
Foreword
England and Wales are leading the way as the only countries in the world where every death receives an independent review, and where the bereaved are always given an opportunity to raise concerns with someone not involved in providing care.
I consider the recent changes in the NHS among the most significant healthcare developments of the past decade. Patients and families are being empowered and given a voice through initiatives such as the medical examiner system and Martha’s Rule in England and Call4Concern in Wales. These initiatives offer significant opportunities to save lives and improve patient safety and care.
This is why I am proud of the impact medical examiners have had, an impact that has grown markedly since the system became a statutory requirement in September 2024. This progress is welcome following more than 2 decades of calls for the introduction of medical examiners, including from independent inquiries such as those in Mid Staffordshire, Gosport and Morecambe Bay. The continuing need for the safeguarding role of medical examiners is clear.
The benefits delivered by medical examiners go further, and Ministry of Justice coroner statistics for 2025 show that medical examiners are having a dramatic impact.
Comparing 2023 (the final full year before medical examiner scrutiny became a statutory requirement for all deaths) with 2025 (the first full year), there were marked reductions in the number of deaths referred to coroners, the number of post-mortem examinations ordered by coroners, and the number of deaths where coroners concluded death had natural causes.
This has reduced unnecessary administration and public spending, while also preventing needless distress and delay for bereaved people.
At the same time, medical examiners are identifying cases which require referral to a coroner, including some that may previously have been missed. The Ministry of Justice has noted that medical examiners enable coronial resources to be focused on cases that require their attention.
Medical examiners in England and Wales reported that half a million families and carers have had the opportunity to speak with an independent medical examiner or officer about the care of their loved one. The fact that almost all bereaved people took up this opportunity indicates how well it has been received.
These discussions often resolve matters that might otherwise have developed into serious or protracted complaints. Unresolved concerns can negatively impact the grieving process, and medical examiners help reduce this impact.
Medical examiners are also improving safeguards and identifying opportunities to improve care. Tens of thousands of such issues have been detected and referred for further review. In many cases, bereaved people have nothing but praise for the staff who provided care, and I ask that this valuable feedback also be made available to front-line healthcare teams.
As one medical examiner office noted, “All themes and trends are reported to the relevant trust or community provider. This includes examples of excellent care as well as care that could be improved.”
Where there can be learning to improve care for future patients, I encourage all healthcare providers and commissioners to take advantage of the insights medical examiners provide.
This is the only process that offers the public a universal opportunity to raise concerns, while also providing such a comprehensive overview and identifying issues so quickly after they arise. No other country has a system in which senior doctors independently review all natural deaths. This collaborative, non-forensic approach, working alongside the legal processes for death review, makes England and Wales world leaders.
The benefits of medical examiners are likely to accumulate over time, including helping the NHS to avoid significant additional financial liabilities through greatly improved assurance . The system already operates at lower cost than previous arrangements, even before wider savings for publicly funded services such as coroners and register offices are considered.
I will continue to work with colleagues across England and Wales to maximise the emerging benefits of the medical examiner system. I would also like to take this opportunity to thank all the medical examiners and medical examiner officers for their hard work and commitment to what I believe is a world-leading service.
Dr Huw Twamley
National Medical Examiner for England and Wales
Executive summary
The National Medical Examiner is required to produce a report for the Secretary of State and Welsh Ministers under the National Medical Examiner (Additional Functions) Regulations 2024.
The report sets out how the National Medical Examiner, medical examiners and attending medical practitioners have exercised their functions under the Medical Certificate of Cause of Death Regulations 2024.
Medical examiners were introduced as part of the death certification reforms with the following aims:
- Better safeguards for the public through independent scrutiny of all non-coronial deaths.
- Improve experience for bereaved people and provide an opportunity for them to raise concerns with someone not involved in caring for the deceased person.
- Reduce unnecessary referrals to coroners, while ensuring that appropriate deaths are referred to the coroner.
- Improve the quality of death certification and of mortality data.
As detailed in the report, key achievements in 2025 include:
- half a million bereaved families every year are now being given an opportunity to raise concerns about care and to ask questions about what caused the death of their loved ones, with 97% taking up this opportunity
- independent scrutiny of all deaths not investigated by coroners, medical examiners in England and Wales reported they provided independent scrutiny of 501,427 deaths
- by giving bereaved people a voice and the opportunity to raise concerns with someone not involved in providing care, medical examiners help the NHS improve care for future patients and reduce the likelihood that concerns escalate into complaints
- official Ministry of Justice coroner statistics reveal unprecedented reductions in unnecessary or unproductive referrals to coroners, with many measures now at their lowest since records began:
- the number of deaths referred to coroners fell by a quarter (24.2%) between 2023 and 2025, reducing bureaucracy, saving public money and avoiding unnecessary distress for bereaved people; (2023 was the last year where there was no statutory medical examiner system, and 2025 the first year medical examiners reviewed all deaths not investigated by coroners)
- coroners ordered 10,000 fewer post-mortems in 2025 than in 2023
- deaths where a natural cause was established without post-mortem examination or inquest, but nevertheless were dealt with by coroners, fell by more than 40% between 2023 and 2025
- inquests that concluded the causes of death were natural fell by more than a third (34%) in 2025 compared to 2023
- medical examiners identified 36,302 deaths for further clinical governance review in England and Wales, and 2,018 patient safety incidents in England
- improving resilience in the system, with medical examiner offices in England reporting they were able to facilitate requests for rapid scrutiny in around 11,400 cases (90% of requests), and in Wales, 611 cases (100%), and steady improvement in turnaround times in almost all areas of England and Wales through 2025
- eradication of deaths which the Office for National Statistics (ONS) classified as uncertified, from an annual rate of more than 10,000 (3 cases in 2025, which were certified in other jurisdictions)
Looking to the future, the National Medical Examiner wishes to:
- strengthen the voice of bereaved people and their ability to raise concerns
- achieve greater alignment and consistency in how medical examiners carry out their duties
- make greater use of data and research for learning to improve healthcare
- understand, when completed, the University of Birmingham’s evaluation of the death certification reforms
Context
In England, there are 125 medical examiner offices located in NHS trusts.
