
What is SNOMED CT?
SNOMED CT (Systemized Nomenclature of Medicine – Clinical Terms) is the most comprehensive and internationally validated system to record clinical information in the patient record. It is a structured clinical vocabulary for recording clinical information in patient records, also known as a ‘terminology’. SNOMED CT is suitable for use across all care settings.
Terminologies like SNOMED CT allow clinicians to represent clinical thoughts or phrases into the patient record in a structured manner. These clinical thoughts or phrases are called ‘clinical concepts’ in SNOMED CT.
Coding information into the patient record using SNOMED CT allows the information to be understood clearly by both humans and computer software. Healthcare systems using SNOMED CT can consistently understand, share, and exchange clinical information effectively.
SNOMED CT was created in 1999 by combining the SNOMED Reference Terminology (SNOMED RT, College of American Pathologists) and the NHS Clinical Terms Version 3 (CTV3) also known as ‘Read codes’.
SNOMED International is a not-for-profit organisation that owns, administers, and develops SNOMED CT. Its mission is: ‘The development of a global language for health – uniting health systems from around the world and enabling them to communicate with and understand one another’.
The organisation keeps SNOMED CT up to date, ensuring it remains fit for its purpose. NHS England then adapts the international edition of SNOMED CT to include UK-specific clinical content or extensions. NHS England is ultimately responsible for maintaining and releasing the UK edition of SNOMED CT.
SNOMED CT | a single coding system
Before its adoption, a single system for coding did not exist for use in all care settings in England. SNOMED CT is the modern-day terminology that can enable our healthcare system to achieve its potential.
In 2014, the then National Information Board (replaced by the Care Quality Commission, NHS England, and Health Research Authority) document Personalised health and care 2020: a framework for action recommended using SNOMED CT as the single terminology system across all care settings in England. The use of SNOMED CT is a new national information standard (ISN SCCI0034) and must be adhered to as part of the Health and Social Care Act 2012.
All NHS healthcare providers in England must use SNOMED CT for capturing clinical information. This includes primary care, secondary care, mental health, and community systems.
Primary care system suppliers have enabled SNOMED CT within their systems since 2018. Secondary care services are in the process of adopting the terminology across their systems.
Read code limitations
SNOMED CT improves upon Read codes previously used to code clinical information in primary care. Read codes had several unresolvable limitations, such as:
- lack of comprehensive coverage for all clinical specialities
- inflexibility for adding new clinical content into the correct place
- inability to meet the needs of the whole healthcare system, e.g. genomics and rare diseases
- incorrect and out of date content
- limitations in the number of parent-child relationships (discussed below)
- presence of duplicate terms
- inappropriate for use in secondary care
Advantages of SNOMED CT
Read codes were not suitable as a single coding system for the whole health system. SNOMED CT solves many of these limitations and has several advantages over Read codes, such as:
- enabling a common clinical language for use across different clinical and care settings
- comprehensive coverage for all clinical specialities and professions
- a broader range of clinical terms
- extensible and configurable to meet the specific needs both locally and nationally
- adapts to new discoveries or requirements
- improving the accuracy and consistency of clinical information in the patient record
- improving interoperability by allowing data to be exchanged easily between IT systems in different clinical and care settings
- reducing the ambiguity of clinical information coded in the patient record
- enriching the ability to run meaningful clinical decision support, sophisticated alerts and unlocking artificial intelligence
- reducing the risk of misinterpretation within the patient record when used correctly
- enhancing data analysis to support clinical audit, clinical research, and support population health management
These advantages are dependent on the proper implementation and use of SNOMED CT by individuals, practices, and organisations.
The use of SNOMED CT is free to the NHS and is a very powerful tool when used correctly. It can help unlock many aspects of the NHS Long Term Plan and integrated care systems.
At the heart of the healthcare system are the citizens that use it. Creating a genuinely interoperable healthcare system that speaks a common language is vital. Implementing SNOMED CT across England’s health and social care settings will help make this a reality. Benefits will be felt across the whole system.
Structure and content of SNOMED CT
SNOMED CT covers more than just diagnoses and includes a vocabulary across various clinical concepts. Content generally comprises three basic building blocks: concepts, descriptions, and relationships.
Concepts, descriptions and relationships
Concepts represent clinical meanings and phrases that we want to record when entering coded information into the record. Myocardial infarction is an example of a clinical concept (see Figure 1).
Descriptions represent the different ways users can describe a clinical concept. The concept of myocardial infarction, for example, can also be described as cardiac infarction or heart attack (see Figure 1)
There are two types of descriptions, ‘fully specified name’ (FSN) and ‘synonym’ (S). The FSN reflects the description that is the most unambiguous and applicable across multiple contexts. The FSN, whilst unambiguous, will not always be the most appropriate description for the user or context, which is why alternatives exist. Synonyms allow for alternative descriptions for a particular concept. Descriptions that are thought to be the most clinically appropriate way of expressing a concept in the patient record are also highlighted as a ‘preferred term’ (PT), see Figure 1.
