
1. Overview
1.1 About this engagement report
This report reflects on the consultation and engagement carried out by NHS England during 2022/23 to inform the development of the equality objectives and targets for 2023/24 and 2024/25. This report only details the insight and feedback obtained through the consultation and engagement process. Information about how this insight and feedback has informed the development of NHS England’s equality objectives is provided in our Future objectives report.
Some of the feedback fell outside the scope of the Public Sector Equality Duty (PSED), the SEDs and the publication of equality objectives and equality information. Consideration was therefore given on how NHS England might address the wider feedback. We have made a record of it (see the annexes) and passed it on, or identified how best to pass it on during 2023/24, to the most appropriate team(s) within NHS England.
1.2 Building on the report to the Board in May 2022
In May 2022, we set out our proposals for future consultation and engagement, which included the following considerations:
- to review the proposed equality objectives to ensure they are fit for the new system landscape
- to explore options for stakeholders to develop and co-design targets for 2023/24 and beyond
- to establish a sustainable and proportionate review framework because equality objectives need to be reviewed at least every four years.
In July 2022, the extent of the transformation programme for the new NHS England became clear (see Review Report, section 1). As a result, it was decided that a wide external consultation was not appropriate during 2022/23 but instead a more focused approach to engagement should be pursued. Our engagement processes also continued to be online and primarily via MS Teams because of the ongoing impact of COVID-19.
1.3 Who we engaged
We carried out focused engagement using NHS England’s established patient forums and our central equality networks. We held online meetings with members of these patient, carer and community groups:
- NHS Citizen Advisory Group
- Learning Disability and Autism Forum
- LGBTQ+ Sounding Board
- Older People Sounding Board
- The Voluntary, Community and Social Enterprise Health and Wellbeing Alliance (VCSE HWA)
- Youth Board
- Youth Advisory Group
We also held meetings with:
- The Healthcare Inequalities Improvement Forum
- The NHS England Engagement and Equality Champions
We also reached out to the members of the NHS Equality and Diversity Council.
Following these engagement meetings, we sent a short online questionnaire to the members of the FutureNHS Equality and Health Inequalities Network (EHIN), combining some multiple-choice questions with the opportunity to provide free text comments. The EHIN is primarily made up of NHS staff with an interest in equalities and health inequalities issues and people from patient and community groups who have signed up as members of EHIN. We also sent the questionnaire to the Healthcare Inequalities Improvement Forum, the NHS England Engagement and Equality Champions, the VCSE HWA and the NHS Citizen Advisory Group. We received 101 responses and the analysis of the feedback is in Annex B.
2. Key themes from the engagement
2.1 Collating and analysing the feedback
The qualitative input provided a range of useful insights. We wish to express our thanks for the input. There were some recurrent issues and themes and these fall within 5 key headings: capability, training and understanding; inclusive language and communication; representation and leadership; issues not clearly covered by the equality objectives and targets; and improving future engagement.
We have considered how to address these themes as part of developing the next round of equality objectives and targets for 2023/24 and 2024/25. Primarily this information was used to inform the discussions with current and potential target leads (see Section 2.2 below). We are also exploring what else can be done with the information. The detailed feedback and themes relevant to each equality objective and the associated targets are set out in Annex A. These have also been considered and summarised in the Future Objectives Report for 2023/24 and 2024/25. Annex B provides an analysis of the EHIN questionnaire. Annex C summarises key feedback from each forum.
2.2 Common themes raised
The individual engagement forums and questionnaire responses provided a range of useful insights and identified some recurrent issues and themes.
Capability, training and understanding
Some of the key themes were the related issues of capability, training and understanding within NHS organisations, and staff members’ understanding of the issues faced by groups and individuals sharing particular protected characteristics. This was summed up as “cultural competency”, with concerns expressed about how well NHS professionals understood the lived experience of particular groups and the ability of staff and managers to hear, see and identify discrimination. There were a number of questions and insights about how [equality] training is delivered and about its quality and effectiveness.
Questions also related to how NHS England and NHS organisations analyse the quality and effectiveness of staff training. For example, is there 100% uptake of mandatory training across organisations and if not, why not.
Inclusive language and communication
Another repeated theme was inclusive language. It was pointed out that poor use of language sends a message that the NHS doesn’t really care about particular groups and communities. Most forums raised questions about the accessibility of NHS communications, particularly questioning how consistently and well organisations are implementing the Accessible Information Standard. Some also identified challenges for particular groups such as individuals with hearing loss, or where digital information isn’t sufficiently accessible.
Representation and leadership
Several of the groups underlined the importance of having the NHS workforce and the NHS leadership reflect the diversity of the communities served. This was partly summarised by the comment that “people from any protected characteristic would feel more valued if staff were more diverse”.
Issues not clearly covered by the equality objectives and targets
The consultation and engagement process sought to identify communities and groups who have crucial equality issues which were not sufficiently addressed by the existing equality objectives and targets. A number of responses identified that the Gypsy, Roma and Traveller community faced particular challenges (though precise issues weren’t identified). Some responses raised the challenges faced by the trans community. It is worth noting that a number of responses identified groups/issues that sit outside the Equality Act 2010’s protected characteristics. For example, socioeconomic deprivation or geographic variation do fit within the framework provided by the health inequalities duty but stand outside of the Equality Act 2010’s protected characteristics.
Improving future engagement
We heard that we need to improve future engagement to enhance links and insight from seldom-heard-from groups. The feedback stressed the importance of working with and through community and VCSE organisations as ‘trusted partners’ especially for less-well engaged groups.
Annex A: Grouping responses and existing objectives and targets
The issues, within scope of the PSED/SEDs, that came out of the meetings with engagement forums and the EHIN questionnaire informed discussions with equality target leads within NHS England. In this annex, we list the central issues by equality objective and target area. The letter Q identifies how the issue raised has been translated into a question(s) to be explored by NHS England.
A1 Internal and external workforce
EO2 T1 – 2 (Capability); EO4 T1-4 (Internal workforce) EO6 T1-4 (System workforce)
- For the NHS England workforce, EO4 T3 (Recruitment Change) and
EO4 T4 (Equality Diversity and Inclusion [EDI] strategy) were two of the highest rated targets from questionnaire respondents - For the wider NHS workforce, EO6 T1 (staff in senior roles) was one of the most popular targets for questionnaire respondents
Capability, training and understanding
- A number of comments were raised about staff capability/training on equalities issues and awareness of the protected characteristics. Some questionnaire responses identified concerns about “cultural competency” in the workplace questioning the ability of colleagues/managers to hear, see and identify discrimination.
Q: Would this be covered by the NHS EDI Improvement Plan? - One questionnaire response said greater priority should be afforded to the updated Equality Objective 2 which begins to consider how PSED, SED and new statutory health inequalities duties overlap and interlink.
- The need to properly and consistently challenge bias among staff with respect to both colleagues and patients was raised.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s workforce EDI plan?
- Specific concerns were raised about the poor understanding by NHS staff of learning disability and autism.
Q: Would this be covered by the NHS EDI Improvement Plan and the new Oliver McGowan mandatory training? - Specific concerns were raised about the levels of understanding by frontline medical professionals of various equalities groups. Poor understanding of trans people was raised as a particular issue.
Q: Would this be covered by the NHS EDI Improvement Plan? - Concerns were expressed about the quality, effectiveness and impact of inclusivity training across NHS England and other NHS organisations. Respondents asked what action is being taken to make the training more effective than the “usual mandatory training”.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s workforce EDI plan? - A number of responses from the engagement forums and questionnaire respondents questioned staff capability/training on equalities issues.This was echoed in one questionnaire response on the need “to ensure NHS staff especially GPs are aware of the protected groups and their characteristics“.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s own workforce EDI plan?
