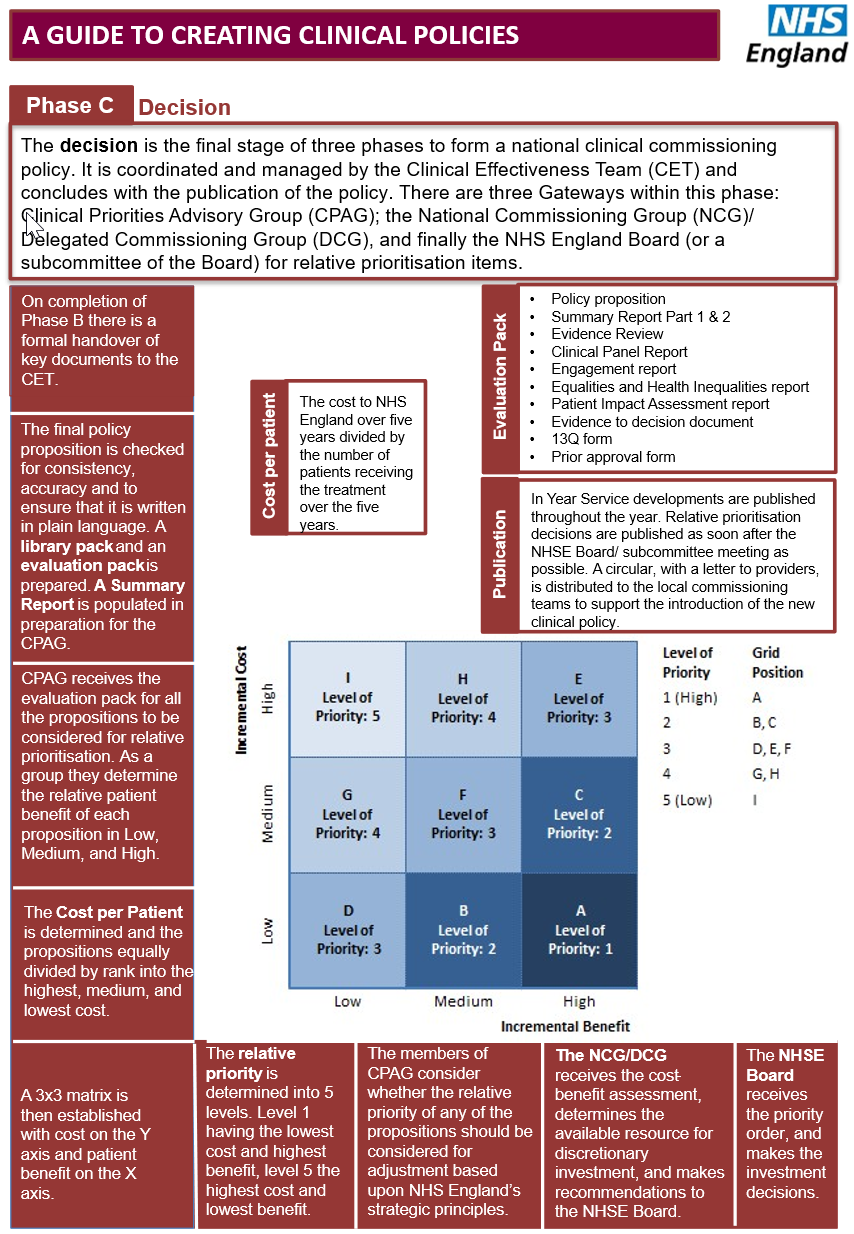
18. The decision is the last of the three phases to form a national clinical commissioning policy. It is co-ordinated and managed by the CET and concludes with the publication of the policy. There are three gateways within this phase: CPAG; the NCG / DCG; and NHS England Board (or a subcommittee of the Board).
Step C1: Editorial checking and preparation
19. The CET checks the final policy proposition for consistency, accuracy and to ensure that it is written in plain English. It prepares two packs of papers: a library pack (see Step 1.2) and an evaluation pack (see Step 1.3). A summary report is populated in preparation for the CPAG meeting.