Figure 1: Clinical concept with descriptions myocardial infarction in SNOMED CT
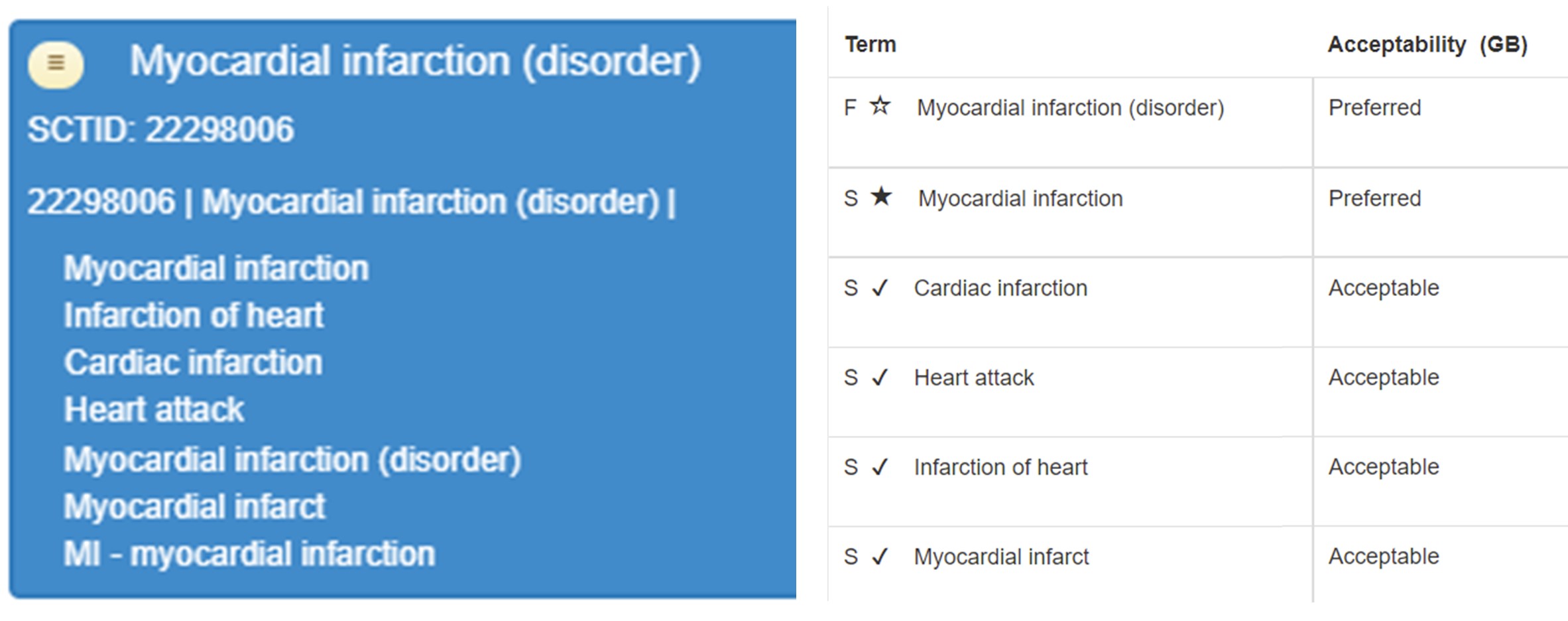
In this example, myocardial infarction is categorised as a disorder in SNOMED CT. The long number SCTID: 22298006 is the computer-readable code for the clinical concept of myocardial infarction. Myocardial infarction (disorder) is the FSN, and the descriptions below are all synonyms. Users should always try to use the FSN or preferred term when entering clinical information into the patient record.
Relationships define how different clinical concepts are related to one another. There are two types of relationships in SNOMED CT. These are both shown in Figure 2.
‘is-a relationships’ describe parent-child relationships. For example, the concept ‘bacterial pneumonia’ (disorder) is a child of two more generalised clinical concepts: infective pneumonia, and bacterial lower respiratory infection.
‘attribute relationships’ describe specific characteristics of a clinical concept. The concept of bacterial pneumonia has four attributes. For example, bacterial pneumonia is bacteria resulting in an infective process causing inflammation and consolidation in the lung structure (see Figure 2).
