
Introduction
This guidance is both a statement of policy intent and a practical planning instruction for neighbourhood health centre (NHC) development in the current planning period. It:
- sets out the strategic framework for how ICBs and NHS England regions, working with providers, should identify and develop NHC schemes to support neighbourhood health: the archetypes to consider, estate planning, pipeline development and funding routes
- instructs ICBs and NHS England regions on the planning work now required to develop a coherent pipeline of NHC schemes
In doing so, it mirrors the principles of the broader capital framework of long-term planning certainty, transparent rules-based approaches, local leadership and a commitment to maximise the value of existing NHS and public estate.
Neighbourhood health is a central pillar of the government’s 10 Year Health Plan and represents one of the most significant shifts in the organisation of health and care services since the creation of integrated care systems. Its purpose is to improve access to general practice, bring care closer to home, reduce unnecessary reliance on hospitals, and support a fundamental shift from reactive treatment to prevention, proactive care and integrated multi-disciplinary working. NHCs are a key physical and operational tool to support the neighbourhood health model, alongside care delivered in people’s homes, digitally and in general practice, pharmacies and other community settings. They will be the place to go for most health needs in every community. This approach also reflects the government’s wider public service reform principles: shifting from reactive services to prevention, integrating services around people’s lives, and devolving power to local areas in partnership with communities and civil society.
This guidance should be read alongside the neighbourhood health framework, which sets out the wider delivery expectations for 2026/27 and beyond.
Spending Review 2025 and subsequent announcements
The 10 Year Health Plan sets a long-term ambition for NHCs to become the place to go for most health needs in every community.
As part of the Autumn Budget, the Government set out its plans in more detail – which confirmed it would deliver 250 NHCs by 2035, with 120 of those by 2030. These will comprise a mixture of upgrades to existing buildings and new build centres, with the balance between the two to be informed over time by local need, value for money and deliverability. New build schemes are expected to be funded through a combination of public capital and public private partnerships (PPPs), with around 20% funded through public capital and the remainder through PPP routes. A first wave of upgrade schemes for delivery in 2026/27 has already been identified and announced.
This investment in NHCs will support improved access to general practice, service transformation and a more strategic reshaping of the community and primary care estate and put us well on the way to our longer-term goal of a centre in every community supported by a combination of new capital investment, disposals and repurposed estate.
Neighbourhood health centre estate proposals
Planning for NHCs must align with the NHS Medium Term Planning Framework and emerging neighbourhood health implementation plans.
NHC estate proposals for upgrading, repurposing or building new centres should build on and be informed by the service changes ICBs are committing to deliver over 2026/27 and beyond in their planning submissions, including improved access to general practice, enhanced support for people with complex needs and the shift of appropriate activity out of acute settings. There should be a clear line of sight between neighbourhood health ambitions, clinical strategies, service redesign plans and the estate solutions proposed to enable them.
The NHC design specification published separately provides detailed guidance on the design, spatial requirements and operational layout of NHCs. It is intended to support greater consistency and efficiency in core components such as digital infrastructure, functional requirements and key design principles, while allowing local flexibility in service mix, use of space and partnership arrangements to reflect population need and local context. While primarily intended for new build centres, the specification should be considered when developing upgrade schemes.
The 10 Year Health Plan establishes a commitment to create a modern neighbourhood health service built around multidisciplinary working and seamless collaboration, including across general practice, community services, social care, mental health, diagnostics, wide LA and public services, and civil society. This model is designed to improve people’s access to services, reduce fragmentation and provide a single coherent offer at neighbourhood level, with professionals organised around population needs rather than organisational or contractual boundaries. This should include where appropriate stronger integration with adult social care and other local authority services as part of the wider neighbourhood health model.
