
Document purpose
This document provides further clarification and supporting information for the Commissioner Assignment Method (CAM) flow chart.
The objective of the Commissioner Assignment Method is to provide a clear interpretation of the NHS England and Department of Health and Social Care guidance documents regarding the application of commissioning rules for payment to national NHS data sets in England.
This document should be read alongside the Who Pays? guidance published by NHS England.
Aligned flow chart version and status
This guidance relates to the version of the flow chart that is designed around the commissioning business rules for the 2024/25 financial year.
Changes from 23/24 Commissioner Assignment Method flow chart and guidance document
The following items describe the changes from the previous guidance and diagram:
- updated dates throughout to refer to 2024/25
- updated references to overseas
- updated references for specialised services to reflect service
- some minor typographical type
- updated armed forces section to remove reference to community services.
Document audience
This document is designed to support those organisations (hereafter referred to as ‘data providers’) that derive and provide commissioner code data within commissioning datasets and other activity-based data sets. These organisations may be:
- healthcare providers, e.g. acute or mental health trusts and independent sector hospitals
- NHS England
- commissioning support organisations, e.g. commissioning support units (CSUs), data services for commissioners regional offices (DSCROs)
- local health boards
- integrated care boards (ICBs)
- integrated care services
- organisations listed within the NHS England lead provider framework for commissioning support services or commissioners running their own contract data processing facility, such as a stage 1 accredited safe haven.
Commissioner Assignment Method objective
This document is designed to support those organisations (hereafter referred to as ‘data providers’) that derive and provide commissioner code data within commissioning datasets and other activity-based data sets.
The objective of the Commissioner Assignment Method is to provide a clear interpretation of the NHS England and Department of Health and Social Care guidance documents regarding the application of commissioning rules for payment to national NHS data sets in England.
This guidance has been developed in conjunction with the NHS England ‘Who Pays?’ team and incorporates several clarifications and revisions as Commissioner Assignment Method is subject to periodic review. Who Pays? sets out a framework for the NHS in England for establishing which NHS organisation has responsibility for commissioning an individual’s care and which has responsibility for paying for that care.
The Commissioner Assignment Method flow chart is designed to assist providers to allocate the correct commissioner code within specified commissioning data set (CDS) records for the healthcare activities they provide. The commissioner code is recorded within the CDS field ORGANISATION CODE (CODE OF COMMISSIONER) within the service agreement details data group.
The commissioner code describes which commissioning organisation has payment responsibility, differentiating activity paid for by NHS England (including subdivisions thereof), ICB commissioners, other commissioners and local health boards as appropriate. It should be noted that there are circumstances in which responsibility for commissioning and responsibility for payment will differ, and where responsibility will not be determined on the basis of GP registration. These are explained in detail in Who Pays?
It embodies the explicit commissioning hierarchy for ICB and NHS England commissioned services, originally as described in the Letter to NHS England Area Teams – Secondary Dental Care (Gateway Reference No. 00781), dated 20 November 2013, and expands this to ensure assignment of commissioner is appropriately aligned to allocations and budgets.
This shows the order of precedence for the different NHS England commissioned services, where more than one can apply for a patient, e.g. member of the armed forces receiving specialised care. After this letter, NHS England commissioning and finance teams have clarified that Health and Justice commissioning should take precedence over Armed Forces commissioning in the commissioning hierarchy, and that public health commissioning for CDS data should be positioned between Armed Forces and Health and Justice.
From April 2023 secondary dental services are no longer commissioned by NHS England and instead are commissioned by sub-integrated care board locations (sub-ICB locations).
From April 2024 a process of service delegation has been established to pass the responsibility for commissioning some specialised services to ICBs. This only relates to specialised services, other directly commissioning services (health and justice, public health and armed forces) are not subject to delegation.
The Commissioner Assignment Method is intended to provide an interpretation of the most likely organisation that will be responsible for care, based on routinely collected data. It does not alone create eligibility or payment responsibility. Other rules may apply, such as local commissioning rules, and eligibility criteria, and use of local data may create situations where the Commissioner Assignment Method cannot derive a correct commissioner. This guidance tries to be comprehensive, but it cannot cover all scenarios. In these cases, where further guidance is required, NHS England commissioning hubs can provide additional advice.
This guidance does not provide for every eventuality or case study covered in Who Pays? In the event of any inconsistency between this guidance and Who Pays?, the provisions of Who Pays? should be followed. In situations where disputes between NHS commissioners within England arise which cannot be resolved locally, a formal dispute resolution process, managed by NHS England’s national team, will apply to determine which commissioner should pay. This process is set out in full in Appendix 1 of Who Pays?
A sub-Integrated Care Board (sub-ICB) location is a sub-division of an Integrated Care Board’s total geographic area, used for data disaggregation purposes. It is expected that providers will continue to use sub-ICB codes through 2024/25, when recording a commissioner code in the Commissioning Data Sets.
CDS scope
The following Commissioning Data Set v6.3 types are within the scope of the Commissioner Assignment Method flow chart:
- CDS 011 Emergency Care Data Set
- CDS 020 Outpatient Appointments
- CDS 120 Admitted Patient Care Finished Birth Episodes
- CDS 130 Admitted Patient Care Finished General Episodes
- CDS 140 Admitted Patient Care Finished Delivery Episodes
- CDS 150 Admitted Patient Care Other Birth Events
- CDS 160 Admitted Patient Care Other Delivery Events
- CDS 180 Admitted Patient Care Unfinished Birth Episodes
- CDS 190 Admitted Patient Care Unfinished General Episodes
- CDS 200 Admitted Patient Care Unfinished Delivery Episodes
When to assign commissioner code
The Commissioner Assignment Method should be applied at the following dates for the described CDS types:
| CDS Type | Date |
| 011 (Emergency Care Data Set) | Emergency care arrival date |
| 020 (Outpatients) | Appointment Date |
| 120 (Admitted Patient Care Finished Birth Episodes) | DISCHARGE DATE (HOSPITAL PROVIDER SPELL) |
| 130 (Admitted Patient Care Finished General Episodes) | DISCHARGE DATE (HOSPITAL PROVIDER SPELL) |
| 140 (Admitted Patient Care Finished Delivery Episodes | DISCHARGE DATE (HOSPITAL PROVIDER SPELL) |
| 150 (Admitted Patient Care Other Birth Events) | DISCHARGE DATE (HOSPITAL PROVIDER SPELL) |
| 160 (Admitted Patient Care Other Delivery Events) | DISCHARGE DATE (HOSPITAL PROVIDER SPELL) |
| 180 (Admitted Patient Care Unfinished Birth Episodes) | START DATE (HOSPITAL PROVIDER SPELL) |
| 190 (Admitted Patient Care Unfinished General Episodes) | START DATE (HOSPITAL PROVIDER SPELL) |
| 200 (Admitted Patient Care Unfinished Delivery Episodes | START DATE (HOSPITAL PROVIDER SPELL) |
- The Commissioner Assignment Method should be applied to completed Admitted Patient Care spells in line with the NHS Payment Scheme/National Tariff/PbR timetable (i.e. during the period between actual discharge date and the published reconciliation and post reconciliation dates).
- The registered GP practice and postcode of usual address data that were valid at a spell’s admission date should be used when applying the Commissioner Assignment Method to Admitted Patient Care spell data (for either finished or unfinished spells).
- If registered GP practice and/or postcode of usual address data changed between admission date and discharge date in completed Admitted Patient Care spells, and if this causes a different commissioner to be derived, then the sub-ICB location responsible for payment is to be determined on the basis of GP registration (or, failing that, usual address), applied at the point of admission for that inpatient hospital spell. The sub-ICB location identified on this basis is responsible for payment for the whole of that hospital spell, even if the patient’s GP or address changes during the spell.
Determining and recording usual place of residence
This document assumes the same rules for deciding usual place of residence of a patient, as described in Appendix 2 in ‘Who Pays?’. The guidance is also maintained for determining the residency status of asylum seekers, patients residing in approved premises, bail accommodation, patients who move during treatment, people taken ill abroad, students/boarding school pupils and persons detained under the Mental Health Act (1983).
Providers should also ensure for any patients with a ‘No Fixed Abode’ postcode (ZZ99 3VZ) or ‘Address Not Known’ postcode (ZZ99 3WZ), or ‘England UK – not specified’ (Z99 3CZ) or ZZ99 3GZ – ‘Wales’; ZZ99 1WZ – ‘Scotland’; ZZ99 2WZ ‘Northern Ireland’, that they identify a usual place of residence based upon the address of the main site of the provider delivering the care and use this address when determining commissioning payment responsibilities. The default country of residence for these postcodes should be ‘England’ (on the rationale that only English providers submit CDS records to SUS).
Country code, where required in this document from the ONS NHS Postcode Directory, should be identified by using the ‘gridall.csv’ file4 from the NHS England ODS service.
Providers should not transmit the postcode of the main site of the provider delivering the care in the CDS itself for any patients who have no fixed abode as the ZZ99 3VZ postcode value may need to be used to segment this population group when undertaking analysis of health inequalities.
Providers should record the full address and postcode for patients from the UK home countries (Scotland, Wales, Northern Ireland). Providers should only use the pseudo postcodes for these countries (ZZ99 3GZ – Wales; ZZ99 1WZ – Scotland; ZZ99 2WZ Northern Ireland), if it is impossible to determine the full address and postcode for a patient.
Where a patient’s usual place of residence is overseas, providers should record the full address and use the relevant pseudo postcode to indicate the country of usual residence. The pseudo postcode list is maintained by the Office of National Statistics (ONS) as part of the ONS NHS Postcode Directory and can be found at the NHS England Organisation Data Services website.
