
Introduction
This document presents the results of all NHS trusts and NHS foundation trusts (termed ‘providers’) in England. The Department of Health and Social Care (DHSC) uses the provider sub-consolidation as part of the DHSC group accounts. We are very grateful to NHS providers for their co-operation in reporting their data to us.
These accounts are presented separately from those of NHS England as NHS England is not the parent body of NHS trusts and NHS foundation trusts.
The introduction describes the legal requirements for NHS trust and NHS foundation trust accounts and organisational changes in the provider sector in 2023/24 and 2024/25.
NHS trusts
Paragraph 11A(3) of Schedule 4 of the National Health Service Act 2006 (the 2006 Act) (as inserted by Section 87 of the Health and Care Act 2022) requires each NHS trust to prepare annual accounts for each financial year ending 31 March. These annual accounts must be audited by auditors appointed by the NHS trust.
NHS trusts that cease to exist as separate legal entities during the year (including on authorisation as an NHS foundation trust) prepare accounts for their final period as directed by the Secretary of State and have them audited.
NHS foundation trusts
Paragraph 25 of Schedule 7 to the 2006 Act (as amended by paragraph 31(3) of Schedule 5 to the Health and Care Act 2022) requires each NHS foundation trust to prepare annual accounts for the period beginning on the date it is authorised and ending the following 31 March and for each successive 12-month period. These annual accounts must be audited by auditors appointed by the NHS foundation trust’s council of governors. The trust must lay a copy of the accounts, and any auditor’s report on them, before Parliament and send them to NHS England.
NHS foundation trusts that cease to exist as separate legal entities before the end of the year continue to prepare accounts for their final period as directed by NHS England and have them audited, but do not present them to the council of governors.
Basis of preparation for consolidated NHS provider accounts
Section 65Z4 of the National Health Service Act 2006 (as inserted by Section 14 of the Health and Care Act 2022) requires NHS England to prepare, for each financial year, a set of accounts that consolidates the annual accounts of all NHS trusts and NHS foundation trusts. The Secretary of State has given directions on the content and form of these consolidated accounts and the principles to be applied in preparing them. The Comptroller and Auditor General is required to examine, certify and report on the consolidated NHS provider accounts and send a copy of any report to the Secretary of State and NHS England. NHS England is required to lay the consolidated provider accounts and the Comptroller and Auditor General’s certificate and report before Parliament.
Organisation terminology
These consolidated accounts reference other documents issued by NHS England; in some cases these will have been issued by predecessor legal bodies. Documents issued by the NHS Trust Development Authority and Monitor before they were abolished are treated, from 1 July 2022, as having been issued by NHS England.
Changes in legal status of NHS providers
These consolidated NHS provider accounts incorporate the results of all NHS trusts and NHS foundation trusts. Entities for which legal status changed in 2023/24 or 2024/25 are as follows:
| NHS trusts | NHS foundation trust | All providers | ||
|---|---|---|---|---|
| 1 April 2023 | Number of providers at start of year Following dissolution of Yeovil District Hospital NHS Foundation Trust on acquisition by Somerset NHS Foundation Trust. | 68 | 143 | 211 |
| 1 July 2023 | Dissolution of Southport and Ormskirk Hospital NHS Trust on acquisition by St Helens and Knowsley Hospital Services NHS Trust; entity renamed as Mersey and West Lancashire Teaching Hospitals NHS Trust. | -1 | 210 | |
| 31 March 2024 | Number of providers at end of year | 67 | 143 | 210 |
| 1 October 2024 | Dissolution of Dudley Integrated Health and Care NHS Trust. This was following transfer of functions, net assets and staff to NHS Black Country Integrated Care Board, Black Country Healthcare NHS Foundation Trust and The Dudley Group NHS Foundation Trust | -1 | -1 | |
| 1 October 2024 | Dissolution of Solent NHS Trust on acquisition by Southern Health NHS Foundation Trust; entity renamed as Hampshire and Isle of Wight Healthcare NHS Foundation Trust | -1 | -1 | |
| 1 November 2024 | Dissolution of Barnet, Enfield and Haringey Mental Health NHS Trust on acquisition by Camden and Islington NHS Foundation Trust; entity renamed as North London NHS Foundation Trust | -1 | -1 | |
| 1 November 2024 | Dissolution of Hounslow and Richmond Community Healthcare NHS Trust on acquisition by Kingston Hospital NHS Foundation Trust; entity renamed as Kingston and Richmond NHS Foundation Trust | -1 | -1 | |
| 1 January 2025 | Dissolution of North Middlesex University Hospital NHS Trust on acquisition by Royal Free London NHS Foundation Trust. | -1 | -1 | |
| 31 March 2025 | Number of providers at end of year | 60 | 143 | 205 |
Review of financial performance of NHS providers
| 2024/25 | 2023/24 | |
|---|---|---|
|
Number of NHS providers in existence during the year |
210 |
211 |
|
Deficit before impairments and transfers |
£553 million |
£2,312 million |
|
Number of NHS providers recording a deficit before impairments, transfers and consolidation of charitable funds |
112 |
136 |
|
Sector cash balance at year end |
£9,977 million |
£10,802 million |
NHS providers have continued to focus on increasing productivity during 2024/25, delivering more care to patients with the resources available to them. In the face of unprecedented industrial action and a continued rise in demand for services, the provider sector improved operational performance in a number of key areas including elective waiting list reductions and cancer diagnosis, while still delivering an improved financial outturn.
NHS providers are not required to break even in every year. Providers are required to exercise their functions in line with the relevant plans of the integrated care board and system partners to achieve balance across the integrated care system as a whole, allowing for local allocation and prioritisation of available resources. The provider sector delivered a net deficit before impairments and gains and losses on transfers by absorption for the year ended 31 March 2025 of £553 million (2023/24: £2,312 million net deficit). 47% of this change in the outturn between the two years arises in operating surplus; 50% stems from a decrease in net finance costs as explained below. Providers held cash of £10.0 billion as at 31 March 2025 (31 March 2024: £10.8 billion).
The following table shows the profile of NHS providers that made up the sector during 2024/25. Providers are classified by their principal services but they may also provide other services. More analysis by trust type is set out in note 2 to the financial statements.