In Wales, NHS Wales Shared Services Partnership (NWSSP) hosts the all-Wales medical examiner service, located in 4 hub offices.
The importance of implementing the death certification reforms and the statutory medical examiner system has been underlined in numerous reports and inquiries, including:
- The Shipman Inquiry third report
- Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry
- Morecambe Bay Investigation report
- Gosport Independent Panel report: government response
The government introduced the medical examiner system with 4 principal aims:
- better safeguards for the public through independent scrutiny of all non-coronial deaths
- improve experience for bereaved people, and provide an opportunity for them to raise concerns with someone not involved in caring for the deceased
- ensure deaths are referred to the coroner when appropriate, and reduce unnecessary referrals
- improve the quality of death certification and mortality data
This report explores the impact of medical examiners against these objectives.
Better safeguards for the public
Medical examiners have transformed the experience of bereaved people, reporting that they provided independent scrutiny of 501,927 deaths in 2025, 472,120 in England and 29,307 in Wales.
Half a million bereaved families in England and Wales had the opportunity to speak with someone independent who had not been involved in caring for their loved one.
The appetite for such a service is almost universal; medical examiner offices in both England and Wales reported that families in the immediate aftermath of a bereavement almost always took up this opportunity.
Feedback from bereaved people about the service remains overwhelmingly positive.
A distinguishing feature of the medical examiner system is the empowerment of the public. The NHS needs to embrace feedback from members of the public, as it enables us to identify and put right areas where we can and should do better.
Too many independent inquiries have highlighted a regrettable pattern: concerns have been overlooked, downplayed or explained away. Early opportunities to put things right are missed, particularly alerts from carers and families.
Through medical examiners, the NHS can identify issues early, take action to resolve them, and respond quickly to complaints before they escalate.
Given time and support, medical examiners have the potential to avoid resource-sapping serious complaints, not to mention preventing significant public resources from being dedicated to litigation and independent inquiries.
Bereaved families may raise points that some find inconvenient, but medical practitioners should always be eager to listen to the views of patients, their families and carers, and to consider how they can learn and improve practice and that of their clinical teams.
Often, bereaved people also provide positive feedback about the care provided to their loved ones, and medical examiner offices are asked to communicate this to front-line staff.
However, where care could have been improved, medical examiners refer cases for further review under established local clinical governance processes, and the coroner, where required.
In 2025, medical examiners referred 9,134 deaths in Wales for review under the Welsh Health and Care Quality Standards (HCQS). In the same year, in England, medical examiners referred 27,158 deaths for further clinical governance review and identified more than 2,000 patient safety incidents.
Once the medical examiner has referred the concern to the appropriate healthcare organisation, it is the responsibility of that healthcare organisation to determine the appropriate review process, carry out the review and take appropriate action.
Medical examiners also notified deaths to coroners where appropriate, 1,856 in Wales and 44,753 in England.
Alongside responding to concerns raised by the pubic, the introduction of the medical examiner system has created a cohort of independent medical practitioners across England and Wales trained to review cases in which they were not involved in care, and who spend the vast majority of their time in clinical practice.
This allows them to apply their enhanced insights across clinical pathways and within their clinical teams.
The increased scrutiny of deaths by independent medical examiners is designed to deter as well as detect deficiencies in healthcare, whether they arise through negligence or criminal intent.
The impact is difficult to quantify, and judgements about the effectiveness of these arrangements can only be made with time.
Many of the opportunities identified for improvements in healthcare are extremely local and do not require regional or national action.
We do not have a comprehensive database of all the safety issues identified and actioned as a result of medical examiner scrutiny in England and Wales.
However, a number of significant examples have been reported. These include:
- 2 cases of potential neglect and physical abuse of a vulnerable adult, which were referred by medical examiners to the coroner, and were passed to the police for investigation
- medical examiner office findings leading to investigations of 2 care homes, 1 leading to a police investigation
- analysis in Wales suggests medical examiners and officers played a significant role in 14 cases that resulted in Prevention of Future Deaths reports by coroners, having identified issues and ensured appropriate referral to the coroner
- increased incidence of infective endocarditis related to aortic valves resulted in a multi-centre investigation and work with the manufacturer
- medical examiner and family input to the coroner resulted in preventing future harm action at a care provider
- on-ward improvements after flagging concerns about naso-gastric tube use
- a case of potential coercion of a patient with a learning disability identified
- concerns about a consultant raised by NHS staff and bereaved people, escalated to the Chief Medical Officer
- concerns about a GP practice, including omissions from patient notes and visits to care homes, under review by the integrated care board (ICB)
- a number of concerns identified relating to particular healthcare providers, which were escalated to appropriate commissioning and oversight bodies, for example, leading to safeguarding reviews
- identifying and escalating repeated concerns from bereaved people about a care home
These are a small sample that demonstrate the value that medical examiners offer through early detection, and by listening to bereaved people and giving them a voice.
Broader themes identified by medical examiners in England and Wales included:
- missed clinical deterioration
- delays such as in diagnosis
- end-of-life concerns
- discharge processes
These themes are set out in more detail in Appendix 1, and other information provided by medical examiner offices is published alongside this report.
Experience of bereaved people
A key distinguishing feature of the medical examiner system is its ability to empower bereaved people and give them a voice.
The appreciation bereaved people have for this opportunity is demonstrated by the fact that take-up is almost universal.
Some people sadly die without known next of kin, and a small proportion of bereaved people understandably prefer not to take up the offer during a period of grief.
Nevertheless, medical examiner offices in both England and Wales report that an interaction with next of kin took place in 97% of cases.
Feedback received by medical examiner offices continues to be overwhelmingly positive, and many medical examiner offices actively seek feedback from bereaved people about their experience of the medical examiner system. This report commends and encourages the sensitive use of such initiatives.
One medical examiner office reported that 88% to 96% of responses indicated that the bereaved had found the medical examiner office helpful or extremely helpful.