NHCs should be planned as part of an asset-based neighbourhood model, connected to wider networks of support, health promotion and community activity, rather than as stand-alone clinical facilities. ICBs should engage with the community, as well as health and wellbeing boards, local authorities, civil society and other partners, to ensure that these spaces meet the needs of local people. This might mean working with the community to design multi-use spaces that work for them or consulting local people on decisions about the location of a new health centre. Where a neighbourhood has received Pride in Place Programme funding, this might mean involving the neighbourhood board in the design and use of public spaces in NHCs.
Neighbourhood health is not limited to a building; it is an operating model. However, without suitable estate many areas will be unable to deliver the integrated teams, the convenient access to co-located services, the urgent neighbourhood services, and the ‘home first’ rehabilitation models envisaged by the 10 Year Health Plan and national neighbourhood guidelines. Estates planning is therefore both a prerequisite and an accelerant for neighbourhood transformation.
What is a neighbourhood health centre?
NHCs bring together GP practices and a mix of community, local authority, adult social care and civil society services, allowing staff to deliver more co-ordinated and effective care for better patient outcomes and experiences.
Centres will be expected to:
- meet the expectation set out in the 10 Year Health Plan to be open at least 12 hours a day and 6 days a week providing access to coordinated services locally
- include on-site general practice as a core element of the model, not solely GP staff or sessional input
As part of developing the neighbourhood health plan, health and wellbeing boards will be agreeing the geography (‘a neighbourhood’) around which services should be delivered. ICBs and regions should align their proposals with this work, and plan for NHCs to serve a population footprint at a scale in line with the Neighbourhood Health Framework (around 50,000, recognising the need for local flexibility), with General Practice at the core. We would generally expect GP services within an NHC to be operating at the scale of a PCN. We recognise of course that other types of services will operate best on different footprints. For example, Minor Diagnostics and UTCs are likely to operate better on a larger footprint, whilst Integrated Neighbourhood Teams, e.g. for frailty, will need to be operating at a neighbourhood level in most places. Proposals should show how the Centre improves integration, access and the range of neighbourhood services available locally, and should improve reasonable patient access to core services.
The infographic below outlines the core components expected in an NHC, with the shaded boxes identifying the minimum requirements for designation as an NHC. The specification explains and describes these more fully.
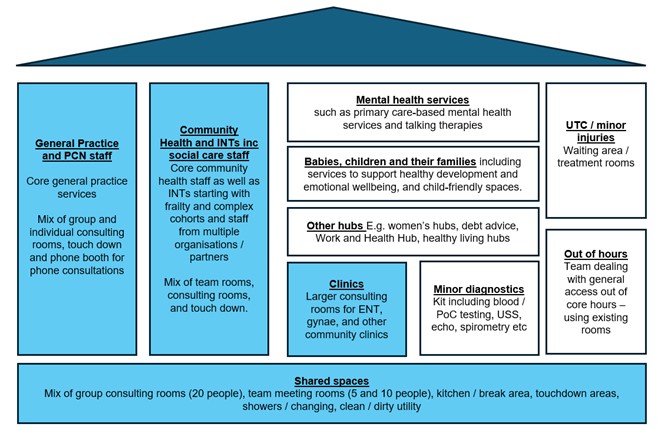
The image is a diagram showing the core components of a neighbourhood health centre, presented as a building layout. The layout is divided into coloured sections that represent different services delivered under one roof, supported by shared facilities.
On the left, a large light‑blue section represents General Practice and Primary Care Network staff, providing core general practice services. This area includes a mix of group and individual consulting rooms, touchdown spaces, and phone booths for telephone consultations.
Next to this is another large light‑blue section for Community Health and Intermediate Care Teams, supporting social care staff, NHS staff, voluntary sector organisations, and partners. This space is designed for staff working with frailty and complex cohorts and includes team rooms, consulting rooms, and touchdown areas.
