
The Frailty Fulcrum
The concept of frailty as a long-term condition brings with it the opportunity to adopt a much more proactive, person-centred, community-based approach to care.
Achieving this requires a new approach to care, particularly through supporting self-care. This new approach will be enabled through a wider awareness of frailty and a greater shared understanding of the condition.
The ‘frailty fulcrum’ is an animated model for frailty that has been developed with these opportunities in mind. This model aims to provide a ‘common language’ for frailty that can be shared between individuals, carers and professionals. It offers an interpretation of frailty that is meaningful, relevant and sustainable for people living with the condition, throughout their journeys of care.
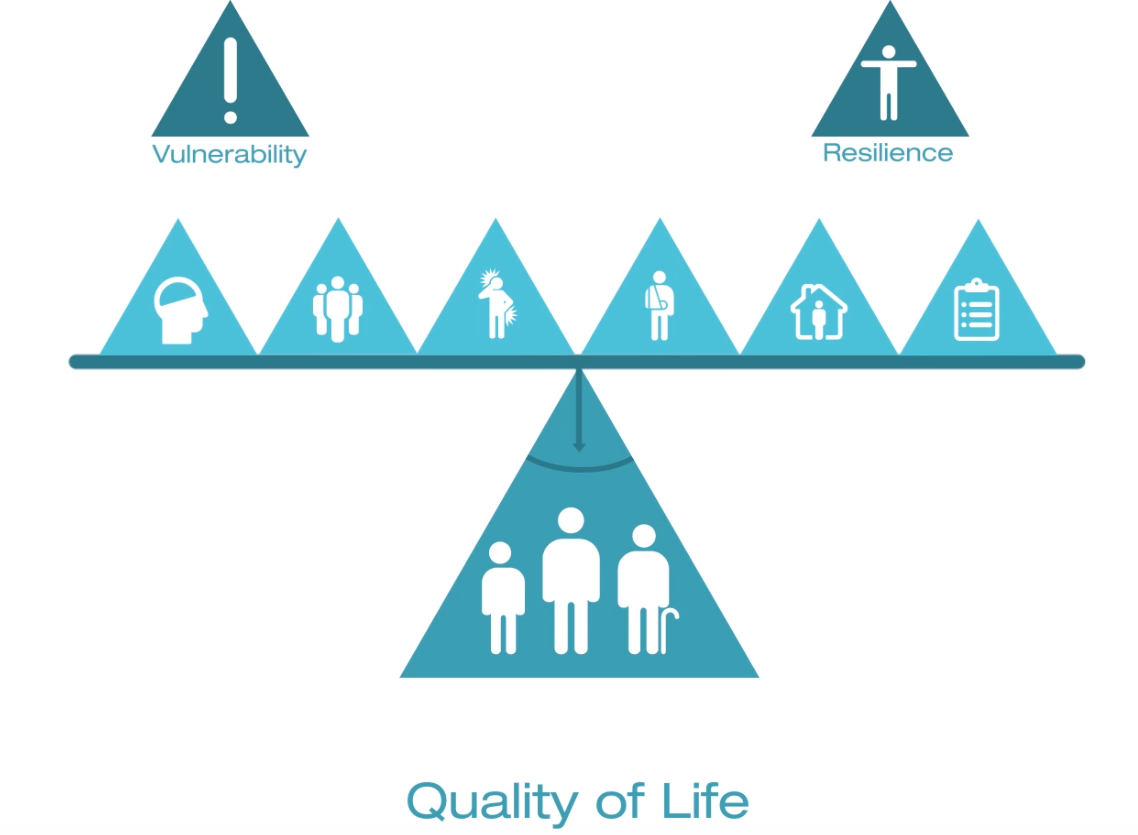
The frailty fulcrum highlights the multi-dimensional nature of frailty. It considers the many different aspects of our lives that contribute to our overall wellbeing through a series of domains. The domains identified in the model are:
- Social environment, including our families, our friends, our communities, any of the people or places that are important to us.
- Physical environment, which is our homes in particular but also the many places that we visit as we live our lives.
- Psychological status, which includes both specific conditions, such as anxiety, or more general feelings like a loss of confidence or a lack of motivation.
- Long-term conditions, such as diabetes, heart disease or respiratory conditions.
- Acute health problems, including for example, infections or injuries.
- Systems of care, which have a direct impact upon wellbeing, not just through the care that they provide, but also through the way in which they deliver that care.
Factors within each of these domains can either promote individual resilience or create individual vulnerability. The frailty fulcrum shows how resilience and vulnerability in these various domains come together to create the holistic condition of frailty. It also shows how the dynamic balance and interactions between the domains influence individual quality of life.
The frailty fulcrum explains how keeping a good balance between all the different things going on in our lives becomes more difficult over time and that as we get older the likelihood of relatively small things causing bigger problems increases. The model also highlights that these changes can occur more quickly for some people than for others and therefore explains both the association and difference between frailty and ageing.
The frailty fulcrum demonstrates that even though challenges in some areas of our lives might in themselves be difficult to overcome, a person’s quality of life can still be improved by promoting resilience in other areas, whatever the individual’s age or degree of frailty. It also highlights the important contribution that supporting individual decisions and choices, and supporting self-care, can make to improving quality of life for people living with frailty.
The frailty fulcrum, therefore, offers a shared language for frailty to enable a consistent approach to holistic assessment and action planning. It helps to identify and understand the multi-dimensional opportunities that exist to optimise quality of life for people living with frailty and is intended to empower these individuals to exercise choice and control over the care they receive and the ways in which they live their lives.
Watch the Frailty Fulcrum animation.
Dr Dawn Moody
Associate National Clinical Director for Older People and Integrated Person-Centred Care for NHS England.
Dr Dawn Moody is a GP in Derbyshire who has a special interest in frailty and person-centred systems of care. She has worked with commissioners, providers and in research in this area and holds an MSc in Geriatric Medicine. Dawn’s current portfolio includes her directorship of Fusion48 being the Clinical Director for Health Education England (East Midlands) Nottinghamshire Frailty Toolkit and Training Programme. She is also Frailty Lead for the West Midlands Primary Care Workforce and Improved Patient Access Plan, Prime Minister’s GP Access Fund Wave 2 Scheme.
Dawn’s previous roles have included Clinical Associate (Frailty and Complex Care) at North Staffordshire CCG and Medical Director North Staffordshire Community Healthcare. She has been a Partner in General Practice for 16 years and GPSI Geriatric Medicine and intermediate care.