
Introduction
This guidance supports systems to implement single point of access (SPoA) in their local area, as set out in the Priorities and operational planning guidance 2024/25 and the Urgent and emergency care recovery plan year 2: building on learning from 2023/24 letter.
Many systems have already established a SPoA function. However, but there are often differences in scope, geographical footprint, maturity and name (for example, SPoA, unscheduled care co-ordination hub and integrated care co-ordination). SPoA models also vary in the range of clinicians who can access them, how they are staffed, the services that the SPoA can refer to and governance arrangements.
While there is no single ‘right’ way to establish a SPoA model, this guidance draws on our engagement with systems, including clinical input, and the emerging findings from an independent national evaluation of existing SPoA models. It sets out the foundation components that all systems are required to have in place for winter 2024/25, and the case studies illustrate the steps that systems have taken in implementation.
Systems are encouraged to think about how they can best establish the components to meet identified local needs, and what further developments are a priority to increase their capacity and capability to support patients to access care.
Single point of access overview
A SPoA simplifies access to services by offering clinicians advice and guidance to support onward referral, ensuring patients get the right care for their needs quickly and safely, to improve patient outcomes regardless of where they present. As a partnership between community, ambulance, primary care, acute services and social care that brings together a multidisciplinary team (MDT), the SPoA can prevent avoidable ambulance dispatches and conveyances, emergency department (ED) attendances and hospital admissions.
Systems may choose to build on existing SPoA models or expand integrated urgent care clinical assessment service (CAS) models, but duplication of these must be avoided.
SPoA implementation is part of the approach to improving patient flow by providing more care to patients outside of hospital settings. SPOAs can also help to ensure patients receive hospital-level care at home by increasing referrals to urgent community response (UCR) and virtual ward (VW), also known as hospital at home.
Timely access to expertise from across the health and social care system means that patients can be managed in the community or booked directly into the right acute care setting – for example, direct to same day emergency care (SDEC) – supporting a ‘right care, right place, right time’ ethos for patient care and better outcomes for patients.
All systems without a SPoA should establish a service that can, as an absolute minimum, meet the SPoA foundation components for winter 2024/25 with full case management (management of the patients ongoing care requirements) to be implemented by March 2025 at the latest. This includes:
- clear pathways in place for provision of remote clinical assessment and advice through a SPoA prior to a decision to convey or attend ED
- ambulance services enabled to identify patients prior to dispatch for alternative pathways, as well as adopting ‘call before convey’
- direct referral pathways from SPoAs into community services such as UCR and VWs
- priority access to clinical advice for paramedics/ambulance staff and extending this in time to other health and care professionals, care homes, primary care (in-hours and out-of-hours GP services), community and other services
The SPoA approach is summarised in the diagram below.
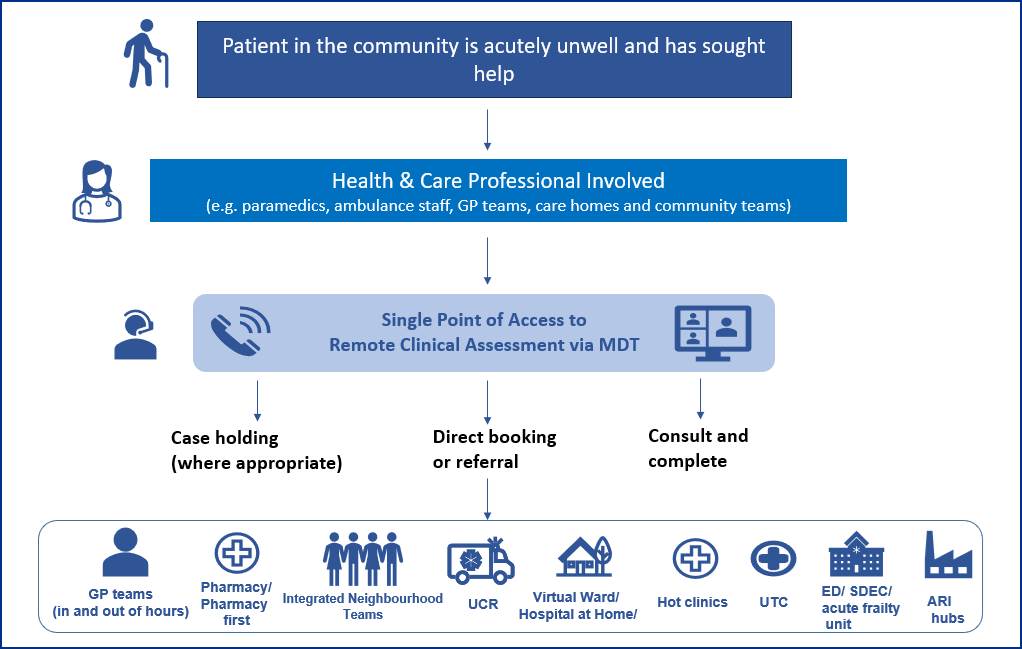
The healthcare professional can contact a SPoA for a remote clinical assessment by a multidisciplinary team. The patient can then be referred to the right service for their needs, for example urgent community response (UCR), a virtual ward (VW) or an urgent treatment centre (UTC), SDEC or general practice. The SPoA can consult and complete or where appropriate case hold. This means that where possible the patient remains in the community or is discharged from secondary care on the same day.