The central white section highlights a range of clinical and support services, including:
- mental health services, such as primary care‑based support and talking therapies
- services for babies, children and families, including support for healthy development and emotional wellbeing in child‑friendly spaces
- other hubs, for example NHS debt advice, Work and Health Hubs, and healthy living hubs
To the right are additional clinical services, including:
- urgent Treatment Centre (UTC) or minor injuries, with waiting areas and treatment rooms
- out‑of‑hours services dealing with general access outside core hours using existing rooms
Below the central block are two clinical areas:
- clinics, providing larger consulting rooms for ENT, gynaecology, and other community clinics
- minor diagnostics, offering blood point‑of‑care testing, ultrasound scanning, echocardiography, and spirometry
At the bottom of the diagram, a long shared blue bar represents Shared Spaces, including group consulting rooms for up to 20 people, meeting rooms for 5–10 people, kitchen and break areas, touchdown workspaces, showers and changing facilities, and clean and dirty utility rooms.
Blue boxes represent the minimum requirements for designation as an NHC. As a minimum, this includes an on-site GP practice and a model capable of operating at scale over time.
These minimum requirements are intended to establish a consistent national threshold for designation, while the precise mix of complementary services, including diagnostics and other hospital-to-community functions, will vary by place according to local need and the wider service model.
Mental health provision within NHCs focuses on primary care‑led and early intervention support, closely integrated with GP services. This is distinct from secondary care mental health services (including community mental health centres where they exist). Community-based mental health centres complement, rather than replace, NHCs and the person’s named GP, ensuring continuity of care and coordinated support across neighbourhood teams.
Neighbourhood health estate archetypes
The optimal approach to delivering the right estate to support neighbourhood health in a local area will depend on the needs of the local population, existing service configuration and how that configuration needs to change, as well as the estate currently available. In many areas, it will not be necessary nor represent good value to create wholly new centres. To illustrate the range of approaches NHS organisations can consider, NHS England has identified 4 archetypes for the neighbourhood health estate.
Archetype 1: Hub-and-spoke and upgrading, repurposing or extending existing NHS estate
Upgrading or reconfiguring existing GP, community or other NHS buildings, often complemented by ‘spokes’ such as mobile units or small satellite sites. This is typically the quickest and most affordable route to creating an NHC and is appropriate where there is high-quality existing estate that can be extended to provide the right neighbourhood health service offer.
Archetype 2: Repurposing community or civic spaces
Across the NHS, local government, the wider public sector and civil society, there is already substantial estate that can be used to host neighbourhood health services. Some high street premises, libraries, leisure centres or other civic assets may be suitable for adaptation to host neighbourhood health services. This brings care closer to people’s homes and can be delivered at pace and comparatively low cost. These facilities often will not be able to provide the full range of services expected from a NHC, but they can form a valuable part of the local offer.
Archetype 3: Cohort-specific hubs
Existing hubs that provide health or care services in the local community for particular groups, such as women’s health hubs, Best Start Family Hubs for children and young people, community based mental health centres or respiratory hubs can be integrated into the wider neighbourhood health offer. These hubs will not always be physically located within an NHC, but should complement, align with and, where it makes sense locally, be co-located or consolidated with NHCs.
Archetype 4: Purpose-built neighbourhood health centres
New-build centres designed specifically for co-located services and multidisciplinary teams (see the NHC design specification for the detail). These will be delivered through a mix of public capital and a new PPP model in areas where current estate cannot readily be repurposed to deliver convenient access for patients to the full range of neighbourhood health services.
These archetypes are not prescribed templates. However, ICBs and regions should consider them in a pragmatic but ambitious way when developing their pipeline of neighbourhood health schemes. They should identify the model or combination of models best suited to each neighbourhood, based on population health needs, existing assets and local service configuration. In doing so, they should seek to develop an estate that supports the full vision for neighbourhood health, maximising opportunities to improve utilisation, exit substandard or no longer fit-for-purpose buildings, and create higher quality facilities in the right locations. We expect ICBs to be able to draw heavily on their existing estates strategies, as well as the work done since last summer in preparation for and as part of medium-term planning.