Serving members of the armed forces will be registered with a Defence Medical Services (DMS) primary care practice. These are located within the UK or overseas. Registration details are held on the Ministry of Defence’s (MoD) health information system ‘DMICP’ (Defence Medical Information Capability Programme).
DMICP is integrated to the Patient Demographic Service on the Spine and the Spine’s demographic data for armed forces personnel are ‘civilianised’ by this integration. This is for security reasons as it prevents serving members of the armed forces being easily identifiable whilst in hospital. The civilianisation process removes rank and other military terminology from the patient demographic data and replaces the patient’s actual place of residence with a civilian form of the address of the DMS practice they are registered with. This address should be used as part of the Commissioner Assignment Method and not the actual address of the patient.
The same principle applies to serving personnel who are based overseas at a British Forces Post Office (BFPO) address and who return to the UK for treatment. The BFPO address should not be recorded as the usual place of residence for the security reason noted above. Instead, the patient’s DMS practice address should be used.
Commissioner Assignment Method flow chart methodology
The flow chart runs through a set of question steps, predominantly of a Yes/No type. These questions lead ultimately to an answer which identifies the commissioning organisation or organisation type with payment responsibility for the activity represented by the CDS activity record. Providers need to write the correct Organisation Data Services organisation code for this organisation in the ORGANISATION CODE (CODE OF COMMISSIONER) field in the CDS. The correct codes to denote commissioning responsibilities for the 2024/25 financial year are described in the NHS England Direct Commissioning Framework Responsibilities Matrix 2024/25 (Appendix A). These organisations are also described in more detail in section 10 below. This matrix/appendix also includes additional information regarding the potential uses of organisation code 13Q in relation to the production of contract monitoring data sets, when recorded alongside the specific Commissioned Service Category Codes (see Appendix J).
The Commissioner Assignment Method flow chart includes annotations for each process step which link to further explanatory detail in the table below. This detail includes derivation logic for each step, where required. This derivation logic uses fields from the in-scope CDS types, and where this is the case the field names are in uppercase, as per the convention in the NHS Data Dictionary. The flow chart logic also relies on several reference files and look-up tables. These are either references to national files or a provided look-up file. In some cases, the derivation logic for a process step explains explicitly how to deal with stated default data values for CDS fields and how the relevant question should be answered for these values. If the derivation logic does not explicitly state how to deal with unstated default codes, invalid or Null or Blank values within a CDS field, then the derivation logic should be followed explicitly. For example, if a question requires a specified value or values to be present in a CDS field for the answer to be ‘Yes’, then any other value in the CDS field, including Null or Blank records, would be answered ‘No.’ This approach should ensure that a commissioner code can be assigned to all CDS records.
Flow chart key
Assigned commissioners and commissioner code logic
The below describes the main commissioner types (known as the ‘Assigned Commissioner’), which are derived from following the Commissioner Assignment Method flow chart, and provides guidance for providers to determine which specific commissioner code to apply in CDS records. For example, the Commissioner Assignment Method may suggest a ‘Host sub-ICB location’ is the responsible commissioner type and this table will then help identify which specific sub-ICB location organisation code is appropriate.
Host sub-ICB location
The host sub-ICB location of a healthcare provider is the sub-ICB location within which the address of the provider’s main site is located.
‘Host sub-ICB location’ is derived as follows:
1. Establish main site of the healthcare provider from the CDS field: ORGANISATION CODE (CODE OF PROVIDER).
2. Derive postcode of the address of the provider’s main site by looking up the provider code in the ODS reference file ‘etr.csv’ and extracting the provider’s postcode.
3. Look up the extracted provider postcode in the ONS NHS Postcode Directory and derive the responsible sub-ICB location from the Postcode Directory for the matching record.
4. Local interpretation of these rules may be required for cases where the host sub-ICB location is not identified via this logic – this may occur in cases where providers have merged, resulting in a change to the main site of the trust HQ of a provider. In this case, local logic may be applied in the short term so that the host sub-ICB location is derived appropriately to meet local financial allocations*.
*Commissioners and providers should be encouraged to use the definition for host sub-ICB location suggested by this document. Where this would result in a shift of activity between sub-ICB locations, local commissioners and finance leads should be engaged to ensure appropriate adjustments are made locally. It is recognised that it may not be possible to implement the change to this definition of host sub-ICB location immediately.
Responsible sub-ICB location
The responsible sub-ICB location is based on the sub-ICB location which a patient’s registered GP belongs to. For patients who are not registered with any GP, the responsible sub-ICB location is the sub-ICB location within which the patient is usually resident.
Responsible sub-ICB location is typically derived as follows:
If the value of the CDS field GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) is either Null or Blank, or V81999 (registered GP Practice Code not known) or V81998 (registered GP Practice code not applicable) or V81997 (No registered GP Practice), or if the patient (adult or child) is part of the health and justice population (POSTCODE OF USUAL
ADDRESS is populated with a postcode value contained within the list of organisations detailed in Appendix F), or if the patient is registered with an English Defence Medical Services (DMS) GP Practice then utilise a postcode-methodology; take the value from the CDS field POSTCODE OF USUAL ADDRESS** and look up this postcode value in the ONS NHS Postcode Directory and derive the responsible sub-ICB location commissioner from the value in the Directory’s sub-ICB location field for the matching record;
ELSE look up the value of GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) in the ODS ‘epraccur’ file where the record has a ‘National Grouping’ value NOT equal to ‘W00’ AND if the record has a Status Code in the national GP file ‘epraccur’ of either A (active) or P (proposed) on the assignment date (as defined in section 5) and derive the responsible sub-ICB location commissioner from ‘epraccur’ (‘Code for the Commissioning Organisation’).
If there is no match to a record in ‘epraccur’, then revert to the postcode methodology.
If the CDS field: POSTCODE OF USUAL ADDRESS is populated with an ‘Unable to be allocated’ pseudo postcode (ZZ99 3WZ or ZZ99 3VZ), ‘England UK – not specified’ (Z99 3CZ), or ZZ99 3GZ – ‘Wales’; ZZ99 1WZ – ‘Scotland’; ZZ99 2WZ ‘Northern Ireland’, or is missing, then identify a usual place of residence based upon the address of the main site of the provider delivering the care and use this address when determining commissioning payment responsibilities. For the purposes of clarity, the pseudo postcode stored in the CDS record should not be replaced.
It is important to note that for looked after children, aged under 18, who are placed outside of their original sub-ICB location (Who Pays? Paragraph 15), the commissioning and payment responsibility will remain with the original sub-ICB location, and be different to which is defined by this process. This cannot be identified from CDS records, but relies on local validation and data. This is described in more detail in the Who Pays? guidance.
** The Spine is assumed to be the definitive record of a patient’s demographic and GP registration details. There are occasions where there might be a discrepancy between the patient postcode supplied by the National Spine Patient Demographic Service (PDS) and the patient postcode provided by the patient and recorded in the Provider CDS submission at the time of care. This may be since PDS can take some time to be updated after a change of address or GP details. If there is evidence that the demographic data on PDS was incorrect when the patient presents for care at a provider, then there may be a valid case to use patient-supplied data and submit this in the CDS submission.
Private Patient/Chargeable Overseas Visitor (COV)
If a patient is a private patient, or a Chargeable Overseas Visitor (COV), the default ODS code of VPP00 should be used as the commissioner code for these patients.
NHS England Armed Forces Commissioning Hub
Who Pays? guidance states that NHS England is responsible for commissioning secondary health services for members of the armed forces who are registered with an English Defence Medical Services (DMS) GP Practice and for the members’ families where they are registered with an English DMS practice.
Providers should use the ‘Parent Organisation Code’ for the English DMS practices in the ‘epraccur’ reference file – ‘13Q’ as the commissioner code for NHS England commissioned armed forces activity. 13Q is the code of the ‘NHS England Commissioning Hub 1’, which was set up to support the implementation of Choose and Book services for DMS practices. The use of this value together with the location of the DMS Practice (i.e. England, Scotland, Wales, Northern Ireland or Overseas) will unambiguously identify the correct commissioning organisation for the eligible armed forces population in commissioning data sets.
If the member of the armed forces, or their families, are not registered with an English DMS practice then their commissioner will be a non-armed forces commissioner.
NHS England Specialised Commissioning Hub
From 2024/25 some specialised services are being delegated from NHS England to ICBs. The different services and their ‘status’ are available from the ‘Delegated NHS England Functions – Supporting Resources’ Future NHS page.
Where a CDS record has been identified as being for specialised care, then the relevant responsible NHS England Specialised Commissioning Hub will be responsible for paying for the care described by the CDS record.
NHS England regional geographies with commissioning responsibility for specialised services (‘Specialised Commissioning Hubs’) agree contracts for specialised services with specified UK NHS and independent providers. The Specialised Commissioning Hubs are described in the NHS England Direct Commissioning Framework Responsibilities Matrix 2024/25 (Appendix A).
Providers MUST NOT use the redundant organisation code ‘YDD82’ as a commissioner code within the CDS.
The relevant responsible NHS England Regional Geography is derived in two different ways. Services that are not delegated (e.g. nationally retained “red services”) use the provider method (as in previous years) and others use the GP practice of the patient.