| Acute | Mental health | Ambulance | Specialist | Community | Charitable funds | Total | |
|---|---|---|---|---|---|---|---|
| Number of providers | 119 | 47 | 10 | 16 | 18 | n/a | 210 |
| % of sector turnover | 75% | 15% | 3% | 4% | 3% | <0.1% | 100% |
| Surplus/(deficit) before impairments and transfers (£m) | (713) | 53 | 17 | 92 | 13 | (16) | (554)* |
| Number of providers reporting deficit | 82 | 16 | 1 | 5 | 8 | n/a | 112 |
* The aggregate of the surplus/(deficit) from individual provider accounts does not equal the consolidated deficit in these accounts due to eliminating lease arrangements between NHS providers
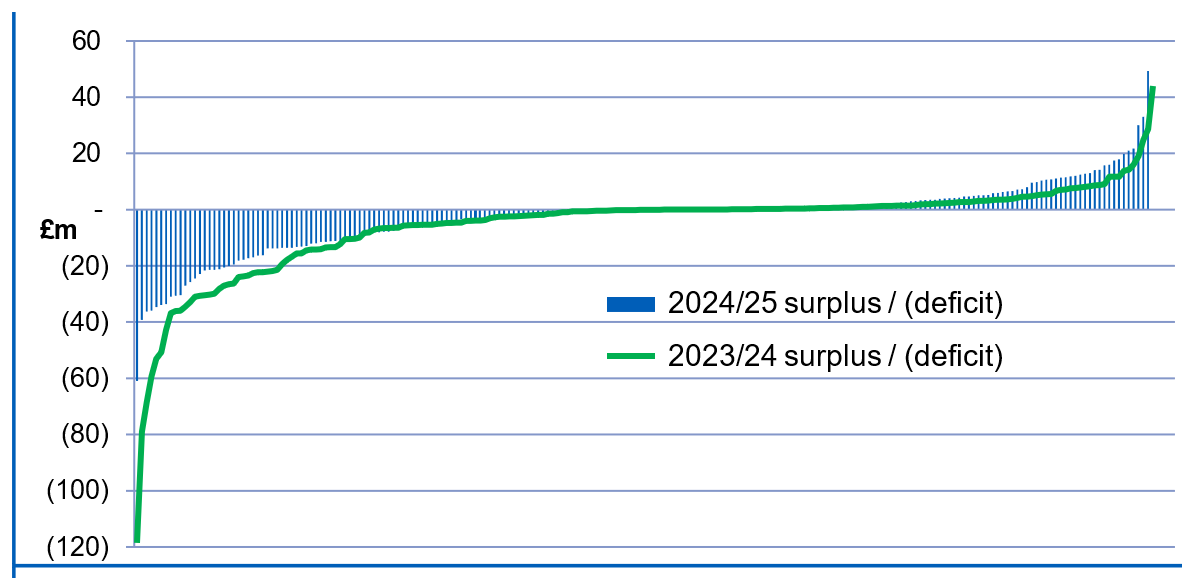
The results for the year showed that, excluding the consolidation of charitable funds, 98 NHS providers (47%) (2023/24: 75 (36%)) delivered a surplus or broke even and 112 providers (53%) (2023/24: 136 (64%)) reported a deficit before impairments and transfers by absorption. The gross deficit of all providers in deficit decreased from £2,550 million in 2023/24 to £1,127 million in 2024/25. Of the 75 trusts that reported a surplus in 2023/24, 19 (25%) reported a deficit in 2024/25, while 42 (31%) of the 136 trusts reporting a deficit in 2023/24 improved to report a surplus in 2024/25.
Figure 1 shows the distribution of providers’ surplus or deficit for 2024/25 and 2023/24. The two lines are plotted independently.
Figure 1: Surplus / (deficit) before impairments and absorption transfers
Where NHS charitable funds are locally deemed to be controlled by an NHS provider, the financial results of the charities are consolidated in these accounts. 40 NHS providers consolidated charitable funds, contributing an aggregate deficit of £16 million (2023/24: 41 providers consolidated an £83 million deficit) and net assets of £247 million (31 March 2024: £264 million).
The NHS Oversight Framework sets out the principles for system accountability and improvement support where appropriate. Providers who were in segment 4 of the 2024/25 oversight framework were entered into the Recovery Support Programme (RSP). This programme provides focused and integrated support to systems as well as individual organisations. As at 31 March 2025, 17 providers reporting a deficit for the year were also receiving support in the RSP (31 March 2024: 17 providers). This support may not be finance related in all cases.
206 of 210 NHS provider audited accounts have been completed at the time of finalising these consolidated accounts on 3 November 2025 (2023/24: 206 of 211 at 1 November 2024). All 206 have unqualified true and fair audit opinions (2023/24: 206 unqualified).
The results of four providers have been consolidated based on unaudited accounts information provided by the Trust; this is explained on page 23. Further information is provided in note 32 to these consolidated financial statements. The timeliness of local and national accounts is discussed further in the consolidated annual governance statement.
All providers have prepared financial statements on a going concern basis. HM Treasury’s Financial Reporting Manual (FReM) defines that a public sector body will be a going concern where continuation of the provision of services is anticipated in the future. The same definition is applied by NHS providers in preparing their financial statements. The accounting policies contain our going concern assessment for these consolidated accounts.
Operating income
In the year to 31 March 2025, 210 NHS providers generated total operating revenues of £140.9 billion, an increase of £12.0 billion (9.3%); a real terms increase of 5.04% when adjusted for inflation*. This increase of £12 billion includes a net 3.3% uplift to baseline contract prices with commissioners, including the impact of pay awards. Contract income was further increased by non-recurrent funding made available to systems to support financial recovery where their deficit plans for 2024/25 reflected an agreed level of financial improvement. The increase to employer contribution rates for the NHS pension scheme (a further 3.1% of pensionable pay compared to the prior year rate) was also funded by NHS England and is reflected in provider income.
* This is calculated with reference to the GDP deflator for 2024/25 published by HM Treasury on 30 June 2025
Operating expenditure
Total operating expenditure increased from £130.6 billion in 2023/24 to £142.2 billion in 2024/25, with key movements set out below. Excluding impairments, operating expenditure increased by £11.1 billion (8.7%) from £128.4 billion to £139.5 billion; a real terms increase of 4.40% when adjusted for inflation1. The real terms increase in income being slightly higher than the real terms increase in expenditure in 2024/25 reverses the trend reported in the consolidated provider accounts in 2022/23 and 2023/24.
Figure 2: Expenditure bridge 2023/24 to 2024/25
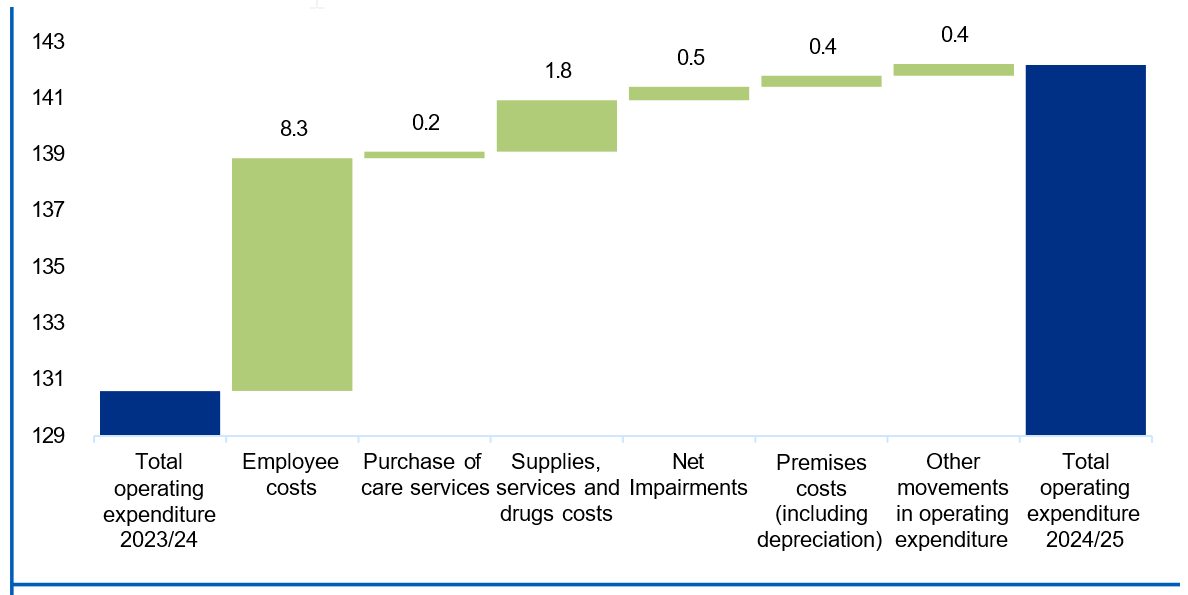
Almost 74% (£8.3 billion) of the increase in operating expenditure related to employee costs, which is largely driven by the pay awards for 2024/25. Recruitment and retention challenges and industrial action have also driven up staff costs.