Digital integration and infrastructure
Digital capability is fundamental to the functioning of neighbourhood health services. NHCs must therefore be planned as digitally enabled facilities, in line with the approach set out in the NHC design specification. Costings for proposed schemes should reflect this.
As part of their planning, ICBs and regions should consider the interaction between physical estate and digital transformation, including the potential to reduce space requirements through modern general practice models, and the need for all clinical and administrative staff working in neighbourhood models to access shared digital systems across organisational boundaries whilst maintaining digital and physical security.
Existing estate, partnerships and other considerations
Existing estate and scale of opportunity
Across the NHS, local government, wider public sector and civil society, there is already substantial estate that can support the development of NHCs. Work with Community Health Partnerships (CHP) and NHS Property Services (NHSPS) suggests that many buildings could already function as NHCs or could do so with modest investment. Community hospitals, local authority facilities, One Public Estate sites and primary care buildings all offer opportunities to bring services together and create a more joined-up local offer. Furthermore, other initiatives such as local Get Britain Working plans and associated partnerships can support agreements around shared estates.
The availability, suitability and scale of existing estate varies significantly between ICBs and neighbourhoods. This variability is expected; NHCs are defined by their function in supporting integrated neighbourhood services, not by ownership of a specific NHS building. ICBs should therefore take a broad and pragmatic view of suitable estate, including all public, community and other civic assets, where these align better with neighbourhood geographies and service models.
Systems should take account of planned population and housing growth when developing NHC plans, so that future estate capacity keeps pace with changes in demand. ICBs and regions should work with local authorities to align neighbourhood health estate planning with local development plans and regeneration activity, for example as part of the Pride in Place Programme, including securing developer contributions such as Section 106, where appropriate, to support the delivery of neighbourhood health centre schemes.
Where new build centres are proposed, locations in or close to existing community focal points, including town and local centres and high streets, should normally be preferred where they support accessibility, integration and wider regeneration objectives. Locating a new neighbourhood health centre away from an existing community focal point should be undertaken with caution and will need to be justified clearly (for example, where there is a clear commitment from the local authority and housing developers to deliver significant future housing growth). Evidence from local authorities and STRATA (previously SHAPE) may be used to support this assessment.
The challenge is as much about consolidating and better using existing estate as extending or creating new facilities. Across the country, there are over three million square metres of primary care and community care estate. Some of it predates the founding of the NHS and is not best suited for providing modern patient care – and needs to be decommissioned and disposed of. However, some of it has the potential to provide the additional capacity needed for neighbourhood health services through improved utilisation (supported by digital pathways, redesigned workflows, reconfiguration and relocation of services, and extended opening).
Partnership, co-location and anchor institutions
Effective partnership working is fundamental to the NHC model. Providing a range of services in a single, trusted location improves access for residents and supports real-time collaboration between professionals. Proposals should demonstrate how local partners, communities and relevant civil society organisations have informed the development of the scheme, particularly in relation to location and the wider service offer.
Centres should bring together NHS, local authority, and civil society services to provide a coordinated, population-focused offer. In doing so, due regard should be given to the Civil Society Covenant principles of partnership, working throughout the planning, decision-making and operational service delivery of NHCs. Clear partnership arrangements, including robust information governance and data-sharing agreements, are essential to enabling seamless multidisciplinary working.
Through their NHC proposals, ICBs should consider co-locating or aligning the following with NHS services, where this represents the best local solution:
- adult social care
- social welfare advice (for issues including housing, family breakdown, employment, welfare benefits, debt, domestic violence and immigration)
- mental health and substance misuse services
- carers’ support
- integrated health and employment support services
- community-led activity
- services for babies, children and their families and other place-based services such as women’s health hubs
Local partners should also consider broader opportunities for co-location that align with initiatives such as community sport, physical activity and leisure provision, which have significant potential to drive shared goals around health and wellbeing.