Figure 2: Clinical concept bacterial pneumonia with relationships
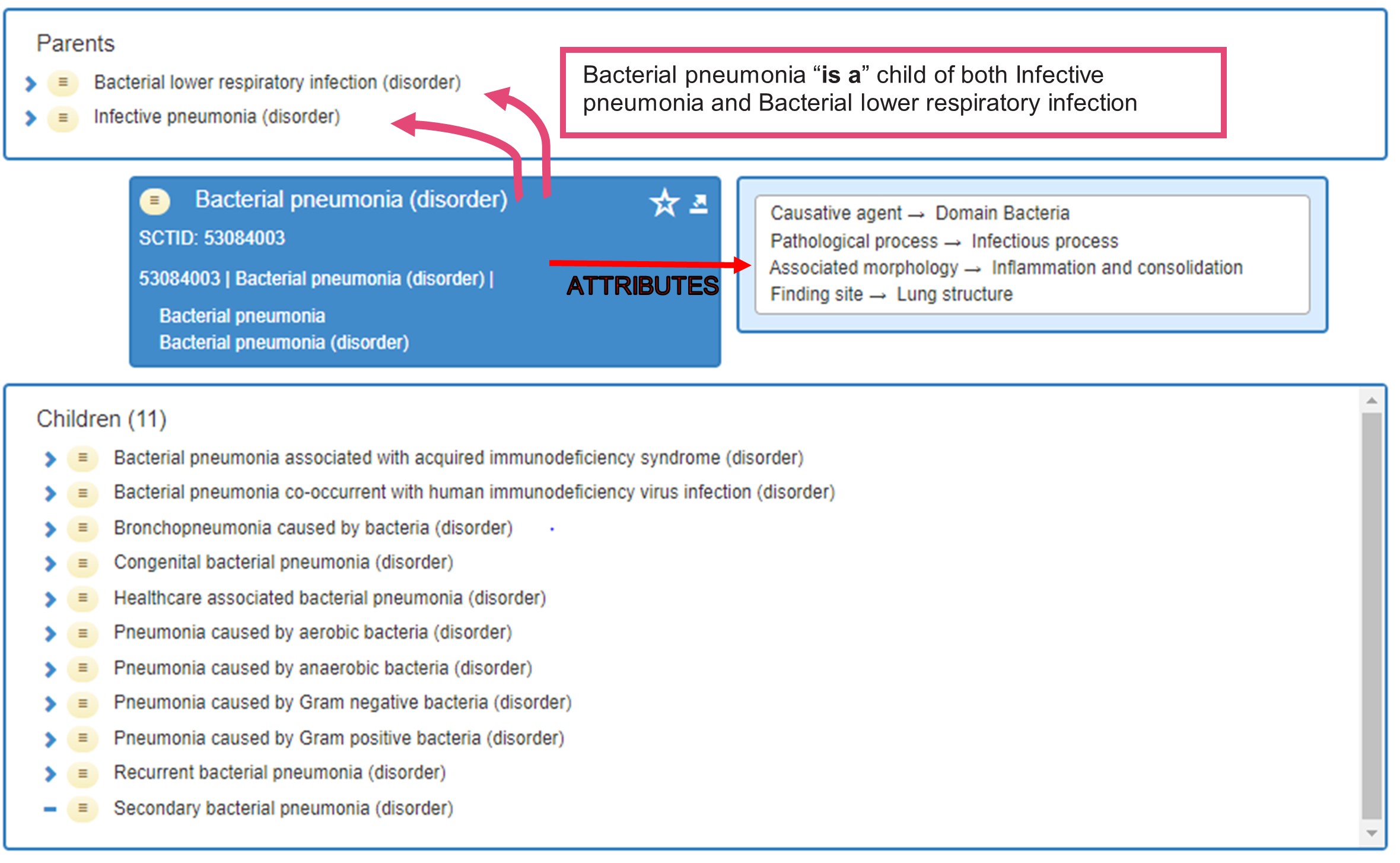
One significant advantage of SNOMED CT over Read codes is that each clinical concept can have more than one parent. In the above example, bacterial pneumonia has two parents. Additionally, there is no limitation on the number of children each clinical concept can have. In the Read code system, each clinical term can only have one parent, and there is a limit on the number of children each term can have.