Foundation components for SPoAs
Systems are required to implement the following foundation components for winter 2024/25, and work towards full case management by March 2025 (To meet identified local need there may be a case for flexibility in approach, and to support our shared learning we would welcome discussion between systems and regional teams).
Operating model
- system (integrated care board) level or place based as agreed locally
- 7 days a week, 365 days a year. Hours should align to locally agreed need and typically be at least 12 a day
- provides clinical assessment, with access to a senior clinical decision-maker (in person and /or virtually)
- referral into a range of receiving services, with activity and subsequent outcomes captured.
- system in place to monitor and act on referrals into receiving services that are rejected
Core multidisciplinary team
- senior clinical decision-maker, for example advanced clinical practitioners (ACPs)/nurse consultant or doctor
- clinical team with representation from community, acute, ambulance and social care services
- GP and/or frailty consultant/geriatrician and/or Emergency Department (ED) clinician involvement to enable referral to the most appropriate setting
Connected teams (in person/hybrid/virtual)
- co-located/connected teams to maximise relationship building, skills/knowledge sharing, joint working and referrals to partner services such as VW and UCR. Physical/virtual links should be developed where appropriate with services such as NHS 111/CAS
System collaboration
- system partnership working across urgent and emergency care (UEC), hospitals, ambulance, primary care, community care and social care services to ensure full involvement in the MDT and maximise referral opportunities
- clear leadership agreed to ensure robust governance, risk management and patient safety
System integration/technology
- ensures timely transfer of appropriate patients from ambulance stack into alternative receiving services by improving interoperability, for example implementing interoperability toolkit messaging as a minimum
This requires:
- visibility of patients waiting for an ambulance dispatch
- access to shared records
- ability to transfer a case between MDT members as required
- visibility of appropriate waiting lists and real-time capacity
- ability to book directly into and referral to key services
Technological limitations should not be a barrier to practical solutions, for example sharing of information among those working in the MDT.
Established referral pathways
- locally agreed referral pathways into community and hospital receiving services and trusted assessor models
- priority receiving services should include, as a minimum, UCR, VWs, SDEC and UTCs
Senior clinical decision-makers
- capability to manage clinical risk appropriately and ‘hold’ clinical risk while arranging appropriate diagnostics and/or follow-up and care for patients, in collaboration with other services including VW and UCR
- the SPoA should ensure that ambulance crews can handover the patient case to the SPoA to manage and then leave the ‘scene’
- the ability to take clinical responsibility for sub-acute patients in real-time marks the start of care co-ordination
Case study – foundation, evolving to improvement – Worcester Integrated Care Co-ordination Hub (place based)
Operating model
- times: open 8am to 8pm, 7 days a week
- location: co-located at the community trust with direct links to the acute site and sharing a space with community teams, reablement, social workers and housing teams
- the hub is separate from the CAS and operates specifically for clinician-to-clinician assessment/conversations. Patients do not access the service directly
- calls taken by admin staff are categorised into acute and community
- workforce: staffing for the community arm includes a community ACP, UCR GP, Band 6 nurses and a paramedic. The acute arm staffing includes an ACP service lead, acute ACPs (with trusted assessor status) and SDEC triage nurses (medical and surgical)
- governance: KPIs and governance have been developed and agreed for the SPoA
Current process
- the hub takes calls from primary care and from West Midlands Ambulance Service (WMAS) paramedics on scene, with a focus on those for patients over 75
- community (UCR calls) are managed by the community arm, and acute calls by the acute arm
- the teams can refer cases to primary or community services and arrange diagnostics if required. The acute arm can access direct specialist advice from and or directly book into acute services, for example VW, hot clinic, outpatient appointments (OPAs)
- the WMAS emergency operations centre (EOC) clinical validation team pushes appropriate 999 cases to the hub via a digital ‘portal’. (Appropriate cases are those that are suitable for referral to an acute community service, preventing unnecessary ambulance dispatch.)
Future plans
- continue to promote the benefits the SPoA can realise for paramedics on scene
- embed test of change approach for pushing a suitable wider cohort of ambulance cases than currently from WMAS to the hub
- adopt incumbent software solution to enable greater integration
- continue to review service pathways to provide additional direct referral routes
- continue work with NHS England relating to data collection and benefits realisation for SPoA
Impact
- SDEC activity has increased by 26.7% – possibly due to the impact of the SPoA.