Areas should take a pragmatic approach to rationalising overlapping hubs and services where this would create a clearer and more joined-up local offer. The Best Start Family Hubs and Healthy Babies: guidance for local authorities emphasises that local authorities should build a coherent network of Best Start Family Hubs and network sites and identifies NHCs as examples of potential network sites.
NHCs should also be viewed as anchor institutions: stable civic assets that contribute to wider social and economic development. By repurposing underused buildings and increasing local footfall, centres can support regeneration and strengthen community resilience, while addressing the wider determinants of health.
For these reasons, ICBs must work closely with a range of local partners in developing their neighbourhood health plans, including the estates elements. Partners may include, MPs, the local authority, mayors and strategic authorities, civil society, leisure providers, and the local Active Partnership.
Relationship with the new system architecture
NHCs will need to operate coherently within the wider neighbourhood health architecture set out in the 10 Year Health Plan and neighbourhood health framework, including the neighbourhood health plans developed by health and wellbeing boards. Over time, this may include alignment with emerging contractual and delivery models such as new single neighbourhood providers, multi-neighbourhood providers and, in some areas, integrated health organisations. These models remain subject to further national development and consultation, and this guidance should not be read as prescribing a single delivery form.
Estate should be capable of supporting population-based neighbourhood models, including multidisciplinary working, co-location, shared use of space and, where relevant, shared clinical, diagnostic or support infrastructure across neighbourhoods, whilst being able to preserve the data and physical security necessary to delivering clinical services.
The development of NHCs is not an end in itself. NHCs are one feature of the new model of care set out in the 10 Year Health plan, which is designed to deliver more proactive, preventative and personalised care for people through a left shift in activity and resources, improved access to General Practice, reduced pressure on hospitals, and enhanced digital and physical access to services locally. For each proposed NHC, the ICB will be expected to demonstrate how the chosen site fits within this and forms part of a coherent clinical strategy.
Programme pipeline and funding
This guidance is intended to support ICBs and regions to work in partnership to develop their full pipeline of schemes, covering both upgrades and new builds. While the national pipeline of schemes may be announced in waves, planning should consider the full future pipeline required across the footprint.
Regions will play a central role in shaping a coherent pipeline across their geographies, working with ICBs and providers to develop their overall estates strategy and individual schemes and ensuring that proposals (refurbishment or new build) are realistic, strategically aligned and deliverable within available funding envelopes.
Upgrades: refurbishment, repurposing and extension of existing estate
Evidence from national estates work indicates that a significant number of NHCs can be delivered through relatively modest investment in upgrading, refurbishment, repurposing, reconfiguration and extension of existing estate across the NHS and public sector: unlocking improved utilisation, co-location and service integration without the time, cost and risk associated with wholly new development.
ICBs and regions should therefore consider upgrades to existing estate where these can support the required neighbourhood service model. This includes upgrading primary care and community buildings, adapting civic or shared spaces, extending existing facilities where appropriate, and improving utilisation through extended hours, digital pathways and redesigned workflows. Where suitable estate exists, upgrading, repurposing or extending existing estate should generally be the preferred approach when it offers a better value for money solution than new build. Proposals should align with the overall criteria for funding NHC schemes set out later in this document, including the expectation that ICBs demonstrate intelligent use of existing estate before proposing new build solutions.
Where multiple small upgrades could be combined into a more strategic scheme (for example converting a community hospital into a major neighbourhood hub) regions should support ICBs to take that broader approach.
Refurbishment schemes will need to be funded through public capital routes – through existing regional capital allocations for constitutional standards and left shift and through additional funding being made available specifically for NHCs.
New builds
ICBs and regions may conclude that building a new centre is the most appropriate option – where there is no existing estate in the right location to serve the population of a NHC, where existing buildings are of low quality or poorly configured, or where the creation of a new centre would better enable the service reorganisation needed to deliver the vision. New build proposals should be brought forward where they represent the strongest overall case in terms of local need, service fit, affordability and value for money, rather than to meet a pre-determined delivery route.