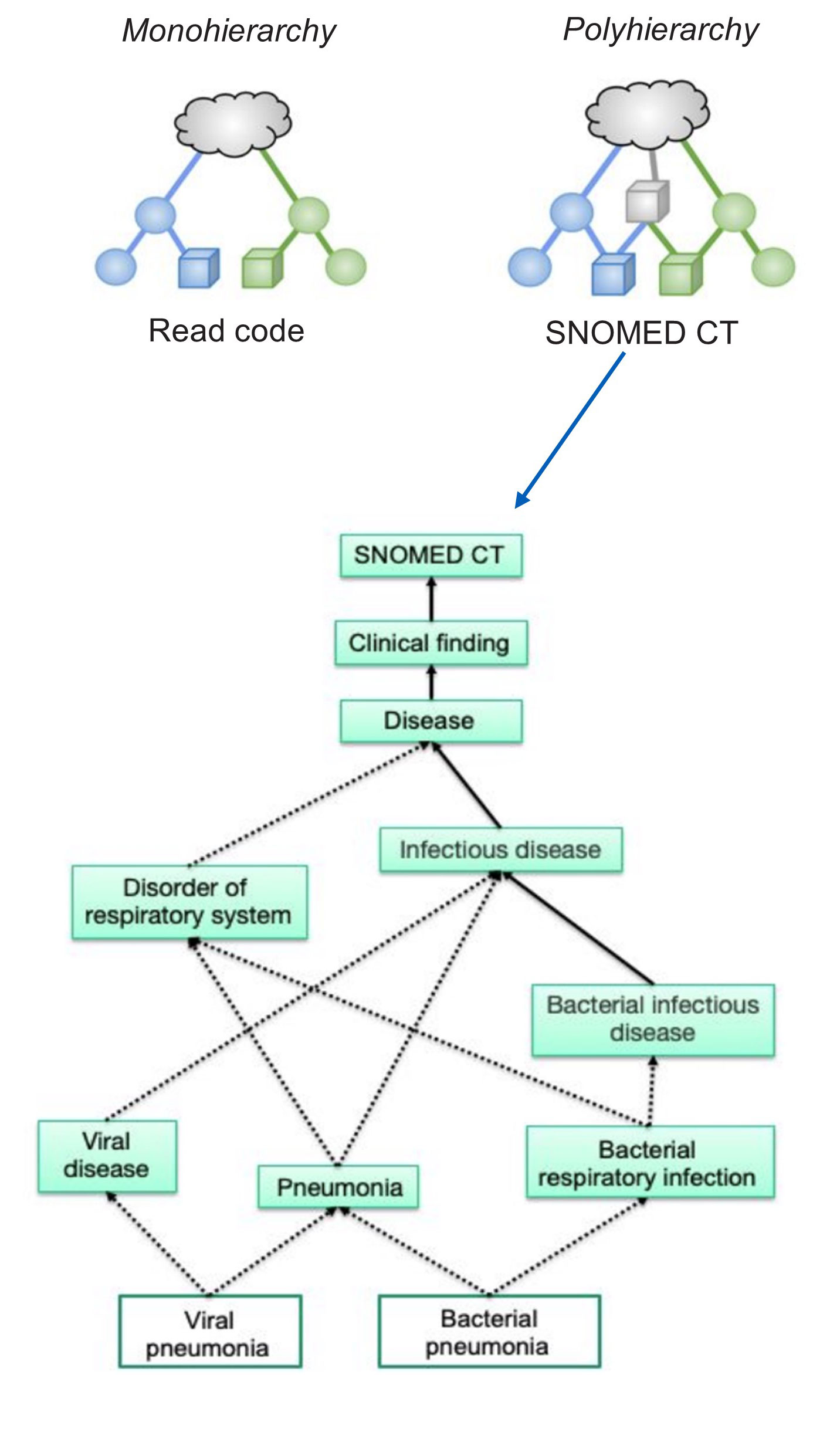
SNOMED CT is, therefore, a ‘polyhierarchical terminology’, see Figure 3. This feature means relationships in SNOMED CT can be powerful tools that provide meaning and richness to clinical concepts. Computer software can then be used to process clinically rich and structured information for a variety of broader uses.
Figure 3: Polyhierarchy vs monohierarchy
Hierarchies
SNOMED CT groups clinical concepts into 19 distinct categories known as ‘hierarchies’ (Figure 3 above). The SNOMED CT international starter guide provides detailed descriptions and examples of these hierarchies. The clinical concept of bacterial pneumonia (disorder), for example, sits within the ‘clinical finding’ hierarchy.