- 4-hour performance: 2.98% reduction.
- 30-minute handover delays halved in the last 60 months.
- WMAS is responding to and releasing Category 3 and 4 in Worcestershire area.
“Big shout out today to SPoA/UCR. Very helpful with getting into AEC [ambulatory urgent care].” – Ambulance Clinician.
“All positive, very happy with the joint working. Has helped with the patient journey as we can pass cases between us for the best outcome” – UCR Clinician.
Improvement activities for SPoAs
Once the foundation components are in place, systems should look to expand and develop their SPoAs. As a minimum this should include:
Supporting care homes and enhanced health in care homes by:
- providing advice and management for patients with urgent and complex needs to avoid ambulance call outs and/or transfer to hospital
Supporting general practice and integrated neighbourhood teams by:
- managing escalation of care and avoiding ambulance call outs
- planning for the inclusion of social care as an integral partner
Reviewing opportunities to further reduce duplication between clinical teams; for example, alignment with care transfer hubs or CAS supporting NHS 111/999.
Learning and improvement cycles by:
- regularly reviewing emerging/changing demand against available capacity
- using care co-ordination output to develop a more detailed understanding of whole system demand and capacity
- reviewing demand and capacity data for acceptance/referral rates of services and action improvements as required
- using system knowledge and learning cycle outputs to inform future commissioning and transformation
Technical development areas – secure visibility/full record sharing of appropriate patient details to enable proactive management (case management) and referral. Achieved by:
-
- developing a ‘portal’ or digital platform that all partners can access, enabling review of eligible Category 3, 4 and 5 ambulance cases before transfer to a suitable receiving service
- having real-time visibility of capacity and demand in sending and receiving services
Key design questions for systems
The following questions should be considered by systems when developing a SPoA. To support local design and implementation a system maturity matrix and a self-assurance template is available on NHS Futures.
Step 1
Patient presents as unwell with an urgent care need and contacts NHS 111, 999, ED or GP.
- what geography will the SPoA cover? Typically, it will be place-based or integrated care system
- what cohort of patients will the SPoA accept, for example Category 3, 4 and 5 999 calls and NHS 111 dispositions, frailty, complex needs, end of life care?
- is there an established baseline activity profile for the patient cohort to support benefits realisation, for example, time in ED department, discharge status and length of stay?
Step 2
NHS 111/999 transfers the case to the SPoA (before ambulance dispatch) or the healthcare professional calls the SPoA (before conveyance).
- is the SPoA operating 7 days a week, 365 days a year and typically for at least 12 hours a day? What will happen outside these hours?
- do the opening hours align with both demand and availability of services?
- are the referral pathways into key services agreed?
Step 3
SPoA facilitates a clinical conversation between the healthcare professional(s) and the MDT to decide onward management of the patient.
- who are the senior clinical decision-makers?
- how is the ambulance service represented and can they facilitate a shared view of the stack to enable review of eligible patients?
- how is the VW/UCR team represented?
- how is medical support from a GPs, consultant geriatricians or ED consultants included?
- how is social care inputting?
Step 4
Same day assessment or follow-up in the right place, (for example, through UCR response, VW admission or SDEC booking) at the right time by the right person, first time.
- are services able to meet demand? For example, does VW capacity align and is there capacity to manage patients in the community (refer to the Virtual Ward Operational Framework)
- is the Directory of Services (DoS) up to date and does it profile receiving services correctly? What is the ongoing plan for keeping the DoS up to date?
- can the SPoA book directly into receiving services?
Key governance design questions:
- is there clear leadership and collaboration across partner services?
- is clinical governance in place including the ability to case manage patients and ‘hold the clinical risk’?
- is there clinical quality safety and reporting?
- is a system in place to monitor and act on referrals that receiving services reject and gather learning that exposes demand and capacity issues?
- does the SPoA have a GP notification (PEM) and feedback loop in place?
The impact of SPoA
As a key enabler service, emerging findings indicate there are numerous benefits of SPoA, many of which will be realised at an ambulance trust / ICB level.
- ambulance dispatch: reduction in the number of dispatches for Category 3, 4 and 5 cases for target patient cohorts. (Note: target patient cohorts will be locally agreed but may include those patients who are at end of life, require social care intervention, require frailty services or are non-ED dispositions with non-life threatening conditions.)