Half of the increase in supplies and services (£0.9 billion) relates to drug costs and is driven mainly by an increase in high cost drugs recharged to commissioners.
Impact of impairments
Impairments to the carrying value of assets are charged to operating surplus except where previous revaluation surpluses remain: in such cases a reduction is first recognised in the revaluation reserve to the extent of the remaining surplus for that asset. Where the impairments reflect a permanent loss, such as fire damage, they are always charged to expenditure. In 2024/25 net impairments charged to income and expenditure were £2,662 million (2023/24: £2,188 million). A further £1,065 million of net impairments was charged to reserves (2023/24: £1,451 million), reducing previously recognised revaluation surpluses. Providers also recognised revaluation surpluses directly in reserves totalling £1,007 million (2023/24: £1,197 million). This results in a net downwards valuation movement on non-current assets of £2,720 million compared to a net downwards valuation movement of £2,442 million in 2023/24.
There were 182 NHS providers recording a net impairment within surplus/deficit in 2024/25 (2023/24: 170) while 14 providers recorded net reversals of impairments (2023/24: 24).
Of the £2,662 million of net impairments charged to income and expenditure, 86% arose from changes in market price (2023/24: 87%). These impairments reflect market conditions at the time of valuation and not a deterioration in the service potential of the asset. Further details of impairments are provided in note 10 to the accounts.
Net finance costs
Net finance costs in 2024/25 decreased by £879 million to £1,933 million. Average inflation during 2024/25 was lower than 2023/24, reducing the value of remeasurements on PFI and similar scheme liabilities recognised in finance costs by £1,008 million.
Working capital and borrowings
At 31 March 2025, NHS providers held cash and cash equivalents of £10.0 billion; equivalent to 4.0 weeks’ operating costs in a sector with annual expenditure of £129.7 billion (31 March 2024: 4.7 weeks). This expenditure figure excludes the 9.4% (2023/24: 6.3%) additional NHS pension contribution made by NHS England. Revenue cash support may be provided by the Department of Health and Social Care to ensure essential day to day spend can be met thereby protecting the continuity of patient services. During 2024/25, 54 providers received public dividend capital to support short term revenue requirements, totalling a net £872 million (2023/24: 44 providers, £1,190 million). Providers in receipt of revenue support must work with NHS England to improve their financial position.
The number of receivables days has decreased to 14.3 days in 2024/25 (2023/24: 14.7 days). Payable days decreased to 35.2 days in 2024/25 from 37.8 days in 2023/24.
Providers are monitored on their reported timeliness in paying suppliers.
Total long-term and working capital borrowing at 31 March 2025 was £21.7 billion (31 March 2024: £22.1 billion). This decrease in borrowings is a result of repayments on PFI obligations and loans exceeding remeasurements for inflation and interest arising in the year.
Capital expenditure
Providers’ ability to invest in capital schemes is limited by constraints in DHSC’s departmental capital expenditure limit. Integrated care systems are allocated capital budgets termed capital envelopes to cover day-to-day operational capital investment which allows for local prioritisation of available resources within the system. These allocations are supplemented with centrally allocated funds to cover nationally strategic projects such as new hospitals and hospital upgrades. Further resource is made available to cover national programmes. In 2024/25 this included continued investment in access to diagnostics to support increased activity, improve productivity and reduce health inequalities.
Systems are required to ensure that capital plans take into account the impact on organisations’ carbon emissions and deliver on objectives for a ‘net-zero’ National Health Service. The NHS is committed to achieving a net-zero NHS by 2040. This includes investing in schemes to reduce air pollution by decarbonising NHS estates and fleet and supporting delivery of high quality, digitally enabled, low carbon care.
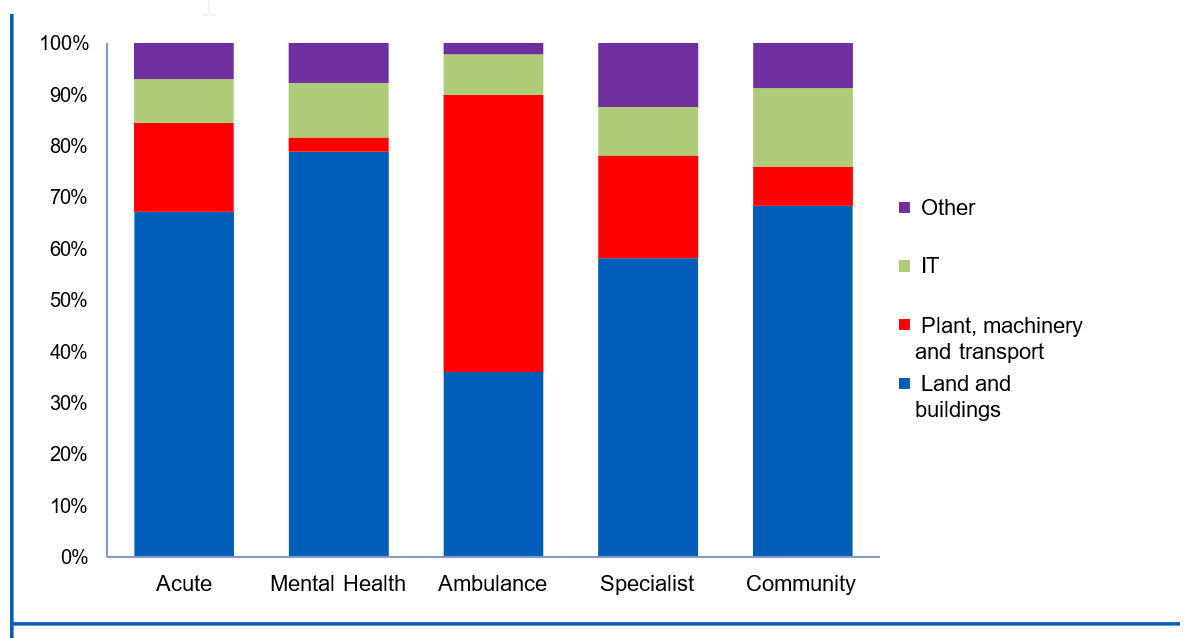
Total purchases and new or modified leases of property, plant and equipment and intangible assets were £8.1 billion (2023/24: £8.2 billion). More than half (67%) of capital spend was on land and buildings, with a further 17% on plant, equipment and transport, 9% on information technology, and 7% on other capital (Figure 3).
Figure 3: Proportion of capital spend by type, 2024/25
The NHS continues to invest in the redevelopment of estates to modernise healthcare and shift care to more suitable settings. For example, in April 2024 South Tees Hospitals NHS Foundation Trust opened a new urgent treatment centre at the James Cook University Hospital, easing pressure on the emergency department and reducing delays in care for patients with minor injuries and illnesses. Following a re-profiling of the New Hospital Programme in January 2025, Royal Cornwall Hospitals NHS Trust received confirmation that a new Women and Children’s Hospital, the largest ever single investment in the NHS in Cornwall, would proceed as part of the first wave of schemes. Digital innovation is core to delivery of the new hospital and during 2024, the Trust successfully piloted the ‘Silent Hospital’ project, which replaced audible patient call bells on the postnatal ward with silent alerts delivered directly to staff-held mobile devices. Reductions in noise levels provided a calmer, more therapeutic environment for patients.
Understanding the NHS position
Central government and NHS bodies prepare their accounts under the principles of International Financial Reporting Standards (IFRS) as adopted by HM Treasury. However central government departments also report their financial outturn on an alternative basis where some items are treated differently, such as interests in private finance initiative (PFI) schemes. It is on this basis that DHSC holds NHS England to account. The government reporting basis is against the ‘non-ringfenced revenue departmental expenditure limit’ (NRF RDEL). The provider outturn on this basis can be combined with the position for the NHS England group to see the overall NHS outturn:
| NHS outturn | 2024/25 £m | 2023/24 £m |
|---|---|---|
| NHS budget in directions (excluding funding for depreciation) * | 186,838 | 171,036 |
| NHS England net expenditure on a government reporting basis ** | (190,193) | (173,762) |
| NHS provider outturn on a government reporting basis | 3,299 | 2,492 |
| NHS outturn | (56) | (234) |
| NHS outturn as percentage of budget | (0.03%) | (0.14%) |
* As contained in annex A1 of the government’s financial directions to NHS England
** NHS England annual report and accounts: financial performance note
Wider context
More information on the performance of the NHS in 2024/25 and priorities going forward can be found in NHS England’s annual report and accounts.
Sir James Mackey, Chief Executive Officer 24 November 2025
Statement of accounting officer’s responsibilities and accountability framework
I am designated as the Accounting Officer for NHS England. In this capacity I am responsible for ensuring that NHS England prepares consolidated NHS provider accounts to send to the Secretary of State and the Comptroller and Auditor General. I am not the accountable/accounting officer for each individual NHS trust/NHS foundation trust; this is the role of each local chief executive. An NHS trust’s chief executive is designated as the accountable officer when their appointment is confirmed by NHS England. NHS foundation trust chief executives are designated as the accounting officer by the NHS Act 2006.
Amanda Pritchard was the accounting officer for NHS England for the period covered by these consolidated accounts, up to 31 March 2025. I, Sir James Mackey as incoming Chief Executive of NHS England, received assurances from Amanda Pritchard at this date.
NHS trusts
The Secretary of State is responsible for determining, with HM Treasury’s approval, the form of accounts each NHS trust must adopt. This is described in the Department of Health and Social Care’s Group Accounting Manual (GAM), which is based on HM Treasury’s Financial Reporting Manual (FReM). NHS England has set out the responsibilities of each NHS trust accountable officer to ensure:
- there are effective management systems in place to safeguard public funds and assets
- the trust achieves value for money from the resources available to it
- the trust’s expenditure and income have been applied to the purposes intended by Parliament and conform to the authorities which govern them
- effective and sound financial management systems are in place
- the Trust’s annual accounts give a true and fair
NHS England has set out the responsibilities of NHS trust directors to:
- apply suitable accounting policies consistently
- make reasonable judgements and estimates
- make a statement within the accounts on whether applicable accounting standards have been followed, and to disclose and explain any material departures and
- prepare the financial statements on a going concern basis and disclose any material uncertainties over going concern.
NHS foundation trusts
NHS England is responsible for determining, with the Secretary of State’s approval, the form of accounts each NHS foundation trust must adopt. The NHS foundation trust annual reporting manual (FT ARM), which is based on the FReM, sets out the responsibilities of each NHS foundation trust accounting officer to:
- apply suitable accounting policies consistently
- make reasonable judgements and estimates
- make a statement within the accounts on whether applicable accounting standards have been followed, and to disclose and explain any material departures
- ensure the use of public funds complies with the relevant legislation, delegated authorities and guidance
- confirm that the annual report and accounts, taken as a whole, is fair, balanced and understandable and provides the information necessary for patients,regulators and stakeholders to assess the NHS foundation trust’s performance, business model and strategy and
- prepare the financial statements on a going concern basis and disclose any material uncertainties over going concern.
Consolidated NHS provider accounts
In discharging its responsibilities in accordance with the directions to NHS England issued by the Secretary of State, NHS England has prepared consolidated NHS provider accounts on a basis consistent with the individual NHS providers’ accounts and consolidated in accordance with International Financial Reporting Standards (IFRS), as amended for NHS providers by the FReM, the FT ARM and the GAM.
The Secretary of State’s directions require NHS England to prepare these consolidated NHS provider accounts to:
- give a true and fair view of the state of affairs of NHS trusts and foundation trusts collectively as at the end of the financial year and the comprehensive income and expenditure, changes in taxpayers’ equity and cash flows for the financial year then ended
- disclose any material expenditure or income that has not been applied for the purposes intended by Parliament or material transactions that have not conformed to the authorities that govern them.
As far as I am aware, there is no relevant audit information of which the auditors of the consolidated NHS provider accounts are unaware. As Accounting Officer I have taken all the steps I ought to have taken to make myself aware of any relevant audit information and to establish that the auditors are aware of this information.
Sir James Mackey, Chief Executive
24 November 2025
Annual governance statement
This annual governance statement (AGS) for the NHS provider sector has been prepared in the context of the accountability framework set out above. It has been prepared as a consolidation of the sector position based on reference to:
- the segmentation of providers under the NHS Oversight Framework
- disclosures in local annual governance statements and
- the audit reports issued by local external
Scope of responsibility
NHS England’s Board is not responsible for the internal control and systems of NHS providers; this is the responsibility of each NHS provider’s board.
NHS trusts
As accountable officer, each NHS trust’s chief executive is accountable to NHS England and is responsible for maintaining a sound system of internal control that supports the achievement of the trust’s policies, aims and objectives. In addition, the chief executive, as accountable officer, has responsibility for safeguarding public funds and the organisation’s assets as set out in the NHS trust accountable officer memorandum.
NHS foundation trusts
As accounting officer, each NHS foundation trust’s chief executive has responsibility to Parliament for maintaining a sound system of internal control that supports the achievement of the trust’s policies, aims and objectives. In addition, the chief executive, as accounting officer, has responsibility for safeguarding public funds and the organisation’s assets as set out in the NHS foundation trust accounting officer memorandum.
Purpose of the system of internal control
NHS England’s system of internal control is designed to support the achievement of its policies, aims and objectives and ensure compliance with legal and other obligations on NHS England and NHS trusts and foundation trusts. As part of this system, NHS England has the following processes to ensure these accounts provide a ‘true and fair’ view of the affairs of NHS providers:
- contributing to the development of guidance to NHS trusts and NHS foundation trusts through the Department of Health and Social Care’s (DHSC’s) Group Accounting Manual (GAM); this has been approved by HM Treasury
- providing guidance to foundation trusts through the NHS foundation trust annual reporting manual (FT ARM); this has been approved by the Secretary of State
- relying on the external auditors appointed by each NHS trust/NHS foundation trust’s council of governors to provide assurance over the truth and fairness of each set of accounts consolidated into these accounts; these auditors have each undertaken an audit in accordance with the Code of audit practice (audit code), issued by the Comptroller and Auditor General, supported by the National Audit Office (NAO)
- appointing the Quality Assurance Directorate of the Institute of Chartered Accountants in England and Wales and Audit Quality Review department of the Financial Reporting Council to review the quality of the work of NHS foundation trust auditors and consider their The audits of NHS trusts are reviewed under similar arrangements by Statute, not overseen by NHS England
- attending the NAO’s Local Auditors’ Advisory Group and associated technical networks, to which senior representatives from each of the audit suppliers appointed as auditors of NHS providers are invited; the forum members discuss technical audit and accounting issues in the public sector, including those concerning NHS bodies and
- consideration by NHS England’s management and by its Audit and Risk Assurance Committee of the consolidated accounts and the processes established to derive them.
Each NHS provider’s annual report and accounts includes an AGS for the year ended 31 March 2025. Each individual AGS explains how the accountable/accounting officer has reviewed the effectiveness of internal control during the period and highlights any significant control issues where the risk cannot be effectively controlled.
Timeliness of local and national accounts
In preparing the consolidated provider accounts based on consolidation schedules from NHS providers, we are reliant on each provider submitting their audited annual report and accounts to us. We and the Department of Health and Social Care issue directions to NHS bodies on the timing by which these should be submitted.
There are many reasons why a set of audited accounts for a local NHS body may go beyond the deadline: for example this may reflect illness in the preparer finance team or audit team, or a significant issue may be encountered that takes time to resolve, which may reflect weaknesses in an entity’s preparation of its accounts. Auditors need to be able to complete their work independently of outside influence and take the necessary time to ensure their audit opinion is the right one and supported by appropriate audit evidence. It is also important that there is a properly functioning local audit market to allow audited bodies to hold their auditors to account for delivery. We welcome the Financial Reporting Council’s publication of its NHS Audit Market Study.
The timeline on which these national accounts are finalised depends on both when the deadline for local audited accounts is set, and compliance with that deadline. For many years prior to 2019/20 the local audit deadline in the NHS was around the end of May. The deadline is set in consultation with the audit firms on what they are willing to sign up to. In recent years the local audit deadline has been around the end of June.
In recent years in the consolidated provider accounts we have described NHS England’s limited direct role in NHS audits but detailed the steps we have been taking to improve compliance with the local deadline for audited accounts in the NHS.
More NHS bodies achieved the deadline for submission of audited accounts in 2024/25 than in recent years. 92% of local NHS bodies (being NHS providers and ICBs) met the deadline in 2024/25, the highest proportion since 2019/20. For NHS providers, 90% met the deadline in 2024/25, compared to only 82% in 2023/24 and 77% 2022/23.
The improvement in performance is welcomed but finalisation of these consolidated accounts requires a critical mass of completed local audits and the time taken to reach this threshold has resulted in these accounts being finalised in November for a second year. While this remains an improvement on the January completion for the years 2019/20 to 2022/23, we did not achieve our plan for earlier finalisation of the 2024/25 accounts in October.
The original plan was predicated on finalising these accounts with the consolidation of a small number of unaudited accounts where local audits were planned to be late due to either outstanding prior year accounts, or local auditors awaiting local government pensions assurance. Additional national procedures are performed to obtain assurance over these unaudited values. This plan was initially affected by unplanned further delays at two trusts who were expected to complete to a September deadline following difficulties in appointing external auditors. Subsequent to this, delays to the audited accounts for University Hospitals Birmingham NHS Foundation Trust impacted on both finalisation of these accounts and assurance for the National Audit Office. As the consolidated provider accounts is a material component of the Department of Health and Social Care (DHSC) group, these delays have also led to DHSC not achieving its November target for its group annual report and accounts.
NHS England and the Department of Health and Social Care (DHSC) have worked closely with the Ministry of Housing, Communities and Local Government (MHCLG) on the relevant elements of its work to reform ‘local’ audit. In July 2025 MHCLG laid the English Devolution and Community Empowerment Bill before Parliament, part four of which makes changes to the local audit system in England and Wales. The reforms include establishing the Local Audit Office, a body to coordinate local audit with responsibilities including determining the framework for auditors to follow, rules for eligibility to be a local auditor, and inspection and enforcement. Bringing these functions together will help set the foundation to strengthen the audit market. These changes directly apply to audits of NHS trusts and ICBs; DHSC and NHS England are exploring ways to replicate them for NHS foundation trusts.
As well as reforms to the local audit system, we have continued our broader work to improve timeliness in NHS financial reporting including:
- encouraging auditors to give clear reporting to audit committees where the preparer’s quality of draft accounts or working papers needs to improve
- working closely with NHS bodies to ensure they appoint external auditors in good time, which helps increase the likelihood of deadlines being achieved
- working with NHS bodies where financial reporting issues arise to ensure they are able to address findings effectively
- regular engagement with the audit firms and responding to their feedback to continue to strengthen the NHS financial reporting landscape, and working with partners to make sure training and guidance is available for preparers
- a rigorous system of monitoring NHS bodies before and after the audited accounts deadline to support them in managing their audited accounts to completion
- prompt escalation of NHS bodies requiring more support to ensure targeted support to bring resolution of issues and
- liaising with broader stakeholders on wider matters that can cause delays in NHS accounts, for example sign offs of local government pension scheme audits, which directly affects a handful of NHS providers with a corresponding impact on these consolidated accounts.
NHS England and DHSC have an ambition to return to laying the main national consolidated accounts (being the DHSC group, NHS England group and consolidated provider accounts) before Parliament in advance of the summer Parliamentary recess in July. Achieving this in the years ahead would require the audit community to accept a significantly earlier deadline for audited accounts than is currently the case, which partly flows from the preparation of accounts and the work required of the auditors. At the present time it is not clear that this is achievable in the short term. We will continue to focus on streamlining processes for preparation and audit of local and national accounts to the extent this falls within our role to seek to facilitate the earlier finalisation of accounts wherever possible.
Overview of internal control systems at NHS trusts and NHS foundation trusts
Regularity
Regularity means the use of public funds complies with the relevant legislation and delegated authorities. Local NHS provider auditors do not issue an opinion on local regularity, but do perform specific procedures as part of their reporting to the NAO. The application of materiality to regularity requires judgement: irregular spending might be material by nature (in a high profile area for example) without the quantum of spend being material. As set out in the statement of accounting officer’s responsibilities, NHS England is required to disclose any material irregularity in the consolidated provider accounts. NHS providers generally have broad powers in spending money but we assess overall regularity by:
- reviewing the detail of our oversight and regulatory decisions (these concepts are explained below) to consider whether they highlight any regularity concerns
- confirmation from our regional teams whether they are aware of any irregular activity in providers
- collating any referrals of unlawful expenditure or activity submitted by local auditors (these are commonly termed ‘section 30 referrals’ and are explained further below)
- considering any fraud investigations known to NHS England
- reviewing the confirmation statements on regularity that each NHS provider chief executive is required to make in their statement of accounting/accountable officer responsibilities
- correlating sources of information on special severance payments and other forms of special payments, where specific controls apply and
- responding to any information provided to the NAO as part of their group
We regularly remind NHS providers of their responsibilities over approval for special severance payments, including via letters, briefings, emails and webinars. If cases of non-compliance arise, we seek to identify issues and incorporate those into subsequent briefings and reminders to NHS bodies.
NHS Oversight Framework
The previous NHS Oversight Framework continued to apply to the 2023/24 and 2024/25 financial years, before being replaced by a new Oversight Framework for 2025/26. The purpose remains the same: it provides the framework for overseeing the delivery of high quality, sustainable care with a focus at both local system and organisational level and identifying potential support needs.
The Framework describes a process to identify where NHS organisations may benefit from or require support to meet the standards required of them in a sustainable way and deliver the overall objectives for the sector in line with the priorities set out in the relevant planning guidance and other documents.
The remainder of this section specifically describes the Framework as in operation during 2023/24 and 2024/25. Details of the revised framework for 2025/26 can be found on our website6.
NHS Oversight Framework in 2023/24 and 2024/25
To provide an overview of the level and nature of support required across systems, inform oversight arrangements and target support capacity as effectively as possible, NHS England regional teams allocated NHS organisations to one of four ‘segments’.
A segmentation decision indicates the scale and general nature of support needs, from no specific support needs (segment 1) to a requirement for mandated intensive support (segment 4). A segment does not determine specific support requirements. By default, all NHS organisations were allocated to segment 2 unless the criteria for moving into another segment were met. These criteria had two components:
- objective and measurable eligibility criteria based on performance against the six oversight themes using the relevant oversight metrics (the themes were: (i) quality of care, access and outcomes; (ii) people; (iii) preventing ill-health and reducing inequalities; (iv) leadership and capability; (v) finance and use of resources; (vi) local strategic priorities)
- additional considerations focused on the assessment of system leadership and behaviours, and improvement capability and capacity.
An NHS trust or foundation trust was placed in segment three or four where it was found to have significant support needs that may require formal intervention and mandated support. They are subject to enhanced direct oversight by NHS England (in partnership with their ICB) and, depending on the nature of the problem(s) identified, additional reporting requirements and financial controls.
NHS trusts were issued licences on 1 April 2023 and from 2023/24 have been subject to the same licence conditions as NHS foundation trusts.
Segmentation of NHS providers is updated regularly. The table below summarises NHS providers’ segmentation as at 31 March 2025. A prior year comparative is not provided as this table provides a snapshot at that point in time and the design and application of the Oversight Framework may evolve over time.
|
| Segmentation at 31 March 2025 | |||
| Number of NHS trusts | Number of NHS FTs | Total number of providers | % of sector | |
|
1 |
8 |
19 |
27 |
13% |
|
2 |
24 |
51 |
75 |
37% |
|
3 |
23 |
59 |
82 |
40% |
|
4 |
7 |
14 |
21 |
10% |
|
Total |
62 |
143 |
205 |
|
NHS providers in segment 3 or 4 in 2023/24 and 2024/25
Where an NHS provider triggered a specific concern, NHS England worked with the ICB to understand why this concern arose and if a support need existed. Based on this assessment, NHS England agreed the subsequent level of support required. Where there was a need for mandated support by NHS England the provider was placed into segment 3 or 4, depending on the complexity of the support need.
A segment 3 decision resulted in a bespoke support offer led by the NHS England regional team drawing on system and national expertise as required.
Segment 4 decisions were reserved for those trusts experiencing long standing complex issues or serious failures in areas such as quality, safety, leadership, governance or financial plans. A segment 4 decision always triggered a referral to NHS England’s national Recovery Support Programme (RSP). Decisions on referrals into this programme were made by an executive committee of NHS England based on recommendations from Regional Directors or the Care Quality Commission. Where a referral into the RSP for a trust was agreed a dedicated Improvement Director was appointed to work alongside the Trust leadership as well as the ICB and regional team to oversee the development and delivery of an improvement plan. A diagnostic review would be undertaken to identify underlying drivers that needed to be addressed and embed improvement upstream to prevent further deterioration and enable stabilisation.
Enforcement action in 2023/24 and 2024/25
Where an NHS provider was in breach of its licence conditions (or where NHS England had reasonable grounds for suspecting a breach), NHS England also considered the use of its enforcement powers. These powers include, among others, agreeing enforcement undertakings or issuing directions to the provider to secure compliance and ensure the breach does not recur. Details of any enforcement action is publicly available via the Provider Directory on our website.
In exceptional circumstances an NHS trust or NHS foundation trust may be placed in trust special administration. Administration is a regime for ensuring the continuity of essential services in the event of provider financial distress. No trusts or foundation trusts were subject to trust special administration in 2023/24 or 2024/25.
NHS trusts’ and NHS foundation trusts’ significant internal control weaknesses
Sources of information
In the information that follows, NHS England has collated a number of sources of information to disclose the position for NHS providers.
NHS Oversight Framework segment 3 or 4
Where an NHS provider was in Oversight Framework segment 3 or 4 and receiving mandated support, the support offered to the provider will be defined in terms of the Oversight Framework themes.
NHS England placing an NHS provider into segment 3 or 4 and mandating support would normally indicate the existence of control weaknesses or failings in the trust’s control environment.
Other significant control issues
NHS providers may also declare other matters as significant control issues. NHS England’s FT ARM for NHS foundation trusts and AGS guidance for NHS trusts gives guidance on how to determine whether an internal control matter is ‘significant’ but does not prescribe an approach; this is a matter for each trust’s board. The table that follows includes all cases where trusts have disclosed one or more significant control weaknesses in their annual governance statement.
External auditor’s conclusion on use of resources
In addition to the ‘true and fair’ audit opinion on the accounts, external auditors of NHS trusts and NHS foundation trusts are required to conclude whether the trust has made proper arrangements for securing economy, efficiency and effectiveness in its use of resources. Where the auditor identifies significant issues, the auditor reports that they are unable to satisfy themselves that the trust has made these proper arrangements. Such reporting does not imply that the ‘true and fair’ audit opinion on the provider’s accounts is qualified. These conclusions are listed in the table that follows. In each case we summarise if this modification relates to the same matters as the reason for Oversight Framework segmentation as 3 or 4 by NHS England.
Defining a significant internal control issue for this document
Our starting point for this consolidated annual governance statement is where a trust has locally assessed and disclosed a significant internal control issue in its own annual governance statement.
In addition, regardless of whether these have been reported locally, we also deem the following to be evidence of significant internal control weaknesses:
- NHS Oversight Framework segmentation of 3 or 4 by NHS England during the year (with respect to the Framework as applicable to 2024/25)
- the external auditor modifying their use of resources
In the table that follows we also disclose notes on other non-standard forms of the auditor’s reporting. We do not consider that entries here necessarily represent a significant internal control weakness.
Summary of results
The table below provides a summary of the detail that follows:
| 2024/25 | 2023/24 | |
|---|---|---|
| Number of providers receiving mandated support from NHS England during the year | 109 | 101 |
| Total number of modified conclusions relating to arrangements for securing economy, efficiency and effectiveness in the provider’s use of resources | 77 | 67* |
| Number of providers where ‘true and fair’ audit opinion has been modified (qualified) | 0 | 0 |
| Providers consolidated without an audit report | 4 | 5 |
* This was 66 at the time of finalising the consolidated provider accounts for 2023/24. The auditor subsequently issued their audit report for Barking, Havering and Redbridge University Hospital NHS Trust which included a modified ‘use of resources’ conclusion.
Providers consolidated without an audit report
The consolidated provider accounts for 2023/24 describes how that document was finalised with five providers not having received their audit report. Three of these five were subsequently received:
- Barking, Havering and Redbridge University Hospitals NHS Trust in March 2025
- East London NHS Foundation Trust in March 2025
- Humber Teaching NHS Foundation Trust in February 2025
The audited 2023/24 accounts for Birmingham Women’s and Children’s NHS Foundation Trust and Croydon Health Services NHS Trust remain outstanding at the time of finalising these 2024/25 consolidated accounts.