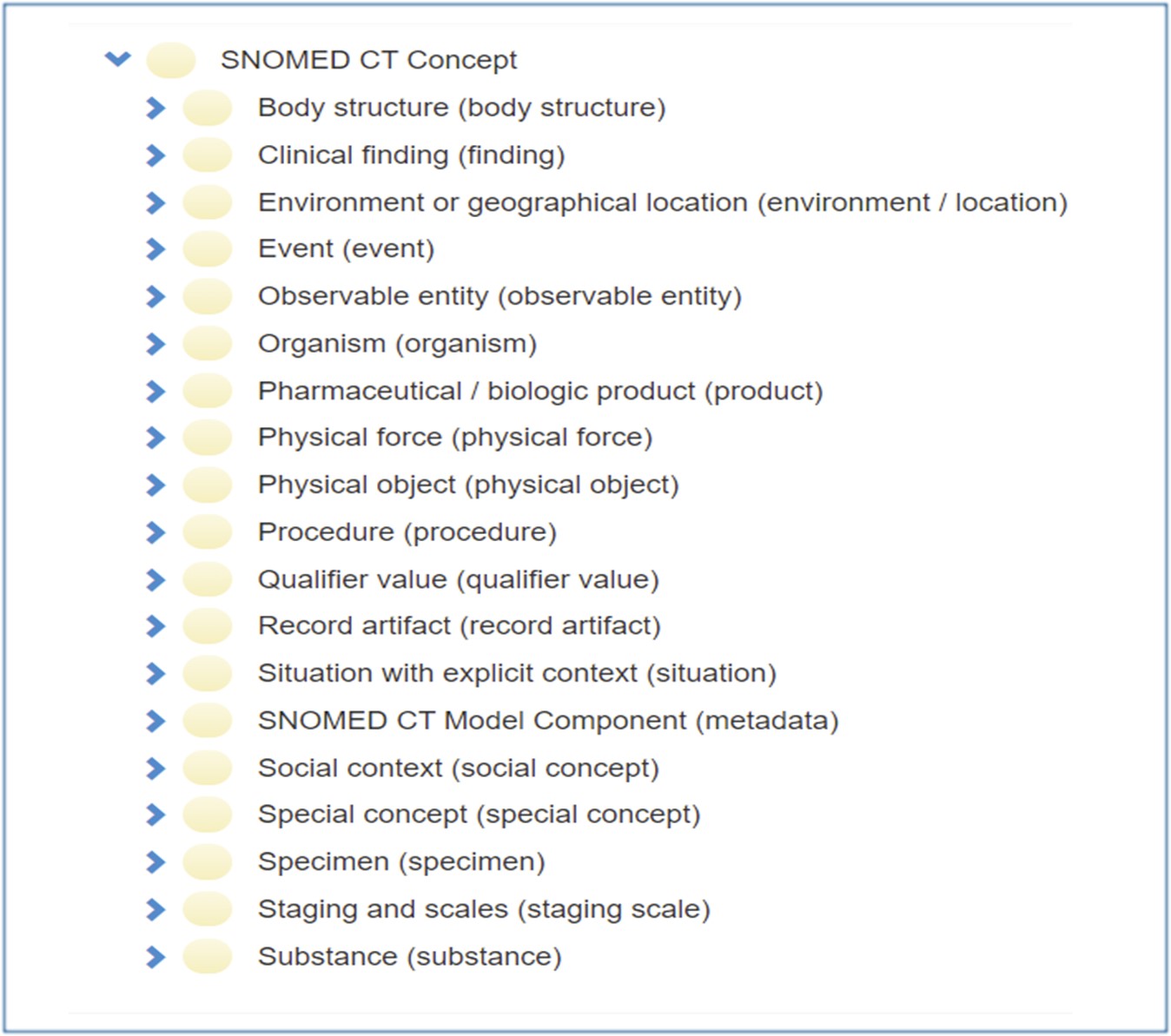
Clinical concepts range from general to more detailed clinical descriptions within each hierarchy. The complete SNOMED CT terminology with all the hierarchies and associated clinical concepts is comprehensive (see Figure 4).
Figure 4: Full list of SNOMED CT hierarchies (some of these will not be available in primary care systems)
Subsets
Even the UK Edition of SNOMED CT will contain hierarchies and concepts that will not be relevant in primary care systems. Mechanisms exist within SNOMED CT to account for this in the form of subsets. Subsets are curated lists of hierarchies and their associated clinical concepts containing content to match a particular use case.
The NHS works with terminologists and experts to create primary care specific subsets. These were initially based on the mapping from Read codes to SNOMED CT but are constantly expanded to include more clinical concepts.
NHS England has released guidance on some of the commonly used hierarchies and associated clinical concepts used in primary care – see Figures 5a and 5b below.