Another office reported that 95% of survey respondents said the medical examiner service was helpful to them; the remaining cases were direct coroner referrals, so the bereaved had no contact with the medical examiner.
Feedback from bereaved people:
- “this has put my mind at ease from worrying if something was missed or something more could have been done to help her”
Feedback reported by medical examiner offices:
- “…during discussions with bereaved [people], we have received ‘surprised’ responses, with regards to the efficiency and the depth that each case is looked into, continuously”
- ” … positive feedback from our local Muslim councillors with regards to our processing of rapid release cases. We have also recently received feedback via the Bereavement Office that our local funeral directors commend our team and service at their regional meetings”
Feedback from register office:
- “I am writing to make you aware that we have had some excellent feedback from a bereaved relative regarding your support in expediting the Medical Certificate of Cause of Death (MCCD) scrutiny for an urgent death registration…knew that he could trust the Medical Examiner Office and registration teams to work together to ensure that all the paperwork was in place in time for his urgent registration appointment”
The fact that medical examiners actively seek the perspectives of families and carers, giving them a voice and providing the NHS with an immediate opportunity to detect issues with care, is unique among mortality review processes.
As has been seen in the success of Martha’s Rule, and the similar principles adopted in Call4Concern in Wales, family and friends often have insights that complement the skills and dedication of clinical staff, because those who know patients best can be more perceptive of soft signs of deterioration and other alterations in the health of patients.
Medical examiners provide the opportunity, in real time or very shortly after a death, to detect things that could have gone better, and for healthcare providers to improve care for future patients.
As medical examiners and officers are not involved in providing care for the deceased, bereaved people can find it easier to raise concerns.
They can do this without awkwardness or feeling that they are challenging staff, whom they also feel grateful to, for most aspects of care.
Questions have been raised about whether the death certification reforms (which changed the work of doctors completing MCCDs, coroners and register offices, not just medical examiners) would significantly increase the time taken to register deaths. There is ambition and commitment to identify and reduce or eliminate avoidable delays to death certification without compromising the integrity of independent medical examiner scrutiny.
Partnership working is effective in most areas; but in a minority there remains room for improvement. The number of areas where such issues remain appears to be falling, but after more than 18 months under the new system, there are few excuses for unnecessary obstructions.
All those involved in certification and registration must continue to work together to avoid causing unnecessary delay and distress to bereaved families. Improvements will require leadership from those overseeing the work of attending medical practitioners, coroners and registrars as well as medical examiners, who do not oversee the process or work of other agencies.
The typical time to register deaths seems to be settling at 7-8 days, compared to 6-7 days under the previous arrangements which offered significantly less assurance and required next of kin to register deaths more quickly. However there is some variation, particularly after public holidays.
NHS England and NWSSP monitor the work of medical examiner offices, including the time taken, though the integrity of scrutiny is also important and kept under review.
Between October and December 2025, 105 medical examiner offices in England (84%) reported a median time of 5 days or fewer to send MCCDs to registrars after a death.
More than a third reported a median time of 3 days or fewer. This includes the time taken by attending practitioners to refer deaths to medical examiners (estimated at slightly less than 2 days on average in England).
In Wales, there were also significant reductions in the time taken to complete MCCDs during 2025. The time taken by attending practitioners to refer deaths to medical examiners in Wales fell from a mean of 7 days at the start of the year to 2 days in November 2025.
This contributed to a reduction in the average (mean) time from death to sending MCCDs to registrars in Wales from 12 days in January and February 2025 to 6 days in October and November.
Medical examiners have delivered a step change in assurance. In many areas, they and their partners in the registration process have worked effectively to maintain existing registration times.
Where times have increased, lead medical examiners and officers are actively exploring solutions with support from regional medical examiners and officers.
In many cases, the causes lie outside the medical examiner office processes, with responsibility shared across the system, including attending medical practitioners, coroners, register offices, funeral directors and crematorium staff.
Changes to the registration period are also likely to have had an impact, as next of kin now have 5 days from the date the MCCD is completed to register a death, rather than 5 days from the date of death. However, whatever the causes, unnecessary delays are undesirable.
During the winter period, there are more deaths, and historically, registrations have taken longer.
After the 2024/25 winter, the previous National Medical Examiner encouraged medical examiner offices to work with partners to refine processes and improve system resilience. In most areas, partnerships with GPs and other attending practitioners, coroners and register offices delivered an improved experience for bereaved people during winter 2025/26.
Recent data illustrates continuing improvement compared to a year ago:
- In January to March 2025, 21 medical examiner offices reported the typical time to receive referrals after death and complete scrutiny was more than 6 days.
- In January to March 2026, this was reduced to 12 offices.
There are occasions where bereaved people request more rapid registration of deaths.
To avoid unnecessary distress for bereaved families, regardless of the reasons for such requests, the National Medical Examiner’s guidance requires medical examiner offices to have a system of prioritisation and arrangements that reflect the needs of the communities they serve.
There can be many reasons for these requests, including:
- families who have travelled long distances (both within the UK and internationally) to make arrangements for the deceased
- organ and tissue donation
- to facilitate certain religious practices
We seek, where possible, to facilitate all such requests to avoid causing distress to bereaved families. Medical examiner offices in England reported they were able to facilitate requests in 11,365 cases (90% of requests), and in Wales, 611 cases (100%).
In cases where this was not possible, medical examiner offices in England reported 6% could not be achieved due to deaths with more complex issues, and in 3%, the attending practitioner was not available to provide an MCCD.
All medical examiner offices are required to have appropriate arrangements in place to meet the needs of their local community. NWSSP operates hub offices in Wales, which are open on public holidays (except Christmas Day) and have a medical examiner and officer available at weekends.
In England, arrangements vary depending on local circumstances and demand, and at 31 December 2025, 79 medical examiner offices reported operating at weekends and bank holidays.
As noted previously, prompt registration of deaths at weekends and public holidays depends on all parts of the system operating out of hours, including attending practitioners (such as GPs) and register offices.