Support in employment
- It was noted that people with a learning disability, autistic people, and people from with any “protected characteristic” would feel more valued if staff were more diverse including more people with a learning disability and autistic people.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by the NHS England’s internal workforce EDI plan?
A: Work under equality objective 6 and target 5 is explicitly intended to increase the number of people with a learning disability and autistic people in the NHS workforce in England.
- Concerns were raised about the levels of post-employment support for people with the NHS workforce. There was an ask for action to be taken to ensure that all staff are treated well and valued across the protected characteristics.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s workforce EDI plan?
- Comments were made about the importance of having diverse NHS leadership teams to deliver equality goals. One response noted “A lot of people when they see themselves represented are more inclined to work towards shared equality goals.”
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s workforce EDI plan?
- Specific concerns were identified around age in relation to employment issues for both younger and older people in the workforce. The Youth Board suggested there should be more routes into employment for younger people.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by the NHS England’s workforce EDI plan?
- Concerns were raised about how extensive the NHS Electronic Staff Record system is recording employment data by reference to protected characteristics. There was a specific question about recording trans status on ESR.
A: Work is ongoing within a broader equality monitoring programme being led by NHS England on behalf of the Department of Health and Social Care (DHSC) (see Equality Objective 3).
- One response suggested that schools in deprived areas should be provided with employment information on opportunities for careers in the NHS.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by the NHS England’s workforce EDI plan?
- One response noted that current workforce EDI activity seemed quite restricted to a few areas of work-life eg recruitment practices. However, the response suggested there are important issues beyond recruitment.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s workforce EDI plan?
Representation and particular groups
- Concerns were noted about the low number of disabled staff in the workplace (compared to those declaring a disability in the general population). Concerns were also raised about what could be done to improve declaration rates (through a safer working culture). Some noted that “this protected characteristic often gets the least attention”. A further comment identified the need for support for disabled staff through the NHS England merger processes.
Q: Would this be covered by the NHS England workforce EDI plan and associated monitoring? In terms of the internal agenda, would this be covered by NHS England’s own workforce EDI plan? Would this be covered by the NHS England merger process in some way? - The question was asked whether there were overall targets to improve the 6% of people with a learning disability known to local authority social service and currently in paid employment.
Q: Is this an issue for the wider NHS EDI Improvement Plan? Would this be covered by the NHS England workforce EDI plan and associated monitoring?
A: The NHS Learning Disability Employment Programme is designed to improve employment opportunities and the number of people with a learning disability and the number of autistic people employed within the NHS in England (see Equality Objective 6 and Target 5).
- One response identified Islamophobia as an issue in the workplace and suggested that there was an under representation of Muslim males in administration roles over Band 7 (not clear which organisation(s) this referred to).
Q: What do the ESR employment statistics say? Would this be covered by the NHS EDI Improvement Plan? In terms of NHS England, would this be addressed by NHS England’s own workforce EDI plan? - One response noted that “BAME” recruitment needs to be reviewed at NHS England team level, suggesting there were unwarranted variations and unrepresentative teams.
A: Need to review ESR statistics? If so, is this an issue for any specific teams? - One response said that there should be an explicit commitment to improve the experience of minority ethnic communities in the same way as there is to improve the experience of LGBT+ staff. Another made a comment about the need to improve the workplace experience across all minoritised groups.
Q: Would this be covered by the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s workforce EDI plan?
- One response raised the particular issues that neurodivergent individuals can face. This concern noted that “especially for those who are considered ‘high functioning’, additional support is not in place”. The concern also noted that this group struggles with engaging with services and NHS staff, potentially leading to longer wait times and poorer outcomes.
- Another response noted that autism may not be seen as a disability, meaning that reasonable adjustments are not made [in the workplace].
Q: This should not be the case, is anything on this already written? Autistica has produced reports and guidance.
A: While not explicitly a target, the NHS LDEP is planning to hold an employment roundtable in the first half of 2023/24 where this issue will be considered.
Outreach
- The question was raised as to whether there were wider routes into employment for young people? There was a specific issue identified about young people with health conditions going into employment.
Q: Is this part of the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s workforce EDI plan? - A comment was made about the importance of using inclusive language in reaching out to people. It was also suggested that social media should be used to reach out to groups.
Q: Should this be picked up as part of the NHS EDI Improvement Plan? In terms of the internal agenda, would this be covered by NHS England’s workforce EDI plan?
A2 Patient access and communication
EO5 T1-2 (Accessible Information)
- One response asked what is happening with AIS implementation – what is the timetable and cost?
A: See assessment in the review and future objectives reports (Equality Objective 5, revised/new targets 1 and 2). Publication of the updated AIS information is planned for the first half of 2023/24.
- One response identified concerns about leadership, resourcing and capacity around the AIS leading to inconsistency and poor quality.
Q: Who is responsible for leadership on the AIS and what will be done to promote involvement? - One response raised particular challenges experienced by the deaf and hearing loss communities.
Q: Is this an issue for the AIS or another team? - One response identified concerns about the accessibility of online information.
Q: Is this covered by the Accessible Information Standard? Is this about communications delivery? This will be explored with the team leading on the AIS. - One response raised concerns about access to interpretation services that meet the needs of patients and service users. [Note: It was not clear if this referred to spoken languages (often called community languages) or British Sign Language (BSL) or both].
Q: Does this refer to the BSL review? To what extent does or should the BSL Review impact on the AIS review?
EO5T3 (inclusive language)
- There were a couple of questionnaire responses expressing concerns about service access being limited by the use of non-inclusive language. One response noted that trans and non-binary people had a worse experience than other LGBT+ communities.
The Youth Board also raised a concern about use of non-inclusive language. This was echoed by the LGBT Sounding Board, again with particular concerns about the effect on the trans community. Other forums argued for inclusive language for all protected characteristic groups. One question was why the focus on LGBT+ language and not on all protected characteristics.
A: This issue will be raised with relevant teams.
- Eight questionnaire responses identified particular concerns and issues for the trans community including issues regarding recording employment data on ESR, access and support. One general comment was “become more trans-inclusive in your approach.” The LGBT Sounding Board also raised concerns about access and waiting times for healthcare for trans people.
- One response to the questionnaire identified concerns about the “cultural competency” in the workplace questioning the ability of colleagues/managers to hear, see and identify discrimination. Another identified the need to challenge bias among staff with respect to both colleagues and patients. The LGBT Sounding Board identified similar concerns, particularly with respect to GPs, noting “all professionals need to have a similar level of understanding” and “a lot of medical professionals aren’t aware of the rights of trans people when it comes to health care as it’s a knowledge gap”.
No current target: Learning Disability and Autism
- The Learning Disability and Autism Advisory Group identified that: “‘autism may not be seen as a disability, meaning adjustments are not made [in the workplace]”.
- One questionnaire response raised a problem about the particular issues that neurodivergent individuals can face noting there was an issue: “…especially those who are considered ‘high functioning’, without additional support in place.
- Anecdotally there is suggestion that this group struggle with engagement leading to potentially waiting longer to seek access with associated worse outcomes etc…”.
- One questionnaire response said they would like to see reference to work tackling the inequalities that people with learning disabilities and autistic people face, linking to NHS England’s existing commitments in this area.
No current target: Mental Health
- A couple of questionnaire responses pointed to the forthcoming changes to the Mental Health Act and Mental Capacity Act.
- Another questionnaire response identified concerns about the slow progress on positive outcomes for African Caribbean men in the mental health system.
No current target: Vaccinations
- One questionnaire response commented that until equalities issues in vaccinations were addressed, these would have a detrimental impact on excess deaths and beyond.
No current target: Community languages and translation
- One questionnaire response identified particular concerns about access to interpretation that meets the needs of patients and service users.
- The Older People’s Sounding Board questioned whether improved translation software would help improve things for people.