Provider method:
Take the value from the CDS field ORGANISATION CODE (CODE OF PROVIDER), and look this value up in the list of specified UK providers who have agreed contracts with NHS England Specialised Commissioning Hubs, as specified in the Provider to Commissioning Hub Mapping, which is available from ODS, and then use this to derive the corresponding NHS England Specialised Commissioning Hub code.GP practice method:
Look up the value of GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) in the ODS ‘epraccur’ file where the record has a ‘National Grouping’ value NOT equal to ‘W00’ AND if the record has a Status Code in the national GP file ‘epraccur’ of either A (active) or P (proposed) on the assignment date (as defined in section 5) and get the National Grouping (NHS England Region), then lookup this value in Appendix A to derive the corresponding NHS England Specialised Commissioning Hub code.
If there is no match to a record in ‘epraccur’, then revert to the provider method.
Where a specific element of specialised service has been agreed to be funded nationally, and therefore given a commissioner code of 13Q, the associated commissioned service category code must be that for a specialised service. A list of the commissioned service category codes can be found at Appendix J.
NHS Scotland National Services Division
The Scottish devolved administration is responsible for paying for all specialised care at English providers for Scottish residents, not covered by pre-existing legacy agreements with NHS England.
The National Services Division of NHS Scotland is the responsible commissioner for specialised care for Scottish residents by managing a pool of funds (risk share scheme) on behalf of Health Boards to pay for individual patient referrals for a “prescribed” list of specialised services in England which are not included in the service agreement with NHS England.
Providers should use the ODS code ‘SD002’ for the NHS Scotland Health National Services Division, as defined in the ODS ‘scotorg’ reference file, as the commissioner code for this activity.
Scottish Health Board
Scottish Health Boards (SHBs) have a responsibility to provide for the health care of patients living within their boundaries, i.e. patients who are “ordinarily resident” in their area. Scottish Health Boards are responsible for paying for non-specialised admitted and outpatient activity for their residents. The responsible Scottish Health Board is derived from the patient’s postcode of place of usual residence, via the ONS NHS Postcode Directory.
Scottish Health Boards are also responsible for paying for care provided to patients registered within Scottish Defence Medical Services Practices. There is no mapping between Scottish DMS practices and Scottish Health Boards, so the correct Scottish Health Board should be derived from a patient’s postcode of usual address which will be the postcode of the DMS practice itself.
Providers should use the ODS for codes in the range SA9 to SZ9, as defined in the ODS ‘scotorg’ reference file, as the commissioner code for this activity. Take the value from the CDS field POSTCODE OF USUAL ADDRESS and look this postcode value up in the ONS NHS Postcode Directory and derive the responsible Scottish Health Board for the matching record.
Northern Ireland Health and Social Care Board
The Northern Ireland Health and Social Care Board is responsible for paying for all other specialised care, not covered by pre-existing legacy agreements with NHS England, for its residents in English providers. It is also responsible for paying for non-specialised admitted and outpatient activity for its residents.
The Northern Ireland Health and Social Care Board discharges its commissioning responsibilities via its five Local Commissioning Groups (LCGs) who commission care for their resident population, therefore the responsible LCG is derived from the patient’s postcode of place of usual residence.
Welsh Local Health Board
The Welsh devolved administration is responsible for paying for care, which is not covered by existing legacy agreements with NHS England for its residents receiving highly-specialised care at English providers. It is also responsible for paying for care provided to patients registered within Welsh Defence Medical Services Practices. It holds payment responsibility for patients residing on both sides of the English/Welsh Border as defined within the Protocol for Cross-Border Healthcare Services. It also holds payment responsibility for services from English providers provided to patients residing in the rest of Wales.
NHS Wales discharges its specialised services commissioning responsibility through the Welsh Health Specialised Services Committee (Wales). Other commissioning responsibilities are covered by the various Welsh Local Health Boards (LHB) who are responsible for planning, funding, designing, developing and securing the delivery of primary, community and in-hospital care services for residents in their respective areas and the responsible body will be established because of the LHB area where the person is usually resident16. Therefore, the responsible LHB is derived from the patient’s postcode of place of usual residence.
However, because of the Welsh Cross-Border protocol, it is possible for an LHB to be the responsible commissioner for patients who are resident in England, specifically for those patients who are resident on the English side of the border who are registered with a Welsh border GP practice.
There is no mapping between Welsh DMS practices and Welsh Local Health Boards, so the Welsh Local Health Board should be derived from a patient’s postcode of usual address which will be the postcode of the DMS practice itself.
For patients that are resident in Wales: take the postcode recorded in the CDS field: POSTCODE OF USUAL ADDRESS and look this up in the ONS NHS Postcode Directory where the relevant Welsh Local Health Board organisation code is listed for the matching record.
If the CDS field: POSTCODE OF USUAL ADDRESS is populated with the default pseudo postcode for Wales (ZZ99 3GZ) rather than a specific Welsh postcode then it will not be possible to allocate a specific Welsh Local Health Board organisation code and instead the code for the Welsh Government (W01) should be used instead.
For patients resident on the English side of the Wales-England border and who are registered with a Welsh GP: take the value from CDS field GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) and look this up in the ODS ‘epraccur’ file and extract the postcode of the relevant GP Practice. Look this derived postcode up in the ONS NHS Postcode Directory where the relevant Welsh Local Health Board organisation code is listed for the matching record.
Welsh Health Specialised Service Committee
NHS Wales discharges its specialised services commissioning responsibility through the Welsh Health Specialised Services Committee (Wales).
The Welsh Health Specialised Service Committee (WHSCC) are hosted by the CWM TAF UNIVERSITY Local Health Board, with a site code 7A5HC. This code should be used as the commissioner code for CDS records where Wales is responsible for paying for specialised care activity.
The Referral Assessment Service (RAS) system has been introduced for when referring English resident cross border patients (who are registered with Welsh border GP practices who have opted into the service) for consultant led secondary care (community services, mental health and urgent suspected cancer referrals are not included). This is summarised below:
Patient’s residency: England
GP registration: Wales
Patient referred by: GP via RAS
Legally responsible body: NHSE
Body which will pay for patient’s care: LHB via WHSSC
English provider: NHS England Constitution
Welsh provider: NHS Wales standards
Patient’s residency: England
GP registration: Wales
Patient referred by: GP referral other than via RAS (Note: Only a specified list of GPs use RAS)
Legally responsible body: NHSE
Body which will pay for patient’s care: NHSE
English provider: NHS England constitution
Welsh provider: NHS Wales standards
Responsible Local Authority
Local Authorities have a duty to improve the health of the people in their areas, funded by a ring-fenced grant. Local Authorities fulfil this duty by commissioning a range of services from providers (e.g. sexual health, smoking cessation).
If the Local Authority services are commissioned from a secondary care provider and a standard CDS flow is used to record the activity, then the responsible commissioner in the data set will need to be the relevant Local Authority organisation.
The default assumption used in this guidance is that each local authority will be responsible for commissioning relevant services for their resident population, specifically those people whose ordinary place of residence is within the geographic boundary of the local authority.
Take the value from the CDS field POSTCODE OF USUAL ADDRESS and look this postcode value up in the ONS NHS Postcode Directory and derive the responsible local authority for the matching record.
Responsible NHS England Regional Geography for Public Health Services
All NHS England Regional Geographies have commissioning and payment responsibility for certain public health services (see Appendix A), therefore the correct Regional Geography code should be used to populate the commissioner code within the CDS for activity records pertaining to these services.
Each NHS England Regional Geography commissioning team commissions public health services for their responsible population which is defined as anyone registered with a GP practice located within the regional geography’s boundary or anyone, not registered with any GP, who lives within the regional geography’s boundary.
Take the value from the CDS field GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION):
If this value is either V81999 (registered GP Practice Code not known) or V81998 (registered GP Practice code not applicable) or V81997 (No registered GP Practice), then take the value from the CDS field POSTCODE OF USUAL ADDRESS and look this postcode value up in the ONS NHS Postcode Directory and derive the code for the responsible Region from the value in the Directory’s ’NHSE Regional’ field for the matching record;
ELSE if this value relates to a non-BFPO DMS practice (i.e. those practices, active or proposed (‘epraccur’ status code equal to ‘A’ or ‘P’) on the assignment date (as defined in section 5), where the value in the ODS ‘epraccur’ file of the practice’s ‘Commissioning Organisation’ code = ‘13Q’ AND the postcode of the practice address does not correspond to the form ‘BFn nAA’), then take the postcode of the organisation from ‘epraccur’, look this postcode value up in the ONS NHS Postcode Directory and derive the responsible NHS England commissioner from the value in the Directory’s region field for the matching record. It should not be necessary to accommodate CDS records relating to BFPO practice registrants when assessing commissioning responsibility for public health section 7a activity as these records will be deemed to be relating to patients who are charge-exempt overseas visitors and will have been filtered out at a preceding part of the flow chart.
ELSE look up the value in the ODS ‘epraccur’ file and derive the code for the responsible Regional Geography from ‘epraccur’.
If there is no match to a record in ‘epraccur’ then revert to the postcode methodology: take the value from the CDS field POSTCODE OF USUAL ADDRESS and look this postcode value up in the ONS NHS Postcode Directory and derive the responsible NHS commissioner from the value in the Directory’s region field for the matching record.
Secondary Care Dental (SCD) Services
NHS England previously had commissioning and payment responsibilities for secondary dental care, this has now been transferred to sub-Integrated Care Board locations. This will be based on responsible sub-ICB location, as described above.
Commissioning hub for Health and Justice Commissioning
NHS England Regional Geographies are responsible for health and justice commissioning (see Appendix A). The NHS England Regional Geography teams commission secondary care based on which prison, Immigration Removal Centre (IRC), children and young people secure estate setting (Young Offender Institution holding under 18s, Secure Children’s Home, Secure Training Centre).