- ambulance conveyance: reduction in the number of conveyances to ED for target patient cohorts
- urgent community response (UCR): increase in the number of referrals and in acceptance rates
- virtual wards: increase in the number of referrals and in acceptance rates
- mental health and social care: increase in the number of referrals and in acceptance rates
- acute services (for example, SDEC, hot clinics): increase in number of direct referrals (avoiding ED) – referral outcome
- ED performance: reduction in the number of ED attendances for target patient cohorts
For patients this will mean:
- improved experience and satisfaction
- increased access to same day urgent assessments where appropriate
- faster access to the right care, resulting in improved outcomes
- optimised care at home, or in their normal place of residence
For systems this will mean:
- greater efficiency
- better use of NHS resources, including limited clinical/non-clinical resource
- reduced ED attendances and ambulance delays and improved ED/ambulance performance against key targets
- alleviation of pressure in primary care allowing focus on complex patients and continuity of care
- reduced healthcare inequalities
Case study – embedding improvement activities – Bath and North-East Somerset, Swindon and Wiltshire (BSW) Care Co-ordination Hub (ICB wide)
Operating model
- times: open 8am to 11pm, 7 days a week
- location: co-located with CAS. Hub and spoke model with 3 places (placed-based hubs within each locality)
- commissioned by the ICB, an independent provider and South Western Ambulance Service NHS Foundation Trusts (SWAST), the key partner in the model
- workforce: staffed by 2 clinicians including a specialist paramedic, and 2 administrators
- a coaching style between care co-ordination hub staff and community staff/paramedics supports increased autonomy and less risk aversity
- governance: memorandum of understanding (MoU) between BSW ICB and SWAST clarifies responsibilities and governance arrangements
Current process
The care co-ordination hub manages patients in 3 ways:
- 999 call stack accessed through a senior SWAST clinician in the centre to identify which patients could be managed differently
- clinicians in the community can contact the care co-ordination hub via a single ‘0300’ telephone number
- cases passed to the care co-ordination hub from the EOC directly via ITK
Future plans
- a business case has been accepted to increase workforce at times of peak demand, for example to 3 clinicians plus a specialist paramedic at weekends
- BSW would like to have more specialist staff in the care co-ordination hub, for example paediatric expertise.
- consideration of expanding the offer to general practice.
- collection of data for re-presentation rates (24, 48 and 72 hours)
Impact
- the BSW care co-ordination hub has taken 22,000 calls since it opened and avoided 18,000 conveyances with 20% referred to out-of-hospital pathways and 50% closed by the hub.
- a comparative study of 60+/frail cohorts showed the conveyance rate with the hub in place was 16% compared to 55% without the hub
“I have used the BSW Nav hub 3 times in the last 2 shifts. Each patient could have been conveyed, but after good clinical discussion with HCPs, they were discharged on scene. This service is invaluable if we are going to manage our patients effectively.” – Paramedic
Further resources to support SPoA implementation
The following tools and processes may help systems with SPoA implementation and to understand the range of opportunities that an SPoA service can enable.
- Maturity Matrix: outlines the principles and components that underpin the successful development of a system approach to co-ordinating patient care. It guides systems through the initial steps towards readiness and actions that enable networks to begin their improvement journey to deliver integrated care to their local population
- example self-assurance template: this can be used by ICBs/systems to assure implementation progress against the foundation components and improvement activities
- AtED/AtA – Getting it Right First Time (GIRFT): an easy-to-use scoring system to help systems and trusts measure, rate and compare the accessibility, availability and opening hours of patient-facing services that are offered as alternatives to attending the ED in their area, including walk-in centres, telephone advice services, urgent clinics and community services
- example of missed opportunity audit/deep dive audit: an MDT review of 24-hours’ worth of ambulance conveyances and ED attendances to consider (based on the pattern of presentation) which patient cohorts would benefit from alternative settings for treatment (UCR, frailty, SDEC, primary care, etc)
- example data collection template: a standardised dataset collection template to support row level analysis and data capture that can demonstrate impact
- test of change cycle example – N&W T1:
- test of change 1 – Implementation of the up streamed clinical conversation
- test of change 2 – Using the care co-ordination hub as a referral pathway that can case hold and co-ordinate patient cases
- test of change 3 – To implement the concept of trusted assessor status within the care co-ordination hub
- test of change 4 – Enhance the referral process for pre-dispatched 999/111 cases to be electronically referred to the hub
- detailed case studies:
- Norfolk and Waveney – Genuine ICS-wide single point of contact to facilitate a supportive senior clinical conversation for patients who may be transported to the ED and/or for those requiring direct streaming access to a speciality
- Worcestershire Acute Hospitals – SPoA for a clinician-to-clinician conversation/same day urgent clinical assessment and ability to refer patients into appropriate acute or community-based services
- BSW – Multiagency team of senior leaders, clinicians (including GPs, hospital consultants, advanced clinical practitioners and mental health specialists), supported by a variety of other health and social care professionals, to provide advice to ambulance crews and to identify community-based alternatives to hospital
- Greater Manchester CAS – CAS-led emerging model with high levels of system digital interoperability
Publication reference: PRN01480