The consolidated provider accounts for 2024/25 have been prepared using unaudited information for four providers as the audit reports remained outstanding at the time of finalising these disclosures on 3 November 2025:
| Provider | Reason for 2024/25 delay |
|---|---|
| Birmingham Women’s and Children’s NHS Foundation Trust | The auditor identified concerns around weaknesses in the system of internal control in 2023/24 which required further investigation by the Trust. Following ongoing delays the audit of the 2024/25 accounts has not yet commenced. |
| Croydon Health Services NHS Trust | The audit of the 2023/24 accounts was delayed while the Trust commissioned an external review into issues raised by a third party. The audit of the 2024/25 accounts has not yet commenced. |
| Humber Teaching NHS Foundation Trust | The accounts are delayed pending the auditor obtaining assurance over local government pensions information. The accounts being delayed is not within the trust’s control. |
| University Hospitals Birmingham NHS Foundation Trust | Following late completion to audited accounts in 2023/24, the Trust experienced difficulties preparing its 2024/25 draft accounts which has delayed completion of the associated audit, alongside a revised audit risk profile. |
More information on the approach taken for finalising these accounts with respect to national materiality is provided in note 32 to the consolidated financial statements.
List of providers with matters to report
This table lists the NHS trusts and NHS foundation trusts for which there are matters to report in the relevant columns. It therefore does not list all NHS providers. Column (3) lists significant internal control issues disclosed in local annual governance statements, excluding matters relating to the same issues as covered by NHS England’s mandated support. Therefore, the absence of a tick in this column does not necessarily mean the provider disclosed no significant internal control issues in its local AGS.
Word version of table: providers with matters to report
Special severance payments
NHS providers are required to obtain approval in advance of making non-contractual departure payments (termed ‘special severance payments’) to employees. At the time of finalising the disclosures in these consolidated provider accounts on 3 November 2025, there are 4 outstanding cases for 2024/25 where payments were made without prior authorisation. These have been submitted for retrospective approval. These cases, while currently irregular, have been judged as individually and collectively not material by nature to these consolidated accounts. The consolidated provider accounts for 2023/24 were finalised with 5 cases of special severance payments having been made without prior authorisation. These were submitted retrospectively and the Chief Secretary to the Treasury subsequently declined to approve them so the cases referenced in the 2023/24 consolidated accounts remain irregular. We will continue to reinforce the requirement that NHS providers obtain the necessary approvals for such payments in advance of offers being made.
Auditor referrals of matters arising
Under Section 30 of the Local Audit and Accountability Act 2014 for NHS trusts, and under Schedule 10 to the NHS Act 2006 for NHS foundation trusts, where an auditor believes that the body or an officer of the body:
- is about to make, or has made, a decision which involves or would involve the incurring of expenditure which is unlawful, or
- is about to take, or has taken, a course of action which, if pursued to its conclusion, would be unlawful and likely to cause a loss or deficiency the auditor should make a referral to the Secretary of State (for NHS trusts)/NHS England (for NHS foundation trusts).
37 NHS trusts (2023/24: 39) and no NHS foundation trusts (2023/24: none) were subject to such referrals in 2024/25. All of these referrals for 2024/25 relate to a failure by the trust to meet the statutory breakeven duty target (2023/34: 38 of 39). This requires an NHS trust to achieve a cumulative breakeven over a three or five-year period. The underlying issues in trust finances are disclosed as part of the detail on significant internal control issues presented above. The statutory breakeven duty does not apply to NHS foundation trusts.
Sir James Mackey, Chief Executive
24 November 2025
The Certificate and Report of the Comptroller and Auditor General to the Houses of Parliament
Opinion on consolidated financial statements
I certify that I have audited the Consolidated NHS Provider Accounts for the year ended 31 March 2025 under the National Health Service Act 2006.
The Consolidated NHS Provider Accounts comprise the:
- Consolidated Statement of Financial Position as at 31 March 2025;
- Consolidated Statement of Comprehensive Income, Consolidated Statement of Cash Flows and Consolidated Statement of Changes in Equity for the year then ended; and
- the related notes including the significant accounting
The financial reporting framework that has been applied in the preparation of the consolidated financial statements is applicable law and UK adopted International Accounting Standards.
In my opinion, the consolidated financial statements:
- give a true and fair view of the state of affairs of NHS trusts and NHS foundation trusts, taken collectively, as at 31 March 2025 and of their deficit for the year then ended; and
- have been properly prepared in accordance with the National Health Service Act 2006 and Secretary of State directions issued thereunder.
Opinion on regularity
In my opinion, in all material respects, the income and expenditure recorded in the consolidated financial statements have been applied to the purposes intended by Parliament and the financial transactions recorded in the consolidated financial statements conform to the authorities which govern them.
Basis for opinions
I conducted my audit in accordance with International Standards on Auditing (UK) (ISAs UK), applicable law and Practice Note 10 Audit of Financial Statements and Regularity of Public Sector Bodies in the United Kingdom (2024). My responsibilities under those standards are further described in the Auditor’s responsibilities for the audit of the financial statements section of my certificate.
Those standards require me and my staff to comply with the Financial Reporting Council’s Revised Ethical Standard 2019. I am independent of NHS England and of NHS trusts and NHS foundation trusts, taken collectively, in accordance with the ethical requirements that are relevant to my audit of the consolidated financial statements in the UK. My staff and I have fulfilled our other ethical responsibilities in accordance with these requirements.
I believe that the audit evidence I have obtained is sufficient and appropriate to provide a basis for my opinion.
Conclusions relating to going concern
In auditing the consolidated financial statements, I have concluded that NHS England’s use of the going concern basis of accounting in the preparation of the consolidated financial statements of the NHS trusts and NHS foundation trusts is appropriate.
Based on the work I have performed, I have not identified any material uncertainties relating to events or conditions that, individually or collectively, may cast significant doubt on the NHS trusts’ and NHS foundation trusts’ collective ability to continue as a going concern for a period of at least twelve months from when the financial statements are authorised for issue.
My responsibilities and the responsibilities of the Accounting Officer with respect to going concern are described in the relevant sections of this certificate.
The going concern basis of accounting for the Consolidated NHS Provider Accounts is adopted in consideration of the requirements set out in HM Treasury’s Government Financial Reporting Manual, which requires entities to adopt the going concern basis of accounting in the preparation of the financial statements where it is anticipated that the services which they provide will continue into the future.
Other Information
The other information comprises information included in the Consolidated NHS Provider Accounts but does not include the consolidated financial statements and my auditor’s certificate and report thereon. The Accounting Officer is responsible for the other information.
My opinion on the consolidated financial statements does not cover the other information and, except to the extent otherwise explicitly stated in my certificate and report, I do not express any form of assurance conclusion thereon.
My responsibility is to read the other information and, in doing so, consider whether the other information is materially inconsistent with the financial statements or my knowledge obtained in the audit, or otherwise appears to be materially misstated.
If I identify such material inconsistencies or apparent material misstatements, I am required to determine whether this gives rise to a material misstatement in the consolidated financial statements themselves. If, based on the work I have performed, I conclude that there is a material misstatement of this other information, I am required to report that fact.
I have nothing to report in this regard.
Opinion on other matters
In my opinion, based on the work undertaken in the course of the audit, the information given in the Introduction, Review of financial performance of NHS providers, Statement of accounting officer’s responsibilities and accountability framework, and the Annual governance statement for the financial year for which the consolidated financial statements are prepared is consistent with the consolidated financial statements and is in accordance with the applicable legal requirements.
Matters on which I report by exception
In the light of the knowledge and understanding of NHS trusts and NHS foundation trusts, taken collectively, and their environment obtained in the course of the audit, I have not identified material misstatements in the Introduction, Review of financial performance of NHS providers, Statement of accounting officer’s responsibilities and accountability framework, and the Annual governance statement.
I have nothing to report in respect of the following matters which I report to you if, in my opinion:
- adequate accounting records have not been kept by NHS England or returns adequate for my audit have not been received from branches not visited by my staff; or
- I have not received all of the information and explanations I require for my audit; or
- the annual governance statement does not reflect compliance with HM Treasury’s guidance.
Responsibilities of the Accounting Officer for the financial statements
As explained more fully in the Statement of accounting officer’s responsibilities and
accountability framework, the accounting officer is responsible for:
- maintaining proper accounting records;
- providing the C&AG with access to all information of which management is aware that is relevant to the preparation of the financial statements such as records, documentation and other matters;
- providing the C&AG with additional information and explanations needed for his audit;
- providing the C&AG with unrestricted access to persons within NHS England (and NHS trusts and NHS foundation trusts) from whom the auditor determines it necessary to obtain audit evidence;
- ensuring such internal controls are in place as deemed necessary to enable the preparation of financial statements to be free from material misstatement, whether due to fraud or error;
- preparing financial statements which give a true and fair view in accordance with Secretary of State directions issued under the National Health Service Act 2006;
- preparing the information which comprises the Introduction, Review of financial performance of NHS providers, the Statement of accounting officer’s responsibilities and accountability framework and the Annual governance statement in accordance with the National Health Service Act 2006, and with the directions made thereunder by the Secretary of State; and
- assessing NHS trusts’ and NHS foundation trusts’ collective ability to continue as a going concern, disclosing, as applicable, matters related to going concern and using the going concern basis of accounting unless the Accounting Officer anticipates that the services provided by NHS trusts and NHS foundation trusts will not continue to be provided in the future
Auditor’s responsibilities for the audit of the financial statements
My responsibility is to audit, certify and report on the financial statements in accordance with the National Health Service Act 2006.
My objectives are to obtain reasonable assurance about whether the financial statements as a whole are free from material misstatement, whether due to fraud or error, and to issue a certificate that includes my opinion. Reasonable assurance is a high level of assurance but is not a guarantee that an audit conducted in accordance with ISAs (UK) will always detect a material misstatement when it exists. Misstatements can arise from fraud or error and are considered material if, individually or in the aggregate, they could reasonably be expected to influence the economic decisions of users taken on the basis of these financial statements.
Extent to which the audit was considered capable of detecting non-compliance with laws and regulations including fraud
I design procedures in line with my responsibilities, outlined above, to detect material misstatements in respect of non-compliance with laws and regulations, including fraud. The extent to which my procedures are capable of detecting non-compliance with laws and regulations, including fraud is detailed below.
Identifying and assessing potential risks related to non-compliance with laws and regulations, including fraud
In identifying and assessing risks of material misstatement in respect of non-compliance with laws and regulations, including fraud, I:
- considered the nature of the sector, control environment and operational performance including the design of the NHS trusts’ and NHS foundation trusts’ accounting policies and performance incentives
- inquired of management, NHS England’s head of internal audit and those charged with governance, including obtaining and reviewing supporting documentation relating to NHS England’s policies and procedures on:
- identifying, evaluating and complying with laws and regulations;
- detecting and responding to the risks of fraud; and
- the internal controls established to mitigate risks related to fraud or non-compliance with laws and regulations including NHS England’s controls relating to NHS trusts’ and NHS foundation trusts’ compliance with the National Health Service Act 2006 and Managing Public Money;
- inquired of management, NHS England’s head of internal audit and those charged with governance whether:
- they were aware of any instances of non-compliance with laws and regulations;
- they had knowledge of any actual, suspected, or alleged fraud;
- discussed with the engagement team regarding how and where fraud might occur in the consolidated financial statements and any potential indicators of fraud.
As a result of these procedures, I considered the opportunities and incentives that may exist within the NHS trusts and NHS foundation trusts for fraud and identified the greatest potential for fraud in the following areas: revenue recognition, posting of unusual journals, complex transactions and bias in management estimates. In common with all audits under ISAs (UK), I am required to perform specific procedures to respond to the risk of management override.
I obtained an understanding of the NHS trusts’ and NHS foundation trusts’ framework of authority and other legal and regulatory frameworks in which NHS trusts and NHS foundation trusts operate. I focused on those laws and regulations that had a direct effect on material amounts and disclosures in the financial statements or that had a fundamental effect on the operations of NHS trust and NHS foundation trusts. The key laws and regulations I considered in this context included National Health Service Act 2006, the Health and Social Care Act 2012, the Health and Care Act 2022, Managing Public Money, employment law and tax legislation.
I considered regulations and regularity relating to special payments including special severance payments, as I identified the completeness and regularity of special payments and special severance payments as a significant risk.
Audit response to identified risk
To respond to the identified risks resulting from the above procedures:
- I reviewed the financial statement disclosures and testing to supporting documentation to assess compliance with provisions of relevant laws and regulations described above as having direct effect on the financial statements;
- I enquired of management and the Audit and Risk Assurance Committee concerning actual and potential litigation and claims;
- I reviewed minutes of meetings of those charged with governance and the NHS England Board and internal audit reports;
- I addressed the risk of fraud through management override of controls by testing the appropriateness of journal entries and other adjustments including consolidation adjustments; assessing whether the judgements on estimates are indicative of a potential bias; and evaluating the business rationale of any significant transactions that are unusual or outside the normal course of business; enquiring with the auditors of NHS trusts and NHS foundation trusts about the findings of their audits; and using the work of component auditors with respect to management override of controls; and
- in addressing the risk of fraud in revenue recognition, I directed the auditors of NHS trusts and NHS foundation trusts of the need to consider the presumed risk of fraud in revenue recognition and enquired with them around the findings of their audits and used the work of component auditors with respect to fraud in revenue recognition.
I communicated relevant identified laws and regulations and potential risks of fraud to all engagement team members and relevant component audit teams and remained alert to any indications of fraud or non-compliance with laws and regulations throughout the audit.
A further description of my responsibilities for the audit of the financial statements is located on the Financial Reporting Council’s website at: www.frc.org.uk/auditorsresponsibilities. This description forms part of my certificate.
Other auditor’s responsibilities
I am required to obtain sufficient appropriate audit evidence to give reasonable assurance that the expenditure and income recorded in the financial statements have been applied to the purposes intended by Parliament and the financial transactions recorded in the financial statements conform to the authorities which govern them.
I communicate with those charged with governance regarding, among other matters, the planned scope and timing of the audit and significant audit findings, including any significant deficiencies in internal control I identify during my audit.
Report
I have no observations to make on these financial statements.
Gareth Davies, Comptroller and Auditor General National Audit Office
1 December 2025
157-197 Buckingham Palace Road Victoria
London SW1W 9SP
Consolidated accounts
This section of the document contains important tables and figures that are an essential part of this document. However, due to accessibility reasons, it is published as a word document. but some of the elements may still not be fully accessible to all users. Please contact england.web@england.nhs.uk if you have a problems with this document.
Consolidate accounts 2024/25 – word version
A print ready PDF version of the full report is available on the GOV.UK website.