Figure 5a: Commonly used hierarchies in primary care
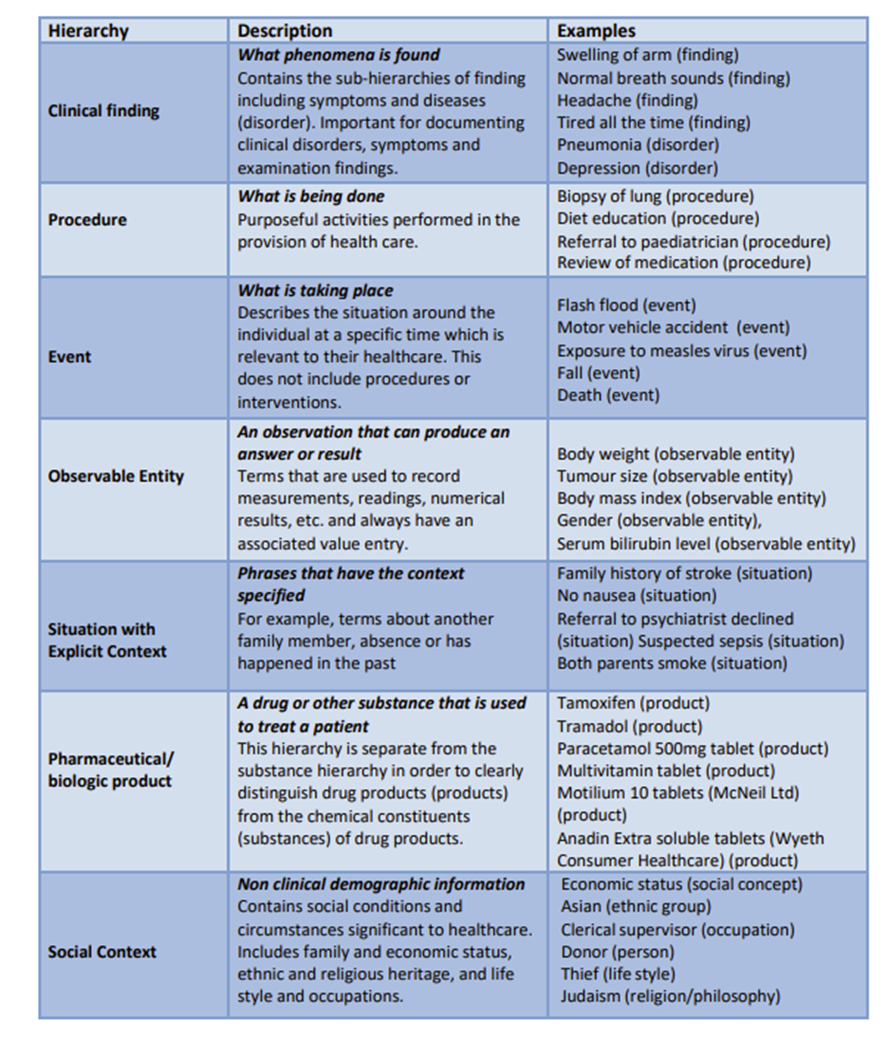
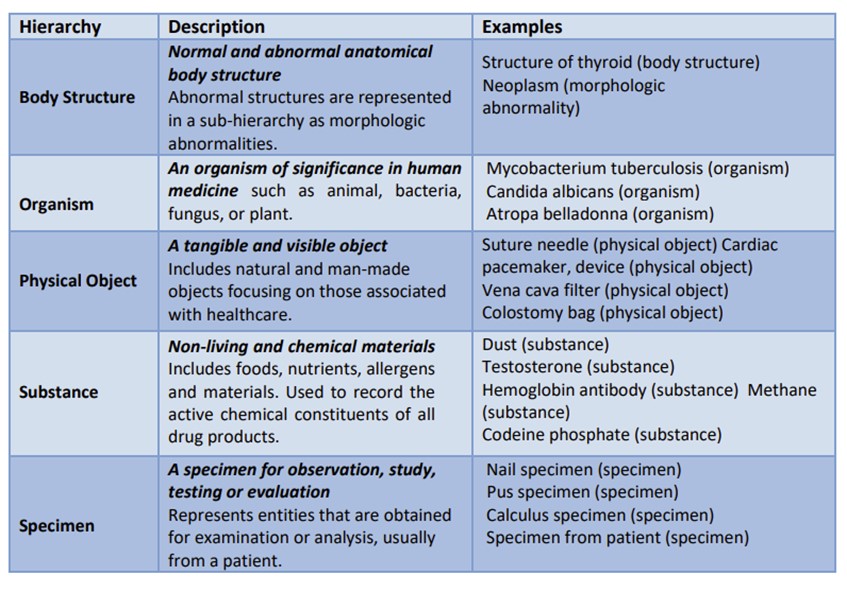
Figure 5b: Regularly used hierarchies usually with additional context.
Further information on hierarchies, concepts, descriptions and relationships can be found on our Learn about SNOMED CT pages.
Interestingly, a hierarchy (e.g. ‘procedure’) may cover a wider range of concepts, some being less obvious to users that are new to SNOMED CT. Carrying out a medication review or carrying out a referral to secondary care are both examples of a ‘procedure’. The Digital First Primary Care group and NHS England have created new ‘procedures’ to capture data on the use of new digital tools, examples include:
- Message sent using general practice online consultation system (procedure) (SNOMEDCT ID 149961000000105
- Encounter using general practice online consultation system (procedure)| SNOMED CT ID 149971000000103
You can explore the full range of content in the UK edition of SNOMED CT via the NHS Digital SNOMED CT browser.
The UK version of SNOMED CT is continually updated and released every six months or more frequently when needed.
Updates and inactivation
The breadth, depth, and continuous development of SNOMED CT allows it to meet the changing requirements of healthcare. System suppliers have processes to deal with updates and the introduction or inactivation of codes within the UK edition of SNOMED CT. When codes are no longer suitable for entry into the patient record, they are inactivated. NHS England or system suppliers will often provide an alternative code that can be used instead.