A3 Volunteers
E06T6 (Volunteer monitoring)
- The target on volunteer equality monitoring was the least popular target with respondents to the questionnaire. It had a net negative favourability of -9.
A4 General comments and questions
Health inequalities
- A number of questionnaire responses identified health inequality issues beyond/outside the Equality Act 2010’s protected characteristics. These included socio-economic status and inclusion health groups that were not also protected characteristic groups.
- The Learning Disability and Autism Advisory Group identified concerns about geographical inequalities in services.
A: These issues fall outside the scope of the SEDs and are being referred to colleagues leading on the implementation of the health inequalities duty.
Individual questions
- One Youth Board member wanted to understand how the learning from COVID-19 was being applied to preparedness for any future pandemics.
- One questionnaire response identified that older women having babies suffered particular discrimination.
- One questionnaire response raised concerns about the access to genetic testing.
Annex B: Evaluation of the EHIN questionnaire
B1 Overview
A short questionnaire asked about NHS England’s 2022/23 equality objectives and targets. This questionnaire was sent out to members of the FutureNHS Equalities and Health Inequalities Network (EHIN). EHIN is made up of around 5000 members, primarily frontline NHS staff but also some local government and VCSE partners. The questionnaire was also sent to NHS England’s Engagement and Equality Champions, the NHS Equality and Diversity Council (EDC), the VCSE Health and Wellbeing Alliance and the NHS Citizen Advisory Group.
The questionnaire was live from 5 December 2022 to 6 January 2023 and 101 people responded. The questionnaire asked for overall views on how the equality objectives addressed priority equality issues, and asked respondents to rate which targets were of greatest and least priority for them. Free text sections allowed for the identification of crucial missing areas related to particular protected characteristics or equality issues.
The questionnaire also sought views to identify any groups less traditionally engaged by and with the NHS who might have issues not addressed by the targets. Respondents were also asked to comment on whether any particular engagement approaches should be used the future development of NHS England’s equality objectives and targets.
B2 Overall view of current objectives
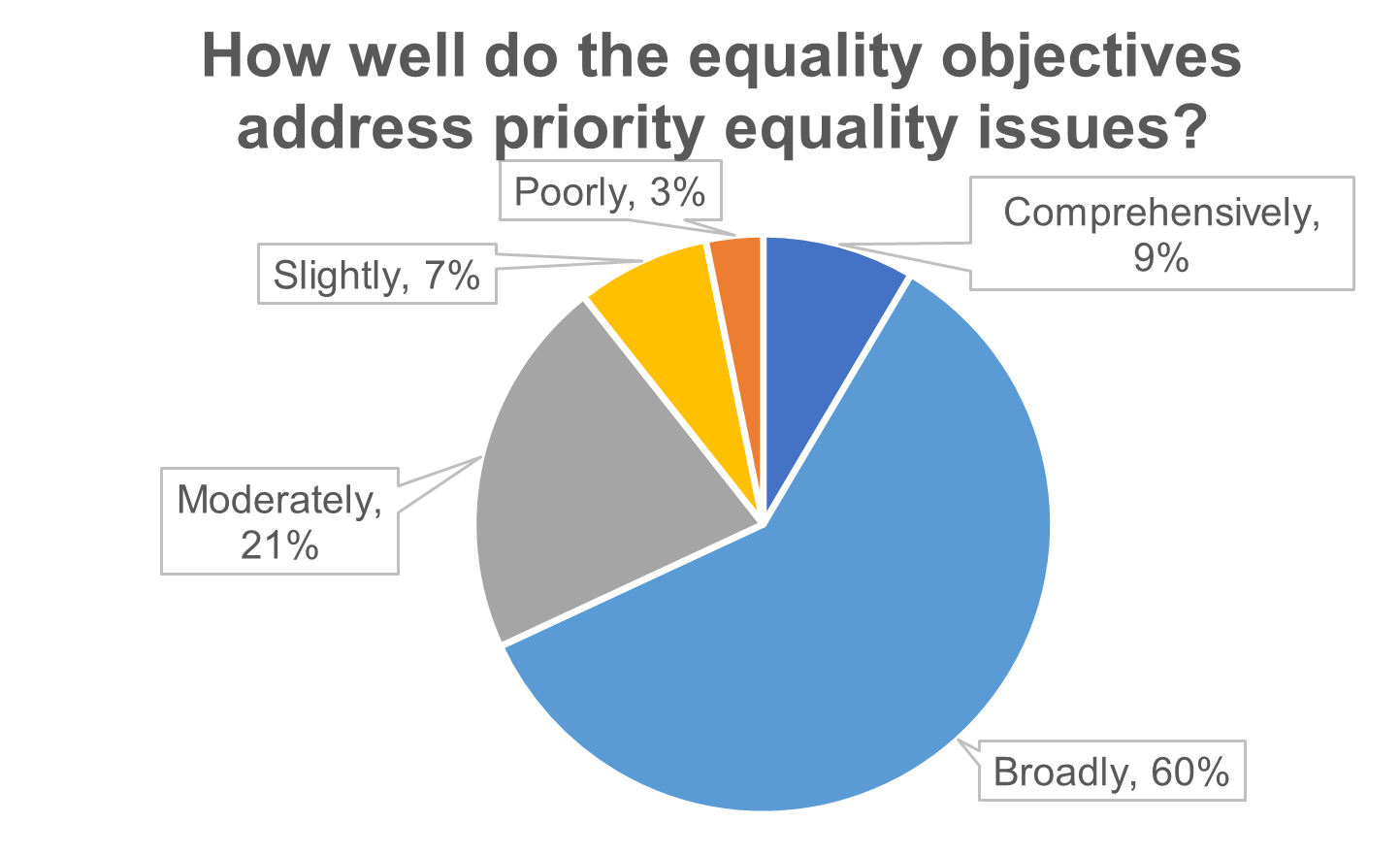
Most responses expressed positive views about how well the equality objectives addressed the priority equality issues within NHS England’s remit. More than two thirds (69%) said that the equality objectives comprehensively or broadly addressed the priority issues. One in 10 responses (10%) said that the equality objectives only slightly or poorly addressed the issues.