We expect 80% of new builds to be delivered through PPP and 20% through public capital. Decisions on which delivery route will be used for which schemes will be taken centrally. ICBs should develop and propose robust schemes that are suitable for either route.
ICBs need to consider long-term affordability and revenue implications when developing any new build proposals (including PPP). This includes consideration of unitary charges over the life of a scheme. In a PPP arrangement, the unitary charge is the payment made to the private partner and typically covers the capital cost of the facility, hard facilities management, lifecycle maintenance and associated funding costs. ICBs should also consider the treatment of soft facilities management costs, together with wider building and site management arrangements. All proposals will need to demonstrate a credible affordability position and value for money case.
Public private partnership model
The government has confirmed that a new publicly led public private partnership (PPP) model will form part of the delivery approach for some new build schemes, alongside schemes delivered through public capital. The purpose of this new PPP model is to support the timely delivery of high-quality, purpose-built NHC infrastructure by harnessing private sector capability to deliver schemes to time and to cost. In doing so, the model is intended to enable the NHS and its partners to focus on service transformation, integration and the delivery of improved outcomes for patients. The PPP model will be suitable only for new build schemes. The PPP model is not intended to displace stronger refurbishment or repurposing options where those better meet local need and offer better value for money. National decisions on scheme progression and delivery route will therefore need to balance local value for money, affordability and strategic fit with the need to maintain a credible and deliverable pipeline of PPP-suitable schemes.
The new PPP model is being developed by the National Infrastructure and Service Transformation Authority, supported by the Department of Health and Social Care (DHSC), and will build on lessons learnt from past and current models and harness private sector expertise to deliver the new NHCs. Areas of consideration include but are not limited to: changes to the payment mechanism, improvements to the variations protocol and enhanced monitoring provisions. To ensure the Neighbourhood Health Centre PPPs are managed transparently and are fiscally sustainable, these projects will be budgeted for as though they are on balance sheet. In addition, by delivering NHCs through a combination of private and public investment the government will be able to build further evidence and compare different models of delivery.
We expect PPP schemes to be procured in batches of 5 to 10 projects, rather than as individual schemes, which is one of the reasons we need a clear early understanding of the future pipeline of new build projects within an area over time. This means early pipeline development will need to identify not only individual suitable schemes, but also a coherent forward pipeline of proposals that could support batching where appropriate.
All new build proposals will need to demonstrate value for money, strategic fit, deliverability, affordability and maturity in order to progress. At this stage, a new build scheme’s inclusion in the pipeline will not in itself imply a funding commitment, as that will be subject to business case approval.
Indicative capital planning approach for the pipeline
DHSC and NHS England will discuss with regions the indicative position re the level of funding available for upgrade schemes and the broad numbers of new builds we anticipate supporting. Regions will then work with ICBs to guide the number and scale proposals to be developed across their geography, informed by neighbourhood health planning and local estates strategies.
Planning requirements to 28 May 2026
Between now and 28 May, regions should complete their work with ICBs to develop a proposed strategic NHC pipeline for each ICB. This should set out the ICB’s latest view of how neighbourhood health centres will be organised across its footprint to deliver effective clinical strategies, the places in which capital investment is likely to be prioritised, and the mix of upgrades and new builds it proposes to deliver over time.
Working with their ICBs, regions must develop early-stage, site-specific proposals that identify location, population served, service model, estate option (refurbishment, extension or new build), site constraints, planning considerations, digital requirements and indicative capital needs, and how local partners and communities have informed the proposal.
This planning exercise is intended to produce a clear, structured articulation of proposed schemes and to test these against the national criteria set out in this guidance. Schemes may continue to be refined or amended after submission as planning develops and further assurance is undertaken. It is not expected that all schemes will be fully worked up by the time of submission, but sufficient detail will be needed to enable regional and national review, challenge and prioritisation.