More appropriate referrals to coroners
A key objective of introducing medical examiners was to reduce unnecessary referrals to coroners and ensure that deaths requiring such referrals were not missed. Medical examiners notified 46,609 deaths in England and Wales to coroners after scrutiny.
Since the death certification reforms were introduced and medical examiners have provided scrutiny of every death not investigated by coroners, the number of deaths certified by doctors increased, and those certified by coroners decreased during 2025, by around 5,000 to 6,000 annually. Chart 1 below illustrates this pattern.
Chart 1: deaths registered in England and Wales
Rolling totals by certification type: doctor-certified deaths compared with deaths certified by coroners and others, January to December 2025 (source: Office for National Statistics)
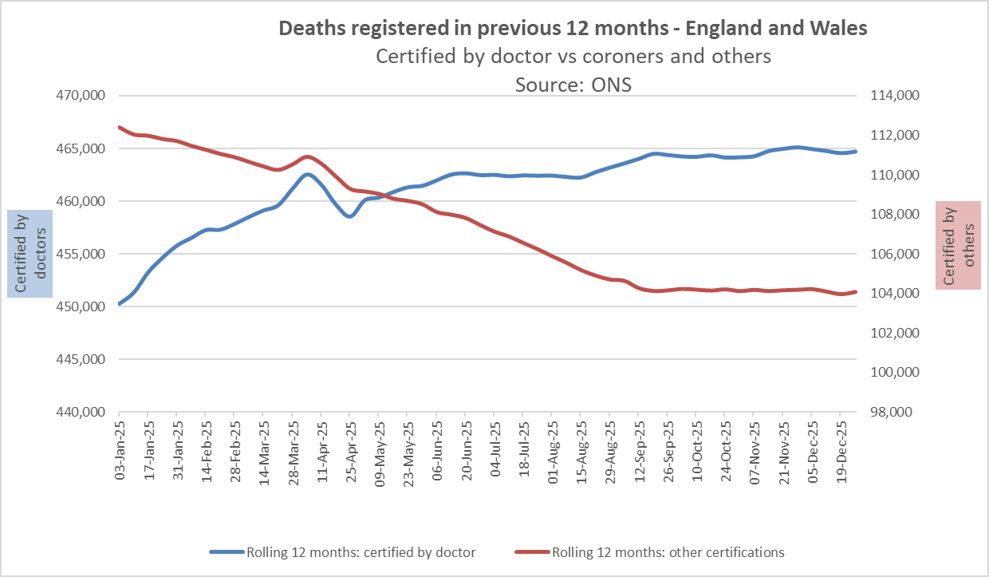
Chart description
The number of deaths certified by doctors increases steadily over the year, rising from around 450,000 at the start of January to approximately 465,000 by December. There is a small dip around late April before the upward trend continues.
In contrast, deaths certified by coroners and others decrease over the same period, falling from about 113,000 at the start of the year to around 104,000 by December. The decline is gradual, with a slight flattening in the autumn months.
Before the introduction of the present system, there were significant inefficiencies and administrative burdens.
In 2019, when the implementation of medical examiners on a non-statutory basis began, just 14% of deaths reported to coroners resulted in an inquest.
Of the remaining 86% of cases, many absorbed resources in the form of post-mortem examinations and unproductive bureaucratic transactions among doctors, registrars and coroners.
In addition, bereaved people were often caught between the various statutory agencies, adding to their distress in a time of grief.
Coroner statistics for 2025 published by the Ministry of Justice clearly illustrate the benefits medical examiners deliver across public services.
Between 2023 (the last full year before medical examiners became a statutory function) and 2025 (the first full year), the number of deaths reported to coroners fell by almost 50,000, a reduction of nearly a quarter.
Consequently, the proportion of all deaths reported to coroners fell from 34% in 2023 to 26% in 2025.
Medical examiners also contributed to a reduction of 10,000 post-mortem examinations ordered by coroners between 2023 and 2025.
This is to be welcomed, given concerns expressed in recent years about the number of post-mortem examinations ordered and the public resource these require.
While some post-mortems will continue to be necessary, the reduction will be welcomed by many stakeholders in the certification and registration process, and not least by bereaved people.
It will also provide reassurance to members of certain faith communities who can find the need for post-mortem examination of the deceased person particularly distressing.
The number of inquests with conclusions of natural causes fell by more than a third between 2023 and 2025, from 5,632 to 3,729.
The number of coronial cases where, despite coronial involvement, neither a post-mortem nor an inquest proved necessary fell by 41% between 2023 and 2025 (these are cases where a natural cause of death was established after the report of death).
These reductions are consistent with medical examiners preventing unnecessary referrals and work for coroners, while identifying cases that may have been missed previously.
The number of cases where an inquest was opened showed only a slight reduction to 36,000, but the proportion of referred deaths that resulted in an inquest rose to 24% in 2025.
The Ministry of Justice notes that several measures are at their lowest since reporting began in 1995, and comments, “The fall in deaths reported to coroners coincides with the introduction of the statutory Medical Examiner system in September 2024. Almost a quarter of these deaths reported to coroners resulted in inquests, the highest proportion since the annual time series began in 1995, although total inquests opened fell slightly over the same period…The new arrangements also ensure that cases are managed in the right parts of the system…”
It is likely that medical examiners were affecting coroner workload before 2023, as the incremental rollout of the non-statutory medical examiner system meant an increasing proportion of deaths from 2019 have been reviewed by medical examiners.
Nevertheless, the change accelerated once it became a requirement that all deaths not investigated by a coroner be reviewed by a medical examiner.
This is illustrated in table 1 and charts 2 to 5 below.
