
1. Transforming sepsis care and outcomes
This framework sets out how the NHS and its partners will improve sepsis care.
It is designed to inform those involved in planning, commissioning and improving services for people with, or at risk of, sepsis.
It sets out the priority actions needed to achieve more consistent, high-quality care. All actions are relevant to all age groups, unless otherwise specified.
1.1 Our ambition
Our ambition is to reduce death, life-threatening complications and long-term impact from sepsis and severe infection in all patient groups by at least 25% by 2035.
This includes reducing the health inequalities that mean some groups are more likely to experience poorer outcomes.
In this framework, ‘severe infection’ refers to infections requiring hospital-level care (including treatment delivered at home in virtual wards).
1.2 What is sepsis?
Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection. While it is an unusual complication of developing an infection, it can be triggered by any infection. When people die from an infection, it is most commonly due to sepsis.
Alongside its immediate risks, sepsis can also have long-term effects for patients and carers.
“Sepsis took all 4 limbs… and people are going, wow, I didn’t know a urinary tract infection could do that. And I’m like, any infection can do that … Just watch out for sepsis.” – Kim, quadruple amputee and sepsis survivor
1.3 Why do we need a modern service framework for sepsis?
Sepsis is a priority because it is a significant cause of death and ill health. It also presents persistent challenges across prevention, diagnosis, treatment and recovery.
Sepsis is complex and hard to diagnose, with no single test and symptoms that overlap with other conditions. Differentiating between severe infections and sepsis can be challenging, and severe infection may lead to the development of sepsis; diagnosing infants and children can be particularly difficult.
It is time‑critical but not always recognised early enough, and delays can lead to organ failure, serious illness and death.
Outcomes are not equal across the population, with higher risks and poorer outcomes for some groups, such as:
- babies
- older people
- people from more deprived areas
- those with serious mental illness
- people experiencing homelessness
- some people with a learning disability and autistic people
Recovery can be long and is often not well supported, with lasting physical and mental health impacts.
Sepsis places significant and growing pressure on services, including emergency care, hospital capacity and critical care.
Sepsis care and outcomes vary across the NHS despite national guidance and improvement programmes.
Data is incomplete and inconsistent, making it harder to understand variation and improve care.
Balancing rapid treatment with antibiotics and tackling antimicrobial resistance is complex, with risks from both delayed treatment and unnecessary antibiotic use.
Facts and figures
133,484 hospital admissions in 2024/25 were recorded with a primary diagnosis of sepsis, although this is likely to be an underestimate of the actual number of sepsis cases.
People admitted with sepsis in 2024/25 stayed in hospital for an average of 14 days.
In 2024/25, 10% of inpatient stays with a primary diagnosis of sepsis resulted in critical care admission, with an average critical care stay of 7 days.
Just over 7% of people with a ‘suspicion of sepsis’ will die during their acute hospital admission, while inpatient mortality for septic shock is around 55.5%.
Sepsis care cost £1.037 billion in 2024/25.
More widely, infection care on acute wards alone cost £6.7 billion in 2024/25. These costs do not include the cost to the economy due to lost productivity, social care and other costs.
Sepsis was involved in over 1,300 clinical negligence claims between 2020/21 and 2024/25, leading to £65.3m in litigation costs. Most claims relate to delays and failures in treatment and diagnosis.
Further detail on the evidence and clinical background underpinning these challenges is provided in Appendix B.
1.4 Our approach to preventing infection and improving sepsis care
This modern service framework aligns with the Quality strategy for NHS-funded care in England and the 10 Year Health Plan, including the 3 strategic shifts: hospital to community, analogue to digital, and sickness to prevention.
It is structured around 6 themes, which together provide the architecture for action.
A personalised approach
We will identify people at risk earlier and tailor prevention, treatment and recovery support to improve outcomes and reduce inequalities.
Supporting people to understand sepsis: our staff and the population
Staff training and public education and awareness will underpin all our efforts to transform care and improve outcomes.
Prevention of severe infection and sepsis where possible
As sepsis can be triggered by all kinds of infections, we will address the burden of infection through effective prevention and management.
Identification of severe infection and sepsis
We will improve the timely identification of patients with infections that may be progressing to sepsis, prioritising those who need urgent investigations and interventions. We will improve the speed and accuracy of identifying infection, its source, antimicrobial sensitivity and sepsis diagnosis.
Escalation of care
We will improve the processes for identifying deteriorating patients and ensuring they receive timely access to the care they need. This will reduce the risk of organ failure and death.
Response that is timely, appropriate and effective
We will deliver timely, safe and individualised care, with effective systems for managing complex interventions and supporting patients through the acute illness onto longer-term recovery and rehabilitation.
The actions we will take to deliver these are set out in Section 3.
1.5 Research and innovation
Delivering required improvements in sepsis care means developing new approaches, as well as improving current practice. Research and innovation will therefore underpin all 6 themes, including overcoming the challenge of translating new discoveries into clinical practice.
2. Defining success
2.1 Why this ambition matters
In setting our ambition to reduce death, life-threatening complications and the long-term impact of sepsis and severe infection by at least 25% in all patient groups by 2035, we wanted to make clear that improving outcomes for survivors sits alongside the imperative to reduce deaths.
Sepsis can have life-changing consequences for patients and carers, including long-term impacts on physical and mental health. Success will therefore mean not only preventing deaths but supporting sepsis survivors to live full and active lives, including returning to work and other usual activities.
2.2 Improving outcomes for all patient groups
What we can achieve will vary between different groups of people. Some variation reflects differences in how sepsis affects individuals and how they respond to treatment. For example, a significant proportion of sepsis deaths are associated with existing co-morbidities or severe frailty, and some patients die despite completely appropriate and high-quality care.
However, some groups experience worse outcomes, even though there is no biological reason for this. It is not enough to improve sepsis outcomes for the whole population without narrowing these unwarranted gaps.
Therefore, when tracking our progress over the next 10 years, we will look at the overall changes in quality of care and outcomes, as well as changes in specific groups.
2.3 What success would look like in 2035
If we succeed, by 2035 people should experience a fundamentally different approach to preventing, identifying and treating infection and sepsis, and we will be able to make the following statements.
We know exactly how many sepsis cases there are across England and use linked data to understand how care was managed across all settings and what outcomes were achieved.
The growth in infection rates has stopped or reversed, particularly among older people.
People are supported to prevent infections through high-quality advice and support, including through vaccination.
Care is more personalised, and services are designed around people’s needs and experiences.
Those at higher risk of infection are using monitoring devices, including wearables, at home that reduce risk and flag deterioration to their neighbourhood health team.
When people feel ill, they can use their mobile and other devices to assess their symptoms, including measuring heart rate and blood pressure using their mobile phone camera.
AI-supported analysis of these measurements identifies people who may need medication and directs them to the most appropriate care pathway.
Staff are skilled and confident in identifying sepsis, including in vulnerable people, and can provide timely, effective care. They know if someone has repeatedly sought help in a short period of time and AI-supported systems help identify if this needs escalation.
Some treatments traditionally delivered in hospital, such as intravenous antibiotics, can be provided safely and reliably in patients’ own homes.
Rapid point-of-care tests – using saliva, urine or a finger-prick of blood – are available wherever needed to identify any infectious agent and its antimicrobial susceptibility.
Tests are available that can identify organ dysfunction and the severe immune and inflammatory response that can occur in sepsis at an early stage, enabling prompt treatment.
We better understand how different people respond to infection and sepsis, allowing us to target specific interventions to patients likely to benefit, such as immunomodulators to reduce the risk of organ dysfunction.
Patients who require intensive treatment receive timely access to enhanced care, immunomodulators that prevent sepsis, antimicrobial therapy and any other support needed, in line with their clinical need and wishes.
Most people recover from infection with no long-term impacts and care quality is consistent and equitable for all patients.
The few who develop sepsis, perhaps related to other co-morbidities, receive long-term recovery support as standard, with a much-reduced risk of readmission.
Those approaching end of life, who develop a severe infection that may lead to sepsis, are cared for in a place of their choosing until they die, pain-free and in comfort.
There is a comprehensive and sustainable sepsis research and innovation infrastructure, guided by patient experience and participation, with clear routes to bring proven innovations into practice.
3. Priority actions to reduce sepsis incidence and improve care and outcomes
The actions in this section are structured under the framework’s 6 themes and include timelines according to the following definitions:
- immediate: within 1 year
- short-term: within 2 to 3 years
- medium-term: within 4 to 5 years
- long-term: within 10 years
Work will be led by the Department of Health and Social Care (DHSC) and NHS England. Where applicable, we also detail key roles for delivery partners and the wider NHS.
3.1 A personalised approach
Action 1: improve our understanding of sepsis to enable personalised care
National Institute for Health and Care Excellence (NICE) guidance lists conditions and contexts which place patients at higher risk of sepsis. We will build on this by using NHS data and advanced analytics to better understand who is at greater risk of sepsis and why, so we can improve the accuracy of sepsis prediction and patient stratification.
Over time, we will incorporate results from innovative tests (such as novel biomarkers, genomics and ‘omic technologies) to improve risk modelling and prediction. This will include evaluating advanced analytics such as machine learning.
