We've put some small files called cookies on your device to make our site work.
We'd also like to use analytics cookies. These send information about how our site is used to a service called Google Analytics. We use this information to improve our site.
Let us know if this is OK. We'll use a cookie to save your choice. You can read more about our cookies before you choose.
National Qualitative Insight – Urgent and Emergency Care 2024
1. Introduction and methodology
The NHS Patient Survey Programme is delivered by the Care Quality Commission (CQC) on behalf of NHS England and the Department of Health and Social Care. The Survey Coordination Centre at Picker, coordinates the NHS Patient Survey Programme on behalf of CQC. There are five surveys within the Programme: Adult Inpatient, Maternity, Children and Young People, Community Mental Health and Urgent and Emergency Care Surveys.
This report has been produced by Solutions Strategy Research Facilitation Ltd (Solutions Research) and NHS England to share national insights from qualitative thematic analysis of written responses provided by respondents that took part in the NHS Patient Survey Programme. The aim of this endeavour is to identify opportunities for learning and improvement through an in-depth understanding of experiences of care.
The focus of this report is on the Urgent and Emergency Care Survey 2024, which captured feedback from 35,670 patients who attended a Type 1 Accident and Emergency (A&E) service in February 2024 and 10,325 patients who attended a Type 3 Urgent Treatment Centre (UTC) service in February 2024.
Further information on the survey is available on the CQC website.
Qualitative data analysis
One open question was included in the survey which allowed respondents to use their own words to respond. This question was positioned at the end of the survey and included the instructions as follows:
Type 1 (A&E): ‘If there is anything else you would like to tell us about your experience in the A&E department, please do so here.’
Type 3 (UTC): ‘If there is anything else you would like to tell us about your experiences in the Urgent Treatment Centre, please do so here.’
To ensure a robust approach a purposive sampling method was used for thematic qualitative analysis:
Type 1 (A&E): 682 comments were analysed as a sample from 15,908 viable comments.
Type 3 (UTC): 681 comments were analysed as a sample from 3,935 viable comments.
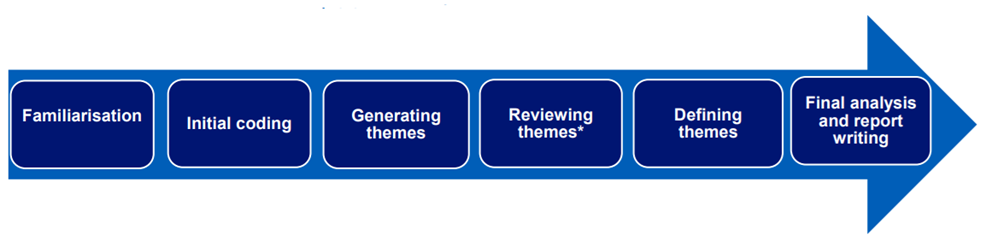
Once the total sample of 1,363 comments had been analysed it was seen that data saturation had been reached i.e. no new themes were emerging from the data. Had this not been achieved, additional comments would have been added to the sample as necessary, in line with best practice in qualitative analysis. Further detail can be found in Appendix 5: Methodology and Appendix 6: Sampling Approach.
Use of illustrative quotes
Throughout the report, quotes are included to illustrate respondents’ experiences in their own words and substantiate the findings. Quotes indicate if the respondent was from the Type 1 sample (Type 1, A&E) or Type 3 sample (Type 3, UTC). Please note that the data is not edited in the interests of correct spelling and punctuation for example, to stay as true to the words of respondents as possible.
Certain information from the qualitative comments used in the report has been redacted to protect the identity of survey respondents and any other individuals referenced. Information that has been removed includes:
names of patients or staff replaced with “(name)”
names of wards, units or hospitals replaced with “(location name)”
names of specific services replaced with “(service name)”
specific dates replaced with “(date)”
Use of quantitative data
Where possible in the findings section, themes are presented in context of the most relevant quantitative survey data. This allows for insights to be considered more holistically and to provide a greater opportunity for reflection and learning.
Statistics from the Type 1 (A&E) sample reference the question number using ‘Q’, and statistics from the Type 3 (UTC) sample reference the question number using ‘T’. To reflect the statistical release, results for the Type 1 survey and Type 3 survey are reported separately.
Context to support interpretation
It was observed that some patients were not always able to identify which type of service they had accessed, particularly seen in the Type 3 (UTC) sample who were more likely not to differentiate between A&E and UTC. For example, in feedback they would use the terms interchangeably or reference their experience at A&E when known to have attended an UTC.
There is evidence that some respondents were not always commenting on the specific visit they were asked about in their survey. Some patients would share their full story, which could include multiple visits to urgent or emergency care and/or wider NHS access.
A small number in each sample, focussed on details of their health status as opposed to the care that they received. It is unclear from the comments why this was the case, and helpful to note that this detail was out of scope for analysis.
Comments reveal varied reasons for attending urgent and emergency care, alongside significant diversity in expectations, attitudes, prior experiences, and social contexts. These factors shaped how patients responded to their care and interactions, creating a challenging environment for delivering consistently high-quality experiences. Themes are closely interwoven and often interlink, and this report highlights these connections throughout. For instance, trust and confidence are influenced by multiple factors spanning the themes of ‘Staff,’ ‘Waiting,’ and ‘Treatment.’
Where feedback varied by setting this is highlighted in the report. If no distinction is made in the commentary, the findings are applicable to both A&E and UTC.
2. Headline findings
Key themes
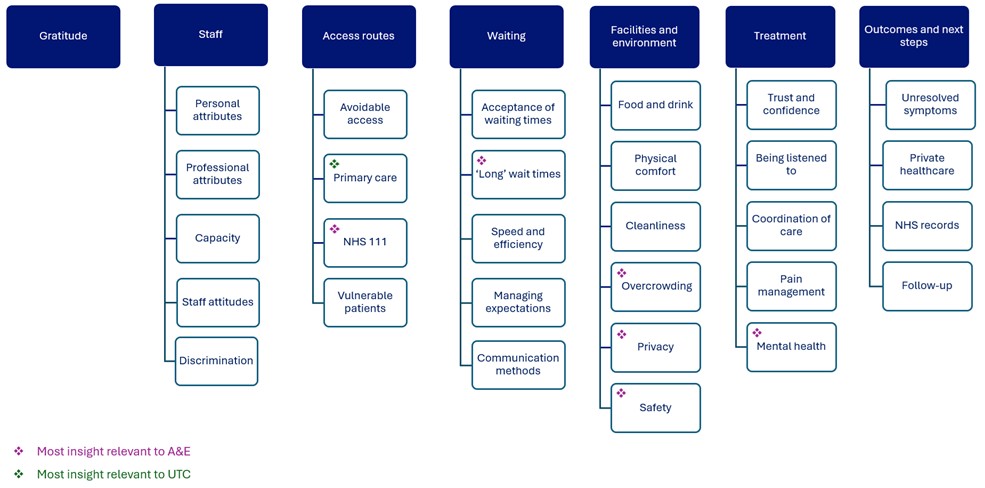
Seven key themes were identified from the thematic analysis, listed below. Within each key theme are several sub-themes which support interpretation and use of the insights. There are 29 sub-themes in total.
Gratitude
Staff
Access routes
Waiting
Facilities and environment
Treatment
Outcomes and next steps
Image description:
A flowchart-style diagram with seven main categories shown as dark blue boxes at the top. Each category has related subtopics listed below in lighter blue boxes. The categories from left to right are:
Gratitude – no subtopics listed.
Staff – subtopics: Personal attributes, Professional attributes, Capacity, Staff attitudes, Discrimination.
Access routes – subtopics: Avoidable access, Primary care (marked with a green star for “Most insight relevant to UTC”), NHS 111 (marked with a pink star for “Most insight relevant to A&E”), Vulnerable patients.
Waiting – subtopics: Acceptance of waiting times, ‘Long’ wait times (pink star), Speed and efficiency, Managing expectations, Communication methods.
Facilities and environment – subtopics: Food and drink, Physical comfort, Cleanliness, Overcrowding (pink star), Privacy (pink star), Safety (pink star).
Treatment – subtopics: Trust and confidence, Being listened to, Coordination of care, Pain management, Mental health (pink star).
Outcomes and next steps – subtopics: Unresolved symptoms, Private healthcare, NHS records, Follow-up.
At the bottom, a legend explains the star symbols:
Pink star: Most insight relevant to A&E.
Green star: Most insight relevant to UTC.
This section of the report contains the detail of each theme with a range of quotations shared to substantiate and exemplify the experience of patients using their own words.
3. Thematic analysis findings
Key themes
Seven key themes were identified from the thematic analysis, listed below. Within each key theme are several sub-themes which support interpretation and use of the insights. There are 29 sub-themes in total.
gratitude
staff
access routes
waiting
facilities and environment
treatment
outcomes and next steps
This section of the report contains the detail of each theme with a range of quotations shared to substantiate and exemplify the experience of patients using their own words.
Theme: gratitude
What does the quantitative data tell us?
Type 1 (A&E): 38% rated their overall experience a 9 or 10 where a score of 0 represented a ‘very poor experience’ and a 10 a ‘very good experience’ (Q43).
Type 1 (A&E): of respondents who left a viable comment, 37% rated their overall experience a 9 or 10 (Q43).
Type 3 (UTC): 54% rated their overall experience a 9 or 10 (T40).
Type 3 (UTC): of respondents who left a viable comment, 58% rated their overall experience a 9 or 10 (T40).
A strong, overarching theme noted across comments was overall gratitude for the NHS or the specific service attended. Often this was one part of an individual’s comment, with patients going on to discuss other aspects of their care both positively and/or negatively.
Comments of gratitude were directed at the NHS generally and broadly.
“Overall apart from waiting 7/8 hours, NHS is doing awesome job. Well done.” [Type 1, A&E]
“First time using NHS services since moving here, brilliant experience. Really reassuring and concentual. Thank you!” [Type 1, A&E]
“My treatment was thorough and excellent.” [Type 3, UTC]
“My experience at the Urgent Care Centre (location name) was very good, I would recommend it rather than going to A&E IF A MINOR INJURY ETC.” [Type 3, UTC]
Often statements expressing appreciation referenced specific teams or individual members of staff, highlighting how the staff influenced their positive experience. The ‘Staff’ theme in this report provides further insight on the behaviours patients experienced as most impactful and valued.