Table 1: Ministry of Justice coroner statistics and analysis
| 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | 2025 | |
|---|---|---|---|---|---|---|---|
|
Deaths reported to coroners |
210,900 |
205,400 |
195,200 |
208,400 |
195,000 |
174,900 |
147,800 |
|
% of registered deaths reported to coroners |
40% |
34% |
33% |
36% |
34% |
31% |
26% |
|
Change in deaths reported to coroners |
-9,700 |
-5,500 |
-10,200 |
13,200 |
-13,400 |
-20,100 |
-27,100 |
|
% change in deaths reported to coroners |
-4% |
-3% |
-5% |
7% |
-6% |
-10% |
-15% |
|
% change since before statutory medical examiners | n/a | n/a | n/a | n/a | n/a | n/a |
-24% |
|
Post-mortem examinations ordered |
82,100 |
79,400 |
84,600 |
90,200 |
86,000 |
81,200 |
75,900 |
|
Change in post-mortem examinations ordered |
-4,400 |
-2,700 |
5,200 |
5,600 |
-4,200 |
-4,800 |
-5,300 |
|
% change in post-mortem examinations ordered |
-5% |
-3% |
7% |
7% |
-5% |
-6% |
-7% |
|
Reduction in postmortems since before statutory ME system | n/a | n/a | n/a | n/a | n/a | n/a |
-10,100 |
|
% change since before statutory medical examiners |
|
|
|
|
|
|
-12% |
|
Inquests opened |
30,000 |
32,000 |
32,800 |
36,300 |
36,900 |
36,700 |
36,000 |
|
% change in inquests opened |
3.1% |
6.7% |
2.5% |
10.7% |
1.7% |
-0.5% |
-1.9% |
|
Inquests opened as % of deaths reported |
14% |
16% |
17% |
17% |
19% |
21% |
24% |
|
% change since before statutory medical examiners | n/a | n/a | n/a | n/a | n/a | n/a |
-2.4% |
|
Inquest conclusions of natural causes | n/a | n/a | n/a |
5,139 |
5,632 |
4,911 |
3,729 |
|
% of inquests with conclusions of natural causes | n/a | n/a | n/a |
14% |
14% |
12% |
10% |
|
% change in inquests with conclusions of natural causes | n/a | n/a | n/a | n/a |
10% |
-13% |
-24% |
|
% change since before statutory medical examiners |
n/a |
n/a |
n/a |
n/a |
n/a |
n/a |
-34% |
|
Cases requiring neither a post-mortem nor inquest |
114,197 |
109,816 |
94,004 |
98,839 |
88,776 |
73,540 |
52,036 |
|
Change in cases requiring no post-mortem or inquest |
-6,703 |
-4,381 |
-15,812 |
4,835 |
-10,063 |
-15,236 |
-21,504 |
|
% change in cases requiring no post-mortem or inquest |
-6% |
-4% |
-14% |
5% |
-10% |
-17% |
-29% |
|
% change since before statutory medical examiners |
n/a |
n/a |
n/a |
n/a |
n/a |
n/a |
-41% |
Chart 2: number of deaths reported to coroners
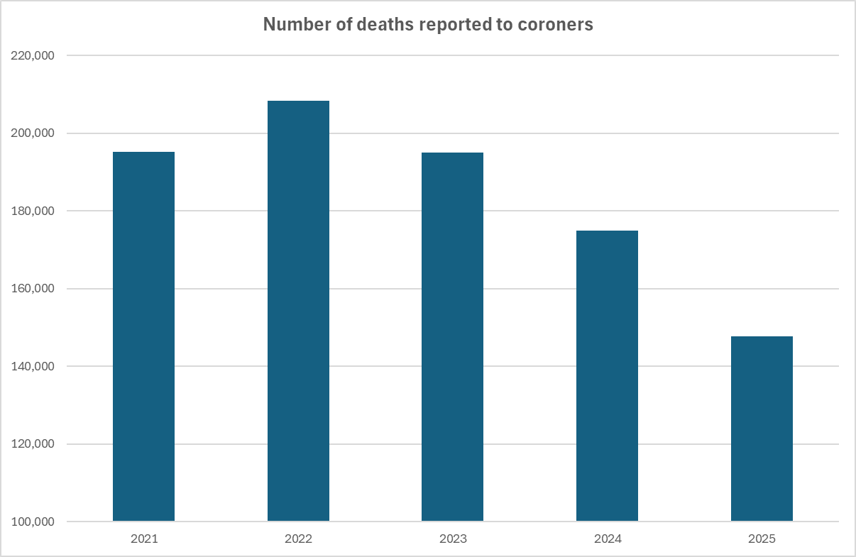
Chart description
The number of deaths reported to coroners increases slightly from 195,000 in 2021 to 208,000 in 2022. It then falls back to 195,000 in 2023, with accelerating falls to 175,000 in 2024 and 148,000 in 2025.
Chart 3: % of registered deaths reported to coroners
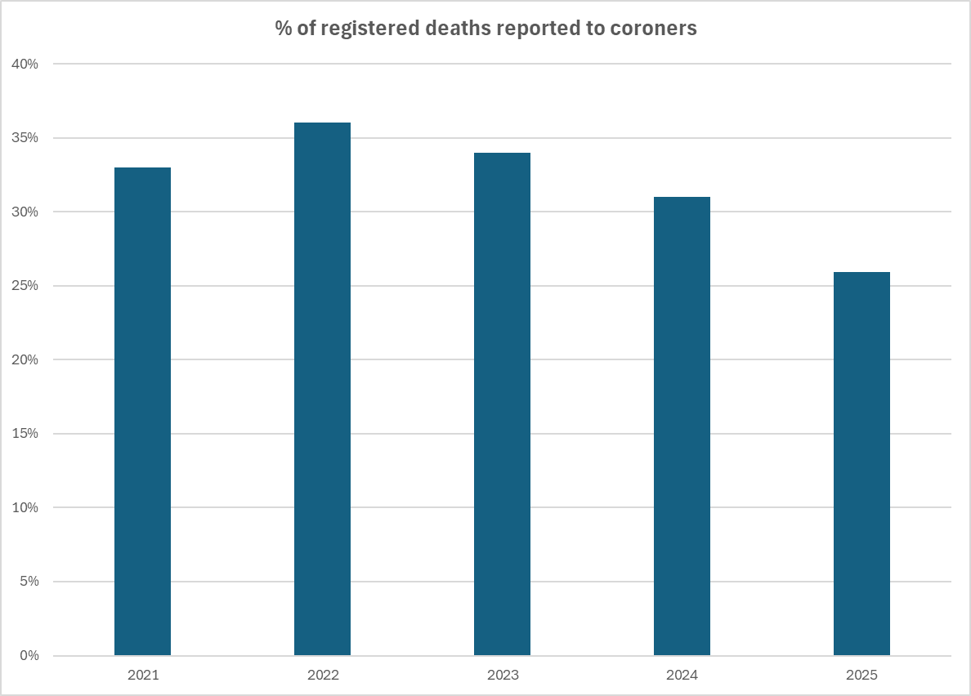
Chart description
The proportion of all registered deaths reported to coroners rises from 33% in 2021 to 36% in 2022. The proportion falls back to 34% in 2023, with accelerating falls to 31% in 2024 and 26% in 2025.