B3 Overall feedback on targets and objectives
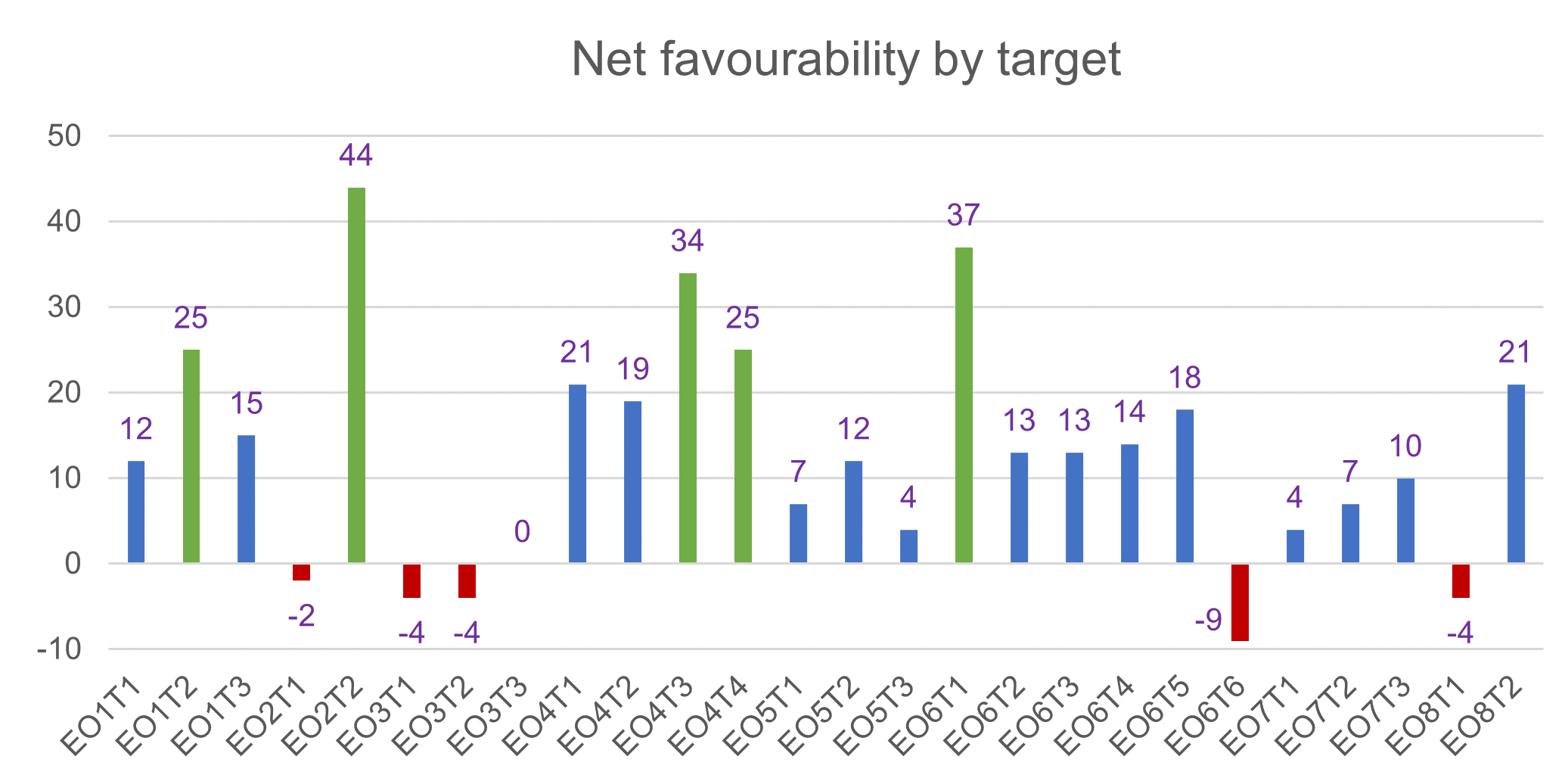
Respondents were asked to select their top 5 and lowest 5 priority equality targets (using the questions Which are the most/least important targets for NHS England to take forward to 2023/24?). From the responses, we calculated a net favourability score for each target by taking the number of people identifying it as a priority and subtracting those who identified it as a low priority.
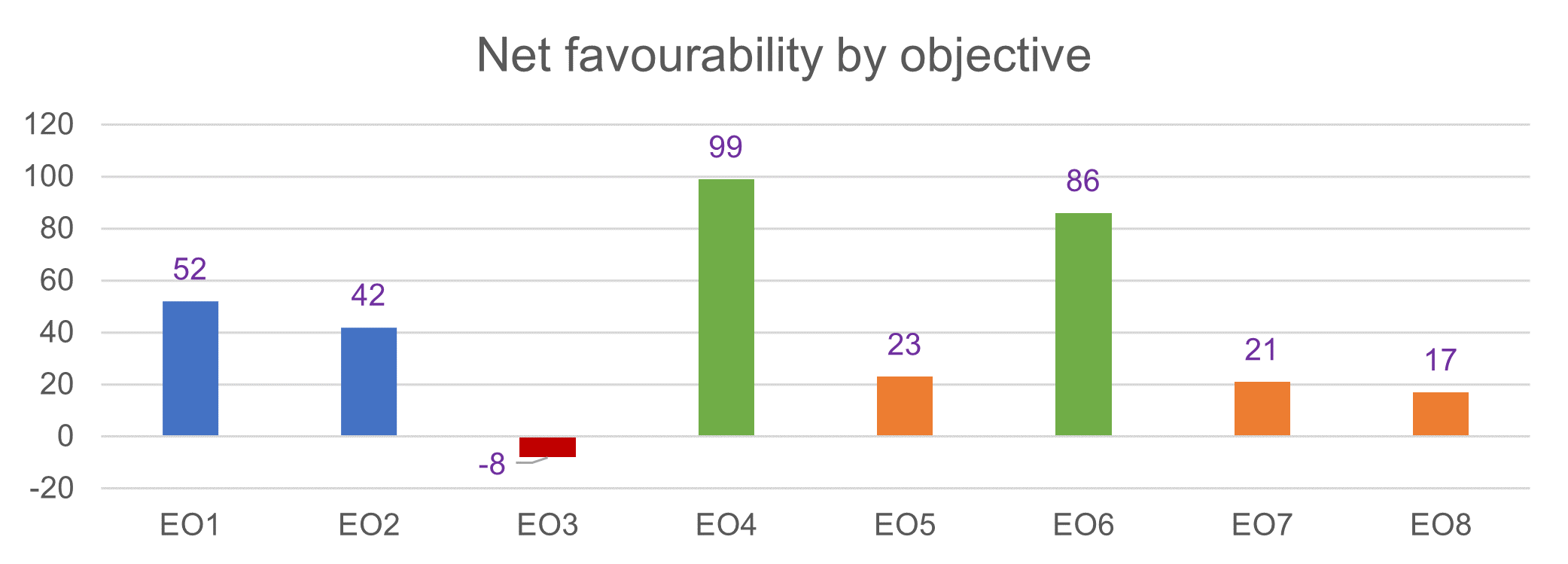
We also combined the figures for all the targets for each equality objective to produce a net favourability score for each equality objective.
Legend
EO = Equality Objective
EOT = Equality Objective Target
1 – 6 = The current targets listed for each relevant Equality Objective
The analysis shows that respondents gave the greatest priority to the targets for the two objectives connected with the workforce: EO4 [Internal Workforce] (99) and EO6 [External Workforce] (86). Respondents gave the lowest priority to the targets under EO3 [Information] (-8). The poor score for this objective probably demonstrates the lack of information available publicly on the Unified Information for Protected Characteristics (UISPC) Project.
The UISPC is still being developed and has not been publicised to the system or launched. Likewise, the targets for EO7 [Integrated Care Boards] (21) and EO8 (17) [System landscape] both refer to areas that relate to the changing infrastructure within both NHS England and the wider NHS. Respondents may be unaware of the implications of structural changes within the NHS for the exercise of NHS England’s functions. It is therefore understandable that these objectives and targets were not prioritised by parties who might not be aware of their significance. Respondents may not be aware that the exercise of public functions is a concept which is central to the Public Sector Equality Duty (PSED) and the Specific Equality Duties (SEDs). The PSED and SEDs govern the requirements in relation to the development of both equality objectives and equality targets.
At a target level, respondents gave the greatest priority to EO2 T2 (44), “To respond to the priorities identified by NHS England’s and NHS Improvement’s Boards to address patient equalities and associated health inequalities.” This clearly supports a drive to emphasise the priorities in addressing equality and health inequalities in policy making by NHS England and by NHS England’s Board.
The importance of diverse leadership was underlined by the priority given to EO6 T1 (37) “To increase the proportion of staff in senior leadership roles who a) are from a BME background b) are women c) disabled, in line with the NHS Long Term Plan commitments.” The importance of NHS England’s own approach to employment was also prioritised by respondents supporting EO4 T3 (34) and EO4 T4 (25). EO4 T3 is to undertake a change programme on our recruitment and promotion, further enabling the organisation to become an employer of choice and a workforce that reflects the communities we serve. EO4 T4 is to reset our EDI strategy and refresh our targets to ensure they are reflective of our EDI values, local labour markets and accommodating a merged workforce.
Target E06T6 on monitoring the diversity of NHS volunteers had a net unfavorability score (-9). Likewise, none of the three targets under EO3 [Information] obtained a net positive score (-4, -4, 0), though this is probably due to the low profile of the UISPC programme.