“The whole team was brilliant throughout my experience from receptionist to treatment. Dealt with appropriate humour and care. Distracted me through chatting whilst several stitches were done. Beyond excellent.” [Type 3, UTC]
“Best A&E visit ever – I was able to go back to caring for my children after breaking my arm. The doctor was fantastic; clear, concise, and listened to my questions and answered them.” [Type 1, A&E]
“The care my dad received on A&E (location name) was outstanding. The quick diagnosis of the ambulance team confirming dad had sepsis, saved his life. The doctor’s & nurses on A&E (location name) were all kind, considerate and understanding. An absolute credit to the NHS.” [Type 1, A&E]
“Depsdite being in agony with my hand, it was a brillaint experience, i felt very well lookeed afrer and the staff were lovely and freindly and efficient, really felt like they wanted to help not just doing their job.” [Type 3, UTC]
Theme: staff
What does the quantitative data tell us?
Type 1 (A&E): 67% reported having confidence and trust in doctors and nurses examining and treating them (Q21).
Type 3 (UTC): 75% reported having confidence and trust in doctors and nurses examining and treating them (T18).
Type 1 (A&E): 70% felt that they had been treated with respect and dignity ‘all of the time’ during their stay (Q42).
Type 3 (UTC): 81% felt that they had been treated with respect and dignity ‘all of the time’ during their stay (T39).
Staff were found to play a critical role in shaping the experience of care in urgent and emergency services, showcasing how every individual within the workforce can have impact.
Personal attributes
Comments about staff referred to their personal qualities and characteristics that were seen to support delivery of high-quality care. Being compassionate, helpful and kind were personal attributes that were highly valued as these helped to provide comfort and reassurance.
“I don’t fully remember my visit to urgent care as it was a few months ago but what I can remember is that the staff who treated me were the kindest and helpful people I’ve ever been treated by.” [Type 3, UTC]
“SDEC team were absolutely brilliant right from the healthcare assistants to the nurses and doctors, cleaners etc, they were all very good and approached everything in a person-centred way whist being thorough with their investigations.” [Type 1, A&E]
“A massive thank you for all the lovely staff at (location name) I saw that day. The A&E staff were so good at informing me, especially as was very nervous – Broken wrist, they were all very good and helped me stay calm and explained everything. Can’t fault the service provided at all levels. Big thank you to the team.” [Type 1, A&E]
“I would describe myself as a ‘difficult’ patient when giving blood. The A+E staff were extremely professional and understanding. Both doctors and nurses were reassuring and caring throughout my visit to (location name) A+E.” [Type 1, A&E]
“One of the nicest bunch of people I’ve had the pleasure of spending 10 hour with.” [Type 3, UTC]
“The staff were so helpful from the moment I arrived and made me feel at ease. Nothing was too much trouble for them.” [Type 3, UTC]
Professional attributes
Professional attributes of staff were described in the context of being treated. Examples spanned efficiency, knowledge, and competency of staff with the impact often described as reassuring.
“During my time in the A&E department, I was thoroughly impressed by the professionalism, efficiency, and compassion of the staff. From the moment I arrived, I was greeted with warmth and empathy, which immediately put me at ease despite the circumstances. The medical team worked seamlessly together, communicating effectively and ensuring that I received prompt and thorough care. Every step of the way, I felt supported and well-informed, as the staff took the time to explain procedures and answer any questions I had.” [Type 1, A&E]
“(name) was excellent. I couldn’t have had a better consultant. He treated me like one of his own and made me feel extremely comfortable. Everything that he said would happen post-surgery happened so I was expecting it. He was amazing, knowlegeable, kind, caring, noble and so easy to talk to. I can now exercise and move amazingly functionally.” [Type 3, UTC]
“I wouldn’t recommend going to A and E, it’s not a vacation location, some scary things going on in the waiting room, but the people working there were excellent, professional, approachable and caring. It’s good to know we have people like this in times of need. Thank you.” [Type 1, A&E]
Other professional attributes highlighted positively were being listened to, and being treated with respect and as an individual. Experiencing these engendered confidence and trust.
“The general feeting was confidence in all staff who were involved with my ‘case’. I was treated as an individual by all staff.” [Type 1, A&E]
“I was at A&E (location name), treated with sympathetic care, respect, and also consideration for my advanced age… I felt certain I mattered to them and that is such a wonderful reassurance to any human being, specially when is offered with a smile and gentle kindness. I thought they were an amazing lot of individuals.” [Type 1, A&E]
“The staff are friendly, polite and always listen to what I have to say. They work with me as a whole person and are positive about treating me, despite my complex medical conditions.” [Type 3, UTC]
“Professional and efficient as always. Easy access and respect for my disability.” [Type 3, UTC]
“Overwhelmingly positive experience. Treated as an individual by a team of individuals. Thank you all for dedicating your lives to the wellbeing of others.” [Type 3, UTC]
Feedback about professional attributes sometimes included references to specific individuals or teams, with patients keen to show their appreciation. This is evident even where patients were unable to recall names but still wanted to highlight their positive experiences with staff.
“I’m gutted that I can’t remember the doctors name that I saw, but he was absolutely fantastic and I cannot thank him enough.” [Type 3, UTC]
“The nurse that I seen at the urgent care was the nicest healthcare professional I have seen I think her name was (name) but I’m not 100% sure, she was very caring and explained everything to me and made me feel at ease.” [Type 3, UTC]
“I had a very good experience with the treatment and was really impressed by how quickly it went and how nice the nurses and the consultant who specialised with broken or sprained ankles so I felt like I was treated fairly and good, nothing more they could of done, and I appreciated everything they did. Thank you.” [Type 3, UTC]
“All the staff who assists me were very friendly and helpful. The doctor who treated me was excellent. The whole experience was very good and very professional.” [Type 3, UTC]
Staff attitudes
In direct contrast to the positive experiences shared, those reporting negative interactions with staff highlighted how pivotal staff attitudes could be in defining the overall experience. In these comments, it was often individual staff members who were the source of the negative experience. Some comments indicate staff stating to the patient that they should not have attended the setting, linking to the ‘Avoidable access’ sub-theme explored later in this report.
“Extra triage nurses would have been good. I had a poor experience with two very impatient junior doctors who weren’t particularly understaning as I tried to keep it together.” [Type 1, A&E]
“Triage nurse was so lovely and helpful, as was the GP who treated. The receptionist, however, was incredibly rude, unnecessarily hostile and unhelpful. Vile individual. I sat for an hour and watched her hostility towards everyone who attended.” [Type 3, UTC]
“The 2 drs and nurse I saw whilst getting assessed, ie taking my bloods and ecg made me feel like I was wasting their time. Kept twisting my words and one dr even laughed when I said I was advised to come in by my private healthcare GP exclaiming that they’re weren’t proper drs and thanks to them I’ve put a strain on NHS resources.” [Type 1, A&E]
“The nurse who dealt with me was overbearing, talked over me and wouldn’t listen to my concerns. She stated that I shouldn’t have come if I wasn’t going to listen to her professional medical advice. She was so arrogant and tried not to treat me, until I became insistent of what was required.” [Type 3, UTC]
Other feedback around staff interactions highlighted the negative impact of dismissive attitudes towards patients and their concerns. Patients shared experiences with staff members at reception and during assessments which left them feeling ignored or that they had not truly been heard.
“Personally have felt victimised by nurses and doctors alike at this hospital, being ignored, being told I am ‘seeking’ pain relief to feed a habit, being told to ‘stop stuffing my mouth with food’ instead listening to symptoms and my complaints very nearly killed me, luckily for me a doctor coming into his shift looked over my scans during handover and noticed I was infact not lying about my pain, I had multiple blood clots, internal bleeding, a ruptured spleen AND deep into a hypoglycaemic episode.” [Type 1, A&E]
“Triage nurse was just off to the side of the waiting area, no separate room or even a curtain. She was extremely dismissive, asked standard questions and didn’t wait for my response.” [Type 1, A&E]
“I have never been happy with the registration or reception staff. No eyes contact, no smile or approachable. I’d understand it’s A&E department and busy, but this is a hospital where everyone attending are in need of care.” [Type 1, A&E]
“Staff are particularly rude when patients enquire about wait times, and sit talking to each other about their weekends, rather than seeing to patients, who they then accuse of being rude.” [Type 3, UTC]
“The triage nurse that I spoke to was very abrupt, patronising, and dismissive of my health concerns despite me being advised to attend Urgent Care by my hospital treatment team.” [Type 3, UTC]
“The staff are often rude and give you very little information, they are very blunt and often leave you waiting very long periods of time without update or assistance.” [Type 3, UTC]
“Doctor/ANP who saw me was extremely rude, dismissing what I was saying before even allowing me to finish and was instructing me to just go home. I really felt like I had to argue my case to be seen which I had not been prepared for. I felt very disrespected and overlooked and had it been a stress fracture the outcome could have been very different.” [Type 3, UTC]
Discrimination
While rare, a few patients reported discrimination relating to a protected characteristic. These examples are noteworthy exceptions against the backdrop of high praise for staff more typically shared. Patients described feeling that their treatment was incomplete because of this experience.
“I completely understand that they deal with a lot of people and this is no easy task, however I feel slighted because as an African person who had to pay for these health services and not get the basic services put my mental health and physical health in a precarious situation.” [Type 1, A&E]
“The care at this Hospital is worse, Rheumatology at (location name), I have this condition Gout and then this hospital can not diagnose my condition, I had blood test but the Doctor that tend to me was racist, and also asking me silly question.” [Type 3, UTC]
“On occasion I have asked politely that I be referred to by preferred pronouns for my own comfort, which has either been fully ignored or seemingly laughed off.” [Type 3, UTC]
Capacity
Explicit mentions were made of the pressures facing staff in regards to capacity. Some comments demonstrated well how this can lead to even greater appreciation of positive experiences with staff when patients held a view or had experienced first-hand the capacity challenges the NHS workforce can face.
“I couldn’t fault the A & E department, the staff are friendly & polite considering the amount of pressure they are under & I would like to thank them for their commitment to the hospital.” [Type 1, A&E]
“Staff are under extreme pressure and still do a outstanding job so they are a credit to the NHS.” [Type 1, A&E]
“The staff worked very hard and were thorough but there just wasn’t enough of them. When one of them took a break, nobody was tending to the patients in our waiting room who needed drips, painkillers and toilet breaks.” [Type 1, A&E]
“Considering the pressure put on the NHS I was treated with respect, courtesy and was never made to feel that I was an inconvenience, thankyou to all concerned for a sometimes thankless job well done.” [Type 3, UTC]
“The staff in A&E are in the main, great, but are under too much pressure. It fills me with dread when I have to go there. It’s a war-zone!” [Type 3, UTC]
“They really need to have more doctors/paediatrician, as there are so many babies/kinds in emergency. And in our case, our daughter’s condition could go Downhill within a few hours very rapidly.” [Type 3, UTC]
Feedback included mentions of the number of staff being too low and how, in their view, this could impact on experiences of care. This was more often seen in the comments from A&E patients. In these examples it was acknowledged to be a systemic problem and not a criticism of the staff as individuals.