For patients in the community at higher clinical risk, such as those with indwelling devices or catheters, we need to better identify when infection may be resistant to first-line antimicrobials and when it is safe to ‘watch and wait’.
We also need systems that reliably identify patients who present repeatedly over a short period and ensure clinicians can access data from previous contacts, especially for those at higher risk.
For patients with repeated infections, we need a better understanding of sepsis risk, pathogen identity and antimicrobial sensitivity.
Priority tasks:
- work with clinical and academic experts including UKHSA to develop, validate and implement risk prediction and stratification tools to support clinical decision-making aligned with NICE guidance (short-term)
- enable identification of at-risk patients in the single patient record, ensuring relevant information on previous infections, antimicrobial sensitivities and suggested treatment plans is available to all relevant health professionals (medium-term)
- use the Federated Data Platform (FDP) to analyse operational, clinical and diagnostic data to support care and service improvement (medium-term)
- work with the NHS, NICE, UKHSA, academia and industry to develop new approaches to predicting risk of sepsis, and risk of adverse outcomes. This will include developing and implementing genomic and ‘omic applications and biomarkers, incorporating them into risk prediction tools, and considering the opportunities presented by machine learning and other forms of AI (long-term) – also see Section 5
Action 2: improve advanced care and treatment escalation planning
Care for people at the end of their lives must be delivered with compassion, with a focus on what matters most to that person. For some people who develop sepsis, irrespective of age, there may be little that can be achieved from highly invasive organ-support interventions.
Advance care planning (ACP) is a voluntary, structured process for people to discuss their preferences and priorities for their future care with their care providers. When done well, it helps ensure people feel more confident that their care and treatment will be focused on what matters most to them as individuals.
Treatment escalation planning (TEP) is a clinician-led process which is helpful when a person with serious illness has the potential for acute deterioration or may be coming towards the end of their life. It provides the opportunity for clinicians to agree a plan with the person, or if they lack capacity, with those important to them, to guide decision-making about what treatments the person would receive should their condition deteriorate.
To ensure that patients and families receive the right treatment and care, we will improve how we identify patients who would benefit from advanced care planning and treatment escalation planning, and how that information is shared across health and care settings. This includes:
- clearly communicating what matters most to the person
- agreed ceilings of treatment
- rapid access to supportive end of life care where escalation is not in the person’s best interests
Improved risk stratification and prediction, using the tools developed in action 1, will support decision-making for patients, families, carers and clinicians.
This work will be co-ordinated with the forthcoming modern service frameworks for end-of-life care, and frailty and dementia, ensuring alignment with wider palliative and end-of-life care priorities.
Priority tasks:
- support teams in primary, secondary and social care to identify patients who are at high risk of poor outcomes from infection and sepsis
- embed shared decision-making, compassionate conversations and advance care planning (including treatment escalation planning where appropriate), so that people’s preferences and wishes for their future care are known, recorded, shared and acted upon (short-term)
- explore the development of digital systems to enable clinicians to record, flag and use advance care planning and treatment escalation planning, including through the shared care record and single patient record (medium-term)
3.2 Supporting people to understand sepsis
Action 3: deliver a targeted public communications campaign for high-risk groups
While most people have heard of sepsis, fewer can recognise the full range of symptoms. We therefore need to raise awareness and improve understanding, while avoiding unnecessary anxiety and demand on health systems.
This means improving our understanding of how to target messaging, using different strategies for different patient groups to support safe self-care and appropriate and efficient use of resources.
We also need to improve public understanding of how to prevent infection and sepsis in the first place, including:
- the importance of vaccination (as detailed by NICE)
- other infection prevention strategies
- symptoms and signs of more severe illness
- what to do based on symptoms and signs
- how to communicate concerns to healthcare professionals
- the role of antimicrobials (as detailed by NICE) and key antimicrobial stewardship messages
These messages are complex, and they will likely need to be tailored to different populations and groups, using community groups, leaders, trusted voices and relevant media.
We will work with patients, carers, communications and clinical experts to test how best to communicate the signs of sepsis in different ways and at different times.
We will also explore leveraging other related public health campaigns, working with organisations like the UK Sepsis Trust, which already work in this area.
In addition, we will ensure alignment with related initiatives that rely on public awareness, including Martha’s Rule, which highlights how listening to patients and carers can support earlier identification and response to severe infection and sepsis.
Priority tasks:
- develop a targeted, public communications campaign to improve prevention, identification, escalation and response to sepsis, focusing on high-risk groups (short-term)
- target communications to aid prevention and increase vaccination uptake and catch-up coverage across the population, including underserved communities, in line with the NHS Vaccination Strategy (see Action 6) (short-term)
“Sepsis should just be one of those things that’s up there with standard first aid training, just knowing the signs – the same way people now know what to look out for with a stroke.” – Charlotte, whose dad, Fitz, died from sepsis
Action 4: improve audit and feedback of sepsis-related data
To better understand sepsis and other infections and track progress, we need a step change in how we collect, analyse and use data. This is essential to the success of the framework and will underpin future incentives, such as best practice tariffs (see Section 6).
At present, there isn’t a robust baseline or sufficiently granular data to fully understand sepsis epidemiology in the NHS. This includes even basic outcomes, such as:
- sepsis-related mortality
- how this relates to wider severe infection
- what the underlying causes are
- which groups are most affected
We also lack data on processes of care related to sepsis, with only limited data in a few specific clinical areas from national audits. As a result, healthcare providers and commissioners do not have the information they need to fully understand their care and outcomes, plan services or monitor and benchmark care quality.
Priority tasks:
- commission a new national infection and sepsis audit programme, initially looking at the acute sector, with potential to expand into community settings, to understand the prevalence and incidence across all populations and patient groups and develop data tools that support quality improvement. Once implemented, this will form the basis of our quality assurance and improvement efforts, and all acute providers will be expected to participate (immediate and short-term)
- work with existing audits to add relevant questions on evidence-based processes of care (short-term)
- scope out the use of routine data to develop a quality surveillance system, similar to the Maternity Outcomes Surveillance System, to enable near-real-time determination of potential outliers, learning from high-performing organisations and directing support to those that need it (short-term)
- use electronic health record data to improve audit and feedback to providers in primary and secondary care, linking with wider work on, for example, the single patient record, NHS App and FDP (medium-term)
- ensure provider organisations use audit and other data to improve compliance with evidence-based care, incentivised through financial and other levers, such as best practice tariffs (see Section 6) and the National Oversight Framework (short-term)
- explore the use of Patient Reported Outcome Measures and Patient Reported Experience Measures to provide a holistic view of quality (medium-term)
Action 5: review and update training and guidance across the care pathway
Delivering standardised, high-quality care will depend on awareness raising and training in sepsis identification, infection prevention and control (IPC), antimicrobial resistance (AMR) and acute deterioration for all relevant people, including:
- NHS staff working across both physical and mental health
- social care staff
- professional and unpaid carers
This must be supported by clear, accessible guidance.
Feedback from stakeholders, patient safety incident investigations and coroners’ reports highlights the need to improve how well symptoms are recognised, and how effectively healthcare staff understand the concerns of patients and carers when they are worried about someone’s symptoms.
Priority tasks:
- work with partners to develop resources for carers, health and care staff, at-risk patients and the wider public to support recognition of symptoms, with a focus on specific risks, such as use of indwelling catheters, severe mental illness or immunosuppressing treatments (short-term)
- assess the role of minimum training standards for relevant staff groups, including executive leaders (immediate)
- lead work to develop and update training on sepsis identification, deterioration management, infection and antimicrobial stewardship, tailored to different staff groups and including innovative methods, such as:
- low and high-fidelity simulation
- augmented and virtual reality and group training
- how best to support staff to recognise the cognitive biases (like diagnostic overshadowing) that can impact care (short-term)
- explore the use and effectiveness of ‘just in time’ resources, which provide rapid accessible support for those involved in triage (short-term)
- consider extending training on the management of sepsis and severe infection in children and young people to all staff, not just paediatric specialists (short-term)
- align training and education with the upcoming NHS 10 Year Workforce Plan and the shift of care from hospital to community (short-term)
- ensure guidance on sepsis, infection, AMR and related areas is up-to-date, relevant, curated, consistent and accessible (immediate and ongoing)
3.3 Prevention of severe infection and sepsis where possible
Action 6: increase vaccination coverage and uptake
Vaccination is important for preventing sepsis-related morbidity and mortality. Addressing unwarranted variation in vaccination rates will also reduce health inequalities.
The future deployment and delivery of national immunisation programmes is set out in the NHS Vaccination Strategy. Delivery of this framework will support shared goals.
Priority tasks:
- deliver actions in the NHS Vaccination Strategy that align with this framework, including:
- improving access to vaccination
- tailoring vaccination services to local population need
- using trusted people and organisations to increase confidence in vaccination
- increasing vaccine uptake in health and social care workers
- including a person’s vaccination status in the NHS App
- supporting the future vaccine pipeline through clinical trials
- working with research funders to develop new vaccines (all actions ongoing and throughout the life-course of the framework)
“I feel passionately that vaccination is the best prevention… not all infections are preventable and it’s part of life, but for the ones that there are vaccines available for, I think they should be encouraged.” – Lily, quadruple amputee and sepsis survivor
Action 7: improve infection prevention and management for higher-risk groups
Vaccination is essential, but it is vital that it’s supported by wider infection prevention and management across all care settings. As this can be complex in practice, it will benefit from co-ordinated improvement support, similar to the implementation support for Martha’s Rule.