By 28 May 2026, regions working with ICBs should set out:
- the latest thinking on how they will define neighbourhoods geographically in their area.
- a clear articulation of proposed neighbourhood health estate, listing existing facilities and the upgrade and new build schemes proposed.
- for upgrade and new build schemes, information about how these proposals align to the criteria against which schemes will be assessed.
- a list of disposals that will be enabled through investment and improved utilisation.
This information should be provided in the single template that NHS England will provide and should build on existing ICS estates strategies and medium-term capital planning work.
Local Improvement Finance Trust estate considerations
Some ICBs will have Local Improvement Finance Trust (LIFT) buildings reaching contractual expiry over the coming years. In developing neighbourhood health plans and NHC proposals, ICBs should explicitly consider the status and future role of any LIFT estate within their area. This includes clearly setting out assumptions on whether existing LIFT facilities are expected to be retained, upgraded, repurposed, replaced, or exited, and how this informs the overall neighbourhood estate strategy.
Where LIFT buildings are expected to continue to play a role in neighbourhood health delivery, proposals should set out how they will be adapted to support neighbourhood models of care and represent value for money. Where LIFT buildings are not assumed to be retained, ICBs should reflect this in their assessment of future estate need and investment requirements.
Regional oversight and national support
Regions have a strengthened role in estates planning under the new operating model and they will lead the planning exercise with ICBs across their geographies.
Regions should ensure that each ICB develops a coherent strategic view of its neighbourhood estate model, aligned to a clear clinical strategy, the places where capital investment is likely to be prioritised to deliver the most value and the pipeline of schemes required to support delivery over time.
Regions should test the extent to which proposed schemes are aligned with the NHC definition and delivering the aims set out in the Neighbourhood Health Framework, the planning requirements in this guidance, and the criteria and metrics against which proposals will be assessed. Regions should challenge areas where proposals are insufficiently developed, inconsistent with neighbourhood health objectives, or do not yet demonstrate a credible case for investment.
National teams will provide technical guidance and template materials to support planning, including a standard submission template. National oversight will support consistency, value for money and a credible national pipeline, while giving local areas flexibility to determine the service model and configuration best suited to their needs.
Scheme approval process
Criteria for funding NHC schemes
NHC scheme funding will prioritise proposals that best support the delivery of neighbourhood health at scale, demonstrate value for money, and can be delivered within the relevant planning and spending periods.
ICB funding prioritisation and national assurance will be guided by 7 criteria:
- Strategic alignment with neighbourhood health objectives – For each proposed NHC, the ICB will be expected to demonstrate how the chosen site forms part of a coherent clinical strategy. Proposals should clearly support the shift toward a neighbourhood health service articulated in the Neighbourhood Health Framework, including prevention, proactive care and delivery closer to home. Schemes should demonstrate how the NHC scheme enables service integration, supports neighbourhood multidisciplinary teams, strengthens integration with relevant non-health services, and helps reduce pressure on acute services. Where possible, schemes should demonstrate alignment with relevant health and wellbeing boards’ work to develop neighbourhood health plans. Proposals will need to demonstrate a link to population need, noting the 10 Year Health Plan commitment to “‘begin establishing NHCs in the places where healthy life expectancy is lowest”. The Wave 1 sites announced in March 2026 were prioritised according to deprivation (among other criteria) and this should continue to be taken into account in future waves.
- Coherence between neighbourhood service model, GP provision and physical estate – The proposed estate solution must be driven by a neighbourhood service model that is anchored around general practice. Schemes should include, as a core component, general practice services operating at scale (generally the scale of a PCN but with some scope for local flexibility where there is a strong rationale). They should enable joined-up delivery across primary care, community services, mental health, local authority and civil society where appropriate, and deliver the expected opening hours. Proposals will be viewed more favourably if they demonstrate coherent co-location with, or rationalisation of, other place-based services while improving the overall offer for local people.