System suppliers also have mechanisms to ensure inactive codes are included in reports or decision support. Inactive codes, however, can no longer be entered into the patient record. This can impact data entry resources such as templates or protocols. Any historic codes that were valid at the time of entry do not need to be changed, In these instances, the inactivated codes will need to be removed or replaced with equivalent active codes. Some system suppliers have mechanisms to help identify affected resources affected by inactivated codes.
Further guidance on managing templates, protocols and reporting concerning inactivated codes can usually be found in education resources supplied by system suppliers.
Essential uses of SNOMED CT in primary care
The clinical information recorded using SNOMED CT has far-ranging impacts and essential uses, such as:
- creating searches and reports
- developing clinical templates and protocols
- extract services (e.g. General practice extraction service or GPES)
- GP2GP record transfer
- receiving electronic data such as discharge summaries in a coded format
- creating and updating information in the summary care record
- sharing information through the electronic referral service
- meeting quality outcomes framework (QOF) specifications
- meeting enhanced service specifications
- identifying patient groups for a specific intervention
SNOMED CT improves the quality of information that feeds into the services, frameworks and specifications above. This depends, of course, on users understanding how to code clinical information correctly and appropriately within the patient record. This is covered in more detail in the high quality patient records article in these Guidelines.
Entering information into clinical systems
System suppliers provide user-friendly interfaces to simplify how clinicians enter clinical information into the patient record. These are sometimes referred to as ‘code browsers’.
How system suppliers allow you to search, select and enter clinical information will vary. Generally, they enable simple search functions based on the first 3-4 letters of a clinical phrase you want to record. The word search will return all related clinical concepts and their associated codes. Users can then look up and down the parents or children for a particular concept and pick the most appropriate one.
Dual coding
Some system suppliers have a dual browser function during information entry that shows both Read codes and their equivalent (mapped) SNOMED CT codes. This means users can code in either Read or SNOMED CT. The clinical system will then dually code in the background based on the mapping between the two. Not all system suppliers have a dual browser function, and many will only allow you to search and code via SNOMED CT.
Specific training on how to interact with these can be found in resources hosted by your system supplier.
Free text
Users should code clinical information using SNOMED CT as much as possible to maximise its benefits. This applies even in systems that have dual browser functionality. It is not, however, always possible or appropriate to code clinical information. In these circumstances, using free-text entry is just as important to provide context and narrative within the patient record. In many situations, free text can be just as powerful as coded clinical entries. This is covered in more detail in the ‘High quality patient records’ article in this series.
Some systems allow free text to be directly linked to the coded information, but free text entry should never be used to alter the meaning of the coded information. Below is an example showing how dangerous inappropriate use of free text can be, Figure 6.
Figure 6: Entering clinical information | dangerous practice
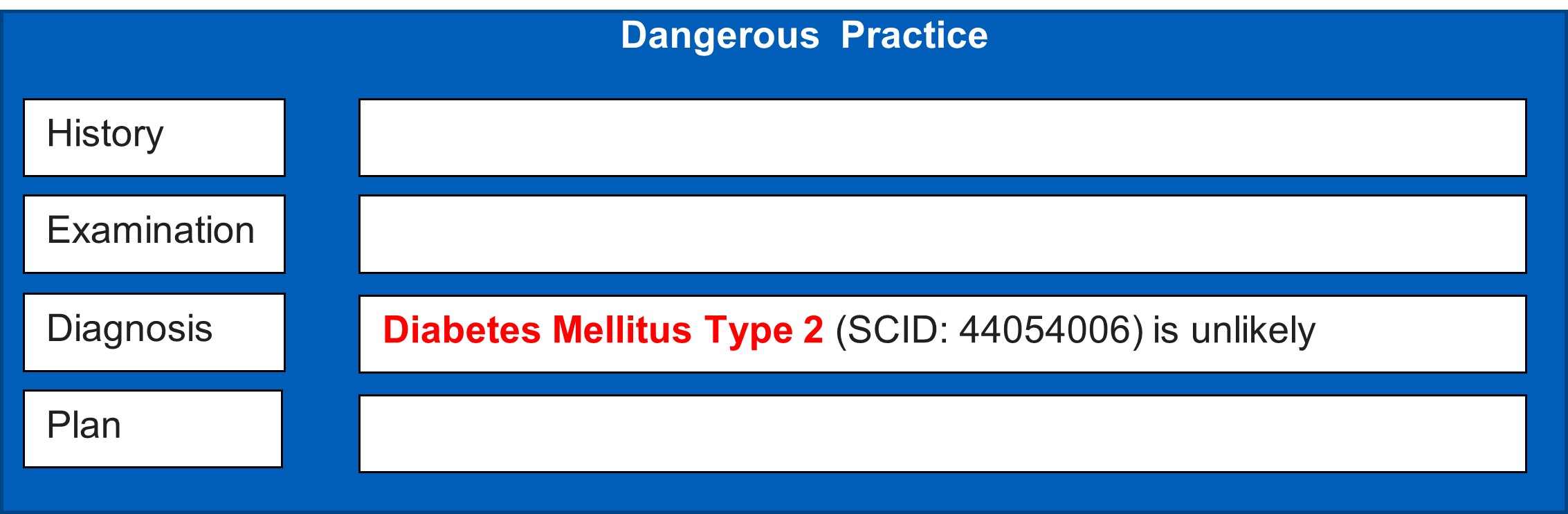
In this scenario, the user has coded diabetes mellitus type 2 and then altered the meaning with the free text entry. Unfortunately, when a computer reads the record or organisations create queries or trigger decision support, it will understand the patient to have diabetes mellitus type 2.