The responsible Health and Justice Commissioning Hub code to site relationship is given in Appendix F, which shows which of the Health and Justice commissioning hubs are responsible for which prison/children and young people secure estate setting/detention centre.
To find the commissioning hub code: take the postcode value from the CDS field: POSTCODE OF USUAL ADDRESS and look this up in Appendix F.
The responsible commissioner can be obtained for the matching record.
The ODS has implemented new Health and Justice Commissioning Hub codes for this activity to facilitate easier identification of health and justice activity within CDS records. It is anticipated that the further ODS reference data release changes will permit derivation of commissioning hub without the need for Appendix F in future versions of the Commissioner Assignment Method.
See Overseas Visitor Guidance
Detailed interpretation of the overseas visitors’ guidance is beyond the scope of the Commissioner Assignment Method documentation. Specific guidance to determine whether a patient is an overseas visitor and whether an overseas visitor is exempt from charges, in whole or part, (referred to as Charge Exempt Overseas Visitors (CEOV)) is detailed within the various Department of Health and Social Care (DHSC) documents on overseas visitor charging and the additional NHS England guidance for recovering costs for overseas visitors. As detailed in the NHS England Who Pays? guidance, the commissioner for CEOV is:
- the sub-ICB location, for a CEOV who is currently registered with a GP in England – or who is not currently registered with a GP in England, but who gives a UK address and can be considered part of the UK resident population
- the ICB in which the organisation providing the relevant health services is physically located, for a CEOV who is not registered with a GP in England and who is resident outside the UK.
However, it is noted from the DHSC guidance that there are many types of International Healthcare Agreements, and there may be occasions where local agreements exist with providers and non-UK commissioners that may need a different commissioner code to be applied. Local understanding is required to interpret the rules and regulations for these cases.
Flow chart annotations
The table below annotates the steps of the Commissioner Assignment Method process, giving guidance to assign the commissioner for CDS records.
| Assignment Process | |||
| Code | Description | Comments / Logic | Assigned Commissioner |
| A&E-1 | This question checks whether the patient is usually resident in England. | Residency will need to be defined by the postcode of the patient’s usual address. For serving members of the armed forces based in the UK, the address of their DMS practice will be used as a proxy for their place of usual residence. If the CDS field: POSTCODE OF USUAL ADDRESS is a postcode from within England (i.e. where the value of the ‘Country’ field for that postcode in the ONS NHS Postcode Directory is equal to E92000001, then the answer to question 2 is ‘Yes’, else the answer is ‘No’. If the CDS field: POSTCODE OF USUAL ADDRESS is populated with an ‘Unable to be allocated’ pseudo postcode (ZZ99 3WZ or ZZ99 3VZ), ‘England UK – not specified’ (Z99 3CZ), or ZZ99 3GZ – ‘Wales’; ZZ99 1WZ – ‘Scotland’; ZZ99 2WZ ‘Northern Ireland’, or is missing, then identify a usual place of residence based upon the address of the main site of the provider delivering the care and use this address when determining commissioning payment responsibilities. In these cases, the answer to question 2 is ‘Yes’. | Yes:- J No:- sub-ICB location |
| A | This question identifies chargeable overseas visitors (COV) and private patients. | Providers must assess a patient’s liability for NHS charges and record appropriate data in the OVERSEAS VISITOR CHARGING CATEGORY and ADMINISTRATIVE CATEGORY fields of the CDS. If the CDS field OVERSEAS VISITOR CHARGING CATEGORY is populated with the value D or F OR if the CDS field ADMINISTRATIVE CATEGORY is populated with the value ‘02’ (Private Patient) then the answer to this question is ‘Yes’ else the answer is ‘No’. |
Yes:- Private Patient / COV (VPP00) No:- B |
| B | This question checks whether the patient is ordinarily resident within the UK and if their usual place of residence is in either England, Wales, Scotland or Northern Ireland. |
Chapter 5 in the Department of Health and Social Care guidance on charging overseas visitors in England describes what is meant by the term ‘ordinarily resident’ and what tests can be performed to determine if a patient is ordinarily resident in the UK. Note that ‘ordinarily resident’ is different to ‘usually resident’. The former relates to a person’s eligibility for NHS treatment without charge, whereas the latter relates to a person’s actual address where they are living. Patients who are ordinarily resident in the UK must have an OVERSEAS VISITOR CHARGING CATEGORY value of A (whilst charging category A is mainly for ordinary residents of the UK the category also includes one type of CEOV, i.e. failed asylum seekers who are in receipt of support under section 95 or section 4(2) of the Immigration Act 1999). Any patient deemed to be not ordinarily resident in the UK (i.e. an overseas visitor) must have the CDS field OVERSEAS VISITOR CHARGING CATEGORY populated with a value of B, C, D, E, or F, depending on their charging status. (Chargeable overseas visitors have an OVERSEAS VISITOR CHARGING CATEGORY value of D or F and will have already been identified in Step A of the assignment process.) A patient’s usual place of residence, and whether this is within the UK or overseas, needs to be established by following the explicit guidance in the Who Pays? guidance. An overseas address should use the ONS pseudo postcodes, starting with ZZ99, to record country of residence. For patients registered with a DMS practice the patient’s actual address will be civilianised by the DMICP-PDS link for security reasons and any patient registered with an overseas DMS practice will be deemed to be living overseas. The address for these practices is recorded in ‘epraccur’ and they are listed with a British Forces Post Office (BFPO) postcode with the form ‘BF1 nAA’ or ’BF2 nAA’. BFPO postcodes are not listed in the ONS NHS Postcode Directory and care must be taken when using postcode reference data to determine country of residence for these patients. DHSC guidance lists the locations of these BFPO post locations. Patients who are ordinarily resident in Bailiwick of Guernsey, Jersey or the Isle of Man may present at English providers for treatment and provide an English address as a temporary residence whilst being treated. In these cases, it is necessary to identify these patients via the use their registered GP practice code. If OVERSEAS VISITOR CHARGING CATEGORY = B, C, D, E or F then the answer to this question is ‘No’. Else if OVERSEAS VISITOR CHARGING CATEGORY = A then find value of CDS field GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) AND look this value up in ODS national GP Practice file ‘epraccur’ for those practices, active or proposed (‘epraccur’ status code equal to ‘A’ or ‘P’) on the assignment date, and if the derived GP Practice record has is a BFPO postcode with the form ‘BF1 nAA’ or ’BF2 nAA’ then the answer to this question is ‘No’. Else if OVERSEAS VISITOR CHARGING CATEGORY = A then find value of CDS field GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) AND look this value up in ODS national GP Practice file ‘epraccur’ for those practices, active or proposed (‘epraccur’ status code equal to ‘A’ or ‘P’) on the assignment date , and if the derived record has a ‘High Level Health Geography’ code (in ‘epraccur’) of either YAC, YAD, YAE or YAF on the assignment date then the answer to this question is ‘No’. Else if OVERSEAS VISITOR CHARGING CATEGORY = A then if the CDS field: POSTCODE OF USUAL ADDRESS is a postcode from a UK home country (i.e. where the value of the ‘Country’ field for that postcode in the ONS NHS Postcode Directory is equal to either E92000001, W92000004, S92000003 or N92000002) then the answer to this question is ‘YES’, else the answer is ‘No’. If the CDS field: POSTCODE OF USUAL ADDRESS is populated with an ‘Unable to be allocated’ pseudo postcode (ZZ99 3WZ or ZZ99 3VZ), ‘England UK – not specified’ (Z99 3CZ), or ZZ99 3GZ – ‘Wales’; ZZ99 1WZ – ‘Scotland’; ZZ99 2WZ ‘Northern Ireland’, or is missing then identify a usual place of residence based upon the address of the main site of the provider delivering the care and use this address when determining commissioning payment responsibilities. |
Yes:- WB-1 No:- B-1 |
| B-1 | Checks whether the activity record pertains to highly- specialised care. |
Is the specialised service line code for the CDS record derived by the specialised services identification rules one of those listed as a Highly Specialised Service Line in the list of Specialised and Highly-Specialised Service Line Codes (see Appendix C for further details), if so the answer to this question is ‘Yes’ else the answer is ‘No’. |
Yes:- B-2 No:- B-3 |
| B-2 | This question requires providers to identify whether the CDS record is for care provided to a patient who is usually resident in an EEA member state who has right of access to English highly-specialised services under arrangements governed by Healthcare Agreements. |
Providers should record a ZZ99 pseudo-postcode within the CDS to identify a patient’s country of residence. The total list of EU states is defined as: Austria, Belgium, Bulgaria, Croatia, Cyprus (Southern), Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Republic of Ireland, Romania, Slovakia, Slovenia, Spain, Sweden. Switzerland, Norway, Iceland and Liechtenstein have separate agreements with the UK. Appendix H lists the ‘ZZ99’ pseudo postcode for each of the member states above. If the CDS field: POSTCODE OF USUAL ADDRESS is a pseudo-postcode representing an EEA member state country whose residents have right of access to English highly-specialised services (relevant pseudo postcode values are listed in appendix H), then the answer to this question is ‘Yes’, else the answer is ‘No’. |
Yes:- Responsible NHS England Specialised Commissioning Hub (based on Provider Mapping Table) No:- Box B-3 |
| B-3 | Is the activity covered by an arrangement outside regular overseas visitor charging rules? |