In the short term, we will focus on improving community infection prevention and management for specific high-risk groups by supporting carers, community nursing teams, domiciliary care staff, care homes and wider services. People considered higher risk include:
- people who are immunosuppressed
- people with severe mental illness
- people with indwelling urinary catheters and central lines
- people with compromised skin integrity
- people with swallowing difficulties and PEG (percutaneous endoscopic gastrostomy) tubes
- pregnant or recently pregnant women
- newborns and younger children
- older adults
Stakeholders have raised concerns about persistent challenges for some groups and the clarity, consistency and implementation of existing guidance, such as NICE guidance on neonatal infection. In pregnancy, sepsis is the second most common direct cause of death (after thromboembolism) and the second most common indirect cause of death (after cardiac disease). Although the overall numbers are small, there has not been a notable improvement in pregnancy-related sepsis deaths over the past decade.
Across all patient groups, there are opportunities to improve how care is delivered, including through community-based models aligned with the 10 Year Health Plan. While sepsis itself likely requires hospital care, community outreach or response teams may improve community infection management. This could:
- support earlier identification and diagnosis
- expand the use of Outpatient Parenteral Antimicrobial Therapy (OPAT)
- help patients return home more quickly after interventions, including surgery
- make use of innovations such as virtual wards
All of these approaches require rigorous evaluation with embedded safety-netting.
This work will be supported by, and aligned with, the work on identifying those at high risk (Action 1), awareness-raising (Action 3) and training (Action 5), as well as the National action plan on antimicrobial resistance.
Priority tasks:
- work with health and social care providers and other experts to design and implement a national infection prevention and management improvement programme in community settings, focusing on high-risk groups (short-term)
- consider whether additional targeted infection prevention and control guidance is needed for specific groups alongside existing NICE Quality Standards (short-term)
- examine opportunities for community-based care, supporting patients with infection and recovering from sepsis, including through neighbourhood health models (medium-term)
- focusing on high-risk groups, review compliance with evidence-based infection prevention and management, and continue to develop the evidence base for novel approaches, such as community infection outreach teams (medium and long-term)
In neonatal care specifically, we will:
- build on the outcomes of the GBS3 study and other research to improve prevention of group B streptococcal infection
- support implementation of the Saving babies’ lives care bundle
- consider opportunities for improved neonatal community support, for example, through standardised and commissioned neonatal outreach services
- work with NICE and other experts to explore the potential for further evidence-based minimum standards for infection prevention, including:
- line-associated infection and ventilator-associated pneumonia
- aseptic non-touch technique
- equipment cleaning
- using personal protective equipment
- explore options for improving the neonatal intensive care unit (NICU) estate so that minimum space and air handling standards can be met and there is sufficient and appropriately trained staff to deliver care, as part of the upcoming NHS 10 Year Workforce Plan
- embed automatic collection of data on positive blood cultures so measures of invasive infections can be measured and tracked to support quality improvement
We will take a similar approach for children and young people (for example, through paediatric early warning system implementation), care homes and pregnant or recently pregnant women (medium-term).
3.4 Identification of severe infection and sepsis
Action 8: improve the speed and accuracy of diagnosis
Faster, more accurate diagnostic tests would significantly improve care, outcomes and antimicrobial stewardship. This includes tests that can identify whether a patient has an infection, which pathogen is causing it, which antimicrobials it is sensitive to, and whether there is organ dysfunction or an overwhelming immune and inflammatory response.
The ADAPT and PRONTO clinical trials have already shown that testing for pro-calcitonin can improve care.
We now need an improved approach to evaluating and adopting new diagnostic tools, ensuring real-world evidence on effectiveness and cost can support quick, safe deployment.
Priority tasks:
- work across the NHS, UKHSA, academia, research funders, NICE and industry to develop and implement diagnostic tools that are clinically and cost-effective to:
- improve infection diagnosis
- differentiate between bacteria, viruses and fungi
- profile antimicrobial sensitivity
- objectively measure the related immune and inflammatory response
- This work should be aligned with the research and innovation action plan (Section 5) and optimise existing pathways (Action 9) (short and medium-term)
- accelerate the implementation of near-patient and rapid diagnostic tools to support objective assessment of organ dysfunction (long-term)
Action 9: optimise existing pathways and care in all settings
Rapid diagnosis and treatment in urgent and emergency care (UEC) can be challenging, particularly for emergency departments and ambulance services, which are often under pressure.
Clinicians need access to rapid diagnostics, for example, through the blood culture pathway or point-of-care diagnostics, so they can narrow the differential diagnoses and ensure patients receive the right treatment. As a minimum, we should ensure lab test results meet existing standards for turnaround times, but we also want to explore opportunities to set more ambitious standards coupled with the expansion of relevant point-of-care diagnostics to speed up the process.
We know optimising acute pathways can be effective. For example, Cambridge University Hospitals implemented a trust-wide electronic patient record improvement programme (Future collaboration platform log-in required) to support community-acquired pneumonia treatment and create an intravenous‑to-oral antimicrobial switch alert. This reduced the length of stay by 2.5 days and saved £120,000 annually through released bed days.
Stakeholders have highlighted significant inequalities in access to specialist reviews in paediatric or neonatal care when specialists are not available on site. Furthermore, variation in the capacity of neonatal and paediatric critical care beds can delay identification, escalation and response.
In the short term, providers should develop networked approaches to specialist review and intervention. This will help establish clear diagnostic and treatment pathways and provide a safe standard of care for all patients, regardless of age, setting or time of day. This ambition aligns with the National Care Delivery Standards, which NHS England will publish in 2026/27.
In the longer term, we will work with stakeholders to establish any workforce and training gaps that affect the speed and quality of investigation and treatment for all patient groups. This will involve carefully balancing risks and may involve further training for non-specialists and the development of new standards.
Priority tasks:
- ensure that all relevant providers have timely access to specialist advice for relevant diagnostics and interventions either on-site or through networked approaches (short-term)
- develop a nationally designed, locally delivered quality improvement programme to optimise acute management of severe infection and sepsis across ambulance, emergency department and the wider UEC pathway (short-term); this will involve:
- improved use of relevant Early Warning Scores
- escalation and response pathways
- consideration of care in the first 24 to 48 hours after admission, building on the Start smart then focus antimicrobial stewardship toolkit
- exploring how we might support this approach through a best practice tariff
- all services that may be responsible for triaging patients with sepsis, including 111 and 999
- work with the National Emergency Laparotomy Audit (NELA) and relevant royal colleges to explore the development of a pathway for acute surgical presentations of sepsis, focusing on emergency abdominal surgery; this work will:
- create standards that can be measured in the NELA
- accelerate access to imaging, antimicrobials, assessment by senior anaesthetists and surgeons, and surgery or interventional radiology for source control (short-term for a diagnostic phase; medium term for implementation)
3.5 Escalation of care
Action 10: improve management of deterioration in community settings
We must improve how quickly and accurately we recognise and respond to deterioration, particularly in community settings and for people at higher risk. This includes timely escalation to acute services, as well as recognising when deterioration is part of end-of-life care and respecting people’s wishes.
We will design and implement a national improvement programme focused on deterioration management in the community for high-risk groups and settings.
This programme will take an all-cause approach, including the use of early warning scores in community settings such as care homes, nursing homes, domiciliary care, at home, primary care, community hospitals and mental health settings. It will link infection response functions referenced in Action 7, as relevant.
Priority tasks:
- design and implement a national improvement programme to support NHS community and primary care providers to manage physical deterioration more effectively, focusing on people at higher risk; this will include:
- how to interpret ‘soft signs’ (including carer concern)
- using Early Warning Scores where relevant
- avoiding diagnostic overshadowing (short-term)
- explore how data on repeated contacts over a short period might help quickly identify patients at risk and direct them to the right care setting, supporting clinicians to:
- prioritise patients who need urgent investigations and interventions
- improve the speed and accuracy of diagnosing deterioration (short-term)
Action 11: improve use of physiological observations, including early warning systems (EWS)
MEWS, NEWTT2, PEWS, NEWS2 and RESTORE2 are all used to support identification and response to acute patient deterioration. However, their use can be limited, inconsistent or inaccurate.
There are opportunities to improve how these systems are used across settings, from primary care through to ambulance services, emergency departments and hospitals. This work involves:
- training
- quality improvement support
- incentives
- ensuring systematic handover processes
Priority tasks:
- create Information Standards Notice requirements to standardise digital specifications for all early warning systems and support integration into electronic patient record systems (immediate)
- work with clinical experts, UKHSA, royal colleges and professional associations to:
- clarify the use of early warning systems in specific patients
- understand what improvements may be appropriate for early warning indicators, such as including risk factors linked with inequalities
- consider what the roll-out of Martha’s Rule tells us about the important role carers and patients can play in identifying deterioration, for example, through routine use of patient wellness questionnaires
- understand how non-acute settings could better use early warning systems (short or medium-term)
- explore the use of wearable and other technologies for high-risk groups and those with suspected infections to support physiological monitoring for early warning systems in community settings, social care and primary care (long-term)
- initiate pilots and use evidence from existing deployments and large‑scale programmes in other conditions to assess the clinical and cost‑effectiveness of wearable and remote monitoring technologies; this will examine whether they improve timely recognition of deterioration and support escalation of care within defined clinical pathways, including in community and primary care (long-term)
Action 12: provide sufficient critical and enhanced care capacity
Prompt treatment saves lives. Where advanced therapies are delayed, for example, due to a lack of available critical care beds, research shows patients are at increased risk of poor outcomes.
One of the initial advanced therapies for sepsis patients is peripherally-administered vasopressors. While these can be delivered outside critical care, safe delivery requires a higher level of monitoring than may be available in emergency departments or general wards. This has led to a consensus by stakeholders that more enhanced (Level 1) care capacity is needed across parts of the country.
We are working to understand whether patients have equitable access to this type of service across different providers. While critical care outreach teams can support these patients, provision is variable and not currently recommended as a standard in existing NICE or commissioning guidance.
Priority tasks:
- examine variation in outreach, enhanced, critical care and step-down capacity, and explore the need for standardising bed numbers by head of population, accounting for case-mix and factors such as population socioeconomic status (immediate)
- provide implementation support to address gaps in capacity, including:
- development of diagnostic blueprints to inform service transformation
- business cases for capital investment in estates and equipment, as well as training and education as part of the upcoming NHS 10 Year Workforce Plan (medium-term)
3.6 Response that is timely, appropriate and effective
Action 13: develop precision-medicine approaches to sepsis care
Our first theme, personalised care, highlighted the opportunity to develop precision-medicine approaches to sepsis care. Beyond antimicrobial prescription and organ support, there may be further opportunities to reduce the morbidity and mortality, particularly through immunomodulatory approaches.
However, decades of clinical trials, including studies of corticosteroids and more complex immunotherapies, have not identified clinically effective approaches.
One explanation may be that some patient groups, who we could identify using genomics and deep clinical phenotyping, respond differently to these interventions. Similarly, advances in genomic pathogen testing, ranging from point-of-care tests (including biosensors for identification of host response to the pathogen) to whole-genome sequencing, have the potential to help identify subgroups of pathogens that are more susceptible to certain treatments.
Priority tasks:
- work with Health Innovation Networks, HealthTech Research Centres, UKHSA, commissioners and providers to evaluate and adopt diagnostic innovations, such as point-of-care genomic sequencing to rapidly detect pathogens, antimicrobial resistance profiles and likely host response; this would align with the creation of a sepsis diagnostics accelerator and infection diagnostics directory and will also build on the NHS genomics network of excellence in respiratory metagenomics and severe infection, the outcomes of which will move into NHS commissioning (medium-term)
- work with industry, academia and research funders to develop and evaluate precision interventions across the care pathway, not limited to antimicrobials, which will reduce the risk of poor outcomes, including organ failure (long-term)
Action 14: improve access to post-discharge support, including rehabilitation
People who survive sepsis can experience a range of long-term physical, psychological and cognitive health consequences, as outlined by The UK Sepsis Trust.
Research shows that more than half of adults discharged after a critical care admission for sepsis are either readmitted as an emergency or die within 1 year. Risk factors for poorer longer-term outcomes in adults include:
- increasing age
- poor health status before the sepsis episode
- living in areas of high socioeconomic deprivation
Readmission to hospital is most common within 30 days of initial discharge, yet most post-critical care follow-up clinics do not see patients until around 3 months after discharge.
Sepsis is a common reason for critical care admission, and recent data has highlighted a significant gap in the assessment and delivery of rehabilitation for critical care survivors. There is therefore a need for improved post-sepsis care.
In the short term, this may include measures such as enhanced surveillance, step-down care, hospital at home, and active support (not just passive surveillance). In the medium to longer term, patients should have access to comprehensive rehabilitation support, including psychological support and improved links to social care to improve post-sepsis care among the most vulnerable.
Priority tasks:
- scope current provision of post-sepsis care in the early days and weeks after discharge to identify effective clinical interventions, safety netting or research needs (short-term)
- consider how to improve the needs assessment, planning and delivery of holistic rehabilitation and multidisciplinary follow-up and monitoring after critical illness, including psychological support, for all patients, including those with sepsis; we will also explore supporting this work with a best practice tariff or ‘year of care’ payment (see Section 6) (short and medium-term)
- evaluate opportunities to improve longer-term monitoring and support of those recovering from sepsis, including earlier transfer of care as close to home as possible, supported by devices and techniques to monitor longer-term change as part of a new sepsis research and innovation action plan working with relevant researchers and industry (see Section 5) (medium and long-term)
“There were so many after effects. My skin started peeling off… My nails were crumbling. I had handfuls of hair falling out. On the first day back [from hospital], I went downstairs and I was trying to make a cup of tea… And I was like what do I do now? I couldn’t figure out how to make this cup of tea. It just took so much energy and processing to be able to do it.” – Kate, sepsis survivor, as told to the UK Sepsis Trust
4. Priority actions for sepsis innovation and research
Achieving the outcomes set out in this framework will require significant advances in science, technology, data and analytics.
Working with the National Institute for Health and Care Research (NIHR) and system partners, we will deliver a paradigm shift in sepsis care underpinned by research and innovation to provide the evidence base for change.
4.1 Working with partners
The UK has a strong research and innovation infrastructure bringing together the NIHR, academia, industry and NHS partners, including:
- the NIHR-Research Delivery Network
- the UK Biobank
- the UK Health Security Agency
- Health Innovation Networks
- Our Future Health
- NHS Genomic Medicine Service
- the Genomics England knowledge base
- data platforms such as OpenSafely
- the connectivity of NHS organisations and their data
During COVID-19, our research infrastructure enabled rapid progress in sequencing the virus, understanding the host response, identifying treatments and delivering large-scale clinical trials.
With sepsis, we need to take a similarly ambitious approach. Using these capabilities, we can move towards personalised prevention and treatment, based on genomic, epigenetic and deep phenotypic characterisation coupled with immune and immunological factors, pathogen characterisation, susceptibility status, biomarkers, clinical and behavioural factors.
The pace of innovation is rapid, particularly when it comes to AI-driven interventions. Recent horizon scanning by the NIHR Innovation Observatory highlighted current and developing innovations that could improve sepsis care, including:
- tests that can detect biomarkers of infection
- molecular tests including metagenomics to detect pathogens or sensitivity or resistance markers to antibiotics
- rapid multiplex point of care testing (POCT)
- microfluidic, cellular or peptide-based technologies
International collaboration
We want to increase international collaboration. For example, we will explore opportunities to collaborate with the PROMETHEUS programme in France to reach definitive conclusions on sepsis-related research questions as soon as possible.
4.2 Our approach to innovation and research
Develop a national research and innovation action plan for sepsis
We will work with NIHR, academia, industry, and the Health Innovation Networks, Health Informatics Collaboratives and partners, to develop a national research and innovation action plan for sepsis.
This will focus on the research and innovation opportunities identified during the development of this framework. Work on the action plan will begin immediately, based on the outline below.
Working with the same partners, we will accelerate the implementation and real-world evaluation of technologies that can improve sepsis care.
Our action plan will build on existing work in this area, most notably the James Lind Alliance Priority Setting Partnership (JLA-PSP) top 10 priority list.
Key sepsis research priorities identified by the James Lind Alliance
- How can the diagnosis of sepsis become faster, more accurate and reliable?
- What are the long-term effects on the body from sepsis (sometimes called post-sepsis syndrome)? How are these long-term effects best treated and managed?
- What is the role of treatments other than antibiotics in the care and management of sepsis?
- Can diagnostic tests be developed for sepsis that can be used wherever the person is receiving care (for example, in a GP surgery, hospital, ambulance or at home)?
- Why and how do some people with sepsis become seriously ill very quickly?
- Would specialist sepsis services improve outcomes for people with sepsis during hospital treatment and for follow-up care?
- Are there ways to tailor treatment of sepsis to the individual (for example, based on blood markers or other indicators)?
- How does an infection lead to sepsis?
- Would treatment before admission to hospital (for example, provided by GPs or ambulance crews) improve outcomes for people with sepsis?
- What are the safest and most effective ways to treat sepsis using antibiotics?
However, the scope of our research and innovation questions extends beyond the James Lind Alliance priorities.
Development of the action plan will be a collaborative effort with academic experts and research funders. We will commission themed calls based on the research and innovation priority areas in Section 4.3 below.
This work builds on the research ambitions set out in the 10 Year Health Plan and involves:
- assessing the feasibility of supporting a national multi-arm, multi-stage platform clinical trial for sepsis diagnostic tests and interventions, including sub-group trials for specific host and pathogen phenotypes
- developing the required infrastructure to enable wider participation in clinical trials and other types of research aimed at improving sepsis care and outcomes, such as biobanking, workforce, and safe access to clinical and operational data
- improving participation in sepsis-related research from under-represented groups
- developing research capability and capacity across diverse professional groups, including healthcare science, nursing, pharmacy and allied health professions, to lead and deliver sepsis-related research
- embedding sepsis-related clinical trials more effectively within the digital infrastructure of the NHS, including:
- using primary and secondary care electronic health records
- considering innovative and accelerative approaches to diagnostics, such as point-of-care randomisation and collection of real-world evidence
- developing the human capacity and systems to deliver this
- supporting sepsis-related research across the entire care pathway, including primary and community care, before and after sepsis
Accelerate implementation
We must ensure novel evidence-based technologies are provided to patients as quickly as possible, while generating effectiveness data from real-world evaluations.