Chart 4: inquests opened as % of deaths reported to coroners
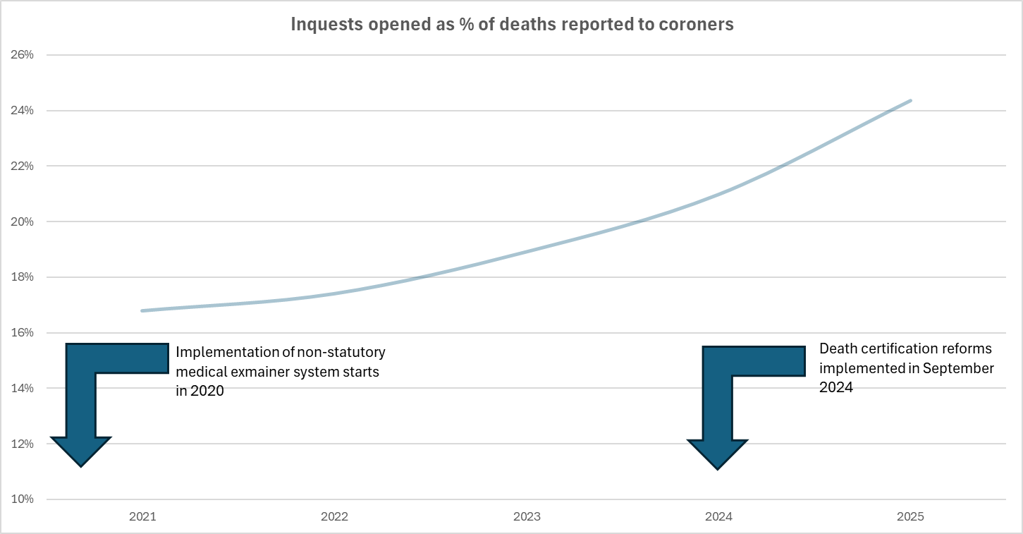
Chart description
The chart shows a smoothed line reflecting the increase between 2021 and 2025 in the proportion of deaths reported to coroners that result in an inquest from.
The proportion increases from 17% in 2021 and 2022, to 19% in 2023, 21% in 2024 and 24% in 2025.
The chart also indicates the start of implementing the medical examiner system on a non-statutory basis in 2020, and commencement of the statutory system in 2024.
Chart 5: cases requiring neither a post-mortem nor inquest
Cases where a natural cause of death was established after the death was reported to the coroner
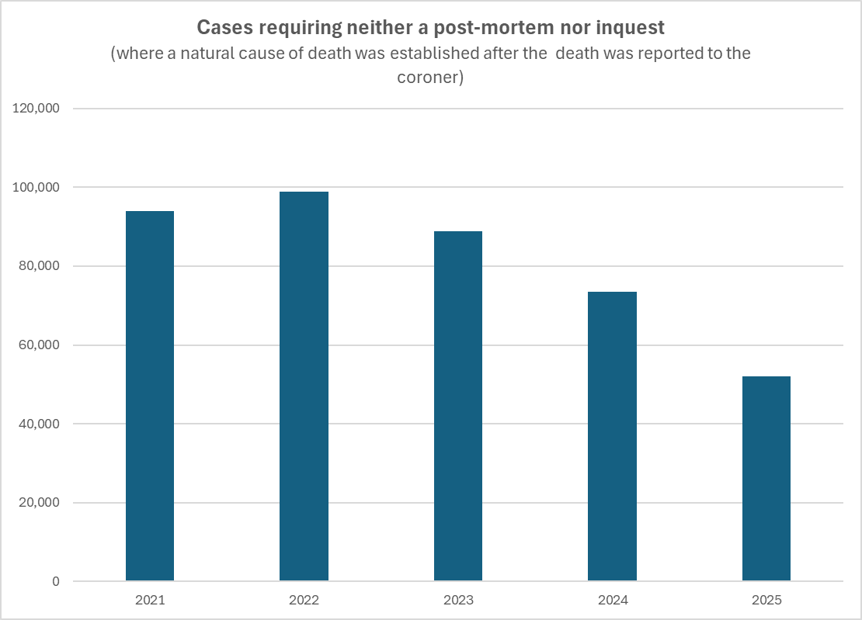
Chart description
The chart shows the number of deaths reported to coroners which did not require a post-mortem or inquest (because natural causes were established after referral to the coroner).
The number increases from 94,000 in 2021 to nearly 99,000 in 2022, before falling back to 89,000 in 2023. The decline accelerates to 73,500 in 2024 and 52,000 in 2025.
Taken together, this data is consistent with fewer unnecessary or unproductive referrals to the coroner, and that referrals made to coroners are more likely to be appropriate and to require inquests.
Overall, they indicate that the ambition to ensure that notifications to the coroner become more appropriate is being realised.
There are matters that should be kept under review to ensure the system continues to deliver the intended safeguards.
In some cases, medical practitioners may sometimes be cautious about proposing causes of death in an MCCD, and in some cases coroners have asked them to provide causes of death when they do not feel able to do so.
Medical examiners provide advice to attending practitioners to help them formulate causes of death.