Specific guidance to determine the correct commissioner for those overseas visitors who are eligible for NHS care without charge (in whole or part), due to International Healthcare Agreements, other international agreements or general exemptions is detailed within the various Department of Health and Social Care documents on overseas visitor funding, the NHS England Who Pays? guidance, and the additional Who Pays? guidance for recovering costs for overseas visitors. The default rule for overseas visitors who are exempt from charges (Referred to as Charge Exempt Overseas Visitors (CEOV)) due to an International Healthcare Agreement is that an sub-ICB location (either host or responsible) will be the commissioner, and will recover costs for overseas visitors, as described in the additional guidance. It is noted from the DHSC guidance that there are many types of International Healthcare Agreements, and there may be occasions where local agreements exist with providers and overseas commissioners that may need a different commissioner code to apply. Local understanding is required to interpret the rules and regulations for these cases, Armed Forces personnel (or their dependents) who are stationed overseas and registered with an overseas DMS practice and who return to England for secondary care treatment are classed as charge-exempt overseas visitors and as such an sub-ICB location (either host or responsible) is responsible for paying for their care, and not NHS England. |
No:- B-4 Yes:- See OSV Guidance |
| B-4 | Residential Population Check |
Checks to see whether an overseas visitor patient is part of the UK residential population for funding purposes. The Who Pays? guidance distinguishes between those charge-exempt overseas visitors (CEOV) who are part of the residential population and those who are not. This distinction is purely to determine whether the sub- ICB location or responsible sub-ICB location should pay for the care provided to the CEOV. If a CEOV patient is registered with an English GP (and who may also give an English address as their place of usual residence. Note usual residence does not mean the same as ordinary residence – see Comments/Logic regarding question (C)). Then they are considered part of the residential population for funding purposes. CEOV who are not registered with an English GP (and who may also not give an English address as their place of usual residence) are not considered as part of the residential population for funding purposes. Take the value from the CDS field GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION); IF this value is neither V81999 (registered GP Practice Code not known) or V81998 (registered GP Practice code not applicable) or V81997 (No registered GP Practice). AND if the value in the national GP file ‘epraccur’ has a ‘National Grouping’ value NOT equal to ‘W00’ OR if this value is not Null or Blank. AND if the record has a Status Code in the national GP file ‘epraccur’ of either A (active) or P (proposed) on the assignment date. THEN the patient is registered with an English GP Practice and the answer to this question is ‘Yes’. |
Yes:- Responsible sub- ICB location No:- Host sub-ICB location |
| WB-1 | Under an agreement between Wales and England, for those patients usually resident in a defined set of Welsh administrative areas and English counties on the Wales-England border and registered with a Welsh GP, then a Welsh Local Health Board will be responsible for paying for the patient’s care and not an English NHS organisation. |
The appropriate Welsh Local Health Board is responsible for paying for care for patients registered with a Welsh border GP and usually resident in one of the defined Welsh administrative areas or English counties described within the agreement between Wales and England. Residency in the relevant geographies is based on sub-ICB location boundaries in England and Welsh administrative areas in Wales. If the value recorded in the CDS field GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) maps to one of the following Welsh Local Health Board codes (7A1, 7A2, 7A3, 7A4, 7A5, 7A6 or 7A7) for active or proposed GP practices (‘epraccur’ status code equal to ‘A’ or ‘P’) on the assignment date in the ‘commissioner’ in the ODS GP Practices in England and Wales reference file ‘epraccur’ AND if the postcode value from the CDS field: POSTCODE OF USUAL ADDRESS maps in the ONS NHS Postcode Directory to either one of the following codes: ‘QYG’ (NHS Cheshire and Merseyside ICB); QOC (NHS Shropshire, Telford and Wrekin ICB);; QGH (NHS Herefordshire and Worcestershire ICB); ‘QR1’ (NHS Gloucestershire ICB); ‘QUY’ (NHS Bristol, North Somerset and South Gloucestershire ICB). (OR if the post code value from the CDS field: POSTCODE OF USUAL ADDRESS maps in the ONS NHS Postcode Directory to one of the following Welsh Unitary Authorities: ‘W06000005’ (Flintshire); ‘W06000006’ (Wrexham); ‘W06000023 (Powys); ‘W06000021’ (Monmouthshire’); ‘W06000004’ (Denbighshire] then the answer to this question is ‘Yes’ else the answer is ‘No’. |
Yes:- C No:- WB-2 |
| WB-2 | Under an agreement between Wales and England, for those patients usually resident in a defined set of Welsh administrative areas and English counties on the Wales-England border and registered with an English GP, then an English NHS organisation will be responsible for paying for the patient’s care. |
As described in rule WB-1 above, the Wales-England Border agreement covers responsibility and payments for care for patients residing in one of the defined Welsh administrative areas or English counties defined within the cross-border agreement. If the value recorded in the CDS field GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) indicates an active or proposed English GP Practice on the assignment date (where the corresponding Higher Level Health Geography code in ‘epraccur’ <> Q99, YAC, YAD, YAE, YAF), and the patient has a home address as determined from the POSTCODE OF USUAL ADDRESS in either of the Welsh Local Health Board or English border areas as defined in the guidance for question WB-1, then the answer to this question is ‘Yes’. If they live outside of the border agreement area or within the agreement area but without a GP, the answer is ‘No’. If the patient is not registered with a GP, but resides in the border area, the responsibility for payment is covered by residence rules as covered in the subsequent question. |
Yes:- C-0 No:- WB-3 |
| WB-3 | This question checks whether the patient is usually resident within England, or otherwise within Scotland, Wales or Northern Ireland. |
Residency will need to be defined by the postcode of the patient’s usual address. For serving members of the armed forces based in the UK, the address of their DMS practice will be used as a proxy for their place of usual residence. If the CDS field: POSTCODE OF USUAL ADDRESS is a postcode from within England (i.e. where the value of the ‘Country’ field for that postcode in the ONS NHS Postcode Directory is equal to E92000001, then the answer to question 2 is ‘Yes’, else the answer is ‘No’. If the CDS field: POSTCODE OF USUAL ADDRESS is populated with an ‘Unable to be allocated’ pseudo postcode (ZZ99 3WZ or ZZ99 3VZ), ‘England UK – not specified’ (Z99 3CZ), or ZZ99 3GZ – ‘Wales’; ZZ99 1WZ – ‘Scotland’; ZZ99 2WZ ‘Northern Ireland’, or is missing, then identify a usual place of residence based upon the address of the main site of the provider delivering the care and use this address when determining commissioning payment responsibilities. |
Yes:- C-0 No:- C |
| C | This question checks whether the activity record pertains to specialised or highly specialised care. |
Specialised and highly-specialised services are identified via the application of the Identification Rules for Prescribed Specialised Services (the IR). NHS England has developed a prescribed specialised services identification rules software tool, maintained by NHS England, which can be used to identify spells and outpatient attendances that represent specialised activity, some of which may be chargeable via a national tariff as part of the National Tariff Payment System. It is important to note that the identification rules software tool is not alone a sufficient means to identify specialised activity in CDS flows as full application of the IR requires the use of additional non- CDS data sets and logic. Providers should apply the rules in full using these other resources as required. See Appendix B for further information regarding specialised service lines. Providers are expected to use the version of the tool from NHS England that is applicable for the year of activity. It is anticipated that this will cover most specialised care, however, should there be local discrepancies, providers should check with their local Specialised Commissioning Hub and seek further advice. A general rule is that if any episode within a spell is specialised, then the whole spell should be considered specialised. If the identification rules software tool flags an episode or episodes in a spell as specialised but does not flag the spell as specialised and chargeable under national tariff arrangements, then the spell should still be considered as a specialised spell for the purposes of commissioner assignment. Likewise, if the full application of the IR logic (including local derogations and deviations) indicates that a spell is specialised, even if the identification rules software tool does not identify any spell or episode within it as specialised, then the spell should still be flagged as specialised. The exceptions to the above rule are where a spell contains unbundled chemotherapy or radiotherapy Healthcare Resource Groups (HRGs) that are specialised and paid for by NHS England, where there are no other episode or spell level flags for specialised care, and where the core HRG for the spell is not either SB97Z or SC97Z (same day chemotherapy or radiotherapy delivery respectively). In this scenario the specialised service line code should only be written into the episode that contains the unbundled HRGs (i.e. the entire spell is not deemed as specialised). Unbundled critical adult care (HRGs: XC01Z-XC07Z) is only regarded as specialised where the core spell itself has been identified as specialised. Unbundled neonatal critical care (HRGs: XA01Z-XA04Z and XA06Z) is paid for by NHS England but the core spell is chargeable to an sub-ICB location, unless that itself has been identified as specialised by the identification rules software. Unbundled paediatric critical care (HRGs: XB01Z-XB09Z) within a Paediatric Intensive Care Unit (PICU) or Paediatric High Dependency Unit (PHDU), is paid for by NHS England but the core spell is chargeable to a sub-ICB location, unless that itself has been identified as specialised by the identification rules software. NHS England does not commission paediatric intensive / high dependency care in general paediatric wards or adult intensive care units. For these and other instances where the only specialised care is expressed via unbundled HRGs, then the relevant specialised service line code should only be written into the episode that contains the unbundled HRGs (i.e. the entire spell is not deemed as specialised). Where an entire spell is designated as specialised using the above logic then providers should record a specialised service line code into the SERVICE CODE (CDS v6.3) or NHS SERVICE AGREEMENT LINE NUMBER (CDS v6.2) CDS field for every episode record in the spell. The service line code used should be the service line for the spell (i.e. each episode in a specialised spell will contain the same spell-level service line code). Likewise, the relevant Specialised Commissioning Hub code should be written into the Organisation Code (Code of Commissioner) CDS field for every episode in a spell deemed as specialised. If an outpatient attendance is designated as specialised, then providers should record a specialised service line code into either the SERVICE CODE (CDS v6.3) or the NHS SERVICE AGREEMENT LINE NUMBER (CDS v6.2) CDS field for the outpatient attendance CDS record. |