We will support locally led implementation across all care settings through combined clinical and technological leadership, and financial and system leverage.
Working with the NIHR, Regional Health Innovation Zones, the Health Innovation Networks and others, we will:
- undertake regular horizon scanning to drive targeted action for implementation and rollout of innovations, particularly in priority areas such as acute deterioration, prediction, monitoring and cost-effectiveness of care
- establish innovation collaboratives and clinical evidence scoring frameworks to share best practice and de-escalation strategies for tests that are superseded
- develop target product profiles (TPP) for diagnostic tests for different points in care pathways for both sepsis and wider infection, working with industry partners and regulators and supporting alignment with clinical needs
- improve health economic analysis, working with NICE and research bodies to update cost-benefit models to reflect whole care pathways and ensure that studies include health economic analysis to better support adoption decisions of innovations
- use metrics to monitor clinical utility and impact of innovations to support effective implementation
- establish a rapid diagnostics and POCT programme to accelerate development, evaluations and evidence-based adoption of the use of POCT in both community and hospital settings; this should involve:
- clinicians
- academics
- patients and the public
- industry
- NICE
- Medicines and Healthcare products Regulatory Agency
- NIHR’s i4i programme
- Health Innovation Networks
- working with NICE to support relevant HealthTech evaluations, including assessing innovations for early use
4.3 Research and innovation priority areas
We have identified 6 priority areas for research and innovation:
- prevention, including vaccination and screening
- prediction
- monitoring
- diagnostics
- intervention
- improving awareness, education and training
These priority areas will form the basis of the research and innovation action plan for sepsis, co-designed with partners.
5. How we will measure progress
5.1 Sepsis
We will establish an authoritative, evidence-based set of clinical diagnosis codes that reliably identify infection and sepsis admissions using NHS administrative datasets.
This will allow us to:
- understand sepsis prevalence across England
- track changes over time and assess the impact of initiatives under this framework
- link sepsis data with other data, such as patient demographics and co-morbidities
5.2 Severe infection
We define ‘severe infection’ as any episode of hospitalisation with an infection.
For this measure, hospitalisation includes treatment at home in virtual wards, reflecting the strategic shift from hospital to community care.
5.3 Mortality
We will measure mortality associated with sepsis or infection using data from death certificates published by the Office for National Statistics (ONS).
Because deaths from infection are often recorded in different ways on death certificates, most deaths attributed to infection will in practice be due to sepsis, although there are some exceptions (for example, thrombotic stroke because of infective endocarditis). In most cases, the underlying cause of death will be a dysregulated host response to infection leading to organ failure: that is sepsis.
Given the context of advanced care planning and to ensure meaningful measurement, we will establish processes that exclude deaths where it was clinically appropriate not to deliver higher-intensity treatments, such as critical care organ support. This is likely to include all deaths from infection where there was no admission to hospital or critical care, as long as a medical examiner or coroner has not raised concerns about the care and treatment pathway.
5.4 Life-threatening complications
We define life-threatening complications from sepsis as any episode where a patient is admitted for at least single organ support to a critical care unit.
This data is available from existing national audits and administrative data.
The requirement for organ support is important in this definition – some patients with sepsis might appropriately be admitted to critical care for monitoring if they are at high risk of deterioration, without the need for organ support; this could be considered a marker of high-quality care and would not be included in this statistic.
5.5 Long-term impact
Patients who survive sepsis often leave hospital with new and ongoing health issues and are at high risk of being readmitted.
We will assess aspects of morbidity and longer-term mortality by:
- measuring ‘Days Alive and Out of Hospital’ (DAOH) at 1 year for patients admitted to critical care with a primary infection diagnosis
- tracking rates of hospital readmission within 90 days of discharge, with the aim of reducing this
To better understand longer-term outcomes for people who have not been readmitted, we will also explore:
- the use of primary and community care data
- the use of patient reported outcome measures (PROMs) and patient reported experience measures (PREMs)
5.6 Supporting metrics
We are establishing a suite of supporting metrics to help track the implementation and impact of the framework.
This will include:
- variation in level 1 (enhanced care) and level 2 and 3 (high dependency and intensive care – collectively known as critical care) capacity for adults, children (paediatric intensive care [PICU]) and neonates (neonatal intensive care [NICU])
- analysis of sepsis outcomes by causative infectious agent, antimicrobial resistance and infection source (for example, community-acquired or healthcare-associated) and, in due course, by any other objective biomarker-based stratification
- outcome metrics, such as length of stay, emergency admissions and 30-day readmissions
- early warning mechanisms to identify services starting to demonstrate a decline in patient outcomes, similar to the Maternity Outcomes Signalling System (MOSS)
- balancing metrics, such as data on antimicrobial resistance and prescribing rates
- measuring processes, such as timely antibiotic administration and antibiotic review, and time to blood culture result or to point of care diagnostic result that guides the next stage of management
- improving our understanding of sepsis in non-clinical settings, by considering relevant metrics that may apply in the adult social care sector and others
This work aligns with the potential development of a new national infection and sepsis audit, ensuring we make use of data that is available from existing clinical audits.
5.7 Health economic analysis
As an immediate priority, we will use our improved understanding of the demand, acuity, activity and outcomes associated with infection and sepsis, and commission a full health economic analysis of the costs and benefits of sepsis care and treatment.
This will help us identify future priority actions and assess the framework over time.
6. How we will deliver improvement
6.1 Innovation, improvement and assurance
The framework’s longer-term ambitions will be supported by research and innovation (see Priority actions for sepsis innovation and research).
In the shorter term, we will focus on ensuring that every patient who develops sepsis reliably receives high-quality care – no matter the time or day – across every care setting. This will require providers to improve adherence to existing standards, thereby reducing unwarranted variation.
We will achieve this through nationally led, locally delivered improvement programmes focusing on:
- community infection prevention and management (Action 7)
- community deterioration management (Action 10)
- optimising the acute management of sepsis (Action 9)
These programmes will support our staff to deliver better care through improved adherence to critical processes. They will also address organisational (including cultural) challenges to delivering what we know good looks like, such as hierarchy gradients, that can be very context- or service-specific.
We will learn from best practice and embed research and evidence generation as part of the improvement activity, so that we accelerate the spread and adoption of effective, innovative approaches both in NHS and social care services.
6.2 Financial levers
Best practice tariffs (BPTs), alongside carefully designed audit and data collection, offer an opportunity to enhance sepsis care.
BPTs provide incentives for delivering best practice by setting higher prices for activity that achieves the tariff criteria. They do not change the total amount of money for a service, so the higher BPT price is paid for by a corresponding reduction in the non-BPT price.
Under the Sepsis modern service framework, we will develop proposals for sepsis BPTs to be introduced the NHS from 2027/28. We will consider approaches that span both acute and community care.
In time, we will also consider a tariff or a ‘year of care’ payment model to support ongoing patient needs after critical illness, including post-sepsis. We will also explore similar approaches for the prevention of sepsis and wider infection, subject to further discussion. These incentives will link to other actions to improve acute care and post-sepsis support.
6.3 Data and measurement
High-quality, timely data underpins both quality improvement and financial levers.
As set out in Action 4, we will commission a new national infection and sepsis audit. This will work alongside existing audits and incorporate emerging measures of quality, such as relevant PROMs and PREMs, to significantly improve our understanding of infection and sepsis care.
Because the incidence of sepsis in primary care is very low, we will explore the potential for retrospective analysis of care in community settings, focusing on patients later admitted to hospital with severe infections and sepsis.
Our data and measurement strategy (as outlined in Section 5) will enable us to:
- explore variation
- implement near-real time feedback systems for surveillance, providing early warning alarms for organisations where performance may be dropping
- increase transparency
- track progress and impact
This can lead to supportive, focused improvement activities to address gaps in quality of care.
6.4 Capacity
We need to address variation in system capacity to manage and treat infection and sepsis. Important areas of focus include:
- enhanced care (level 1) and critical care (level 2 and 3) capacity
- children and young people’s emergency department services
- options to appropriately treat patients in the community
There are also wider system pressures, including the impact of emergency department demand on patient discharge from critical care, as well as the capacity to see patients with infection on the same day in the community.
We know that there is no quick fix to these capacity challenges. While significant expansion of acute capacity is unlikely, there is an opportunity to better understand and reduce unwarranted variation and to set clearer expectations for service provision based on population need.
6.5 Workforce
Several workforce challenges have been highlighted while creating this framework.
These challenges include the need to clarify the seniority and qualifications required to care for specific patient groups or lead triage and initial decision-making (for example, whether children and young people always need paediatric-trained clinicians). They also include the numbers of existing staff groups considered key to sepsis care, such as:
- call handlers
- healthcare scientists
- social care staff
- community infection, prevention and control team
- critical care staff including outreach teams.
Workforce planning for the NHS should not be undertaken in isolation through individual frameworks. We will therefore work with the NHS 10 Year Workforce Planning team to assess and address relevant workforce requirements for sepsis care.
6.6 Training and education
Clear expectations for and access to relevant training and education programmes are critical to improving infection and sepsis care.
As set out in action 5, we will undertake work to review, align and clarify the training and education expectations related to sepsis, infection prevention and control and deterioration management across the workforce, including social care, clinical and non-clinical staff, and those in leadership roles.
6.7 Digital
The NHS is moving from analogue to digital and taking a digital-first approach to all its work. Digital inventions offer significant opportunities to improve sepsis care.
A high-level digital roadmap will detail the required developments and the likely timescales (see Appendix A). We can group these into the following categories:
- digital and data infrastructure – including work on the single patient record, FDP, linked primary–secondary–community datasets, electronic patient records and interoperability (Action 1, Action 2, Action 4)
- digital risk stratification, analysis, decision support – including predictive analytics, machine learning‑driven phenotyping, AI‑enabled decision support, tracking of repeat presentation (Action 1, Action 8, Action 9)
- digital diagnostics – including integrating POCT and genomics and other -omics, digitally enabled rapid POCT, pathogen sequencing, digital integration of results into electronic patient records (Action 8, Section 4)
- digital deterioration detection – including digital EWS standards, wearables and continuous monitoring, community deterioration management (Action 10, Action 11)
- data, audit and standards – including the new national infection and sepsis audit, near‑real‑time feedback and surveillance systems, coding quality and benchmarking (Action 4, Section 5)
- citizen‑ and clinician‑facing digital – including shared care records, digital advance care plans and treatment escalation plans and NHS App integration (Action 1, Action 2)
6.8 Regulation
Our improvement efforts will be underpinned by clear, agreed minimum standards and expectations. This will support the Care Quality Commission (CQC) and other regulators to reinforce our work, including efforts to drive and support innovation.
6.9 Communications
As described under Action 3, we will develop a new, targeted communications campaign and associated strategies to support infection and sepsis prevention, identification, escalation and response.
This will include both direct communications to raise awareness of sepsis and indirect communications, such as promoting vaccine uptake. We will target those groups most at risk through public-facing activity, carers and staff. We will work with a range of expert stakeholders to help us engage specific target audiences.
6.10 Innovation pipeline
Section 4 sets out our research and innovation approach. We will work with industry, healthcare and academia to develop, test and spread innovations that will deliver high-quality care for everyone.
7. Next steps
This is a 10-year plan for delivering a step change in the management of sepsis in England. While ambitious, it begins by improving what we do now while supporting long-term innovation.
Delivery of these plans will be the responsibility of NHS England (while it remains in operation) and the Department of Health and Social Care, working with partner organisations and stakeholders.
A Sepsis Modern Service Framework Implementation Steering Group will oversee delivery of the plan, accountable to senior leadership of NHS England, DHSC and ministers. Its membership will be drawn from:
- those leading delivery
- wider stakeholders
- patient representatives
The modern service framework will not be static. Its themes, actions and priority tasks will be kept under continuous review and will flex as our understanding of how to improve sepsis care develops and the wider NHS changes.
We will review and, if necessary, update the framework on an annual basis, ensuring the regular publication of data and insights.
Appendix A: digital roadmap
This roadmap provides a high-level overview of the actions, recommendations and timelines related to digital infrastructure in this framework.
Immediate (within 1 year): foundational digital enablers
Data, audit and standards
- Commission a new national infection and sepsis audit, initially in the acute sector, with digital data collection and reporting as the core mechanism (Action 4).
- Establish minimum digital information standards for early warning systems to ensure consistent implementation across electronic patient record systems (Action 11).
- Examine variation in enhanced and critical care capacity using national data, including digital benchmarking and analytics to identify gaps (Action 12).
- Ensure sepsis, infection, antimicrobial resistance and deterioration guidance is digitally curated, consistent and easy to access, rather than fragmented across platforms (Action 5).
Why this matters
These actions create the data backbone (audit, standards and interoperability) without which later AI, diagnostics and monitoring ambitions cannot be delivered at scale.
Short‑term (within 2 to 3 years): main window for digital improvement
Digital risk stratification, analysis and decision support
- Develop and validate sepsis risk prediction and stratification tools, aligned with NICE guidance and supported by analytics and machine learning (Action 1).
Data, audit and standards
- Link primary, secondary and community care datasets to understand pathways, delays, outcomes and inequalities and detect outliers (Action 4).
Digital deterioration detection
- Build on the Community Deterioration Management improvement programme to look at using digital early warning systems and embedding patient and carer‑reported concerns where appropriate (Action 10 and Action 11).
Digital diagnostics, point-of-care tests, genomics and other -omics
- Develop, assess and implement near‑patient and rapid diagnostic tools, digitally integrating results into clinical records (Action 8).
Why this matters
Short‑term actions focus on using data better: connecting it, feeding it back faster and embedding it into everyday clinical decisions.
Medium‑term (within 4 to 5 years): scaling and maturing the digital infrastructure
Digital and data infrastructure
- Maximise the use of the Federated Data Platform for large‑scale analysis of infection and sepsis data, including equity and outcomes analysis (Action 1, Section 5).
Citizen‑ and clinician‑facing digital
- Flag patients at risk of sepsis in the single patient record, including prior infections, pathogens and antimicrobial sensitivities (Action 1).
- Enable digital sharing of support advance care plans and treatment escalation plans through shared care records, ensuring availability across primary, community and acute care (Action 2).
- Explore digital PROMs and PREMs to capture longer‑term patient experience and recovery after sepsis (Section 5 and Action 4).
Data, audit and standards
- Use administrative data to track longer‑term outcomes, including Days Alive and Out of Hospital (DAOH) and readmissions (Section 5).
Why this matters
Medium‑term actions turn early digital wins into system‑level capabilities that support population management and accountability.
Long‑term (within 10 years): transformational digital ambition
Digital diagnostics, point-of-care tests, genomics and other -omics
- Use deep phenotyping, –omics and machine learning to enable personalised prediction, diagnosis and treatment of sepsis (Action 1 and Action 13).
- Implement genomic pathogen testing and sequencing at pace, with digital integration into routine care pathways and surveillance systems (Action 8 and Section 4).
Digital risk stratification, analysis, decision support
- Develop AI‑enabled clinical decision-support systems, integrating host response, pathogen data and patient risk profiles (Section 4).
Digital deterioration detection
- Deploy wearable and continuous monitoring tech, supported by integrated digital systems and AI, to detect deterioration earlier across all settings (Action 11).
Digital and data infrastructure
- Embed sepsis research and trials into NHS digital infrastructure, including point‑of‑care randomisation and real‑world evidence generation (Section 4).
Why this matters
Shifting care from reactive to predictive, personalised and digitally enabled.
Appendix B: context and evidence
This appendix summarises the context and evidence underpinning the framework, including the nature of sepsis, its impact on patients and services, and variation in outcomes.
Sepsis is complex, hard to diagnose and has significant impacts on people
Sepsis is a serious, time-sensitive condition that occurs when the body’s response to an infection leads to tissue and organ injury.
Sepsis is unusual, and most infections do not cause sepsis, but it can be triggered by any kind of infection. It can be challenging for clinicians to distinguish between different types of infection, and to identify where in the body the infection originated, which may include the lungs, urinary tract, gastrointestinal tract and skin. Sepsis can also start with infections at surgical sites, central lines and other breaches of skin integrity as well as from other indwelling devices such as catheters and pacemakers.
Sepsis involves an abnormal immune response and can quickly affect multiple organs and systems. Sepsis can disrupt the usual balance of oxygen supply and demand in major organs, leading to organ malfunction and, sometimes, failure. It is this organ failure that can then cause serious illness, and in some cases, death.
There is no single, simple test for sepsis, and the range of possible sepsis symptoms overlaps with those of other conditions. To identify sepsis, clinicians need to diagnose organ dysfunction and infection.
Clinicians use vital sign measurements (for example, heart and respiratory rates) and some bedside tests (for example, oxygen saturations and blood pressure) to evaluate for organ dysfunction. These signs are brought together in early warning systems, such as NEWS2, to identify patients at risk of clinical deterioration, regardless of cause.
Diagnosing infection can be challenging because we have no completely sensitive or specific diagnostic tests that provide immediate or rapid results and can be used reliably for monitoring. Just because someone has signs of organ dysfunction, this does not mean they have sepsis.
If infection is suspected, clinicians need to make quick, accurate decisions about whether it is caused by a bacterium, virus, or fungus, so they can use the appropriate treatment and avoid prescribing antibiotics to patients who do not need them, thereby reducing the risk of antimicrobial resistance.
In children and infants in particular, it can be difficult to distinguish between self-limited and serious infections.
When sepsis is suspected, clinicians will start treatment with broad-spectrum antibiotics. Once the source and type of infection are confirmed, more targeted antibiotics are used instead.
Not all cases of sepsis, or deaths from sepsis, are preventable. A significant proportion of sepsis deaths are associated with existing comorbidities or severe frailty, and some happen despite appropriate, high-quality care. Some people will also prefer not to receive invasive and intensive organ support if they are nearing the end of their lives.
For those who recover, sepsis can have long-term effects on both physical and mental health. These can last for months or years and may include:
- feeling very tired and weak, loss of appetite and difficulty sleeping
- getting ill more often, including repeat episodes of sepsis
- changes in mood, anxiety, depression or post-traumatic stress disorder (PTSD)
Some people may need both physical and psychological support. Recent evaluations suggest that there is an unmet need in how the NHS supports survivors of critical illness with rehabilitation. This framework therefore also considers post-sepsis care, not just the prevention and treatment of sepsis itself.
“Recovery is life long, not just getting home. Recovery doesn’t stop once home.’’ – Jeremy, sepsis survivor
Sepsis affects different groups unequally
Sepsis, or poor outcomes from sepsis, are more common in some patient groups. Risk factors are not completely understood but are unavoidable in many cases. Sepsis is more likely in those who are immunocompromised for any reason, for example people at the extremes of age (babies and older people). Older people in particular are far more likely to experience infections and to die from sepsis than other groups.
Figure 1: Deaths due to sepsis by age group
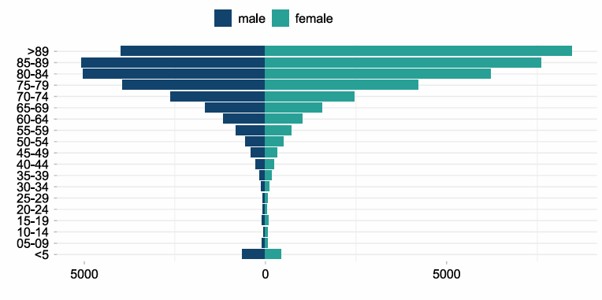
Chart description: Figure 1 shows that deaths involving sepsis are concentrated in older age groups. The highest numbers for females are in those aged over 89, with around 8,000 deaths. The highest numbers for males are in those aged 85 to 89, with around 5,000 deaths.
In most older age groups, more deaths are recorded in females than in males. Numbers fall steadily with decreasing age and are very low below age 40, although there is a small increase in the number of deaths in children under 5.
Others at higher risk include:
- people taking immunosuppressant medications
- people with impaired immune systems, for example, due to genetic factors or long-term conditions such as diabetes, chronic liver disease or sickle cell disease
- people who have recently had surgery, as wound infection at the surgical site and the physiological demand of major surgery can increase the risk of sepsis
However, for some people, while there is no clinical reason for them to be at higher risk, they still experience sepsis more often or are more likely to die or incur serious or long-lasting complications from it. This includes:
- people living in more deprived areas
- people with serious mental illness
- people experiencing homelessness
- some people with a learning disability or autistic people
Research on risk factors for non-COVID-19 related sepsis deaths in the UK during the pandemic found that the risk of death for people with a learning disability, even when adjusted for other risk factors, was more than 3.5 times the baseline. This was a much higher risk than was associated with cancer, or most other long-term clinical conditions. People with severe mental illness also had over twice the risk of death from non-COVID-19 sepsis.
This increased risk is likely due to a range of factors, including:
- the accessibility and availability of services
- delays in presentation
- challenges with carrying out observations and clinical history taking
- diagnostic overshadowing, where clinicians may consider that symptoms relate to pre-existing conditions rather than infection or sepsis
For some groups, both clinical and non-clinical risk factors will contribute to their risk. For example, some people with a learning or physical disability may have clinical conditions that increase their risk of infection and sepsis, while also experiencing less accessible services or diagnostic overshadowing.
Summary of sepsis risk factors
Age-related considerations:
- babies under 1, particularly if they’re born prematurely or their mother had an infection while pregnant
- women who have just given birth, had a miscarriage or had an abortion
- those who are 75 or over
Clinical history (acute and long-term):
- people with clinical features such as:
- frailty
- multimorbidity or poorly controlled long-term conditions such as diabetes
- impaired immune function because of illness, including cancer or heart failure, or immunosuppression due to medical treatment
- surgery or invasive procedures in the past 6 weeks
- indwelling urinary catheters or other invasive lines
- repeated antibiotic use
- breach of skin integrity
People at high risk of health inequalities:
- people from an ethnic minority background
- people who need an interpreter
- people with a learning disability and autistic people
- people with severe mental illness
- people with cognitive impairment
- people with drug or alcohol dependency
- people experiencing homelessness
- people living in more deprived areas
Sepsis and infection lead to significant healthcare activity and cost
In addition to the human cost, sepsis places significant pressure on health and care services.
There were 133,484 hospital admissions (all ages) in 2024/25 recorded with a primary diagnosis of sepsis. This is unlikely to be an underestimation. The mean length of stay for these admissions was 14 days. If secondary sepsis diagnoses are included, the number of sepsis admissions recorded is almost 250,000.
Sepsis also impacts critical care activity. In 2024/25, 10% of inpatient spells with a primary diagnosis of sepsis resulted in admission to critical care, with 32% requiring level 3 critical care. The mean length of stay in critical care (all levels) was 7 days. Overall, 4.4% of inpatient spells involving a critical care admission in 2024/25 had a primary diagnosis of sepsis, rising to 12.2% when all sepsis diagnoses are included, with a mean length of stay of 11 days.
More broadly, bacterial infections – the most common cause of sepsis – were recorded as the primary diagnosis during the inpatient spell for around 1.4 million emergency admissions in 2024/25, which is 22% of all emergency admissions. When all diagnoses and admission types are included, the total increases to around 2.7 million admissions, reflecting 15% of all admissions.
Admission volumes for key infections are shown in Table 1. For example, there were 359,323 admissions with a primary diagnosis of pneumonia during the inpatient spell in 2024/25.
Table 1. Counts of admissions for key infections in 2024/25
Source: Hospital Episode Statistics (see Technical annex: hospital admitted patient care and critical care activity)
| Infection type | Emergency admissions with a primary diagnosis | All admissions with any diagnosis |
| Urinary tract infection | 147,173 | 422,306 |
| Pneumonia | 359,323 | 629,400 |
| Upper respiratory tract infection | 41,321 | 57,710 |
| Lower respiratory tract infection | 132,051 | 257,744 |
| Gastrointestinal infections | 128,065 | 355,525 |
| Cellulitis | 88,216 | 206,222 |
| Surgical site infections | 56,701 | 135,251 |
Around 20% of patients with an emergency admission and a primary diagnosis of sepsis died.
6% of hospital deaths with a primary diagnosis of sepsis are related to ‘surgical’ sepsis, compared with 92% relating to ‘medical’ sepsis (2024/25, based on treatment function definitions). Figures do not sum to 100% because some treatment functions, including paediatrics, have not been classified as medical or surgical (see Technical annex: hospital admitted patient care and critical care activity).
Sepsis is expensive to treat. It often requires long hospital stays, critical care admission, and a long period of rehabilitation. During recovery, people may be unable to support themselves and contribute to the economy. Sepsis care cost £1.037 billion in 2024/25 and had wider economic costs, including lost productivity, social care and other costs.
A study of sepsis in Wales showed that 55.2% of patients died within 3 years of their first admission, with around a quarter (24.7%) dying within 7 days of the index admission.
Data from NHS Resolution shows that 696 clinical negligence claims were received between 2020/21 and 2024/25 where the primary injury was sepsis. The total cost of these claims was £32.2 million.
More broadly, there were 1,346 claims where any injury was sepsis, with a total cost of £65.3 million. Emergency medicine accounted for 31% of the cost of claims in which any injury was related to sepsis (the largest single category).
Failures or delays in treatment or diagnosis accounted for almost all of the primary causes cited.
There is variation in sepsis outcomes
There have been multiple high-profile efforts to improve sepsis care and outcomes, including the Surviving Sepsis Campaign, the use of care ‘bundles’ and the development by NICE of comprehensive sepsis guidance and quality standards for adults, children and in pregnancy. However, sepsis outcomes remain variable across the NHS.
For example, mortality varies between regions (see figure 2). Note that comparisons between NHS organisations are limited by data challenges, and age-standardised mortality rates between regions cannot be readily adjusted for known risk factors other than age and sex.
Figure 2. Age-standardised mortality rates per 100,000 population by region from sepsis in 2025
Data source: Civil Registrations of Death. See Technical annex: age-standardised mortality rates for definitions used.
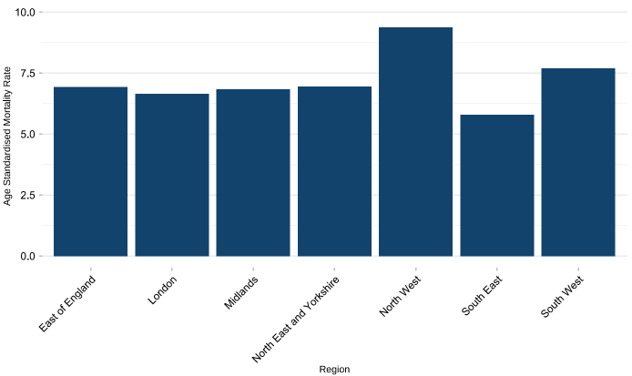
Chart description: The bar chart shows age-standardised mortality rates for sepsis by region in 2025. The North West has the highest rate, at around 9 deaths per 100,000 population, followed by the South West at around 8 deaths per 100,000 population. Most other regions, including the Midlands, North East and Yorkshire, East of England and London, are clustered between around 6 and 7. The South East has the lowest rate, at just under 6.