Requesting new content
System suppliers work closely with experts, professional bodies and NHS England to create primary care specific clinical content for use in their systems. Occasionally users may not be able to find a suitable clinical concept when trying to code clinical information in the patient record. This may be because the system supplier has limited the types of clinical information users can enter. For this reason, you should log requests for new content directly with your system supplier first. They can then support you on the next steps.
In general, practices should not be requesting local codes specific to their organisation, as this can have implications when sharing clinical data. Users should contact their system supplier to discuss best practices and next steps if required.
SNOMED CT queries/searches/templates
Some users in primary care will need to create searches, reports and templates based on SNOMED CT content recorded within the patient record. Examples include, but are not limited to:
- clinical reporting – tracing patients with a specific disorder or condition
- strategic reporting/searching – identifying a group of patients with a blood pressure > 140/90 over a specified period
- clinical entry template creation
Understanding how SNOMED CT is organised is important when carrying out these functions. The structured nature of SNOMED CT means users can retrieve information using broad or very specific categories of detail. Remember, SNOMED CT covers a large range of clinical information such as immunisations, family history, procedures, allergies, and medications.
Practices can use the breadth of coding in a variety of ways, some examples include:
- screening patients with long-term conditions
- targeting specific patient populations
- carrying out medicine optimisation searches
- searching for outstanding QOF (Quality and Outcomes Framework) targets
‘Delen‘ is the information and collaboration platform maintained by the NHS for terminology and classification products. Additional information can also be found in the resources within the Digital Primary Care portal .
Training on querying both SNOMED CT and historical Read code content can be found in the primary care education and training section in the Delen portal.
Championing and maximising the benefits of SNOMED CT
The primary users of SNOMED CT are clinical staff entering information into the patient record during care delivery. Information can, however, also be entered into patient records by summarisers, coders, and admin staff. Championing how to code effectively is very important.
Education and training
Educating and training staff helps to ensure the patient record is accurate and enables accurate record sharing and information retrieval. SNOMED International education) provides free to use e-learning modules on the basics of SNOMED CT. The Delen portal also hosts an education and training section that can be used to develop skills within an organisation.
Using SNOMED CT will not automatically result in high quality data being recorded in the patient record. High quality patient records depend on users understanding the system they are using. Organisations and individuals need to engage in best practice principles when recording clinical information in records. Users need to know why they are entering the information in a particular format and what it could mean.
The FutureNHS collaboration platform has a SNOMED CT workspace for the sharing of information and ideas (log-in required).
Practices should ensure users understand the following:
- organisational rules for coding clinical information during care encounters
- organisational rules or policies for coding incoming clinical information from outside sources
- system specific features that enable clinical coding within the patient record
- how to add coded information to problem lists and its implications
- the patient facing view of coded clinical and free text information within the patient record
- guidance on linking coded information within the patient record
- procedures for maintaining, updating, and correcting coded information within the patient record
Summary
- SNOMED CT is the most comprehensive common clinical language currently available.
- It can be used across all care settings and clinical domains. Using SNOMED CT across these settings will allow these systems to communicate and share information effectively.
- Communicating accurately recorded clinical information will ensure the right information is available to the right people at the right time.
- Patients, clinical users, local and national health organisation all stand to benefit from SNOMED CT.
- Effective use of SNOMED CT is vital to achieving elements of the NHS Long Term Plan and enabling integrated care systems.
- SNOMED CT will, however, only be a success if it is supported and championed across the NHS.
- Clinical coding is everybody’s responsibility. Individuals and organisations delivering care must play all their part in making SNOMED CT a success.
Related GPG content
- Shared care records
- Summary care records (SCR)
- e-Referrals
- GP2GP – transferred in records – processing
- High quality patient records
- Calculating Quality Reporting Service (CQRS) and Quality Outcomes Framework (QOF)
- Interoperability
Other helpful resources
- NHS Digital, editorial standards SNOMED CT editorial standards