Similarly, the internally facing targets regarding the reconfiguration of NHS England scored relatively poorly, with the harmonisation of the approach across the incoming organisation (EO8 T1) scoring poorly (-4). However, the ‘fit for purpose’ test (EO8 T2) did score much more highly (21). Nevertheless, in order for the new NHS England to approach addressing the SEDs and the PSED effectively such harmonisation is crucial. It is also worth noting that all three targets under Patient Access and Communication [EO5] received relatively weak support. (7,12, 4) from the EHIN questionnaire but the narrative responses from Patient Forums indicated that patient access and communication is crucial (see Annex A).
B4 The free text questions
The questionnaire contained five sections where respondents were able to give free-text responses on five questions around the scope and delivery of the equality objectives and improving engagement to inform this work. Inevitably, this analysis has not sought to capture every single comment made, particularly those outside the scope of the equality objectives process (such as on broader health inequalities issues)*. However, this analysis does aim to convey the broad weight of the responses, particularly where clear common themes emerged.
*These predominantly related to socio-economic status, deprivation, homelessness and in some cases groups such as veterans. This information will be shared with the Healthcare Inequalities Improvement Team which leads on the health inequalities duty.
Suggestions on any crucial missed objectives and targets
Respondents were asked if the current objectives and targets had missed anything crucial with regard to the full range of protected characteristics, 34 responses answered this question.
This question attracted a range of comments and, as with all of the free-text questions in the questionnaire, there were a few responses (4) about factors driving health inequalities that fell outside the protected characteristics (such as deprivation or inclusion health groups). There were also a few comments (3) highlighting how intersectionality issues compound the challenges that people face. Alongside this there were some general comments and questions about how the existing objectives and targets will be delivered and implemented.
There were some specific comments relating to disability. One response commented on government proposals to reform the Mental Health Act which specifically aim to address ethnic disparities. This respondent also commented on the upcoming implementation of changes to the Mental Capacity Act.
Another response identified issues with the accessibility of online information for people with a disability, noting poor compliance with the requirements of the Public Sector Bodies (Websites and Mobile Applications) (No. 2) Accessibility Regulations 2018. Other responses noted the importance – and challenges – of the digital transformation agenda across the range of protected characteristics.
There were also a couple of responses about trans and non-binary people, noting they have particular issues with access to services due to the use of non-inclusive language. These responses also noted that NHS workforce IT systems do not currently allow trans/non-binary status to be recorded.
Equality issues of greater priority
Respondents were asked if there were any equality issues of greater priority that should be included in the equality objectives and targets, 40 respondents answered this question. A quarter (10) flagged up the interface with wider health inequality issues that extend beyond the protected characteristics (eg deprivation). A couple also flagged up other intersectionality issues.
There were also comments (4) about the need for closer monitoring of the experience of people with protected characteristics in both care and employment settings, and a broader call for better analysis of our current equality performance. One response pointed out that it wasn’t sufficient to just have diversity monitored in numbers, but also that people’s voices needed to be heard in employment and service settings. This coupled with another comment about the “cultural competency” in the workplace questioned the ability of colleagues/managers to hear, see and identify discrimination. Another response linked this concern to Objective 8, saying that it was important to baseline and track experience and outcomes for people with protected characteristics as NHS England transforms through the merger with NHS Digital and Health Education England and changes its strategic purpose.
Challenges with service access for groups sharing protected characteristics was identified by a few people (4). A couple of specific concerns around age in relation to employment issues – both for younger people and older people in the workforce – were identified.
Communities with issues not addressed by the existing objectives and targets
The questionnaire asked about communities or groups who are less traditionally engaged with the NHS (‘Seldom seen, seldom heard’ groups) that respondents thought had crucial equality issues which were not sufficiently addressed by the existing equality objectives and targets set for 2022/23.
This question was answered by about two-thirds of respondents (66 responses). In general, respondents replied by identifying groups, rather than identifying the issues that they face. As with previous questions, a quarter of responses (17) identified groups beyond the protected characteristics (including veterans, carers, socioeconomically deprived people and the inclusion health groups).
Intersectionality was identified as an issue (6 responses), with some responses identifying particular sub-groups with protected characteristics who faced specific issues (eg older women having babies, trans and non-binary people of colour, disabled children). Just over a quarter of these responses (17 of 66) identified that the Gypsy, Roma and Traveller community faced particular equality issues, but no specific issues were identified. Another sub-group identified by 12% of responses (8) were people with mental health conditions, including those with severe and long-term mental illness, neurodivergent individuals and people with learning disabilities.
The deaf and hearing loss community, particularly BSL users, was also identified by a small number of people (3) as facing particular issues. Digital exclusion (which strongly correlates with the protected characteristic of age) was also identified in replies (3), intersecting with age and ethnicity and health inequalities.
The quality of action and implementation was identified as an issue by some people (4), for example the slow progress on improving outcomes for African Caribbean men in the mental health system, or the effectiveness of engagement with certain communities.
Improving engagement
Respondents were asked about suggestions for effective forms of engagement for NHS England around the equality objectives and targets. A key focus was on reaching seldom-heard-from groups and 62 people, six in ten, responded. One clear and common theme from just over two-thirds of the responses (42) was the importance of working with, and through, community and VCSE organisations as ‘trusted partners’ of less-well engaged groups.
Suggestions included that NHS England should go to where communities are and listening at their groups, rather than forming new groups or panels. The importance of reaching out, tailored communications and coproduction was also emphasised. Some responses (4) suggested new structures – such as generating ICB-level structures, patient experience panels and marketing campaigns.
Some responses (3) raised the importance of ensuring communications are properly accessible, especially where digital engagement approaches are being used.
Other comments on delivery
This attracted a range of comments with a focus on implementation and evaluation and 30 people, just under 30%, responded to this question. Some responses praised the amount of work that was being done (4) and what was achieved, while others expressed frustration about the amount of progress (3).
The need for clear specific targets was highlighted (4) and the need for careful monitoring and reporting (5) was emphasised, saying this was more likely to deliver change than broader aims. There were also comments about the importance of progress updates on this work (4) and on improved communication and engagement to the NHS and the public.
There was also a specific call (1) to have a clear ask of Integrated Care Boards and Integrated Care Systems, rather than just focusing on NHS providers.
B5 About the respondents
Respondents were given the option to tell us something about themselves, though this wasn’t compulsory. These three demographic questions identified which of the groups the individual was a member of, their employing organisation and their broad job role (coded from the job title they gave us).