However there will be examples where, despite the absence of evidence that a death was unnatural, medical practitioners will not be able to confirm a cause of death with confidence to the best of their knowledge and belief.
If the principle that doctors must certify all deaths with natural causes is applied too extensively, there is a risk that important concerns – only identifiable through the information and evidence available at an inquest – could be missed.
Coroners, medical practitioners and medical examiners must therefore work together constructively, with mutual respect for their distinct roles, to support the interests of bereaved people and to maintain the integrity of the system.
Improving death certification and mortality data
Improvements in mortality and death certification data will become more apparent over time, though some benefits are already evident.
The number of deaths classified by ONS as uncertified or unknown fell from an annual rate of more than 10,000 per year before the death certification reforms to just 3 deaths in 2025.
These 3 deaths were uncertified or unknown because they were deaths of foreign service personnel, which were certified in the jurisdiction of origin.
In Wales, medical examiners improved the formulation of the cause of death in 39% of MCCDs sent to register offices.
We are currently working up a time-limited survey of medical examiner offices in England in 2026 to evaluate the impact of medical examiners on causes of death.
A new field for ethnicity was added to the MCCD as part of the reforms, to record self-declared information from the deceased’s health record.
By 30 June 2025, 454,958 deaths had been registered, and an average of 81.1% recorded ethnicity on the MCCD.
The proportion increased steadily after the statutory medical examiner system commenced, rising from 79.3% in September 2024 to 83.5% in June 2025.
Resources
The deterrence and detection of malign or negligent activity in healthcare are difficult to measure or quantify, though they are objectives of the medical examiner system.
While no system is perfect, medical examiners provide greater protection to prevent recurrence of harm arising from criminal intent or failures of probity.
The previous system of cremation forms provided significantly lower assurance levels, at a higher cost, and with fewer assurance measures for burials. The government decided to avoid levying new charges on the public for the work of medical examiners, and costs in England are met through the NHS mandate payment.
The workforce at medical examiner offices in 2025 is broadly in line with modelled expectations.
In Wales, the medical examiner system workforce comprised 12.8 whole time equivalent (WTE) medical examiners and 39.1 WTE medical examiner officers.
In England, there were 180.6 WTE medical examiners and 510.2 WTE medical examiner officers.
Comparing the position in England at 31 December 2025 with a year earlier, there has been a small increase in medical examiner officer WTEs and a 0.7% decline in the number of medical examiner WTEs in post (from 181.9 WTEs, noting that a data issue caused an error in the total medical examiner WTEs originally reported for 2024).
Regional medical examiners will continue to monitor workforce levels.
Overall, activity in all regions in England and Wales is within expected parameters. The workforce appears sufficient from a national and regional perspective. The Royal College of Pathologists trained an additional 197 medical examiners in 2025 (cumulative total 2,663), and an additional 113 staff attended medical examiner officer training (cumulative total 909).
Training ensures a pipeline of replacement medical examiners and officers to fill vacancies as they arise, but the reduced annual total of those trained compared to previous years reflects the maturity and stability of the workforce.
There can be particular challenges in replacing medical examiner officers, as this is a new discipline, and there is no pool of staff with direct experience of the role.
A minority of offices in England continued to experience higher numbers of deaths than expected, and others experience workforce pressures. Regional medical examiners have taken a number of actions to support such offices.
Ultimately, local NHS bodies are responsible for ensuring there are adequate resources (Health Boards and NWSSP in Wales, NHS trusts and ICBs in England).
A small number of ICBs and NHS trusts have increased the resources available to medical examiner offices, which is very welcome.
Other areas with high activity should also consider this, especially in the context of wider assurance and savings delivered by medical examiners, for example, through reduced referrals to coroners.
Working with regional medical examiners in England, colleagues in Wales and government departments – including the General Register Office and Ministry of Justice, which are responsible for the work of coroners and register offices – we will continue to monitor resources and impact on the objectives of the medical examiner system.
We will request support for areas where activity is above expectations or where processes appear to take longer. NHS trusts and ICBs should ensure the resources available to medical examiner offices are maintained and are appropriate.
Earlier this year, we assessed whether the introduction of medical examiners has increased pressures on NHS mortuaries in England.
No evidence of increased pressure was identified in the data available. On the contrary, the number of deceased people waiting more than 21 days in mortuaries had fallen over the past 2 years.
The number of bodies being held in NHS mortuaries for coroners also fell.
It is not possible to deduce a causal link between the introduction of medical examiners and the fall in the number of bodies being held for coroners.
However, the reduction is consistent with medical examiners helping to reduce unnecessary coroner referrals.
It is important to note that medical examiners do not control the release of the deceased from mortuaries, and there is no national guidance preventing the release of the deceased before medical examiner scrutiny and completion of MCCDs.
Future steps
Looking ahead, work is underway with the Department of Health and Social Care (DHSC), regional medical examiners and officers, Welsh Government and NWSSP to consolidate and develop the medical examiner system.
Along with DHSC, we will also continue to work closely with national partners, including the General Register Office, the Chief Coroner and the Ministry of Justice.
Broadly speaking, the areas of development for the medical examiner system are to:
- strengthen the voice of bereaved people and their ability to raise concerns
- achieve greater alignment and consistency in its various activities
- more clearly demonstrate impact
- make greater use of data and research to support learning and improve healthcare
We have started work with regional medical examiners to improve consistency in referrals for clinical governance reviews.
This remains complex, as clinical governance thresholds and criteria can differ between geographical areas and across primary, secondary and tertiary care.
DHSC has commissioned the University of Birmingham to conduct an evaluation of the death certification reforms.
The research team has started work with medical examiner offices and other stakeholders, and their findings will help identify lessons to further improve the support medical examiners provide to bereaved people.
We understand that ONS also plan to analyse the impact of the death certification reforms. It is important that this analysis reflects the original aims of the reforms, as outlined in the Context section.
If ONS further evaluate the time taken to register deaths, an analysis that considers each stage of the process would be particularly helpful rather than a simple analysis of the overall time taken.
This would include:
- the time attending practitioners take to complete MCCDs appropriately and send them to medical examiner offices
- medical examiner scrutiny and delays caused by attending practitioners formulating causes of death incorrectly and failing to provide health records or other information
- the impact of deaths referred back to attending practitioners by coroners
- the time taken by informants after MCCD completion to register the death
Appendix 1 – themes identified by medical examiners in 2025
England
AI-assisted analysis of narrative reports from medical examiner offices in England, each quarter in 2025, identified the following themes.
Clinical deterioration and missed opportunities:
- late or missed recognition of end‑of‑life
- failure to escalate deteriorating patients in a timely manner
- delayed senior or consultant review, especially at weekends and out of hours
- inadequate triage or delayed assessment in emergency departments
- long emergency department waits contributing to death (for example, exposure to infection and corridor care)
- patients left unmonitored for extended periods, including in overstretched acute wards
Delays in diagnosis, investigation, or treatment:
- delayed investigations (for example, imaging, biopsies, blood tests)
- missed or delayed cancer diagnoses
- delayed treatment escalation (for example, intravenous fluids, antibiotics, critical interventions)
- delays in reporting and acting on radiology results
- slow responses to abnormal results or clinical deterioration
Medication-related harms:
- missed or delayed administration of essential medications (for example, antibiotics or end-of-life medication)
- incorrect dosages or prescribing errors (for example, opiates in renal impairment)
- failure to administer routine medications on time (for example, Parkinson’s or cardiac medications)
- medication omissions contributing to hospital deterioration or death
- delays in reviewing high‑risk medications (for example, anticoagulation, insulin)
Poor basic care (hydration, nutrition, regular observation):
- inadequate hydration or nutrition monitoring
- poor escalation for worsening intake or dehydration
- failure to meet basic care needs (turning, toileting, feeding, oral care)
Pressure ulcers and wound care:
- development of pressure sores during admission
- incorrect grading or under‑reporting of pressure ulcers on discharge
- delayed wound assessment or follow‑up in community and care home patients
Unsafe discharge or failed discharge processes:
- premature discharge leading to avoidable readmissions and death within days
- discharge without adequate safety netting or end-of-life planning
- discharge of high‑risk patients without medications, equipment or community support
- severe pressure sores present at discharge, contradicting assessments
Care home and community clinical failures:
- failure to provide appropriate end‑of‑life care in nursing or care homes
- lack of regular GP review for care home residents
- failure of care staff to recognise deterioration
Accident and emergency services:
- pressures, including corridor care and ambulance delays, adversely affecting health and outcomes
- lack of communication between paramedics and GPs, resulting in missed clinical information
End-of-life care concerns:
- poor communication with families regarding prognosis and care decisions
- lack of do not attempt cardiopulmonary resuscitation (DNACPR) or Treatment Escalation Plan (TEP) discussions
- inappropriate treatment escalation in actively dying patients (for example, avoidable ICU or critical care referrals)
- delayed access to anticipatory medications in the community
Infection-related issues:
- hospital-acquired infections (for example, influenza, respiratory syncytial virus) in overcrowded emergency departments and wards
- failure to isolate infectious patients due to bed shortages
- missed or delayed sepsis screening and treatment
- infections linked to poor wound or ulcer management
Safeguarding and neglect indicators:
- concerns raised around care home neglect (for example, overmedication, poor hygiene)
- reports of unsafe living environments or inadequate home care support
- cases requiring referral to police or adult safeguarding teams
Wales
Medical examiners working for NWSSP identified the following themes for care providers through feedback using the HCQS framework.
Safe care:
- development of pressure areas (grade 3 or 4 deep tissue injuries or ungradable) while in a care setting
- falls without injury and injurious fall while in a care setting
- iatrogenic injuries pneumothorax following chest drain or central line, post-endoscopic retrograde cholangiopancreatography pancreatitis
- safeguarding or neglect of vulnerable patients
- omissions of care and treatment
- healthcare associated infections, including nosocomial covid
- transfusion incidents
- medication or prescribing errors
- hospital-acquired thrombosis without appropriate venous thromboembolism management
- Ionising Radiation (Medical Exposure) Regulations or radiation incidents ‘significant’ or ‘clinically significant’ accidental or unintended exposures
- inappropriate identification and management of a patient with sepsis
- inappropriate identification and management of hyperkalaemia and hypokalaemia
- inappropriate management of a patient with hypoglycaemia and hyperglycaemia
- issues with poor clinical record keeping and documentation
Timely care:
- delays in diagnosis related to clinical oversight and delayed reporting
- delays in treatment
- delays in escalation of a deteriorating patient
- delays in referral to appropriate services
- delays in assessment or triage
- delays in transfer or admission
- next of kin concerns regarding access to and provision of services
Effective care:
- precipitous readmission (readmission within a week for the same condition)
- delayed discharge
- apparent insufficient senior management of the patient
- concerns over inappropriate care at the end-of-life care (failure to recognise and palliate)
- right ward or speciality for the patient’s care (including concerns with outlier wards)
Efficient care:
- inappropriate requests of bloods and observations where the patient is near the end of life
- inappropriate and inefficient use of antibiotics and fluids
- inappropriate investigations or procedures
- inappropriate cardiopulmonary resuscitation
- absence of treatment escalation plan
- avoidable admissions or unsuitable place of treatment (that is emergency department corridor, ambulance bay)
Equitable care:
- inappropriate provision of appropriate mental health care
- inappropriate consideration of mental health assessments
- inappropriate language for the service user – availability of translation services
- age discrimination – where treatment is withheld based solely based on the age of the patient
- learning disabilities – diagnostic over shadowing and access to appropriate information
Person-centred care:
- lack of empathetic care
- lack of compassionate care
- lack advanced care planning and individual wishes including cpr planning
- family wishes or input not considered in patient management
- concerns regarding poor communication – verbal or written
- individualised treatment and care plan not followed
- concerns regarding dignity and respect after death
Publication reference: PRN02347