Sepsis mortality also varies between hospital trusts. The Summary Hospital-level Mortality Indicator (SHMI) adjusts for patient risk factors. The SHMI for the diagnosis group named ‘Septicaemia (except in labour), Shock’ shows that some hospitals have a higher-than-expected number of deaths, while others have a lower number than expected. This requires further investigation, and the data must be treated with some caution given challenges that exist, including coding variation.
We need to improve our sepsis data
Analysis of variation in sepsis care is difficult because the data collected has changed over time and varies between organisations. There are also differences in how infection, sepsis and some outcomes are recorded globally, which make international comparisons difficult.
Recent work to improve how sepsis diagnoses are recorded in the NHS was associated with a doubling of the number of recorded emergency admissions with a diagnosis of sepsis between 2016/17 and 2017/18 (figure 3a), with an even greater increase seen in admissions with a primary diagnosis of sepsis (figure 3b). The COVID-19 pandemic has also had a significant effect on the number of sepsis cases recorded over time (figures 3a and 3b)
Figure 3a. Admissions with any diagnosis of sepsis, by financial year and admission method
Source: Hospital Episode Statistics (see Technical annex: hospital admitted patient care and critical care activity).
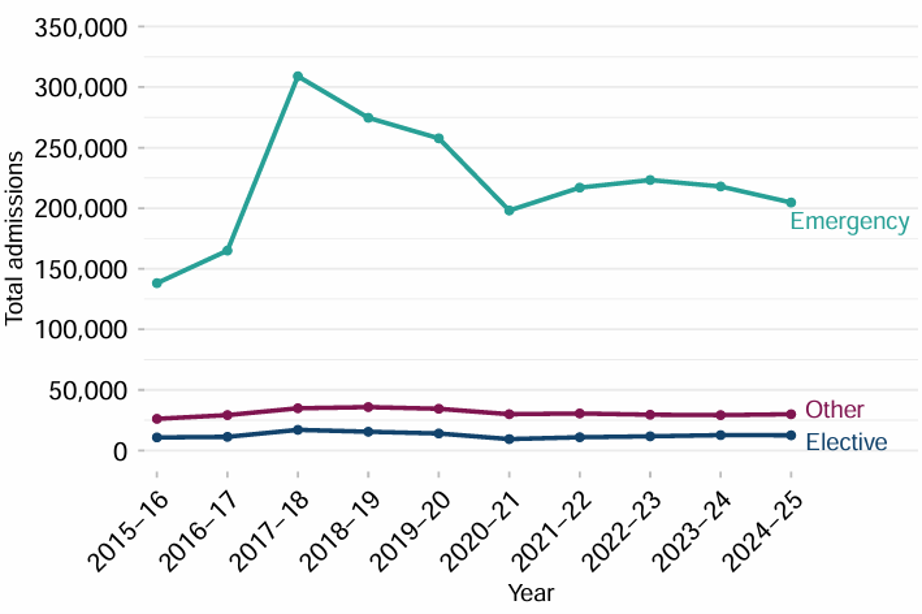
Chart description: Figure 3a shows the total number of admissions with any diagnosis of sepsis in each financial year from 2015/16 to 2024/25, split by elective, emergency or other admission methods. Elective admissions are relatively stable, with around 10,000 to 20,000 each year. Other admissions are also stable, varying between around 25,000 and 40,000 each year. Emergency admission numbers are very variable, rising sharply from around 140,000 in 2015/16 to over 300,000 in 2017/18, then declining to around 200,000 to 220,000 between 2020/21 and 2024/25.
Figure 3b. Admissions with a primary diagnosis of sepsis during the inpatient spell, by financial year and admission method
Source: Hospital Episode Statistics (see Technical annex: hospital admitted patient care and critical care activity)
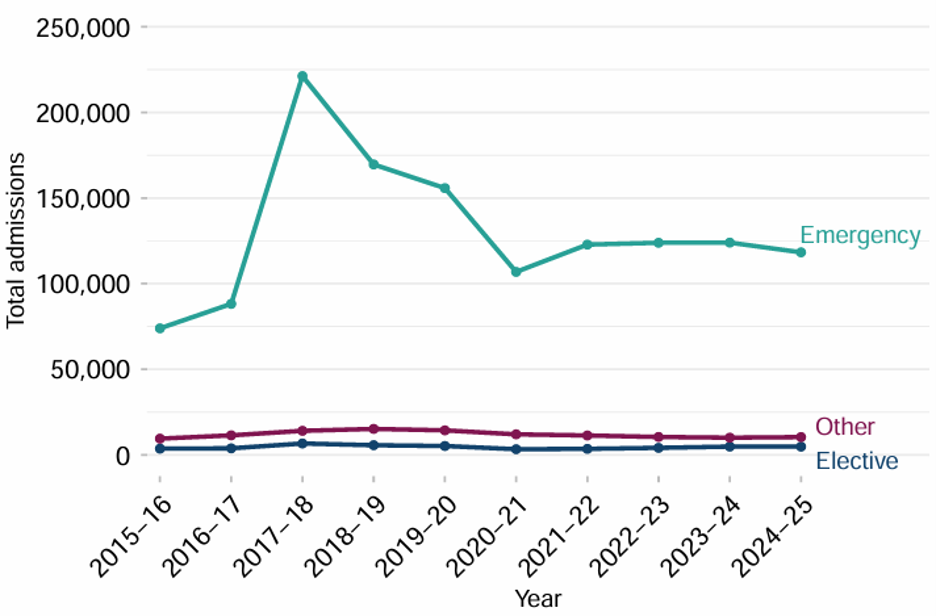
Chart description: Figure 3b shows the total number of admissions with a primary diagnosis of sepsis during the inpatient spell in each financial year from 2015/16 to 2024/25, split by elective, emergency or other admission methods. Elective admissions are relatively stable, with around 3,000 to 7,000 each year. Other admissions are also relatively stable at around 9,000 to 15,000 each year. Emergency admission numbers are very variable, rising sharply from around 75,000 in 2015/16 to over 220,000 in 2017/18, then declining and remaining between around 120,000 and 125,000 between 2021/22 and 2024/25.
The most recent available data from the Office for National Statistics (ONS) shows that, in 2025, 23,628 deaths in England had sepsis recorded as an underlying cause or contributing factor (Figure 4). Of these, 4,063 deaths were recorded as being directly caused by sepsis. However, in the majority of cases of death from infection, sepsis leading to organ failure will be the mechanism that causes death.
This does not mean that all these deaths are avoidable, or that everyone who develops sepsis would benefit from some of the highly invasive treatments available. Part of our challenge with this framework, and for clinicians everywhere, is ensuring that every individual is treated to the highest possible standards, while acknowledging that for some people, infection is part of the dying process. For these individuals, our priority must be to provide the right supportive end-of-life care for their individual needs.
Figure 4. Deaths due to and involving sepsis, England, registered between 2010 and 2025
Source: Office for National Statistics
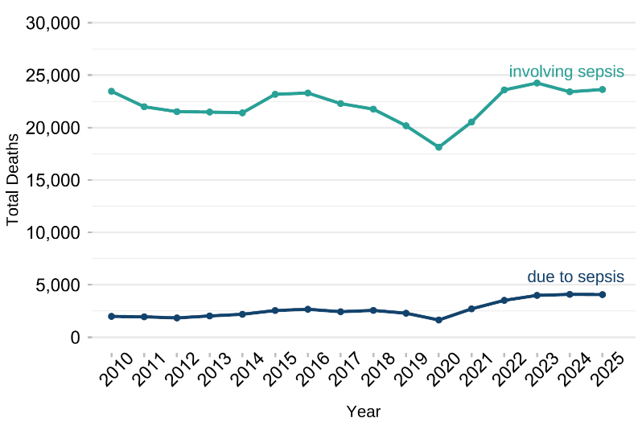
Chart description: Figure 4 shows the total number of deaths due to sepsis and involving sepsis each year from 2010 to 2025. Deaths due to sepsis are relatively stable at around 2,000 to 3,000 each year until 2019. There is then a slight dip in 2020 before rising to around 4,000 deaths per year in 2023, 2024 and 2025. There were between around 20,000 and 23,000 deaths involving sepsis per year between 2010 and 2019, declining to just over 18,000 in 2020. Deaths increased to between around 23,000 and 24,000 between 2022 and 2025.
Antimicrobial stewardship
There is significant clinical and operational tension between the need to administer antimicrobials promptly to prevent and treat sepsis and the recognition that unnecessary antimicrobials are not good for patients and drive resistance in pathogens.
Antimicrobial stewardship describes the system-wide appropriate use of antimicrobials, including prescribing and deprescribing, to prevent antimicrobial resistance (AMR), which is where infective organisms cannot be treated with standard therapeutics.
Action on AMR means:
- preventing infections
- improving the management and control of infections
- optimal use of antimicrobials
These are largely the same actions needed to reduce mortality from sepsis. Newer, faster ways of diagnosing infection presence and type will also significantly help clinicians and patients and tackle AMR.
For this reason, any strategy to address sepsis must build on efforts to address AMR and consider potential negative impacts on AMR. This framework therefore includes actions which aim to reduce the risk of inappropriate antimicrobial usage and make the best use of existing AMR initiatives.
Publication reference: PRN02407_ii