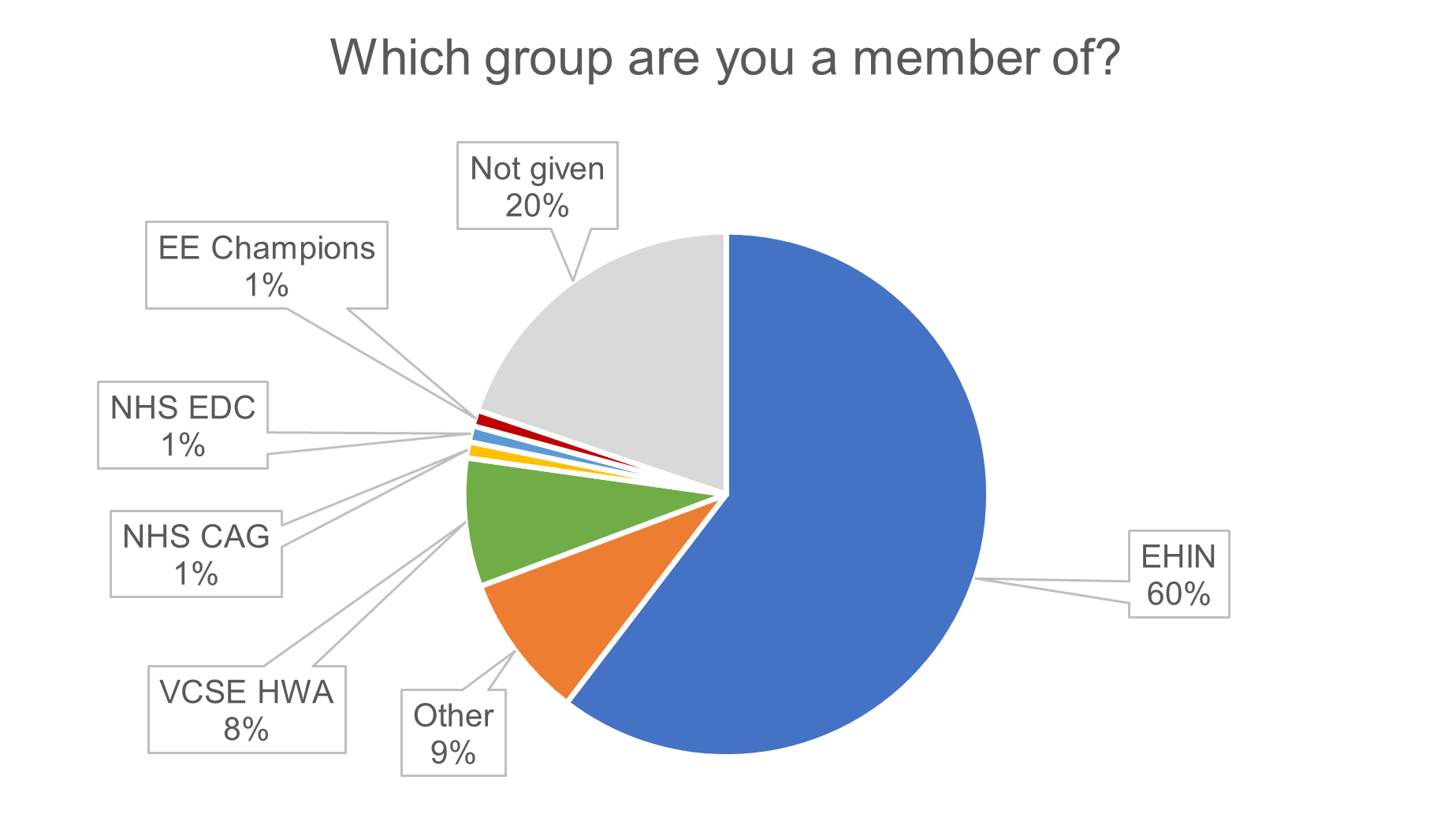
Sixty of the respondents told us they were a member of the EHIN, 8 were members of the VCSE HWA, 3 were members of the NHS CAG, the NHS EDC and the NHS England Engagement and Equality Champions. 9 came from other groups and 20 of respondents chose not to answer this question.
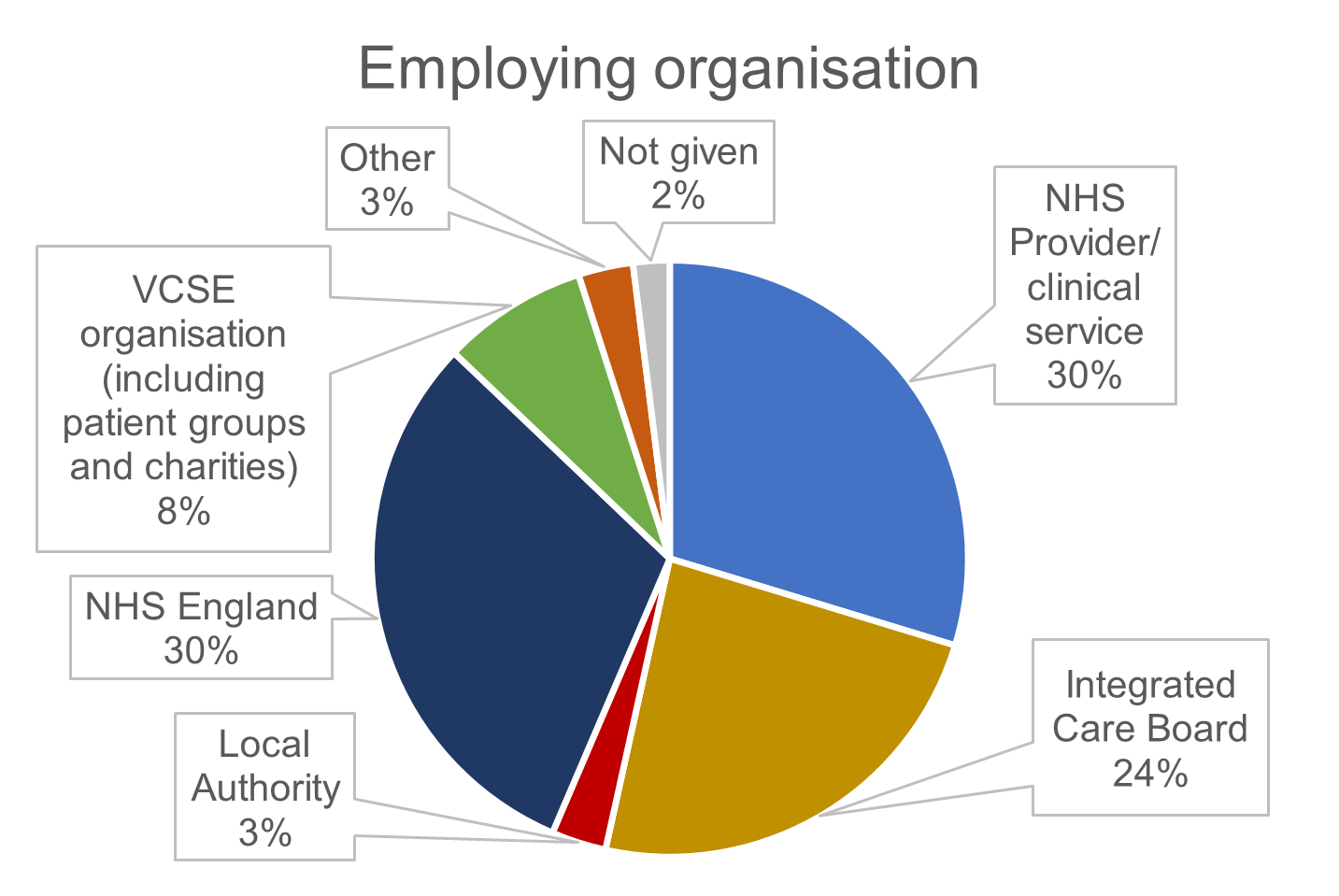
Thirty of the respondents told us they worked for an NHS provider or clinical service, 30 worked for NHS England and 24 of respondents worked for an Integrated Care Board. Eight of the respondents worked for VCSE organisations and 3 for local authorities. 3 respondents came from other groups and 2 of respondents chose not to answer this question.