Yes:- C-1 No:- Welsh Health Specialised Services Committee/Scotland National Services Division/N Ireland Health and Social Care Board |
| C-0 | The same as code C |
Please see code C. |
Yes:- C-0a No:- D |
| C-1 |
NHS England commissions highly specialised services on behalf of patients from Scotland, Wales and Northern Ireland. These ‘Pre- 1991’ services were commissioned prior to health becoming a devolved function. Scotland and Northern Ireland have additional agreements for extra highly specialised services that are commissioned by NHS England. |
Appendix C lists the highly specialised services that are included in the ‘Pre- 1991’ agreement. The extra services for Scotland and Northern Ireland are listed in Appendix C Part A (Scotland) and Part B (Northern Ireland). Providers need to check whether the specialised service line code is in these lists. Other highly specialised services not specifically listed should be assigned to the Local Health Board or equivalent. If the SERVICE CODE (CDS v6.3) or NHS SERVICE AGREEMENT LINE NUMBER (CDS v6.2) CDS field contains a value contained within the list of specialised service line codes in Appendix C then the answer to this question is ‘Yes’ else the answer is ‘No’. |
No:- WB10 Yes:- Responsible NHS England Specialised Commissioning Hub |
| WB-10 |
The same as code WB1 |
Please see code WB1 |
Yes:- C3 No:- Welsh Health Specialised Services Committee/Scotland National Services Division/N Ireland Health and Social Care Board |
| C-0a |
Some specialised services are in scope for delegation. This question checks whether the service is in scope for delegation, or not. |
The different services and their ‘status’ are available from the ‘Delegated NHS England Functions – Supporting Resources’ Future NHS page. Take the service line for the activity and if it is in the list the answer to this question is ‘Yes’ else the answer is ‘No’. |
Yes:- C-0b No:- C-2 |
| C-0b |
Some specialised services are considered green and ready for delegation. This question checks whether the service is green and ready for delegation. |
Specialised services are split into red, amber and green services. This question tests whether the service is a green service, or not. The different services and their ‘status’ are available from the ‘Delegated NHS England Functions – Supporting Resources’ Future NHS page. Where the service line is listed as a green service, and so ready for delegation, the answer to this question is ‘Yes’ else the answer is ‘No’. Where the answer is no, the assigned commissioner should be the Responsible NHS England Specialised Commissioning Hub, based on the GP practice of the patient. |
Yes:- D No:- Responsible NHS England Specialised Commissioning Hub (GP Practice) |
| C-2 |
NHS England Regional Geographies have agreed contracts with specific providers of specialised services. This question checks whether the specialised care has been provided by a contracted provider. |
The specialised service contracts specify which services are provided by which providers and which NHS England Specialised Commissioning Hub holds the contract with each provider listed. If a provider identifies activity as specialised, but that provider does not have a contract for specialised services with an NHS England Specialised Commissioning Hub, then it is expected that the provider will not be paid for that activity. Providers may have agreed local rules which determine that even though a specialised services contract is held with NHS England, certain rules are excluded where the provider is deemed not to provide a specialised service. Reference should be made to the specific local rules in place. The relevant responsible NHS England Regional Geography is derived as follows: Take the value from the CDS field ORGANISATION CODE (CODE OF PROVIDER), AND look this value up in the list of specified UK providers who have agreed contracts with NHS England Specialised Commissioning Hubs, as specified in the Provider to Commissioning Hub Mapping, available from ODS, and then use this to derive the corresponding NHS England Specialised Commissioning Hub code. |
Yes:- Responsible NHS England Specialised Commissioning Hub No:- N/A |
| C-3 |
NHS England will be responsible for facilitating payment of specialised care when referrals are not made through NHS Referral Assessment Service (RAS). |
Where a patient is an English resident cross border patient (i.e. they live in an English border county, but are registered with a Welsh border GP practice) and they are referred via the NHS Referral Assessment Service (RAS), then the Welsh Local Health Board (via the Welsh Health Specialised Services Committee (WHSSC)) will pay for care. Where a patient is not referred via the RAS, NHS England is responsible for paying for the care. It is expected that, in time, all such referrals will be via the RAS. Further details, including the list of GP practices using the RAS are available from NHS England website. |
Yes:- Welsh Local Health Board (via the Welsh Health Specialised Services Committee (WHSSC) No:- Responsible NHS England Specialised Commissioning Hub |
| C-5 |
Some specialised services are considered green and ready for delegation. This question checks whether the service is green and ready for delegation. |
Specialised services are split into red, amber and green services to indicate their suitability for delegation. This question tests whether the service is a green service (suitable for delegation), or not. The different services and their ‘status’ are available from the ‘Delegated NHS England Functions – Supporting Resources’ Future NHS page. Where the service line is listed as a green service, and so ready for delegation, the answer to this question is ‘Yes’ else the answer is ‘No’. |
Yes:- C-6 No:- Responsible sub- ICB location |
| C-6 |
Different ICBs commission different services. This question checks if the ICB commissions the service. |
A list of the delegation status for each of the ICBs is available from the NHS England ‘Directly commissioned services reporting requirements’ webpages. Where the Responsible sub-ICB location Is listed as accepting delegation, for the service line, the answer to this question is ‘Yes’ else the answer is ‘No’. Where the answer is no, the assigned commissioner should be the Responsible NHS England Specialised Commissioning Hub, based on the GP practice of the patient. |
Yes:- Responsible sub- ICB location No:- Responsible NHS England Specialised Commissioning Hub (GP Practice) |
| D |
‘Securing excellence in commissioning NHS dental services’ describes secondary dental activity as activity carried out by General Dental Council (GDC)- recognised dental specialties within general and dental hospital and dental teaching-hospital based services. |
Annex A of ‘Securing excellence in commissioning NHS dental services’ lists which specialties and services constitute secondary dental activity. This has been used to construct a preliminary mapping table to identify secondary dental activity based on certain values of Treatment Function Code and/or Main Specialty Code (see Appendix D). The Securing Excellence document describes a future need to disaggregate the dental component of Oral Maxillofacial Surgery activity which might be facilitated using ICD-10 and OPCS4 codes, however this disaggregation is not currently part of the derivation logic. If the value in the CDS field ACTIVITY TREATMENT FUNCTION CODE is in the following list: 140 (oral surgery), 143 (orthodontics), 142 (paediatric dentistry), 141 (restorative dentistry), 217 (paediatric maxillofacial surgery), 450 (dental medicine specialties), 144 (oral and maxillofacial surgery), 145 (oral and maxillofacial surgery service) and 451 (special care dentistry service) then the answer to this question is ‘Yes’ else the answer is ‘No’. NHS England previously had commissioning and payment responsibilities for secondary dental care, this has now been transferred to sub-Integrated Care Board locations. |
Yes:- Responsible sub- ICB location No:- E |
| E |
The Who Pays? guidance and the ‘Securing Excellence for Commissioning in Offender Health’ state that NHS England is responsible for commissioning admitted and outpatient care provided by secondary care health services for persons who are detained in English Prisons, Secure Training Centres, Secure Children’s Homes, Young Offender Institutions and Immigration Removal Centres. This includes people who have been convicted and people held on remand. This question is designed to identify whether patients fall into this category. |
NHS England Health and Justice commissioning teams commission admitted patient care, outpatient care and public health Section 7a services for these patients, but do not commission accident and emergency care. Note that NHS England is not responsible for paying for secondary care for persons detained in and referred from police custody suites, other places of temporary secure accommodation such as courts, or people held on remand in the community whilst on bail. The use of prison practice codes to identify the eligible health and justice population is not recommended as offenders have the choice to remain registered with their usual community GP taking into account the length of their sentence and may not choose to register for GMS services at the establishment. It is anticipated that from March 2024 female patients residing in the secure and detained estate will be given the choice to register for GMS services. All patients entering the secure and detained estate should have their Patient Demographic Service (PDS) record updated which will reflect the address of the place of detention. Providers should record the place of permanent detention as the place of usual residence for any patient referred for secondary care from a place of secure accommodation. This is in line with Connecting for Health Guidance from 2010. The specific institutions that are in-scope are described in Appendix 1 of Securing Excellence for Commissioning for Offender Health. Just under 95% of these institutions have a unique postcode, with the remaining institutions sharing a postcode with another address site. To identify the addresses of institutions, a lookup table has been provided in appendix F. Is it anticipated that this will be redundant due to changes to the Organisation Data Service records commissioning hubs for Health and Justice. It is anticipated that Prescribing Cost Centres should map between all appropriate prisons, children and young people secure estate settings, and detention centres and the Health and Justice Commissioning Hub, and these data could be used to create a lookup providing postcodes to identify patients where activity should be mapped to a Health and Justice Commissioning Hub. The details of this are still being agreed. Providers should also ensure that the CDS field SOURCE OF ADMISSION CODE (HOSPITAL PROVIDER SPELL) is populated with the value ‘40’ (penal establishment) for any patients who have been admitted from a prison, children and young people secure estate setting, or other detention centre. Any patient whose postcode of place of usual residence is one of either the institutions listed in Appendix F (or found via a matching record in the ‘ejustice’ prison lookup described above), AND whose admission source is a penal establishment will be deemed to be part of the eligible health and justice population. It is acknowledged that for the ~ 5% of institutions that do not have a unique postcode then there is a small risk of incorrect allocation using this methodology. However, since full address data does not flow in the CDS where there is a valid NHS number there is currently no other unequivocal identification method. For Admitted Patient Care CDS records: if the CDS field: POSTCODE OF USUAL ADDRESS is populated with a postcode value contained within the list of organisations detailed in Appendix F or via the new ODS lookups, AND if CDS field SOURCE OF ADMISSION CODE (HOSPITAL PROVIDER SPELL) is populated with the value ‘39’ then the answer to this question is ‘Yes’, else the answer is ‘No’. For Outpatient CDS records, if the CDS field: POSTCODE OF USUAL ADDRESS is populated with a postcode value contained within the list of organisations detailed in Appendix F or via the ODS Prison lookups, then the answer to this question is ‘Yes’, else the answer is ‘No’. NHS England Regional Geographies are responsible for health and justice commissioning (see Appendix A) and a Health and Justice Commissioning Hub code will be available for each region. Take the postcode value from the CDS field: POSTCODE OF USUAL ADDRESS and look this up in Appendix F. |
Yes:- Responsible NHS England Regional Geography for Health and Justice Commissioning No:- F |
| F |
Is the activity part of the agreed list of Public Health section 7a services, detailed in the NHS England service specifications? |
NHS England commissions public health (PH) services as part of the Section 7a agreement. NHS England published service specifications for public health services on the NHS England website. Many of these service specifications do not result in a CDS record, however, those relating to screening can create records – for example, Service Specifications 22 to 26 cover Diabetic Eye Screening, Abdominal Aortic Aneurysm, Breast, Cervical and Bowel screening. Service codes have been created to enable reporting of the public health screening activity. This question should be answered with a ‘Yes’ only if the activity described by the record is covered explicitly by the NHS England service specifications. Some activity along the care Section 7a screening care pathways may also occur via the symptomatic pathways and be excluded from Section 7a CDS, and be the responsibility of the sub-ICB location i.e. colonoscopies can be carried out as part of the Section 7a care pathway or via GP / tertiary service referrals. The answer to this question should be no for services that are in development, such as pilot programmes like the wave three Bowel Scope screening programmes, or HPV primary screening tests. While some public health Section 7a activities occur in maternity services (e.g. Bloodspot screening) these form part of the maternity payment pathway and are not funded by NHS England, but NHS England have commissioning responsibility. |
Yes:- Responsible NHS England Regional Geography for Public Health Services No:- H |
| H |
Check to determine if the activity is another part of Public Health activity. |
The scope of the mandated public health services, not covered by the Section 7a agreement, is described in the DHSC document “Public Health in Local Government – Commissioning Responsibilities” gateway reference number 16747(12). If a provider does flow activity data for these services, via a commissioning dataset, then a local authority organisation should be recorded as the commissioner for all relevant CDS records. There is currently no national identification for public health to assign a Service Category. Therefore, providers are required to agree locally with commissioners and supply contracted business rules to document this agreement. |
Yes:- Responsible Local Authority No:- I |
| I |
Does the CDS activity record describe any form of infertility care or treatment? |
If the CDS field PRIMARY DIAGNOSIS or the CDS field SECONDARY DIAGNOSIS (ICD) includes any of the following ICD10 diagnosis codes: N46 plus all 4th digit suffices, N97 plus all 4th digit suffices, Z31 plus all 4th digit suffices Z35.0; OR if the CDS field PRIMARY PROCEDURE (OPCS) or if the CDS field SECONDARY PROCEDURE (OPCS) includes any of the following OPCS4 intervention codes: N34.1-6, Q13.1-9, Q21.1, Q21.8, Q21.9, Q38.2-3, Q48.1-4, Q48.8, Q48.9, Q56.1-2, Y96.1-6, Y96.8-9. Then the answer to this question is ‘Yes’ else the answer is ‘No’. |
Yes:- Check Armed Forces Eligibility Criteria No:- J |
| I-1 |
Check Armed Forces treatment eligibility. |
The policy for commissioning fertility treatment for Defence Medical Service registered patients and their families provides consistent guidance on the eligibility for infertility treatments. NHS England Armed Forces health leads operate a process to determine whether a patient’s infertility treatment needs to be paid for under the special rules applying to armed forces health (see Appendix E). Where this is found to be the case providers will be contacted by NHS England before the patient attends for care. Providers will then need to manually modify the commissioner code within the relevant CDS submission records from the default responsible sub-ICB location code to the agreed code for NHS England Armed Forces Health Commissioning Hub – ‘13Q’. |
Yes:- NHS England Armed Forces Commissioning Hub No:- Responsible sub- ICB location |
| J |
DMS GP Practice Code Check. |
Who Pays? guidance states that NHS England is responsible for commissioning secondary health services for members of the armed forces who are registered with an English Defence Medical Services (DMS) GP Practice, for the members’ families where they are registered with an English DMS practice, irrespective of their registration status. Patients who fall within this commissioning responsibility are registered with an English GP practice, which have the code ‘13Q’ as their parent commissioning organisation in the national GP practice reference file ‘epraccur’. Where GENERAL MEDICAL PRACTICE CODE (PATIENT REGISTRATION) in the CDS record is populated with an organisation code that has the code ’13Q’ listed as the Commissioner organisation in the national GP practice reference file ‘epraccur’, for active or proposed GP practices (‘epraccur’ status code equal to ‘A’ or ‘P’) on the assignment date AND where the postcode of the practice address (in the national GP practice reference file ‘epraccur’) has the value E92000001 in the ‘Country’ field in the ONS NHS Postcode Directory then the answer to this question is ‘Yes’ else the answer is ‘No’. |
Yes:- NHS England Armed Forces Commissioning Hub No:- C-5 |
Appendix A – NHS England direct commissioning framework responsibilities matrix 2024/25
Please see separate Commissioner assignment method supporting tables spreadsheet 2024/25, for full list.
Updated to include a table to show that sometimes it is valid for the code of 13Q to be used for services other than Armed Forces. This code may also be used in instances where a service is funded on a national basis. The matrix shows the instances of where the use of this code is valid in the production of contract monitoring data sets when recorded alongside specific Commissioned Service Category Codes (see Appendix J).
Appendix B – Specialised and highly-specialised service line codes
This appendix is no longer published as a part of the Commissioner Assignment Method, instead this is available within any one of the four information standards for contract monitoring for all directly commissioned services.
Appendix C – Specialised services cross border flows within the UK
Please see separate Commissioner assignment method supporting tables spreadsheet 2024/25, for full list.
Appendix D – Mapping Table to Identify Secondary Dental Activity
Please see separate Commissioner assignment method supporting tables spreadsheet 2024/25, for full list.
Appendix E – Identification of correct commissioning organisation for infertility care
NHS England is the commissioner of infertility treatment for Defence Medical Service patients and their partners, as described in the NHS England Clinical Commissioning Policy: Assisted Conception to ensure that Armed Forces members receive treatment in line with NICE guidance, regardless of where they live. In addition, a very small number of patients each year (<10) will receive infertility care funded by NHS England under the special rules governing members of the armed forces, their dependents and veterans. NHS England uses the following algorithm to determine whether an infertility patient should be
funded by this route (see diagram below).
Providers will be contacted directly by NHS England before patients receive the treatment and advised whether NHS England will fund the care or whether the patient’s sub-ICB location will be responsible. For this reason, it is not possible to provide a definitive and consistent means of identifying commissioner for this activity.
Where a patient is not ordinarily resident in the UK, assisted conception services must be paid for by the patient (in advance of receiving treatment) unless the patient meets an exemption from NHS charges (it is the duty of the relevant provider, and not the commissioner, to determine whether a patient is an overseas visitor to whom NHS charges for assisted conception apply). This applies most commonly where the patient is in the UK on a visa that is subject to the Immigration Health Surcharge (IHS) as identified by the CDS field OVERSEAS VISITOR CHARGING CATEGORY where the value is B. Where one person in a couple is not ordinarily resident in the UK and their partner is ordinarily resident, the partner who is ordinarily resident is entitled to receive assisted conception services without charge and cannot be denied access.