C1.1 The library pack is compiled to include:
- agreed PICO provided to the reviewer of the clinical evidence, which includes the search criteria and the literature search publication list
- impact analysis report
- finance spreadsheet
- engagement report appendices
- commissioning implementation plan, draft circular and provider letter
- CPAG summary report section 2 (for policies entering prioritisation only)
- presentation slides and script
C1.2 The evaluation pack is compiled to include:
- policy proposition
- evidence review or three supporting evidence papers
- CPAG summary report section 1 (evidence, service impact and PIA) and section 2 (finance) (for IYSDs) or CPAG summary report section 1 (for policies entering prioritisation)
- clinical panel report
- engagement report
- evidence report (where applicable)
- EHIA report
- Evidence to decision document
- 13Q form
- prior approval form
C1.3 The library pack and evaluation pack are submitted to the deputy director of the relevant Programme of Care; deputy director of Finance (or nominated deputy) and Director of Clinical Commissioning, CPAG regional medical directors of commissioning and deputy director of quality and nursing to confirm assurance in advance of the deadline. If any amendments are required, the packs will be returned to the NPoCSM for resolution before the deadline provided. The commissioning implementation plan, which forms part of the library pack, is approved by the relevant deputy director of programmes and director of clinical commissioning.
C1.4 Once assurance has been confirmed, the library pack and evaluation pack will then be submitted to the deputy director of clinical effectiveness to confirm assurance in advance of the deadline. If any amendments are required, the packs will be returned to the NPoCSM for resolution before the deadline provided.
Step C2: Clinical Priorities Advisory Group
20. Service developments considered outside the relative prioritisation process. The CPAG members receive the evaluation pack including the summary report sections 1 and 2. The CPAG then considers the clinical patient benefit and financial impact that the implementation of the policy would deliver. The CPAG will make a commissioning recommendation for approval by the NCG / DCG.For clinical policies to be considered through this route they would have to be confirmed as cost neutral or cost saving, or satisfy the factors stated in the service development policy.
21. Appraisal of cost/benefit (relative prioritisation). The CPAG members receive the evaluation pack (except the summary report section 2 and the financial information it contains). The CPAG then considers the patient benefit that the implementation of the policy would deliver. The CPAG then determines the relative patient benefit of all the policy propositions being considered as part of the relative prioritisation process. This is done without reference to the costs of implementation. Policy propositions are allocated in equal proportion to one of three patient benefit categories: low, medium and high.
C2.1 CPAG members receive the evaluation pack a minimum of one week before the relative prioritisation meeting. Members are asked to identify questions to help clarify their interpretation before the meeting and to consider which of the three categories each proposition should be allocated. Assurance from all parties outlined in the CPAG summary report, as gained in Steps C1.3 and C1.4, is confirmed.
C2.2 The CPAG meeting begins with a presentation of each policy proposition followed by discussion and questions for clarification. Members of the CET, NPoCSMs and deputy directors of relevant programmes of care are in attendance to support the CPAG discussion and to provide answers to questions raised. The library pack is available at the meeting for reference if required.
C2.3 In the next part of the meeting the CPAG chair leads a deliberative debate on the relative patient benefits for each of the policy propositions: low, medium or high.
C2.4 The CET separates all the propositions into five groups, depending on the consensus of the CPAG determined by the chair. The grouping needs to take account of the differences in opinions between members and is an intermediate grouping pending final allocation of policy proposals in equal proportion to low, medium and high patient benefit categories:
- low
- low/medium
- medium
- medium/high
- high
C2.5 The number of available positions in the three categories (low/medium/high) is determined by the total number of propositions presented. An equal number of propositions will be placed in each group. Where propositions clearly provide low or high benefit they are placed in the corresponding category. If there is any uncertainty, they are placed in either the low/medium or medium/high category. The members then focus on the propositions in the low/medium and medium/high groups and move them through deliberative debate, filling the available slots in each category of low, medium or high. An equal number of propositions are in each category.
C2.6 All members review the allocations as a group to consider and agree whether any further adjustment is required or not.
C2.7 The chair calls a close to the discussion on patient benefit.
Step C3: Clinical Priorities Advisory Group – application of relative cost (relative prioritisation)
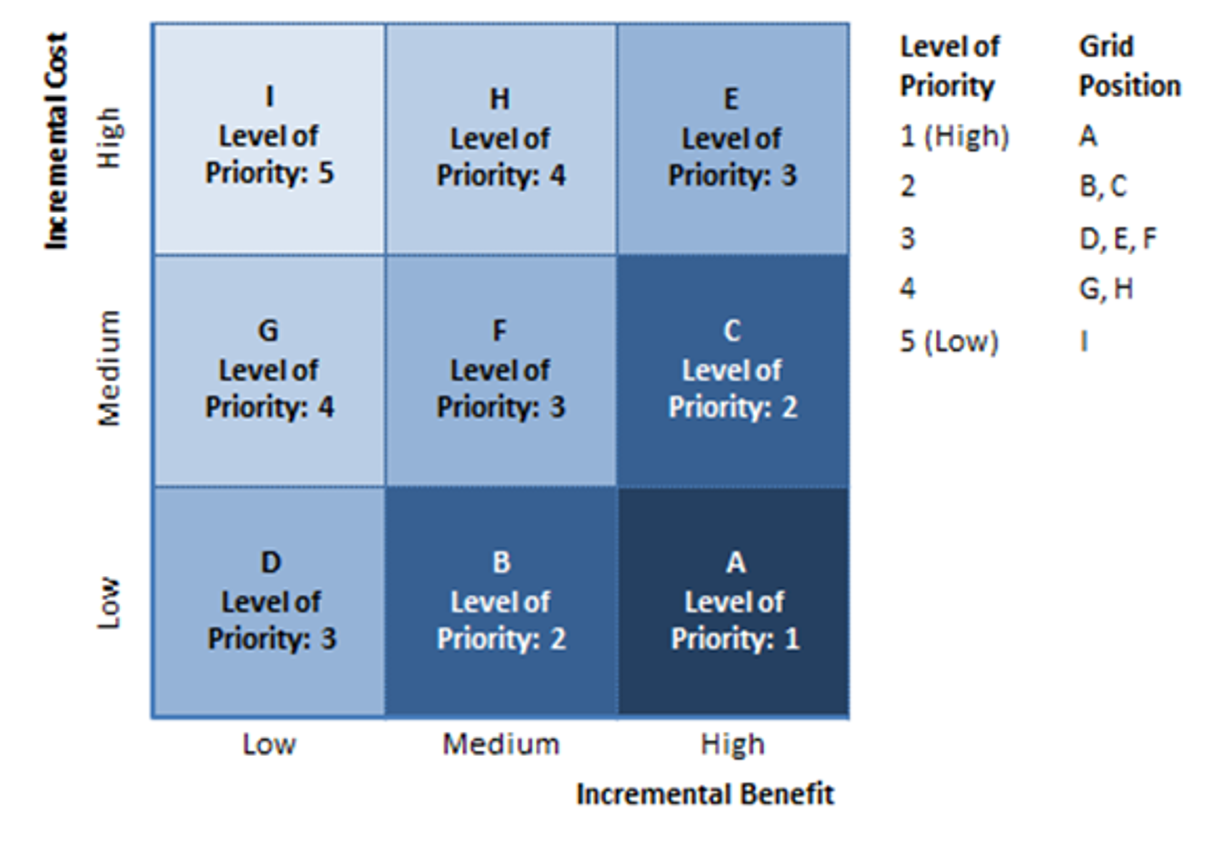
C3.1 While CPAG members are in recess, the finance analysts will determine three cost per patient ranges that will equally divide the propositions into three categories of cost – low, medium and high – based on the information received.
C3.2 A three by three 9-box matrix is populated (see Figure A below). All propositions are then presented according to five levels of equivalent cost–benefit per patient. Level I is the highest benefit at lowest cost; level 5 is the lowest benefit at highest cost.
The unadjusted cost–benefit list is locked at this point.
C3.3 If it is clear that propositions in a number of levels can be considered for funding within the available resource (e.g. levels 1 and 2), and it is clear that all those lying in the next level (e.g. level 3) could not be considered in totality but some might, then the original clinical benefit category for each proposition in that level would be referred to. Those propositions in the highest categories falling within the available resource would be recommended for funding. The remaining propositions in that level and those positioned in, for example, levels 4 and 5, would not be recommended for funding.
Figure A: Three 9-box matrix
Step C4: Clinical Priorities Advisory Group – consideration of the strategic principles (relative prioritisation)
22. The CPAG members consider whether the relative priority of any of the propositions should be considered for adjustment based on NHS England’s strategic principles. Any adjustment is supported by a narrative of the reasons for the adjustment.
C4.1 The strategic principles that should be considered include:
- the intervention should benefit the wider health and care system
- the intervention should advance parity between mental and physical health
- consider the benefit of stimulating innovation
- reduce health inequalities
C4.2 Once each proposition has been reviewed, an adjusted cost–benefit list is locked at this point.
C5.1 The Medical Director presents the unadjusted and adjusted (using NHS England’s strategic principles) cost–benefit assessment from the CPAG, and the narrative for the adjustments. The budget impact for each of the propositions is presented, and the total budget impact for each of the five levels of cost–benefit is presented.
C5.2 The NCG/DCG considers whether it supports or rejects the adjustments on individual propositions and forms a revised adjusted cost-benefit list. The budget impact of the revisions to the levels is reviewed.
C5.3 The NCG/DCG considers the associated commissioning implementation plans and approves these, where agreed. Feedback is provided to the NPoCSMs where further amendments to individual plans are required before implementation, should the NHS England Board (or a subcommittee of the Board) approve the adoption and publication.
Step C6: NHS England Board (or a subcommittee of the Board) – approval
25. Service developments considered outside the relative prioritisation process. The NCG/ DCG receives CPAG recommendations and makes a final decision on adoption.
26. Relative prioritisation. The NHS England Board (or a subcommittee of the Board) receives the cost–benefit level assessments and the NCG/ DCG recommendations, and determines the final investment.
C6.1 The NHS England Board (or subcommittee of the Board) receives the NCG/ DCG investment recommendations and the recommendation for CPAG prioritisation of policy propositions.
C6.2 The Board/ subcommittee considers the recommendations and makes a final decision on investment.
C6.3 The CET works with the Communications Team to complete the final stages of policy approval for publication and accompanying communications.
C6.4 The final clinical policies are published on the NHS England website.
C6.5 The communication circular and accompanying provider letter, detailing the clinical policies due for publication and confirming the date of publication, will be extracted from the appendix of the commissioning implementation plan for distribution to local commissioning teams. This will reflect the relevant elements of the agreed commissioning implementation plan.
Glossary
- CDF – Cancer Drugs Fund
- CET – Clinical Effectiveness Team
- CPT – Clinical Policy Team
- CPAG – Clinical Priorities Advisory Group
- CRG – Clinical Reference Group
- DCG – Delegated Commissioning Group
- EHIA – Equality and health inequalities assessment
- HST – Highly Specialised Technology
- IFR – Individual funding request
- NCG – National Commissioning Group
- NPoC – National Programme of Care
- NPoCSM – National Programme of Care Senior Manager
- PPP – Preliminary policy proposal
- PPVAG – Patient and Public Voice Assurance Group
- PWG – Policy Working Group
- RDAG – Rare Disease Advisory Group
- TA – Technology appraisal
Appendix A: guide to crating clinical polices
NHS England is accountable for specialised services for the whole populations o England to ensure that everyone has access to treatment and services which are effective and a good use of NHS resources. Clinical polices are used to determine the commissioning position on new treatments and technologies for patients or revised existing treatments of technologies. They form a critical part of NHS contracts and hold providers (hospitals, healthcare providers) to account for the treatment they deliver to patients. Clinical polices are developed via the work of the clinical reference group (CRGs) following a standard process called the Clinical Policy Pipeline that has 3 phases:
- Phase A: clinical build
- Phase B: impact analysis
- Phase C: decision
See below for a guide on each phase.
Phase A: clinical build
Phase B: impact analysis
Phase C: decision
Appendix B: change notice for published specifications and products
Amendment to the published products
Product name: Methods: National clinical policies
Ref no: 06181
Description of changes required
| Describe what was stated in original document | Describe new text in the document | Section/ paragraph to which changes apply | Describe why document change required | Changes made by | Date change made |
|---|---|---|---|---|---|
| NHS England governance structures and committee names listed | Board and committee names have been updated to reflect the NHS England and NHS Improvement governance structure as of 1 April 2019. Specialised commission committee names have also been amended. | Throughout | The names of boards and committees have been updated to reflect the new structures implemented following the move to joint working of NHS England and NHS Improvement as of 1 April 2019. | Deputy Director Clinical Effectiveness | 05/2020 |
| Outline of stakeholder engagement and consultation process | 13Q assessment and associated consultation decision making and processes described. | B1.8 | A new approach to stakeholder testing and public consultation agreed with PPVAG. | Deputy Director Clinical Effectiveness | 05/2020 |
| Equality impact assessment process detailed | Completion of EHIA assessment form is an iterative process starting at the beginning of policy proposition development and is revised based on stakeholder | Throughout | A new EHIA assessment form has been introduced for use throughout NHS England and NHS Improvement. | Deputy Director Clinical Effectiveness | 05/2020 |
| Appendix A | Various text changes to align with changes above | Appendix A | The appendices have been updated to reflect changes in the text outlined above. | Deputy Director Clinical Effectiveness | 05/2020 |
| Reference to Service Specifications | Removal of erroneous reference to service specifications | Equality statement and step C6 | Removal of erroneous reference to service specifications | Clinical Effectiveness Project Manager | 08/2021 |
| The PICO process | Introducing the EHIA drafting process at this stage. | A5.2 | Ensure sufficient consideration of the EHIA in the PICO development | Clinical Effectiveness Project Manager | 02/2023 |
| Outline of impact analysis process- | NPoCSM and Head of the relevant NPoC | B1.8 | Revision of correct acronyms | Clinical Effectiveness Project Manager | 02/2023 |
| Impact analysis report | Evidence to decision | Documents for assurance throughout | The Evidence to Decision document has now been incorporated to the assurance pack | Clinical Effectiveness Project Manager | 02/2023 |
| Reference to Specialised Commissioning Health & Justice Strategy Group SCHJ | National Commissioning Group (NCG)/Delegated Commissioning Group (DCG) | Throughout | The SCHJ is no longer in place and has now been replaced with the NCG & DCG | Clinical Effectiveness Project Manager | 02/2023 |
| Reference to the EHIA | Addition of the Patient Impact Assessment (PIA) | Throughout | In addition to the EHIA the Patient Impact Assessment has been added to the clinical build process | Clinical Effectiveness Project Manager | 02/2023 |
| Reference to NHS England and NHS improvement | NHS Improvement has been removed- now known as NHS England | Throughout | Organisational changes | Clinical Effectiveness Project Manager | 02/2023 |
| Appendix A | Various text changes to align with changes above | Appendix A | The appendices have been updated to reflect changes in the text outlined above. | Clinical Effectiveness Project Manager | 02/2023 |
| References to staff role titles | Updated to reflect new role titles in line with organisational reorganisation outcome. | Throughout | Organisational changes | Deputy Director Clinical Effectiveness | 04/25 |
| Policy documents | Updated to reflect policy document types introduced in recent years and in use | Throughout | Introduced to add flexibility to types of policy products availability and more rapid timeline of development | Deputy Director Clinical Effectiveness | 04/25 |
Publication reference: PAR0013 updated PRN02424