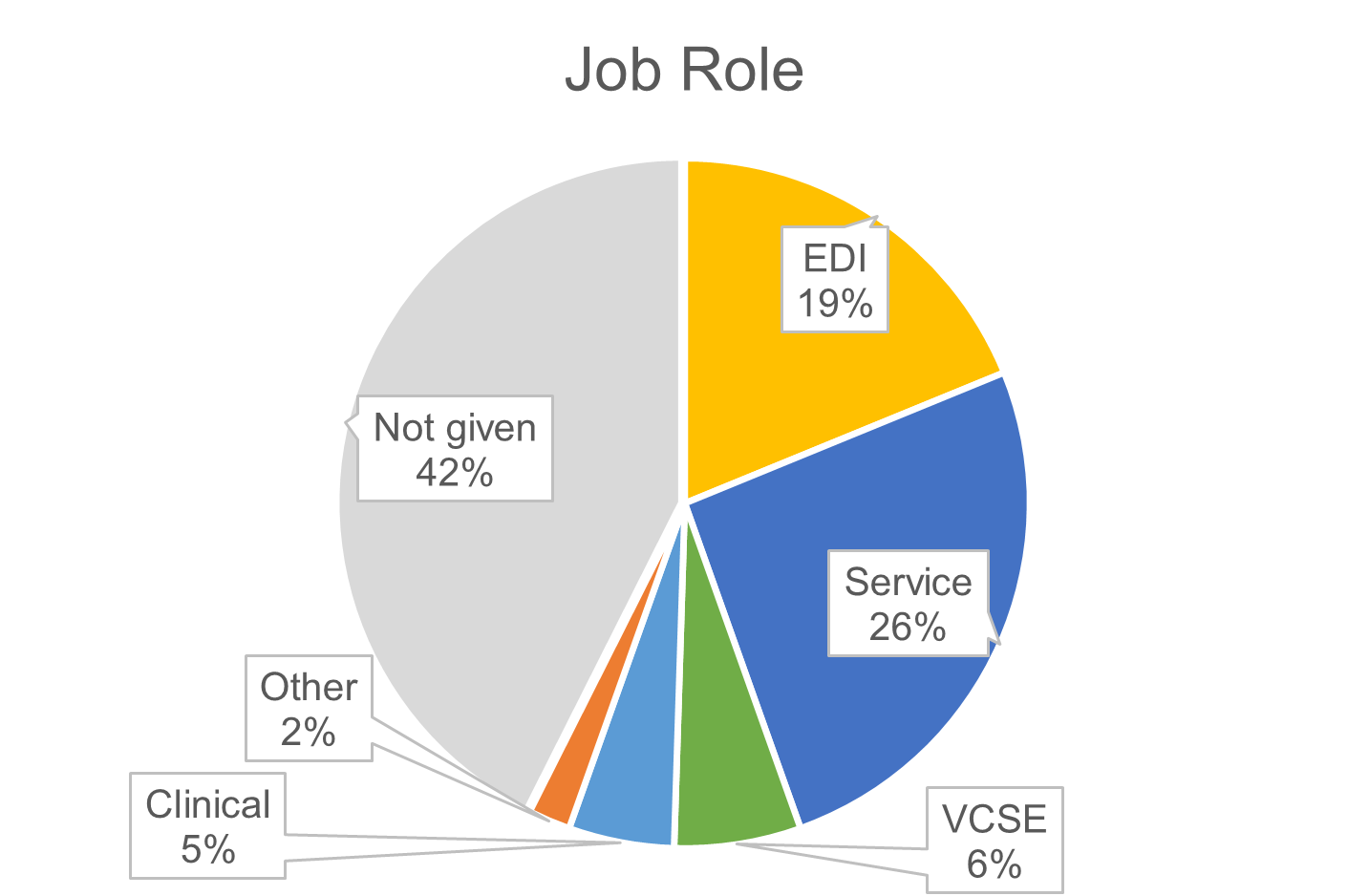
Twenty six of the respondents told us they worked in NHS service roles, while 19 worked in EDI roles. Six of the respondents worked for an Integrated Care Board and 5 had direct clinical roles. Two came from other groups and 42 of respondents chose not to answer this question.
Annex C: What we heard from the NHS England forums
We received rich and comprehensive feedback from the forums and groups we met. The following is a condensed version of their feedback which has been anonymised. We are incredibly grateful for the time and courtesy extended to us and this process. This EHIN questionnaire was sent out to members of the FutureNHS Equalities and Health Inequalities Network and other groups. The questionnaire was live from 5 December 2022 to 6 January 2023. Further information and analysis of the questionnaire can be found in Annex A.
C1 Citizen Advisory Group (CAG)
Early interaction with this group identified the importance of engaging with the member groups that make up CAG. Members of this group were also invited to engage via the EHIN questionnaire. One person identified themselves as a representative from the CAG, however, given the number of questionnaire responses who did not share which group or groups that they were a member of, the question was not mandatory, the actual figure could be higher (see Annex B).
C2 Equality and Diversity Council (EDC)
Members of this group were invited to engage via the EHIN questionnaire. Only one person identified themselves as a representative from the EDC however, given the number of questionnaire respondents who did not share which group they represented (it was not mandatory), the actual figure could be higher.
C3 Learning Disability and Autism Advisory Group
PET met with this group in November 2022 and the session included a presentation (an easy read version was also provided) on NHS England’s Equality Objectives and why they are important, followed by an engagement session with the comments grouped into themes:
Themes identified
Q: How do we make NHS England become a more inclusive employer? (eg how we train our staff; how we improve staff progression)
Culture:
- Making the NHS a more inclusive employer that people from any ‘protected characteristic’ can feel valued
- Employing people with lived experience will mean having easy read and alternative communications that are not just an afterthought
- Does NHS England involve its staff in setting its equality objectives?
- Staff surveys take time and this can be a barrier. Employees who are autistic and/or who are people with a learning disability won’t always like the survey format
Supporting and enabling inclusive employment:
- NHS England does some good work – we need to celebrate this
- Currently only 6% of people with a learning disability are in paid employment. Are there targets to improve this figure?
- Advertise vacancies where people with learning disabilities are likely to see them, and put them in easy read
- Induction and training – must be accessible
- Chances to progress and succeed
- Bringing in diverse voices through our groups and forums
- Why not have co-senior roles, where two people can share some of these very complex and demanding responsibilities?
Accessible processes for applications and interviews:
- “So many hurdles before you even get through the front door.”
- As routine, offer reasonable adjustments. This includes at interviews as well as in post
- As a reasonable adjustment, give questions in advance – this allows autistic people to prepare / process
- Use different methods for different groups of people applying for jobs
Practical considerations (in addition to reasonable adjustments):
- NHS England tends to be northern-centred, plus London. This excludes other areas, notably Cornwall/Devon
- Consider the impact of programmes and jobs on people’s benefits
- Make work as comfortable and flexible as possible
Demographic monitoring, disclosure:
- Not everybody identifies themselves as having a disability
- Stigma is a major concern for autistic people, who may well not want to disclose being autistic for fear of judgement
- Forms where people disclose being autistic often don’t have ‘autism’ as an option: it doesn’t feel good having to tick “other”
- It must be clear why information is being asked for
- Autism may not be seen as a disability, meaning adjustments are not made, and being seen as ‘able’ can mean you fall through the cracks; but also people reported experience of being told they can’t make decisions’
Accountability, responsibility:
- One of the problems in NHS trusts is that each trust is independent and some aspects are not accessible
- Guidance to NHS employers and organisations about the recruitment process and applying reasonable adjustments is inconsistently applied eg the accessible information standard
- Having a better culture and getting things right for people using services will lead to more people wanting to work in the NHS
- Sell the benefits – NHS England often cannot mandate actions for NHS organisations but it can promote them with examples of the potential for positive impact and improvement
- For some roles there is a challenge that recruitment can only happen for qualified people – what happens if there is not the diversity in the pool of qualified people that is being sought in the workforce of an organisation?
Q: How do we make NHS England a leader for equalities for the whole NHS?
Accessible communication:
- Accessible Information Standard – it is often unclear in NHS organisations who holds overall responsibility and a championing role – “it’s everybody’s job” leads to inconsistency and poor quality without this leadership
- Templates may be useful as a resource but they need to be readily adapted and tailored to individual needs
- There are many things that come under the heading of “accessible communication” – signage, letters, etc. Some of this will be outside the scope / capacity for influence of the equality objectives
Covid recovery:
- The move to digital and virtual provision that the Covid-19 pandemic accelerated is a cause for concern
- Covid has highlighted issues about ‘next of kin’: there was concern about people only being able to have one next of kin listed, despite there being several family members who jointly provided care and support
- People need to be in appropriate places; people should not die on busy wards; carers and loved ones who are (or want to be) but are prevented from being with a person when they die.