- Intelligent strategic estates planning – Opportunities to reuse, repurpose or upgrade existing estate should be fully explored before proposing new-build solutions. New-build schemes should be justified on the basis of estate quality, backlog maintenance, fitness for purpose, location and value for money. Investment in additional space, through upgrades, new builds and improved utilisation, should be leveraged to enable the disposal of estate that is in poor condition or no longer required.
- Deliverability and pipeline readiness – Proposals should be deliverable within the timeframe proposed by the ICB. This includes clarity on site availability, planning position, stakeholder alignment, and a realistic delivery timetable.
- Financial sustainability and revenue affordability – Proposals must demonstrate clear revenue (RDEL) affordability, including how running costs will be met within existing or agreed funding flows. This includes consideration of workforce, unitary charges, occupancy, utilisation, and the long-term financial implications of the estate solution.
- Governance, leadership and partnership maturity – Governance arrangements should be clear and robust, with strong clinical and system leadership and effective partnership working across NHS, local authority and wider civil society partners. Proposals should demonstrate readiness to operate the NHC as a shared system asset rather than a single organisation facility but also set out clearly which organisation will be accountable for delivery of the scheme and full utilisation of the NHC.
- Local strategic alignment – Proposals are expected to be locally generated, drawing on the expertise and insight of providers, general practice and other partners, including local authorities. Proposals should demonstrate early engagement with relevant stakeholders, such as local authorities, MPs, and civil society, and provide evidence that services, estates and local integration plans are aligned and take account of wider plans for local infrastructure investment as well as wider public estate development opportunities. Where relevant,ICBs should consider local regeneration plans and highlight how facilities will form anchor institutions in their communities. New build schemes should demonstrate that they are in locations accessible to residents and that attract footfall to high streets and town centres.
In assessing proposals against the criteria set out above, regions and national teams will use a common set of strategic and scheme-level metrics and tests. NHS England will use these to support a broadly consistent national approach to data collection, monitoring and impact assessment across the programme, while recognising that some additional local metrics may also be needed to reflect different service models and population needs.
ICB wide planning metrics include the:
- current utilisation of the community and primary care estate and how utilisation will improve through investment
- square metres used for neighbourhood health per the proposed population size
- number and size of disposals enabled through the proposed estate model
- number and size of poor-quality GP estate that could be exited over time through the proposed pipeline
Scheme-level metrics will include the:
- left-shift benefits enabled by the scheme
- proportion of relevant providers signed up to the proposed utilisation model
- scale of GP practice provision
- cost per square metre
- indicative RDEL affordability case, particularly for new build proposals
Planning and business case approvals
The approvals process for NHC schemes will mirror other national approaches (as detailed in the 2026/27 to 2029/30 capital guidance), ensuring consistency, pace and value for money, while being as streamlined as possible. The process is designed to focus national assurance on strategic fit, affordability and deliverability.
The first stage will be consideration of ICBs’ proposed schemes for outline approval based on the information provided in the planning templates being shared separately. We aim to hold approval panels from early June so that we have an agreed pipeline of schemes during summer 2026. ICBs and/or providers will then need to develop more detailed business cases in order to secure funding and/or inclusion in the PPP programme. Both stages of approval will be taken through the Neighbourhood Estates Investment Committee, a new, nationally convened panel that will provide assurance in line with HM Treasury Green Book principles. Where needed, support will be provided to help new-build schemes progress their business cases once they have received first stage approval.
Planning and submission
Planning for NHC provision should align with place-based planning arrangements, including health and wellbeing boards, where NHS, local authority and voluntary, community and social enterprise (VCSE) partners agree priorities for prevention, left shift and asset use. Local authorities should also be engaged early to ensure that public transport and, in particular, parking provision are considered up front as part of the planning of schemes.
Publication reference: PRN02463