“Staffing levels between admin and clinicians needs to be looked at, there is no need for 6 receptionists at one time when the desk sits 3 at max.” [Type 1, A&E]
“There was a system of sorts not enough senior staff and not a doctor in sight all of the 5 hours I was there.” [Type 1, A&E]
“The hospital is under funded needs more staff to carry out day to day care and support for patients and their family member’s.” [Type 1, A&E]
“Length of time waiting in A&E to be seen. Once on the other side of A&E you can see how hard the medical team are working to cope. I was lucky in that the A&E doctor with me was extremely helpful. I feel the answer to the current situation in A&E is that more doctors/nurses etc are needed.” [Type 1, A&E]
Theme: access routes
There was a range of access routes into urgent and emergency care services evident in written feedback, with several patients sharing this information as a focus of what could be improved about their experience. This demonstrated that there were opportunities, both within and beyond the A&E or UTC setting, that could be a focus for improvement.
Avoidable access
What does the quantitative data tell us?
Type 1 (A&E): 66% had contacted another service before attending (Q1).
Type 3 (UTC): 50% had contacted another service before attending (T1).
Type 1 (A&E): Among those who sought prior advice, 40% had called NHS 111 (Q3).
Type 3 (UTC): Among those who sought prior advice, 48% had visited a GP practice (T3).
Type 1 (A&E): 68% said their main reason for attending A&E was another service directed or advised them to do so (Q4).
Type 3 (UTC): 56% said their main reason for attending UTC was another service directed or advised them to do so (T4).
Feedback included patients who themselves recognised that urgent and emergency care was probably avoidable for their situation. Some stated a preference to access care elsewhere but due to difficulties, both experienced and perceived in resolving their situation, had used urgent or emergency care instead.
“The problem I needed a consultation for was something I felt I should have been dealt with at my GP surgery and did not really need treatment at the urgent care centre, but was still urgent enough that I needed an examination by a doctor. Despite speaking to a GP before I went to urgent care. I felt they did not regard my problem as urgent enough to fit me in to their schedule.” [Type 3, UTC]
“I was very disappointed with the way I was treated by the doctor from 111 and in the end I had to wait until after the the weekend to go to my doctor which resulted in me attending the A&E this could have been avoided.” [Type 1, A&E]
“After trying my GP ((location name) Medical Centre) and being told the first appointment would be in 2weeks time and that would be a telephone call I went to the Pharmacist at (location name) Chemist who was very helpful but said I really needed to see a doctor as my neck was inflamed.” [Type 3, UTC]
“It seemed my only option to use the MIU as my GP practice did not provide the regular availability with my working hours to provide the treatment needed.” [Type 3, UTC]
“If it had been possible to have a face to face appointment with my local surgery I would not have had to try various ways to get treatment, saying that the pharmacist was very good but couldn’t help me.” [Type 3, UTC]
Several patients shared examples of directly being told that they shouldn’t be using urgent and emergency care by a member of staff. This was experienced negatively in most examples, finding it rude and/or upsetting, linking this insight to the sub-theme ‘Staff attitudes’ detailed earlier in this report.
“When I finally saw the doctor, he dismissed me within minutes saying I should not be there as I should have made an appointment with my GP. He didn’t examine me properly.” [Type 3, UTC]
“I arrived in a&e waited for hours just to get spoken to like I shouldn’t of been there and more or less told to not bother them and go home so I walked out in tears.” [Type 1, A&E]
“The first thing the health professional said to me in triage was: ‘So you think it’s appropriate to come to A&E for athlete’s foot?’. This was before even looking at my foot and was very rude.” [Type 3, UTC]
“Woman at reception was not very friendly and said I should have been at A&E, I told her they had sent me there and she clearly was unhappy about it and let it show.” [Type 3, UTC]
Primary care
Building on comments earlier shared about ‘Avoidable access’, feedback from Type 3 patients indicated that an UTC was sometimes used as an alternative when they were unable to secure an appointment in General Practice.
“I couldn’t get an appointment with my GP so went to the Walk-in Centre.” [Type 3, UTC]
“The treatment, information and advice I received was wonderful. Howevery, the GP practice should not have to direct patients to this service due to no capacity themselve I rang GP at 08:00 and advised to use urgent came. This is not what hospital services are for. Tha fault is with GP surgeries!!” [Type 3, UTC]
“I had to go to the treatment centre as I could not get an appointment at my GP.” [Type 3, UTC]
“I have used this centre a number of times for a few conditions (infections and wounds, usually when GP services are unavailable).” [Type 3, UTC]
“The reason I went to urgent care was because I had been trying for 3 weeks to get an appointment at my Doctors. When I left urgent care I was told I needed a doctors appointment so they could refer me to see a specialist. I eventually was given an appointment at a different doctors surgery.” [Type 3, UTC]
Further comments indicated patients were sometimes directed to an UTC by a healthcare practitioner in primary care. For those who experienced ‘Staff attitudes’ linked to ‘Avoidable access’ this highlighted a disconnect between primary and urgent care as to what was considered appropriate for referral and/or access to be made to an UTC.
“There is a recognition amongst healthcare professionals in the UC setting that this is exactly what they are experiencing and are re-directing some patients back to their GPs. He asked why the GP sent me & made me feel silly & also proceeded to make judgemental comments about me running & that I should swim insted.” [Type 3, UTC]
“The centre were brilliant ONCE we had overcome the issue that they wouldn’t see me because my GP had suggested I go as she suspected I’d broken my leg.” [Type 3, UTC]
“I was sent to A&E by my doctor due to very high blood pressure, chest pains. When seeing doctor they did not take time to read my notes or ask about my symptoms. The doctor asked why I had come in for ‘stomach pains’. My paperwork also seemed to have incorrect information on it.” [Type 3, UTC]
NHS 111
Contact with NHS 111 was often mentioned, with varied experiences shared. It was common for patients to specify that they were directed to attend urgent or emergency care by NHS 111. Some comments where this was mentioned indicated that individuals were reluctant to use urgent and emergency care and had been seeking an alternative when they called NHS 111.
“We called 111 to explain my symptoms and the circumstances, to which they sent out an ambulance to take me to (location name) A&E, I didnt want to go.” [Type 1, A&E]
“Nurses/doctors were nice and friendly, though I often felt as though they didn’t understand why I had come to A&E with the condition I had, even though it was the NHS’ own service (111) that told me to.” [Type 1, A&E]
“Told by 111 to attend UTC as I was passing a large amount of blood.” [Type 3, UTC]
“We brought her in after seeing the GP and having a video appointment with the 111 clinician who advised us to bring her in due to atypical rash that was rapidly spreading, diarrhoea, fever, cough, congestion.” [Type 3, UTC]
Frustrations were shared when patients experienced long waits when directed to urgent and emergency care services by NHS 111, especially if alternative settings were discussed retrospectively, while being treated.
“The 111 service had already told me to go to A&E with my post operation symptoms. This was an unnecessary step, but 111 doesn’t seem to be linked into the hospital receptions.” [Type 1, A&E]
“According to the doctor I eventually saw after hours of waiting (not brilliant when having a hypertensive crisis) the 111 service should never have sent me to (location name) Emergency service.” [Type 3, UTC]
“I was sent to the Urgent Care centre in (location name) which was quite busy and I was told I should have go to the UC in (location name) next time. Apparently the operators at 111 should have sent me there as they have more staff on.” [Type 3, UTC]
“I will not call 111 service again in the middle on the night left for hours on end at A and E with no updates and when I asked I was given no information.” [Type 1, A&E]
“Huge disconnect as well from the urgency that 111 portrayed, if I had known how dismissively the person in a&e was going tontreat me i wouldnt have attended. I felt dismissed, my concerns undermined, and poorly assessed, and was very disappointed by the whole experience and felt more worried about my health despite visit.” [Type 1, A&E]
Examples of misunderstanding or miscommunication were also evident, with some patients attending A&E or an UTC on the premise that they had an appointment or would be expected by the setting. This could lead to frustrations when this didn’t happen.
“NHS111 said the urgent care centre would have the details of the call and know I was coming. This wasn’t the case so I had to repeat everything to the receptionist. This was a shame as a connected service would have been all the better.” [Type 3, UTC]
“NHS111 booked me into A&E for 18.15. I thought that was my appointment time. When I told the reception I had an appointment for then she said ‘There are no appointments, you’ll just have to wait like everyone else’.” [Type 1, A&E]
“I came to A and E with an appointment time that was made when I called NHS 111 for advice. On arrival it became clear quite quickly that the appointment time meant nothing and was made to wait for hours.” [Type 1, A&E]
“I was told by 111 that I would have an appointment at 11 at the Urgent Care Centre. When I got there I was told I had to sit in A&E, so why was I told I had an appointment.” [Type 3, UTC]
“The 111 service has booked my appointment but the receptionist had no record of it which was the only distressing part of the appointment.” [Type 3, UTC]
“The information given by 111 was misleading. They said an appointment was made but the urgent care centre I visit was **** a first come first serve basis.” [Type 3, UTC]
In contrast, other patients shared positive experiences of the co-ordinated care between NHS 111 and A&E, which they felt expediated their access to treatment.
“I have nothing but praise for the A&E and 111, as I have a blood cancer months ago I was coughing up brown liquid, phoned 111 they were here in 10 minutes and was taken straight to A&E or had a scan and had an emergency operation for strangulated hernia.” [Type 1, A&E]
“Through my contacting 111, by them asking me lots of questions, by the time I arrived at A&E they had the relevant form in front of them. I went straight for an ECG, no waiting.” [Type 1, A&E]
Vulnerable patients
Feedback from individuals who shared they had specific needs or vulnerabilities often included requests for different access or separate areas to minimise the risks they felt were involved when attending urgent or emergency care settings. While there are strong links to the ‘Waiting’ theme detailed later in this report, examples from vulnerable patients indicated that their requirements were broader, including access and treatment. This included those who knew they were immunocompromised asking for an effective, dedicated and separate area at A&E to minimise the risk of infection.
“As I am on chemotherapy treatment, it was concerning to have to wait, for hours, in a room full of ‘ill’ people. I wore a mask but it did make me anxious. Although I was fast tracked (5 hours wait, instead of 8), I think I should have been given the chance to sit in a room, away from the crowds. This should really be offered to all those with reduced immunity.” [Type 1, A&E]
“I am immune suppressed and so should have been isolated in A&E. I sat in an area cordoned off from the rest of the seats by a flimsy fabric partition, and felt very unsafe. This ‘isolation’ area was purely voluntary – A&E was so crowded that anyone could – and did – sit there as seats were vacated.” [Type 1, A&E]
“When I went to A&E I was sent from oncology from (location name) out of hours service, I was left in the main reception for over five hours even though I explained I had had chemotherapy a few days before leaving me open to all sorts of infections. I wasn’t feeling well due to the chemo but still left in reception.” [Type 1, A&E]
There were also comments from patients with diagnosed mental health conditions who felt they should have been afforded more consideration given their condition or offered some form of different access to avoid aggravating their situation.
“Those who are in the same situation as me and have serious mental problems should be treated separately and better and faster, but they don’t care about this issue and when I asked for help, they often behaved indifferently and rudely. This has made me avoid going to the hospital and treatment in the A&E department despite the need.” [Type 1, A&E]
“My COMBAT PTSD was affected, I felt alone and vulnerable. No Priority Service under the Armed Forces Covenant. I have sensitivity to light and sound, it was a nightmare for me. Too bright and very noisy.” [Type 1, A&E]
Similar, but more general comments relating to vulnerabilities were also made by patients who felt they were putting themselves at risk by attending A&E or an UTC, due to the potential for contact with other ill or dangerous patients, including where specific vulnerabilities were unclear.
“I feel that there should be a separate area for vulnerable patients with more comfortable chairs and more space between patients.” [Type 1, A&E]
“Lots of people in attendance who had contagious conditions (chest infections etc). Didn’t want to get near them but had no choice. Masks should be worn & patient advised to sit apart if has a contagious condition. I have a germ phobia!” [Type 3, UTC]
“I found the whole experience very stressful especially when you are not feeling well. I will always think twice about going to the UTC as I feel you could end up coming away with picking up more infection.” [Type 3, UTC]
“I was terrified. I tried on my own life but I waited alone with no support the entire night and morning. The other patients in the waiting room were dangerous and no one checked if I was safe. It made me feel hopeless at the time and had no faith in the mental health system.” [Type 1, A&E]
Of note were comments from people who were pregnant seeking more consideration and understanding of the specific needs that they had, particularly those experiencing miscarriage.
“I was left in agony lying on the floor of an and e whilst experiencing a miscarriage.” [Type 1, A&E]
“I would have liked to be prioritised as I was heavily pregnant at the time. The walk-in centre had prioritised me for triage and assessment before advising me to go to A&E.” [Type 1, A&E]
“I was pregnant 38weeks and in lots of pain and I waited 5 hours and half. I wasn’t able to sit for long or stand it was a bit too much. I believe there is a problem with system I terms of staff or procedures.” [Type 3, UTC]
Another notable theme in the comments related to the need for better communication support, such as BSL interpreters, so that patients could fully access care, feel involved and have a clear understanding of what was happening to them. This was only found in comments from Type 1 (A&E) patients.
“it was difficult to communicate with the doctor. I could not explain what hurts i had. and I missed it when the doctor called my name but I couldn’t hear it. I need a BSL interpreter at this hospital.” [Type 1, A&E]
“The patient is profoundly deaf (since birth). There was no accessible to get BSL interpreter. I had to call to my support worker, who acts as my interpreter.” [Type 1, A&E]
“I’m sorry but I’m not good at English and I can’t explain it to you in detail. This is the reason why I asked for a translator.” [Type 1, A&E]
Theme: waiting
What does the quantitative data tell us?
Type 1 (A&E): 29% reported being seen within 15 minutes for their first assessment (Q11).
Type 3 (UTC): Among walk-in patients, 34% were assessed within 15 minutes (T8).
Type 3 (UTC): Of patients that had a booked appointment, 64% were assessed within 30 minutes (T8).
Type 1 (A&E): 74% said they were not informed how long they would have to wait to be examined or treated (Q13).
Type 3 (UTC): 61% said they were not informed how long they would have to wait to be examined or treated (T10).
Type 1 (A&E): 64% of visits lasted more than four hours (Q16).
Type 3 (UTC): 30% of visits lasted less than one hour; 18% lasted more than four hours (T13).
There was predominantly negative feedback shared about the experience of waiting, though some expressions of surprise were made as to the speed some patients were treated and cared for. This theme demonstrates that the experience of waiting is very diverse, individual and context specific for many patients. Please also note there is relevant insight shared within the theme ‘Facilities and environment’ as to other factors which impacted on the experience of waiting.
Acceptance of waiting times
There is evidence that patients arrive expecting to have to wait when they access urgent or emergency care. However, among those who commented on the experience of waiting times there lacked consistency as to what would be considered a reasonable timeframe. Diverse examples were shared as to when patients’ thresholds of tolerance or their acceptability levels of time waiting were surpassed.
“I felt my experience in A&E was marred by having to wait in a wheelchair for over 2 hours to be seen. I understand that is not an overly long time but I was told that because I had had surgery 2 days before I would be seen quickly.” [Type 1, A&E]
“I waited to be seen by a doctor for over 2 hours, nobody told me it would be this long and other people went in before me.” [Type 3, UTC]
“The wait in the department was exceptional, and I was kept in the waiting room for 12+ hrs despite being triage to majors.” [Type 1, A&E]
“Waiting time was too long I attended … 10pm I wasn’t seen by a doctor until 8am the following day then transferred to another dept at 4pm to be sent home at 7pm to come back the following day for scans.” [Type 1, A&E]
“I waited at A&E for test and results for nearly 12 hours, I left without these result
‘Long’ wait times
As demonstrated earlier, there was variation amongst patients as to what was considered ‘long’ in terms of waiting times. Some comments explicitly referred to the wait being ‘long’ while in others it was inferred through statements that improvements in waiting time were needed.
This insight links to the ‘Trust and confidence’ sub-theme outlined earlier, when wait times did not match the patient’s sense of urgency as to how this undermined their confidence. Rarely did patients clarify which part of their experience required them to wait, though when shared, examples varied and included amongst others, waits for assessment; for triage; to be treated; and for medication.
“Better waiting times” [Type 1, A&E]
“Waiting time is too long” [Type 1, A&E]
“To be seen by the doctors in less than an hour if possible. Thanks” [Type 1, A&E]
“I have visited the [location] centre in the past and have always been treated very well. The only issue is the time spent waiting.” [Type 3, UTC]
“The time between triage and being seen by a doctor needs to be shorter.” [Type 3, UTC]
Impact of waiting: self-discharge
Regarding the impact of waiting, it was observed in the data that several patients left the service and/or discharged themselves due to the length of time that had either passed or was anticipated to be spent waiting to receive care. It was often unclear if these patients accessed and received care elsewhere thereafter.
“I was left to sit in A&E for over 12 hours, and staff didn’t know I was there. Discharged myself.” [Type 1, A&E]
“I did not wait to see a doctor because I was told I would be waiting for four hours.” [Type 1, A&E]
“After just 6 hours of waiting, I went home without medical care.” [Type 3, UTC]
“Waited over 20 hours and still no blood results discharged myself as I needed somewhere to sleep.” [Type 1, A&E]
“I discharged myself because the wait was too long and no estimate given of how long till I was seen” [Type 1, A&E]
“I was told by hospital staff that they cannot guarantee if I would be seen by health practitioner (nurse/doctor) today! I waited several hours and then went back home because my condition was worsening due to tiredness.” [Type 3, UTC]
“Never got seen it was a heart problem I had I think but nobody seen me waited 4 hours and went home, will never bother with the NHS ever again.” [Type 3, UTC]
Pharmacy access delays
Of note, there were several patients that spoke of delays in accessing prescribed medication due to the closing times of the hospital pharmacy.
“I had to return the next day as hospital pharmacy only place that could issue medication. I believe the pharmacy should not close so early. The queue following day at 9am had hour wait.” [Type 3, UTC]
“I had come back to the hospital to collect my medication because when I left the hospital around 5am the pharmacy was closed? I didn’t expect that the pharmacy inside the hospital can be closed.” [Type 3, UTC]
“Finally I saw a doctor who prescribed antibiotics immediately, but then told me the pharmacy was closed 5.15pm. Surely they should stay open later to help people?” [Type 1, A&E]
“I was also prescribed medication but was not able to get this from A&E as the pharmacy was closed at that time of night and I was told to call my GP to get a prescription.” [Type 1, A&E]
Speed and efficiency
While not typical, there were patients who were impressed with how quickly and efficiently they had been seen and treated in urgent or emergency care. This was sometimes shared in such a way that inferred there were low expectations held by patients, which had been easy therefore to exceed. As with the sub-theme ‘Acceptance of waiting times’ there was no consistency identified as to what timeframe was considered ‘quick’ or ‘efficient’ and examples varied.
“The triage nurse had mentioned that the scan would probably be done at [location] and I asked the doctor if that was possible. He agreed and 30 minutes later I had the scan and was discharged.” [Type 3, UTC]
“I was treated very quickly and efficiently no problems at all.” [Type 3, UTC]
“I was treated very well. The staff were all very kind and professional and there was hardly any waiting time.” [Type 3, UTC]
“After sustaining a deep leg wound, my treatment at [location] hospital was extremely good, expecting a prolonged wait the triage nurse assessed my condition and treatment shortly followed.” [Type 1, A&E]
“I was seen quickly because of cardiac condition but clearly others kept waiting long time with no privacy or facilities.” [Type 1, A&E]
“Given the reports on how bad the NHS is, I had no issues or delays in the whole process from dialling 999 to being admitted to the hospital.” [Type 1, A&E]
“Waiting times are always extremely reasonable and the staff are friendly and efficient. What more can you ask for?” [Type 3, UTC]
“I was triaged after about half hour. Then straight into x-ray after 5 min, and then to doctor 10 min after that. Amazing service.” [Type 3, UTC]
“I just feel they were very good, one of the best hospitals I have been to. I would recommend it, and I have met others that had the same level treatment. It was very quick, I was back home within two hours of leaving for the Urgent Treatment Centre.” [Type 3, UTC]
Managing expectations
A lack of communication while waiting for an initial assessment was raised as an issue which created additional anxiety and stress. Examples highlighted the need to manage expectations, with patients looking for clear and up to date information on the status of their wait to help minimise their frustration.
“Would be nice if there was an update about how long the wait would be realistically. If it’s going to take 6 hours I don’t mind but would rather be told the truth than being told that the wait is 2 hours then having to wait 6 hours.” [Type 1, A&E]
“I wasn’t given any information about the waiting times. I was told to sit in the main waiting area in A&E. After asking several times, 4 hours later I was told by a nurse that I shouldn’t be sitting here and should be in the urgent care centre. This made me very angry as there was no communication whatsoever.” [Type 3, UTC]
“To take the stress out of the wait, it would help if some form of communication could be provided electronically about patients position in the queue.” [Type 1, A&E]
Communication methods
Comments highlighted the difficulties attached to large, crowded waiting areas such as individuals waiting to hear their name being called, meaning they missed this even when vigilant.
“I sat and waited patiently in the main waiting area which got busier and noisier but I stayed in the same place and listened out for my name to be shouted. After hours I was then phoned to ask if I was still in the hospital as they had apparently shouted me and received no answer. I had a family member with me, neither one of us heard my name being called. We were right next to the reception desk and heard plenty of other people being called. I would suggest that if staff are expected to bellow names this will delay patient care. Electronic systems better.” [Type 1, A&E]
“The only comment I would make is to say that the waiting room was overcrowded and very noisy and consequently it was very difficult to hear when your name was called out for treatment. In fact I did not hear my name being called out to see the doctor for the first time.” [Type 3, UTC]
Some comments highlighted that electronic boards were either unavailable when needed or not consistently updated, which contributed to the frustration of waiting. Note the link to ‘Managing expectations’ as a sub-theme shared earlier.
“I think the hospital should provide information of the waiting times by means of an electronic sign in the waiting room. I had to ask a nurse after five hours when I hadn’t been seen by a doctor.” [Type 1, A&E]
“Had to find out for myself how long I would be before seeing a doctor as no information available on boards anywhere!” [Type 1, A&E]
“The electronic info. System was not up to date which was mistaking re-timings. And to be in the department for so long was really frustrating.” [Type 1, A&E]
“The waiting system needs to be amended. I was having a heart attack and expected to move seats as soon as a person was seen for treatment. A numbering system is required so people can remain seated.” [Type 3, UTC]
Theme: facilities and environment
Predominantly experience was discussed in negative terms and there were lots of suggestions to improve the facilities and environment of urgent or emergency care settings. It is noteworthy that most of the feedback within this section of the report, speaks to the experience of ‘Waiting’ and is linked to this key theme closely. There are also interconnections between the sub-themes shared within this section whereby one issue experienced is seen to impact and/or lead to another. For example, the experience of overcrowded waiting areas can contribute to feelings of being unsafe.
Food and drink
What does the quantitative data tell us?
Type 1 (A&E): 44% who wanted something to eat or drink reported ‘always’ having access to food and drink (Q32).
Type 3 (UTC): 47% said they were ‘always’ able to get food or drinks (T29).
Many comments regarding facilities focussed on there being a lack of access to food and drinks, including water. This was experienced both while waiting for their first assessment and after their first assessment, particularly for those who attended A&E. It appeared there was variation in the offering across settings, though notable was the pattern of feedback highlighting that there was no access to cafes; restaurants; shops; and vending machines. In terms of impact, there was mention of hunger and (de)hydration, as well as mention of risks for vulnerable patients such as those with diabetes.
“Waiting room too small with poor facilities and little to no refreshments.” [Type 1, A&E]
“My main problem was access to water and because of being sent for tests over meal times, food. As this was served from trolley at set times and not overseen due to pressure on qualified staff. It would have been helpful for staff to have access to bottled water or equivalent in the lockers beside bed as requested items often got forgotten due to other urgent situations.” [Type 1, A&E]
“Was never offered a drink of any kind in A&E. Yet there are posters up about staff keeping one hydrated!” [Type 1, A&E]
“No food and drink in the children’s waiting area, the vending machine is in other area where I could not go whilst my son was sleeping on a coat on the floor.” [Type 1, A&E]
“Have access to food (warm) there was no source to get something to eat other than vending machine.” [Type 1, A&E]
“I’m diabetic, on insulin, no food or drinks were left with me…I felt very vulnerable. I had to call out to someone in the corridor at 9am, to ask for some breakfast and so I could take my insulin.” [Type 1, A&E]
“The principal issue I had whilst waiting to be admitted to a ward was that there was little food offered to me; even though I was in this holding area for about 27 hours. During this time I had about 3 sandwiches.” [Type 1, A&E]
“I was there nearly 4 hours (11am-3pm) and was ravenous! Cafe/restaurant closed, got a sandwich.” [Type 3, UTC]
“Would have been helpful to have food available while waiting. Just a machine with choc etc. A sandwich etc trolley would be good to have come round and would do a great trade.” [Type 3, UTC]
Physical comfort
Another key area of focus regarding facilities was how the chairs in waiting areas were uncomfortable. A connection was made by some patients to waiting times when describing this experience, i.e. the longer they waited, the more uncomfortable they became in the chair(s) available.
“The chairs in the waiting room couldn’t have been more uncomfortable if you tried. This alone puts me off going back to [location] A&E.” [Type 1, A&E]
“I was in a lot of discomfort in the waiting room. The chair provided made it more difficult to get comfortable. I would ask that some more comfortable seating would be provided.” [Type 1, A&E]
“My pain was a 9 on a scale of 1-10 and sitting for 4 hours on uncomfortable seats was awful.” [Type 3, UTC]
“I was in a lot of discomfort in the waiting room and could not sit on the hard chairs and was left waiting for much longer than the 1 hour I had been told without receiving any updates on expected waiting time.” [Type 3, UTC]
In terms of impact on patients, the lack of comfort while waiting was described by some as exacerbating symptoms. This included those who could not find seating at all, with some concern noted over vulnerable patients particularly.
“Seating. It’s awful. When you’re sometimes there for 6+ hours the seating is so uncomfortable. There’s no way near enough space – the chairs hurt and you leave feeling worse.” [Type 1, A&E]
“I had severe spasms and the hard chairs in the waiting area were hard and very uncomfortable to the extent that even if I had no pain it would be so.” [Type 1, A&E]
“I told my husband I wanted to go home due to the pain and swelling in my leg because I need to lay down. My routine at home is sitting for a maximum of 10 minutes then laying on my bed to keep my leg elevated to prevent swelling as directed by my orthopaedic consultant.” [Type 1, A&E]
“I had a severe back pain and the waiting made it worse. I asked if I can wait somewhere more comfortable than a chair and they said no. Also everything was closed in the hospital I couldn’t find place to buy food or drink for 7 hours.” [Type 3, UTC]
“I rated my experience as 6 based on the waiting area. There were not enough seats available for all patients, some of the patients were elderly and children and they were very poorly and unable to stand for and wait for long hours. In addition, the cleanliness of the place wasn’t good either.” [Type 3, UTC]
Cleanliness
Cleanliness was commonly mentioned as an issue in comments focussed on the environment of the setting. While some patients acknowledged that the volume of people would make cleaning difficult, unclean facilities were felt to be unacceptable and contributed to a sense that there was a lack of care. Of note is that issues of cleanliness were identified typically during the patients’ experience of waiting for care, relating primarily to toilets but also to floors and lifts.
“The hospital was crowded and hard to get a seat and was dirty with stuff on the floor and rubbish on the sides. The toilets were dirty and someone was being sick in there and it wasn’t cleaned afterwards. One of the patients walked out saying they would kill themselves and wasn’t seen again after that in the waiting area.” [Type 1, A&E]
“On all visits to A&E. I found the toilets to be very unclean, unhygienic very dirty. They are always dirty. This needs to be addressed it seems no-one cares.” [Type 1, A&E]
“It was dirty the floors needed sweeping and cleaning for a few hours there was no toilet in use because they were flooded urine also on the floor I personally reported it a number of times people were desperate it was disgusting a person in their slippers went in and their feet were soaked in urine.” [Type 1, A&E]
“The physical conditions in the A&E waiting area/reception need to be addressed. It is not up to the standard acceptable in a health setting and is grubby and it was uncomfortably cold.” [Type 1, A&E]
“Washing and toileting facilities whilst waiting for a ward abysmally poor.” [Type 1, A&E]
“Weekend cleaners had ‘couldn’t be bothered’ attitude and I saw one cleaner wipe the toilet and use same cloth to wipe the sink!” [Type 3, UTC]
“The lift was in a poor hygiene state and I can remember a strong smelly odour that was foul. Please pass this information onto the building facility management, as reactive cleaning might be necessary and hope this was just a one-off.” [Type 3, UTC]
Overcrowding
Overcrowding was experienced, particularly in A&E, with observations that waiting areas contained large volumes of people. A key cause of this were instances of patients taking (multiple) people along with them to wait for care, including children, which was not appreciated by those providing feedback. Some patients connected this to a lack of seating being available for patients, as well as a need for a calm/peaceful environment while unwell and waiting. A need to improve the management of the waiting area by staff was also highlighted.
“In the A&E admission room sometimes there tends to be large groups with patients (especially young) that take a lot of room and noise.” [Type 1, A&E]
“The waiting areas were full and some peoples attitude towards staff and other patients was unacceptable; security staff may be helpful.” [Type 1, A&E]
“Patients with multiple family members attending blocking seats for patients; 1 group had a picnic!” [Type 1, A&E]
“I spent 11 hrs sat in a chair in the waiting room, there were an average of 60 / 70 people in that one room all night, possibly 50 of those were patients the rest were friends / relatives etc, but out of those 50 patients you could tell that perhaps 25 of us were genuinely poorly people, the rest were drunks / druggies or whatever.” [Type 1, A&E]
“Lack of seating in main reception area for patients, I was unable to use the toilet at the risk of loosing the chair I was sat on to others, until I had a relative come to be with me. As some patients had more than one person with them which in my view were totally unnecessary.” [Type 1, A&E]
“Bigger waiting area as very crowded & not enough seating for everyone there.” [Type 3, UTC]
“There were several children running around and the parents didn’t stop them. When everyone there is there for a medical reason, the last thing you want is kids running riot it’s not a playground. A nurse did come out and tell them to stop as there are poorly people here thankfully.” [Type 3, UTC]
Privacy
What does the quantitative data tell us?
Type 1 (A&E): 46% felt that they ‘definitely’ had privacy when discussing their condition initially (Q10)
Type 3 (UTC): 51% felt that they ‘definitely’ had privacy when discussing their condition initially (T7)
Type 1 (A&E): 75% reported ‘definitely’ having privacy during examinations or treatment (Q25)
Type 3 (UTC): 87% reported ‘definitely’ having privacy during examinations or treatment (T22)
Feedback on the lack of privacy and how this increased feelings of vulnerability was evident. Concerns around a lack of privacy were raised predominantly by female patients. While this theme was mainly seen in A&E, with comments relating to both waiting and consultation spaces, there were also observations at the lack of privacy at reception areas in urgent care settings.
“There is a lack of privacy in all areas of A&E and the related bays/clinical decisions unit etc. Curtains do not give proper privacy. Patient details and conversations are overheard. A nurse came into the bay I was in to use the computer but she never locked it when leaving the room so I could see and potentially access confidential patient and Trust records/systems.” [Type 1, A&E]
“more privacy while checking observations etc, not in front of other patients.” [Type 1, A&E]
“There was not much room and the triage room is not locked when a patient is in there having a ECG – there was no privacy and a male doctor just came in with only a small screen barely covering the patient.” [Type 1, A&E]
“I was left to sit in a chair in reception, partially dressed as I was attached to a drip. It was the early hours of the morning I was very tired and unable to sleep due to the number of people coming in and out. There was no privacy and very little dignity.” [Type 1, A&E]
“I was in a four curtained small bay. Very noisy. No privacy others could hear all my conversation with the Staff and me theirs. NOT ACCEPTABLE. Privacy issue.” [Type 1, A&E]
“There was not enough privacy when reporting to the reception, especially when you have to discuss your private [details].” [Type 3, UTC]
“The receptionist had a propensity to be rude, and little regard for patients confidentiality. The treating doctor (not nurse) was excellent.” [Type 3, UTC]
Safety
What does the quantitative data tell us?
Type 1 (A&E): 61% said that they ‘always’ felt safe around other patients and visitors (Q31)
Type 3 (UTC): 77% said that they ‘always’ felt safe around other patients and visitors (T28)
Patients described feeling unsafe while in the waiting area in A&E due to the actions of other people, particularly when they did not think there was effective management of patient behaviour by staff. This was linked by some patients to ‘Overcrowding,’ where there were concerns raised about the ability of the setting to manage large numbers. Concerns about security were also evident, which could leave patients feeling less safe.
“The management of the waiting room was also really bad, with drunk people trying to get in fights and loads of homeless people choosing to sleep there. The security seemed to not care about this and it made my waiting time quite unpleasant.” [Type 1, A&E]
“A&E waiting area is a centre of drug dealing. Local dealers charge their phones for free and use the toilets. Because the public toilets are closed, everybody accesses the toilets in A&E behind closed doors – not safe.” [Type 1, A&E]
“The whole experience in A&E was shocking to put it mildly. There was one man taking his top off and attempting to fight with a police officer. The nurses were trying to move the patients to the other side. But elderly and myself who could not move were in the firing line. There should have been security on as one man was quite clearly on drugs and annoying patients waiting.” [Type 1, A&E]
Feedback about ‘treatment’ includes experience of investigations, tests, scans, assessments, support and medication. While experiences of treatment can be found throughout the report, a focus here highlights there was negative experience of pain management and variation in regards to mental health support particularly. The concept of trust and confidence spanned different treatment scenarios and was found to be of great importance and linked to themes shared earlier in the report of ‘Staff’ and ‘Waiting.’
“The environment was awful and not safe. I had to walk my son through very drunk and rowdy adults.” [Type 1, A&E]
“There was many shouting and arguing & that made my anxiety even worse and I ended up hiding in the toilet whilst waiting for the male who was being aggressive to leave. I then watched him open a door and enter a room where a lady was having an ECG. He was wondering round the hospital and it was very unnerving.” [Type 1, A&E]
Theme: treatment
Trust and confidence
What does the quantitative data tell us?
Type 1 (A&E): 66% said that staff completely explained the reasons for any tests in a way they could understand (Q28).
Type 3 (UTC): 76% said that staff completely explained the reasons for any tests in a way they could understand (T25).
Type 1 (A&E): Of those that had further tests, 60% felt staff had explained the results in an understandable way (Q29).
Type 3 (UTC): Of those that had further tests, 72% felt staff had explained the results in an understandable way (T26).
Type 1 (A&E): 60% said their condition and treatment were explained in a way they could understand (Q18).
Type 3 (UTC): 73% said their condition and treatment were explained in a way they could understand (T15).
Feedback demonstrated a lack of confidence some patients had in their treatment, particularly when they didn’t undergo investigations they had expected due to their symptoms. Within these comments there was an underlying sense that patients feeling ignored by staff contributed to a lack of trust, for example where their requests for specific tests were refused.
“I was in the A&E for chest pain but I did not got any screens for my heart. I think they need to do more screenings.” [Type 1, A&E]
“I was hit by a car which was traumatised my day to day life I thought I would be in the best hands but yet I felt my injuries and accident was nothing and left in the corner for hours I had pains and joint problems since the accident which the hospital could have prevented if they did the right examinations and tests they knew to carry out I felt rushed and ignored and basically push to one side considering the accident was hit by a car and basic checks was done.” [Type 1, A&E]
“Begged doctor for a scan or x-ray during 2nd visit at midnight. Doctor refused for an urgent CT scan, due to the pressure of calling on-call technicians and sent home without any meds, promised to return next day.” [Type 1, A&E]
“I came in with head injury and was not given any type of CT scan or any scan matter of fact.” [Type 1, A&E]
“Although I had multiple episodes of severe allergic reactions which could be classified as suspected anaphylactic reactions, after my visit to the emergency treatment I wasn’t referred to the Specialist Allergy Services as it is recommended by the NICE guidelines (2016).” [Type 3, UTC]
Further contributing factors linked to experience of ‘Long wait times’, particularly where these were seen to jar with the perceived seriousness of their symptoms. When patients were left for long periods, this could lead to questions over the decisions made about their treatment.
“Was not happy that I was sent to A&E with a suspected heart attack and was left sitting in a waiting room for a long period of time with no pain relief or anything else, I was told I would be having tests and none were done.” [Type 3, UTC]
“After waiting over 3 hours to be seen by the doctor I was told to go home with no treatment at all while in horrific pain. Went to a [location] urgent care centre the day after where I was seen within the hour, was examined properly and taken seriously and was given antibiotics straight and even they were shocked I was not treated the day before at [location].” [Type 3, UTC]
“Although I was satisfied that I had the opportunity to discuss my concerns with a medical professional I needed to have an urgent ultrasound scan as we thought it was my appendix however as I visited on a Sunday I was told that the ultrasound department closed at 12pm so I was sent home and had to wait 2 days for the scan which was worrying for me. I feel that I should have had a scan the same day.” [Type 3, UTC]
“I waited all night with no food or drink and no communication at all. I eventually asked if I had been forgotten about and I got the distinct impression that I had been and having spent all night there was seen for 10 minutes and sent home. All in all – very unprofessional and does not inspire confidence.” [Type 1, A&E]
Being listened to
What does the quantitative data tell us?
Type 1 (A&E): 69% felt doctors and nurses ‘definitely’ listened to them (Q19).
Type 3 (UTC): 80% felt doctors and nurses ‘definitely’ listened to them (T16).
Type 1 (A&E): 58% reported being ‘definitely’ involved as much as they wanted in decisions about their care and treatment (Q27).
Type 3 (UTC): 71% reported being ‘definitely’ involved as much as they wanted in decisions about their care and treatment (T24).
Some patients shared that they had not felt listened to by staff, which strongly relates to other sub-themes of ‘Trust and confidence,’ ‘Unresolved symptoms’ and ‘Staff attitudes.’ Examples shared here demonstrate that patients not being listened to can be experienced as having an impact on their treatment.
“I was left in a side room for hours on end with no monitoring, I was constantly asking nurses if the volume of blood I was losing was normal and was dismissed on every occasion. They did not blood match me therefor when needing a transfusion I was again delayed. Due to this negligence I am now suffering anemia and PTSD and health anxiety which I am being treated by the wellbeing service for.” [Type 1, A&E]
“I informed doctors about a new lump I had found on my stomach next to my belly button and they completely disregarded my worry about this and didn’t look at it properly at all. It seemed like they just wanted to get rid of me from the centre. My questions were not answered and I was not given any of the tests that my GP said I would be given.” [Type 3, UTC]
“I didn’t feel like I was listened to when explaining my symptoms. I was told I had something which I didn’t and now my issues have got worse. I’m now under the care of my Doctor.” [Type 1, A&E]
“The nurses were extremely unhelpful. All 4 just sat there talking. Didn’t offer any drinks. I was in a lot of pain and all they told me to do was wait. The doctor told me he could instantly see that my stitches were infected. Surely the nurses could have knew what.” [Type 1, A&E]
Coordination of care
Breakdowns in communication and a lack of coordination within settings as the cause of delays, was a focus for some patients. Feedback indicated that patients felt they had to take responsibility for coordinating their treatment or ensuring that information was shared between different staff/teams.
“The specialist asked for an x-ray. However after a long time (1 hour) I discovered that I wasn’t even on the list for an x-ray, so there were people turning up and being given x-rays whilst I was sitting and waiting. I could have been there all afternoon if I hadn’t asked someone to look into it.” [Type 3, UTC]
“When a doctor did arrive from ENT, they explained that the staff changeover to the night team had resulted in the message from triage ‘not being handed over’ and so I had essentially been waiting all night with post surgery bleeding due to a miscommunication.” [Type 1, A&E]
“Some tests had to be repeated as there seemed to be lack of coordination between the out of hours GP, A&E and Minor injuries.” [Type 1, A&E]
“Staff failed to record details passed on to them by myself so when saw consultant on the Ward they had no idea of symptoms I experienced before going to A&E.” [Type 1, A&E]
“I think the doctor who met with me at the end to discuss my condition, treatment etc was incredibly kind and helpful. However the rest of my time in A&E was very confusing and poor. I was given pain medication and asked multiple times what it was but was not told. I was also not sure what the next steps were after being triaged and was told I needed tests but after waiting and asking multiple people what happened next I was told i didn’t need tests (I stopped one staff member in uniform and was told to ask a nurse but I didn’t know who the nurses were based on uniform so then had to ask multiple people.” [Type 1, A&E]
Pain management
What does the quantitative data tell us?
Type 1 (A&E): 42% said staff ‘definitely’ helped control their pain; 27% did not receive help (Q30).
Type 3 (UTC): 47% said staff ‘definitely’ helped control their pain; 26% did not receive help (T27).
Where comments mentioned pain management this was overwhelmingly negative, with experiences closely tied in with the experience of ‘Waiting’. While there were comments from UTC patients about pain, this sub-theme was more often seen in feedback from A&E patients. This included examples where no pain relief was given or when patients felt it had taken too long to receive pain relief, although it was not always clear whether this was before or after their first assessment.
“No pain relief offered at all!” [Type 1, A&E]
“I had to wait more than 6 hours to be seen, which is fine if other people are in more serious conditions than me need to be seen first. But in those 6 hours I was in pain, a pain that could have been stopped earlier.” [Type 1, A&E]
“Kept being sent home without any further investigations, pain kept getting worse and the hospital staff kept saying I had to wait for referrals which is what I need to do however my pain wasn’t managed and that’s where I was struggling.” [Type 1, A&E]
“Whilst at the A&E, after my first dose of pain medications, the subsequent doses were not given on time, this made my pain worse. It was like moving forward 1 step and then moving backwards 2 steps.” [Type 1, A&E]
“I was told that I would be given anti nausea medication and pain relief through a tube they stuck in my arm but they never did.” [Type 1, A&E]
“I went to A&E because I was in a huge amount of pain in my back and was pregnant. I was crying from pain and nobody would give me anything to help with the pain at any point.” [Type 1, A&E]
“I would have liked some pain relief in the more than 6 hour wait. Considering I came in with a lot of pain. I felt like it shouldn’t have taken 6 hours to be prescribed antibiotics for a UTI.” [Type 3, UTC]
“When I got to UTC I was there 7 hours before I got moved to (location name) with no pain killers.” [Type 3, UTC]
Mental health
What does the quantitative data tell us?
Type 1 (A&E): 11% indicated having a mental health condition (Q48).
Type 3 (UTC): 9% indicated having a mental health condition (T45).
Type 1 (A&E): 45% said doctors or nurses completely discussed any anxieties or fears about their condition or treatment (Q20).
Type 3 (UTC): 57% said doctors or nurses completely discussed any anxieties or fears about their condition or treatment (T17).
Some A&E patients shared their experience of care in relation to their mental health needs, linking to the pivotal role of staff outlined earlier in the ‘Personal attributes’ and ‘Staff attitudes’ sub-themes. A common thread when mental health was explicitly mentioned being the impact of negative experiences leaving them in the same, if not a worse place than when they first attended.
“I was in A&E for a total for 5 days, in a dark room with no windows, being watched by security. This did not help my mental health situation and made me feel trapped and like a prisoner. I did not eat in 5 days and no one checked on this. I requested lots of walks as it’s the only way I could get out for fresh air, I was always escorted by staff.” [Type 1, A&E]
“Psychiatry liaison are not very helpful telling me the same things every time I go in which is leaving me in the same crisis that I was in prior to going to a and e to speak to them.” [Type 1, A&E]
“Liason Psych Staff questioned my attendance. I felt like an inconvenience and an “eye-roll” patient. There was no room in the mental health area so I was in the main waiting area. There was a lack of privacy, communication, care & I didn’t feel safe.” [Type 1, A&E]
Feedback also included positive examples where the support from staff was noted as being exceptional, with observations on the compassion shown when experiencing a crisis having a deep impact.
“I went to the A&E department because I was feeling suicidal. I suffer profusely with passive suicidal ideation but on this day it felt cripplingly active. The receptionist was an amazing individual who did her best to accommodate to me while I tried to articulate my situation through my silent sobs and need to articulate myself quietly for privacy reasons. She was incredibly kind and compassionate.” [Type 1, A&E]
“The A&E staff saved my life and were exceptionally patient whilst I was confused an non-compliant. They identified I was very unwell and helped me regardless on my confusion and non compliant nature.” [Type 1, A&E]
“I suffer really bad with anxiety and the night I visited the hospital I was in such a panic, I broke 3 of my toes really bad results in surgery. On arrival at hospital, the staff and nurses were brilliant, they did there best to try and calm me down as well as to treat me.” [Type 3, UTC]
“I am autisitic so find it difficult to understand what people are saying to me however i felt that the dr who spoke to me seemed to understood this without me having to tell them, they rephrased the information in way i could understand, this i apprexiate as i was emotional state ag the time.” [Type 3, UTC]
Theme: outcomes and next steps
Feedback from discharge through to aftercare demonstrated areas for improvement were needed to ensure patients were clear and understood both what had happened and would happen next. Clarity on roles and responsibilities including expectations of the patient would support this, linking this theme closely to ‘Treatment’ outlined earlier in this report. Note there were also examples of self-discharge linked to ‘Waiting’ and access of private healthcare when symptoms were left unresolved.
Unresolved symptoms
What does the quantitative data tell us?
Type 1 (A&E): 30% said they had been to the same service previously for the same condition (Q8)
Type 3 (UTC): 20% said they had been to a UTC previously for the same condition (T5)
Both A&E and UTC patients shared experiences where a lack of resolution to their initial attendance led to further interactions with NHS services. This included patients who lacked confidence in their initial diagnosis or treatment, and either contacted other NHS services or reattended urgent and emergency care settings.
“I was told the swelling in my left knee was Osteoarthritis but I’ve already been diagnosed with this in the past and this pain felt different – especially compared to my other arthritic knee …I have since been back to my GP and been referred for an MRI scan and a Bone Density Test as I’m at risk of Osteoporosis due to an extra chromosome.” [Type 3, UTC]
“I was told that I must have a viral infection. The next day I ended up in hospital by visiting a&e at [location] as I was getting worse. I tested positive for the flu. I was at this point 8 months pregnant & this could have been very dangerous for me and baby. I felt robbed off by the urgent treatment centre.” [Type 3, UTC]
“Poorly managed burn-infected led to me going to A&E several times over 2 weeks. The nurse didn’t explain it was getting necrotic and only after 4th visit and a nice nurse whom sent me to specialist burns service. The wound needed managing over 2 months and a permanent scar. Was told, all could be avoided if given correct bandages at beginning.” [Type 3, UTC]
“The Dr prescribed cream and gave advice at the hospital, However, he did so by looking at photos off a phone? At no point during the appointment were the bandages removed and did not look at wound. When patient went to her district nurse appointment both asked if the Dr at the hospital was qualified, as both cream and advice was totally wrong?” [Type 3, UTC]
“X-ray results were explained as clear but when returning to GP with same issue there should have been a follow up as they weren’t clear and I had not been informed. It then developed into pneumonia.” [Type 1, A&E]
Other examples given indicated that opportunities were perceived as missed either in terms of diagnosis and/or treatment, sometimes linked to feeling staff did not listen to the concerns raised by the patient. Commonly, these patients reported reattendance at urgent or emergency care settings.
“I was told I’m too young to have Ulcerative colitis I was then seen at [location] hospital where they admitted me straight away as my inflammation was really bad to the point I was admitted for a week and had to do IV/MORPHINE/CODINE/STEROIDS.” [Type 1, A&E]
“I attended A&E in Feb with a suspected broken neck stated to reception staff I feel I’ve broke my neck, back or arm to be discharged with shoulder injury to then have worse pain to find out my neck was seriously broken.” [Type 1, A&E]
“Even after telling them that the object was covered in dirt and germs they still didn’t offer me antibiotics and I ended up with a huge infection a couple days later putting me out of work and college for 2 weeks.” [Type 1, A&E]
“I went to [location] the day before being seen at [location] due to my concerns of my ongoing symptoms I was experiencing from a concussion I had whilst playing rugby a few days prior. After waiting 6 hours to be seen at [location], I was told my feelings of faintness and dizzy spells were down to anxiety (after disclosing I had anxiety and depression during my initial triage) and not concussion. The next day, my dizzy spells continued and I was very anxious about my regular loss of balance and my previous diagnosis of anxiety being the cause. My friend took me to [location] as I was in the area, staying at his house. I was triaged immediately then seen by a caring doctor who confirmed I had severe concussion and laughed at [location] appalling diagnosis of anxiety being the cause.” [Type 3, UTC]
“[Location] A&E first sent me home saying I’d got ligament damage and that the X-rays were clear. 3 days later I was contacted and told to report to my nearest A&E as my X-rays had been reviewed and I had broken my foot.” [Type 1, A&E]
“I was told by the nurse in triage that I had bruised the muscle in my arm. I tried telling her I had done more than that and wanted an X-ray she said I didn’t need one, she gave me medication and sent me home. The next evening I went to [location] hospital where they X-rayed it and my shoulder was broken in 3 places and I needed surgery.” [Type 1, A&E]
“The nurse told me to go home and put a cold bag of peas on my knee when in reality I tore a tendon, split my meniscus and completely ripped off my ACL and urgently needed surgery.” [Type 3, UTC]
“I was told when I was seen by a doctor at the hospital that I had sacroiliitis and would need steroids I took the course of steroids but still remained in the same pain. When I saw rheumatology a few weeks later they advised I can only be diagnosed with sacroiliitis if it’s seen in a scan and the doctor was wrong to have given me steroids because if it wasn’t sacroiliitis then the steroids could cause me harm. I’m disappointed to have found this out as I thought I had answers as to why I was in pain.” [Type 3, UTC]
Although limited in volume or detail, there were comments which indicated some patients were discharged without a clear idea of their diagnosis, which they believed had a negative impact on care and support after their visit.
Private healthcare
Comments which discussed patients’ use of private healthcare often shared a common thread that they felt driven to do so by their needs going unmet either during or after interactions in NHS urgent or emergency care settings.
“I had to see a private physiotherapist to help with my recovery and this was not mentioned. The instructions I was given to recover were okay but not enough to fully recover. Hence why I had to seek help from a physio to massage the area and break down scar tissue. I don’t trust NHS physiotherapists hence why I went private.” [Type 3, UTC]
“I had to make another appointment after visiting the UTC to see my doctor to get signed off work as I could not walk. I cannot understand why the doctor in the UTC could not have done this. It was over 6 weeks before I was given a physiotherapist appointment. I was forced to go private or my problem would not have healed correctly.” [Type 3, UTC]
“My initial appointment was requested as urgent by my Doctor, because of a scan report sent by [service], back in Feb! Despite the urgency of the matter, I had to visit A&E several times, with the same old result take these pills, or go back to your GP. I paid at enormous expense to see a private specialist.” [Type 3, UTC]
“Over the last 6 months I’ve had ECGs and two echos which showed lower performing heart, also white and red blood cells depleted. 2 weeks ago I had a letter from [location] cardiology discharging me even though I’m still having pains and can’t do my normal life! I’ve ended up going private and immediately being put back on medication and cardiac MRI as I have myocarditis.” [Type 1, A&E]
“I ended up paying to see a private consultant who diagnosed my issue and told me the drugs I had been prescribed at A&E would not help. In A&E I felt rushed and as though the consultant did not think I should be there.” [Type 1, A&E]
NHS records
Feedback which touched on what happened after their visit included experiences where NHS records were not fully updated after attending urgent or emergency care. Some reported that this impacted on their ability to access appropriate follow up care.
“Not all notes were put on file from the visit meaning follow up consultation was made very hard due to a lack of notes from the visit to A&E.” [Type 1, A&E]
“I was late getting my next appointment because my records had not been updated, I don’t understand how different departments of the NHS do not have the same details.” [Type 3, UTC]
“Not all information was documented in my discharge letter i.e. I had lost 2 teeth in a fall, only my superficial abrasions were noted, I would not have attended A&E with superficial injuries.” [Type 1, A&E]
“The outcome was to not take the medication that caused the issue, but that information was not passed to cardiology or put on my record as I can tell.” [Type 3, UTC]
Follow-up
What does the quantitative data tell us?
Type 1 (A&E): 67% received information on how to care for their condition at home (Q36).
Type 3 (UTC): 82% received information on how to care for their condition at home (T33).
Type 1 (A&E): Of those given the information, 70% said that they understood the information given ‘very well’ (Q37).
Type 3 (UTC): Of those given the information, 77% said that they understood the information given ‘very well’ (T34).
Type 1 (A&E): 79% were told who to contact if they were worried about their condition or treatment (Q39).
Type 3 (UTC): 82% were told who to contact if they were worried about their condition or treatment (T36).
Some patients described a lack of clarity about where test results would be sent, along with not being clear on who to contact to discuss them. The impact of these experiences was that patients were left wondering what the results could be and feeling unsure how to move forwards in terms of follow-up care.
“Sending out CT-Scan results after being discharged should come with clear information who to contact for further clarification. My results were not clear and been bounced around and across departments still not knowing the final diagnosis after 4m+ without full results regarding my head injury I am forced to wait in a limbo without guarantee I’ll get better and back to living.” [Type 1, A&E]
“I was referred to [location] for an echocardiogram on [date] (I think) but have been unable to find out the results. Am I to assume they were OK? Inconclusive? Not serious? Serious? How do I find out the result of this test? My GP says she cannot help as she is based in [location]. (I am 85 – so please don’t say ‘go online’).” [Type 1, A&E]
“I was told at [location] UTC that I would be contacted if there were issues with my X ray. I was not contacted so assumed there were no problems. 12 weeks later I am still in pain so returned to my GP who referred me to the Fracture Clinic in [location]. I was told there that I should have been called two weeks after my fall to be re X rayed. This did not happen and was then termed as a ‘missed referral’. I am now waiting to see the wrist/hand consultant to discuss pain management. [Location] UTC have been negligent in their follow up. So this has not been a good experience for me.” [Type 3, UTC]
Concerns were also raised about uncertainty over next steps following a visit to urgent or emergency care, with feedback on the need to improve clarity on what communication would be received once discharged. This included patients who were informed of a need for follow up appointments but were unclear about where responsibility lay to arrange these.
“The biggest problem has been with the follow up appointment with cardiology which still has not been arranged 3 months after my visit to A&E. Conversely my ENT appointment took place within a week.” [Type 1, A&E]
“The after care was not that good, no communication, I had to call to arrange physio and no one had any idea what I was talking about, passed around and given different telephone numbers to call. Finally after a few days managed to get a date to start physio. Which was weeks after and I was told it would be within a week, with this delay it affected my road to recovery, which is to date still on-going.” [Type 3, UTC]
“The follow-up treatment for my condition since the visit is very slow and no contact from the department dealing with my condition is of concern as it’s the not knowing if anything is being done.” [Type 3, UTC]
“A&E told me my GP would be notified about my condition the next day. This was what happened. It took few weeks for a GP to contact me after persistent phone calls from me. I have been referred to a cardiologist but to date, three months later, I have heard nothing. A&E were great, the NHS a disappointment.” [Type 1, A&E]
Other observations
Below is a list of other topics commented upon in the data that were noted during the analysis process. There was a lack of volume of comments or depth and detail to inform themes and sub-themes but suggestions are noteworthy:
concerns for staff wellbeing were shared, with observations made on other patients being rude to staff
observed discriminatory comments about staff within survey responses, relating to protected characteristics
concern raised about aftercare following surgery being insufficient and creating a need to use emergency care
experience of a lack of care, for example with open wounds, while waiting for first assessment
4. Conclusions
This is the first national qualitative analysis delivered for the Urgent and Emergency Care Survey, and the breadth and depth of the insights demonstrates the value of inviting patients to share their experiences in their own words. This approach has enabled patients voices to shape the focus of the findings, highlighting what is important to them and what impacts their experience of urgent and emergency care.
Overall, the report shows that while there is appreciation and gratitude for NHS urgent and emergency care, there are significant challenges in access and delivery that can undermine experiences and confidence in care. Feedback focused largely on the early part of the patient’s journey, particularly the waiting experience, and on the outcomes and follow-up. This appears to reflect the transactional nature of the experience, along with the heightened anxiety many experience at these points.
Reflecting on what constitutes high-quality urgent or emergency care, the analysis points to a gold standard for experience: clear information on waiting times, and responsive care delivered by staff who listen and communicate effectively. Trust and confidence emerge as the foundation – critical is that patients feel heard, feel safe, and understand why they have received care (or not) along with being clear on what their next steps could be. The importance of staff listening appears across the themes, with indications that improvements across pathways into as well as within settings would significantly build trust in patients decision making on when to appropriately access urgent or emergency care. The findings also highlight the need for consistent information provision across NHS 111 and primary care on the role and capabilities of urgent and emergency care settings.
The diversity of patients, their expectations and needs identified in this analysis demonstrate a challenging context. The findings evidence the challenge of delivering personalised care for patients including those vulnerable, and a level of complexity more broadly, given the variability of expectations of patients, such as what constitutes a ‘long’ wait.
This report offers a comprehensive view of improvement opportunities though has limitations in determining which matter most and would make the biggest impact for patients. Triangulation with other datasets and targeted engagement activities are recommended to identify high-impact priorities. Ongoing listening and involvement of service users will be vital to ensure that national and local improvement efforts deliver the most meaningful gains.
5. Appendix: methodology
Survey methodology
The survey has undergone significant changes to methodology, sampling and content in 2024 which prevents comparisons to data from prior iterations. Through extensive consultations, stakeholders prioritised understanding patients’ experience of care during winter pressures and identifying factors that may account for unnecessary attendances. To this end, patients who received care in February 2024 from A&E (Type 1) or urgent treatment centres (Type 3, UTC) were invited to participate.
The Type 1 survey received responses from 35,670 people – a response rate of 29%. The Type 3 survey received responses from 10,325 people – a response rate of 26%. A total of 120 NHS acute trusts in England with an A&E department (Type 1) took part in the survey, of which 70 trusts also had an urgent treatment centre (Type 3).
Qualitative analysis
Thematic analysis was undertaken to achieve a deep understanding of the findings from the open questions asked in the survey. This sought to facilitate reflection and learning across services delivering urgent and emergency care in England.
To analyse qualitative data, the standard six steps of thematic analysis were used to identify patterns of meaning within the data and explore commonality and contrast – see Figure 1.
Figure 1: Thematic Analysis Approach
The image shows a horizontal blue arrow pointing to the right, representing a process flow. Inside the arrow are six dark blue rounded rectangles arranged sequentially from left to right, each containing white text. The steps are:
Familiarisation
Initial coding
Generating themes
Reviewing themes*
Defining themes
Final analysis and report writing
The arrow visually indicates progression from familiarisation through to final analysis and report writing, suggesting a structured process for thematic analysis.
The results of the thematic analysis have been reviewed and are shared in context of the relevant quantitative survey findings. This exploits the value of both the quantitative results, which tells us the proportion of respondents feeling a certain way, and the qualitative findings, which tells us why people feel that way. For example, where there is a high degree of agreement / positive experience evidenced in the survey data, the thematic findings offer an opportunity to understand why there was not 100% agreement / positive experience and therein, where the opportunities lie for reflection and learning.
Sub-group comparisons
Sub-group comparisons were not the focus of the analysis. Where variations were observed in the national sample, this has been included within commentary. It is recommended that further focused sampling would allow for in-depth exploration of how experiences of urgent and emergency care may vary for different groups. Observations included will unlikely be exhaustive due to the national sample and focus.
6. Appendix: Sampling approach
16,185 (A&E, Type 1) and 4,029 (UTC, Type 3) written responses were collected in total, meaning 45% and 39% respectively of the survey sample provided qualitative data in answering the open ended question.
Qualitative data cleaning
Before sampling, further data cleaning was carried out to identify and remove extremely short comments which were of no analytical value, for example those which simply stated ‘No’, ‘N/A’ or consisted of a single character.
For the Type 1 sample, 277 comments were removed in this way, leaving 15,908 comments for the sample to be drawn from. For the Type 3 sample, 94 comments were removed in this way, leaving 3,935 comments for the sample to be drawn from.
Sampling
It was decided to sample each of the surveys separately so that all respondents with viable response to an open question had the potential to be included in the final sample for analysis.
To ensure a robust approach to sampling, a purposive sampling approach was taken. This is an established best practice technique when analysing qualitative data, as it ensures that the data has enough diversity across the most relevant criteria to allow the impact of the criteria to be explored and compared. For example, if age is a criteria, including responses from all the different age groups in sufficient volume means that differences in experiences between age groups can be explored.
The criteria chosen to sample on were the age, ethnicity, sex, and deprivation level of respondents, as these were key demographic groups recorded in the data. A sample matrix was drawn up to establish how many comments from each of the demographic groups were to be included in the analysis to allow for sufficient coverage.
In addition to the three key demographic groups a minimum of 30 comments were included on all other characteristics including sexuality for instance. Please note that as there was a low volume of data from respondents identifying as Arab or other ethnic group, Intersex or different gender identity than sex assigned at birth, all of these cohorts were included in the sample. The breakdown of the volume of comments in the sample by these different criteria is provided below.
Once the original sample of 1,363 comments had been analysed it was seen that data saturation had been reached, i.e. no new themes were emerging from the data. Had this not been achieved, additional comments would have been added to the sample as necessary, in line with best practice in qualitative analysis.
The tables below show the number of comments in the analysed sample per characteristic for Type 1 (A&E) and Type 3 (UTC) services. The sampling approach ensured sufficient coverage across key demographic groups to allow for exploration of how experiences may vary.
Table 1: Number of comments in analysed sample per characteristic for Type 1 (A&E)
Characteristic
Sub-group
Number of comments analysed
% of comments analysed
% of comments overall
Age
16-35
95
13.9%
10.4%
36-50
103
15.1%
13.6%
51-65
183
26.8%
26.1%
66-80
204
29.9%
33.7%
>81
97
14.2%
16.2%
Ethnic background
White
522
76.5%
86.5%
Mixed
31
4.5%
1.6%
Asian
44
6.5%
4.9%
Black
36
5.3%
3.0%
Other
30
4.4%
0.7%
Not given
19
2.8%
3.3%
Deprivation level (IMD Quintile)
1 (most deprived)
107
15.7%
15.6%
2
128
18.8%
18.8%
3
152
22.3%
21.3%
4
155
22.7%
21.6%
5 (least deprived)
137
20.1%
22.2%
Blanks
3
0.4%
0.5%
Sex
Female
368
54.0%
57.8%
Male
298
43.7%
41.5%
Intersex
9
1.3%
0.1%
Prefer not to say
7
1.0%
0.6%
Gender different to sex assigned at birth
Yes
33
4.8%
0.5%
Sexual orientation
Heterosexual or Straight
556
81.5%
89.3%
Other
8
1.2%
0.6%
Gay or Lesbian
30
4.4%
1.6%
Bisexual
30
4.4%
1.2%
Prefer not to say
37
5.4%
4.5%
Not given
21
3.1%
2.8%
Table 2: Number of comments in analysed sample per characteristic for Type 3 (UTC)