- Waiting lists should be tackled to stop people with a learning disability and autistic people dying prematurely
- Blocking access to other kinds of healthcare
Leadership and culture:
- ‘Humanity’, leadership should embody this
- How much do EHIAs actually impact on our strategies?
- Oliver McGowan training is being launched and will be co-delivered by people with lived experience of learning disability and autism
- Empower staff to do the right thing and not be criticised for having the best intentions
- Make sure nobody is left without care or “fobbed off”
- Treat relatives with compassion
- What guarantees that the things we talk about today will actually be done rather than going on a shelf somewhere?
- Listening, respecting and seeking change led from the top of the NHS
Involving people – across the system:
- Co-production is important
Accountability:
- Provide a feedback service – where people have a chance to express how they felt on a particular occasion about a service they are receiving
- It’s not very transparent how data [such as feedback data] has been used to shape policy
- Policy implementation needs to have more fluidity for services to respond to feedback and respond to the voices of service users
Equality vs equity – quality of care:
- Stop focusing on difference. There are endless subgroups – it will be impossible to be representative of all of them, especially in proportion
- There is a need to recognise that people’s differences should be met where possible through proactive adjustments rather than just reactive adjustments
- We [autistic people] need to be clear for ourselves how we want organisations to help us, whether we want to be “treated differently” or “treated the same”
C4 LGBTI+ Sounding Board
PET met with this group in November 2022 and the session included a presentation (an easy read version was also provided) on NHS England’s equality objectives and why they are important, followed by an engagement session with the comments grouped into themes:
Themes identified
Q: How do we make NHS England become a more inclusive employer? (eg how we train our staff; how we improve staff progression)
Language
- Gender inclusive language on websites and in information / literature
- Stop asking if you’re male or female
- Visibility of LGBT+ people/experiences through visual signifiers demonstrating supportive and welcoming environments
- Patient Care
- Work together on a guide for GPs – so many GPs don’t know how to treat us
- Develop a resource card. A lot of medical professionals aren’t aware of the rights of trans people when it comes to healthcare
Training
- Partner with LGBT+ organisations to develop and deliver some awareness training
Q: How do we make NHS England a leader for equalities for the whole NHS?
Training
- Improve education on LGBT+ health inequalities. Educate on microaggressions and everything LGBT+ people go through – eg self-loathing, having children, etc
- All professionals need to have same level of understanding – eg knowing not to misgender people based on voice or appearance
Policy
- Look at policies and to ensure they are LGBT inclusive
- NHS should be a vocal and visible leader advocating for LGBT rights and challenging LGBT phobic behaviour. This should be in its policies and in communications and information shared with patients and staff
Patient care
- If you cannot access an element of the healthcare process you need as a trans person, this will have huge detrimental impacts on mental health, ability to work etc and can perpetuate a cycle
- Stand up for the trans community instead of harming it
- Waiting times for trans healthcare are unacceptable
C5 Older People’s Sounding Board
The PET met with this group in October 2022 to seek feedback on NHS England’s equality objectives for 2022/23 and 2023/24. PET was specifically interested in feedback on the targets for 2022/23 and the development of the targets for 2023/24. PET explained the legal framework that governs the scope and the purpose of equality objectives. We also explained the impact of the current changes across the NHS, following the enactment of the Health and Care Act 2022. Forum members provided comments in the MS Team session with PET and provided additional clarification.
Changes to existing equality objectives
- You need to remove the references to NHS Improvement.
- What is the timetable for the implementation of the AIS (Accessible Information Standard)?
- Are equality objectives 3 and 5 the same?
Areas to be considered as part of the wider review of the Equality Objectives and targets
- EO1: Something has to be said about long Covid, it will be a huge drain to the system.
- EO1: Concerns about disability and mental health related to COVID-19.
- EO4/6: There appears to be no percentage target for staff with a disability, only for BME staff.
- EO4/6: We should be able to see who is being employed and in what proportions.
- EO4/6: Is staff training on inequalities mandatory?
- EO4/6: Are there statistics around mandatory training?
- EO4/6: Are there ‘published’ statistics of the outcomes of training around equalities?
- EO5: End of life brings out inequalities in care.
- EO5: Improved translation software should improve things for people shouldn’t it?
- EO5: How do you get ‘seldom seen, seldom heard’ groups to listen to what NHS is saying / comms approaches?
- EO5: Is the AIS (Accessible Information Standard) signed off? How much is the AIS going to cost?
- EO5: How do you reduce communication barriers in practice?
- EO5: I am ageing and childless with no one at all. No support and the NHS takes no interest in the fact I am totally alone and ageing. There is a less robust network for independent living for people like me.
- EO5: Not enough is being done for deaf people – masks make hearing difficult.
C6 VCSE HWA
The PET met with this group in January 2023 to seek feedback on NHS England’s equality objectives for 2022/23 and 2023/24. PET was specifically interested in feedback on the targets for 2022/23 and the development of the targets for 2023/24 and 2024/25. Attendees were provided with information about the legal framework that governs the scope and purpose of equality objectives. Information was also provided on the impact of the current changes across the NHS, following the enactment of the Health and Care Act 2022. Members of this group were also invited to engage via the EHIN questionnaire.
Changes to existing equality objectives
- Some equality issues not being delivered before Covid meant Covid had a greater adverse impact. Don’t want it to be seen as just Covid when bigger system issues than that.
Areas to be considered as part of the wider review of the equality objectives and targets
- What if something falls between the health inequalities duty and PSED gap?
- From disability and access, life is more than just accessing a clinical service.
- Most organisations have the evidence [on inclusive employment], but it is not in a format you need.
- It’s all about the narrative underneath. So not just about getting an appointment, it’s all about making sure reasonable adjustments are there.
C7 Youth Board and Youth Forum
The PET met with these groups in November 2022 (Youth Forum) and December 2022 (Youth Board). The Youth Forum discussion focused on how the engagement with the Youth Board would be undertaken. The session included a presentation on NHS England’s equality objectives and why they are important, followed by an engagement session with the comments grouped into themes:
Themes identified
Q: How do we make NHS England become a more inclusive employer? (eg how we train our staff; how we improve staff progression)
Training
- Are we issuing inclusivity training across NHS England and the local trusts? This could be a great way of ensuring people are kept up to date with ‘new’ inclusivity rules/legislation changes?
- Making sure it’s accessible, this does not just go for physical limitations
- There is stigma around mandatory training being boring or uninspiring. Can we make this more interesting and bring people together? What about asking people to share best practice of reducing inequalities?
Equality information
- Could we record information through ESR – asking about their characteristics?
- Communication
- Using social medial to reach hard to reach individuals
- More outreach. Making sure schools in deprived areas get the same information about how to go into a career within the NHS. Also support networks and more advertising about these.
Q: How do we make NHS England a leader for equalities for the whole NHS?
Case studies
- Share best practice
Policy
- Ensure that equality is an integral part of all policy writing – and ensure that it is referenced and referred to in every policy and guidance document
- Ensure that inclusive language is used
- When writing policies and guidance for patients, could you review the written pieces against any published NHS England HI framework?
Communication
- Being open about changes and progress – updating on social media platforms what has been done
- Regular communication and meetings
- Look into how we deliver messages to digitally excluded individuals. Do we still use ‘traditional’ forms of communication – leaflets, TV ads, word of mouth?
- Let people know how they can help contribute to the change in equality and that it’s okay to do so
- Being open to suggestions.
Publications reference: PRN00344
See also: