
Advancing ethnic equalities in NHS talking therapies services
We welcome the recent launch of the Patient and carer race equality framework – NHS England’s first ever anti-racism framework, which requires every mental health service provider to become an actively anti-racism organisation and take concrete action to reduce racial inequalities. We support its implementation in NHS talking therapies for anxiety and depression services. Thanks to the hard work of many dedicated individuals and teams, these services have made significant progress towards greater race equality, but there is further to go. The PCREF can help continue the push, requiring organisations to act on:
- leadership and governance: with concrete plans to reduce health inequalities
- cultural competences: building competences that improve the experience of racialised communities
- feedback mechanisms: with clear processes to act on patients’ and carers’ feedback about the service.
Cause for hope – the progress made so far
From the beginnings of the NHS Talking Therapies Programme (previously known as Improving Access to Psychological Therapies) 15 years ago, advancing equalities has been a key priority for service development and delivery, and data have been used to drive improvements. One of the first pilots for the programme (Newham Talking Therapies) had a particular focus on developing ways to enhance referrals from ethnic minority communities. It found that self-referral led to more equitable access, a finding that prompted the decision to open all NHS talking therapies services to self-referral, which is still accessible and promoted today via NHS.uk/talk.
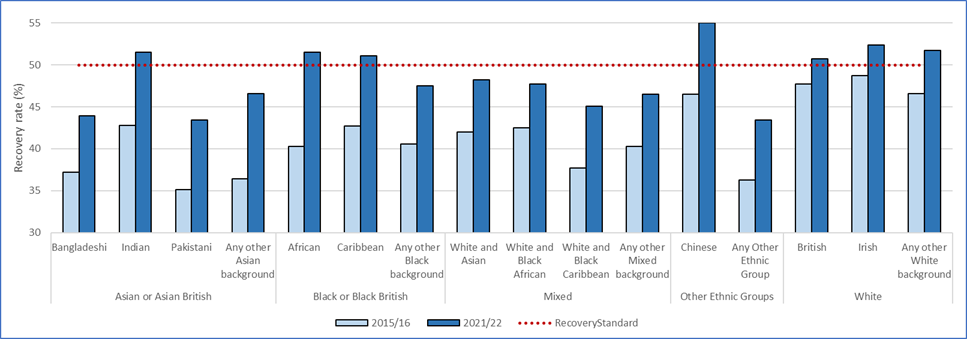
Over the years, there has been progress on ethnic minority outcomes, which are monitored and reported nationally. Comparing outcomes in 2015/16 and 2021/22 across ethnicities (figure 1), we see that recovery rates (percentage of people who complete treatment who no longer meet the criteria for anxiety or depression) have improved across all ethnicities. The overall recovery rate in 2015/16 was 46.3%, whilst the recovery rate in 2021/22 (the latest annual data) was 50.2%. They have improved the most for ethnic minorities, and by 2021/22, the recovery target was met for seven ethnic groups: Indian, Black African, Black Caribbean, Chinese, White British, White Irish and Other White Background. In 2020/21, there was the introduction of a national support metric to close the gap between White British and all other ethnicities. In 2021/22, the gap was 1.8% overall, reduced from 4% in 2020/21 (and from 6% in 2015/16).
Figure 1: Outcomes data by ethnicity 2015/16 versus 2021/22
How has this progress been made?
The backbone of the work has been the NHS talking therapies Black, Asian and Minority Ethnic service user positive practice guide, which was published in 2019. The guide was authored by members of the British Association for Behavioural and Cognitive Psychotherapies (BABCP) Board and Equality and Culture Special Interest Group (Andrew Beck, Saiqa Naz, Michelle Brooks-Ucheaga and Maja Jankowska) and co-developed with NHS talking therapies clinicians and racially and ethnically diverse service users. It guides good practice in increasing access, reducing rates of non-attendance, developing an appropriately skilled workforce, and ensuring talking therapies is delivered with cultural humility. It also provides an audit tool that allows services to identify areas for improvement. NHS England, working alongside some of the authors, have since launched an e-learning module based on the guide to increase uptake of the positive practice.
We believe part of the reason for the notable improvements in outcomes for certain groups between 2018/19 and 2021/22 in NHS talking therapies services is due to services acting on the good practice in the guidance. We are hugely grateful to those who have worked tirelessly across the years to personally promote the guide with services.
In addition, NHS England has been supporting proactive anti-racism work in services including:
- sharing learning from services that have developed comprehensive strategies to improve access and outcomes for ethnic minorities, via national webinars
- launching a protected characteristics outcomes dashboard to allow local services to interrogate their data, address inequalities and share learning from the best
- incorporating additional equality, diversity and inclusion content into the core NHS talking therapies training curricula and sharing national training materials among the existing workforce.
More to be done – what next?
Of course, the data shows that there is much more to do to enable all ethnic communities to achieve equitable access and outcomes. Particular focus will be needed where outcomes are poorest, for example for Bangladeshi and Pakistani groups. It is vital to continue to close the gap, and address variations across geographies. Some of the remaining inequalities were highlighted in the NHS race and health observatory independent review of NHS talking therapies services, which recommends a range of actions to tackle these that we fully endorse. These include further action on community engagement, leaders’ attention to local inequalities data, comprehensive uptake of the Positive practice guide, and ensuring culturally-sensitive care.
We are encouraged by the progress that can be demonstrated when there are collective and concerted local, regional and national efforts to advance equalities. The launch of the Patient and carer race equality framework means we, collectively, have additional momentum behind this essential drive towards eliminating health inequalities from our services. We encourage NHS talking therapies services, commissioners and leads, to review and implement the Patient and carer race equality framework as it provides a structured, participatory, and transparent context for mental health service transformation and innovation. It will be mandatory from April 2024. It also creates an opportunity for the recommendations in the NHS Race and Health Observatory review to be implemented.
Dr Adrian Whittington
Adrian is the National Clinical Lead for the Psychological Professions at NHS England. In this role, Adrian provides professional leadership and advice across the national NHS teams aimed at maximising the impact of the psychological professions for the public and delivering the ambitions of the NHS Long Term Plan.
He is a Consultant Clinical Psychologist. He is passionate about making the NHS more psychological, including increasing access to evidence-based psychological interventions and therapies.
Adrian also co-chairs the Psychological Professions Network England Board. Adrian is a clinical specialist in psychological therapy for post-traumatic stress Disorder.
He has written and co-edited books on anxiety, cognitive behavioural therapy, and clinical psychology.
Professor David M Clark
Professor David M Clark is Clinical and Informatics Advisor: NHS Talking Therapies for Anxiety and Depression, NHS England.
Professor David M Clark holds the Chair of Experimental Psychology at University of Oxford and is the National Clinical and Informatics Advisor for the NHS Talking Therapies Programme. Along with Lord Richard Layard and other colleagues, he is one of the original architects of the programme.
He is well-known for his research on the understanding and treatment of anxiety disorders, especially panic disorder, social anxiety disorder and post-traumatic stress disorder.
Recognition of his work includes Lifetime Achievement Awards from the British Psychological Society and the American Psychological Association.
Jullie Tran Graham
Jullie Tran Graham is a Senior Programme Manager in NHS England’s Mental Health Team. She is currently leading on the delivery of the NHS Talking Therapies Programme with the aim of achieving the ambitions set out in the NHS Long Term Plan.
She has a particular interest and focus on equalities and she has worked on a number of the programme’s advancing equalities projects.
Jullie has a background in health economics and applied sciences.