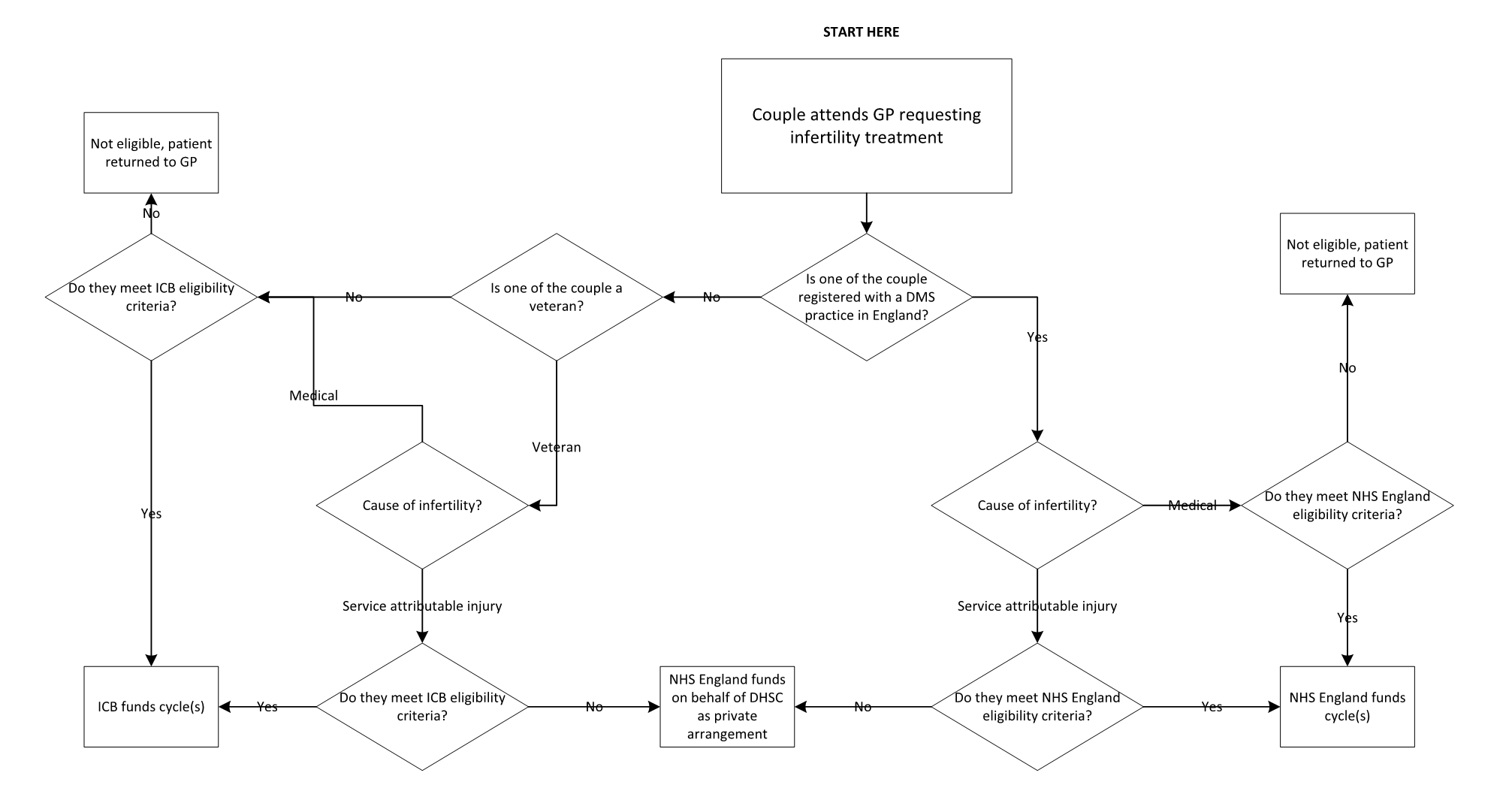
Appendix F – Mapping table of detention centre addresses and regional geography commissioners responsible for paying for treatment for referrals from that detention centre
Please see separate Commissioner assignment method supporting tables spreadsheet 2024/25, for full list.
Appendix G – Glossary
- A&E: Accident and Emergency
- Accident and Emergency attendance: An Accident and Emergency Attendance is an individual visit by one patient to an Accident and Emergency Department to receive treatment from the accident and emergency service
- BFPO: British Forces Post Office
- CCG: Clinical Commissioning Groups (CCGs) were created following the Health and Social Care Act in 2012, and replaced Primary Care Trusts on 1 April 2013. They are clinically-led statutory NHS bodies responsible for the planning and commissioning of health care services for their local area. From 1 July 2022, CCGs will be replaced as commissioner organisations by Integrated Care Boards (see ICBs). CCG boundaries have been (broadly) maintained and referred to as ‘sub ICB locations’
- CDS: Commissioning Data Sets form the basis of data on activity carried out by Organisations reported centrally for monitoring and payment purposes. They support the current Healthcare Resource Group (HRG) version for calculation of payment to trusts and monitoring of other initiatives
- CEOV: charge exempt overseas visitor is when a charge cannot be made or recovered from an overseas visitor
- COV: when a patient is a chargeable overseas visitor
- DHSC (formerly DH): Department of Health and Social Care (DHSC) is a ministerial department, supported by 15 arm’s length bodies and a number of other agencies and public bodies. The department employs 2,160 staff, who work in locations across the country
- DMICP: Defence Medical Information Capability Programme
- DMS: the primary role of the Defence Medical Service (DMS) is to promote, protect and restore the health of service personnel to ensure that they are ready and medically fit to go where they are required in the UK and throughout the world; generally referred to as being ‘fit for task’
- DSCRO: The law says commissioners are not allowed to access Personal Confidential Data (PCD) because they are not providing direct patient care. they need an intermediary service called Data Services for Commissioners Regional Office (DSRCO), that specialise in processing, analysing and packaging patient information within a secure environment into a format various commissioner can legally use; anonymised patient level data
- EEA Resident: A resident of the European Economic Area, a free-trade zone created in 1994, composed of the states of the European Union together with Iceland, Norway, and Liechtenstein
- ECDS: Emergency Care Data Set (a replacement for the A&E dataset)
- EHIC: European Health Insurance Card
- GDC: General Dental Council
- GP: General Practitioner
- HRG: Healthcare Resource Group
- ICD-10: International Classification of Diseases (10th edition)
- ICB: Each integrated care system (ICS) will have an integrated care board (ICB), a statutory organisation bringing the NHS together locally to improve population health and establish shared strategic priorities within the NHS. ICBs have replaced clinical commissioning groups (CCGs)
- ICS: Integrated Care Systems (ICSs) are partnerships of organisations that come together to plan and deliver joined up health and care services, and to improve the lives of people who live and work in their area
- IR: Identification Rules for Prescribed Specialised Services
- IRC: Immigration Removal Centre
- LHB: Established and hosted by local authorities, health and wellbeing boards bring together the NHS, public health, adult social care and children’s services, including elected representatives and Local Healthwatch, to plan how best to meet the needs of their local population and tackle local inequalities in health
- Local Health Board (Wales): A Local Health Board (Wales) (formerly known as Welsh Local Health Board) is an Organisation. Local Health Boards (Wales) are bodies corporate established by the Welsh Ministers under s.11 of the National Health Service (Wales) Act 2006
- MHL&D: Mental Health Liaison and Diversion
- NECS: The North East Commissioning Support Unit works across the UK to support health and social care customers in meeting strategic and operational challenges, to improve outcomes and increase efficiency
- NHAIS: National Health Applications & Infrastructure Services
- NHS Digital: NHS Digital, and their responsibilities, have merged with NHS England. NHS Digital were able to disseminate data to commissioners under the Health and Social Care Act (2012). The act provided the powers for NHS Digital to collect, analyse and disseminate national data and statistical information. To access this data organisations must submit an application and demonstrate that they meet the appropriate governance and security requirements
- NHS England: NHS England leads the National Health Service (NHS) in England
- NIHSCB: The National Health Service Commissioning Board is a statutory organisation. They arrange or ‘commission’ health and social care services for the population of Northern Ireland
- ODS: The Organisation Data Service (ODS) is responsible for publishing organisation and practitioner codes, along with related national policies and standards
- ONS: The UK’s largest independent producer of official statistics and its recognised national statistical institute. The ONS responsible for collecting and publishing statistics related to the economy, population and society at national, regional and local levels. They also conduct the census in England and Wales every 10 years
- OPCS4: Office of Population Census and Surveys, Classification of Interventions and Procedures (version four)
- Outpatient attendance: An attendance to enable a patient to see a consultant (or a GP acting as a consultant employed by the trust as a hospital practitioner) or clinical assistant, in respect of one referral
- PAS: Patient Administration System
- PbR: Payment by Results (PbR) was a system of paying NHS healthcare providers a standard national price or tariff for each patient seen or treated. This was replaced by the National Tariff Payment System, and latterly with the NHS Payment Scheme
- PDS: Personal Demographic Service
- RAS: The NHS e-Referral Service (e-RS) programme has introduced Referral Assessment Services (RAS), which now allow providers to:
- assess the Clinical Referral Information from the GP/referrer
- decide on the most appropriate onward clinical pathway
- contact the patient to discuss choice (if an elective referral)
- arrange an appointment, where needed
- return the triage request to the original referrer with advice, if an onward referral isn’t needed
- SARC: Sexual Assault Referral Centre
- SHB: Scottish Health Board is a regional authority in Scotland with responsibility for the delivery of health services
- Specialised commissioning team: There are over 130 specialised services that are commissioned by 10 specialised commissioning teams that are part of NHS England. The specialised commissioning teams (or hubs) are grouped by the NHS England regions – North, Midlands and East, London and South. The South region is split into South West, South East and Wessex
- SUS+: Secondary Uses Service
- WHSSC: The Welsh Health Specialised Services Committee (WHSSC) is responsible for the joint planning of Specialised and Tertiary Services on behalf of Local Health Boards in Wales
- YOI: Youth Offender Institution
Appendix H – Pseudo postcodes for EU member states and other states with similar arrangements (starred)
The following pseudo postcodes are for EU member states and other states with similar arrangements.
- Austria: ZZ99 4MZ
- Belgium: ZZ99 2DZ
- Bulgaria: ZZ99 4UZ
- Croatia: ZZ99 5VZ
- Cyprus (Southern): ZZ99 6AZ
- Czech Republic: ZZ99 5XZ
- Denmark: ZZ99 4FZ
- Estonia: ZZ99 7LZ
- Finland: ZZ99 4BZ
- France: ZZ99 4GZ
- Germany: ZZ99 4QZ
- Greece: ZZ99 4RZ
- Hungary: ZZ99 4XZ
- Italy: ZZ99 4LZ
- Latvia: ZZ99 7RZ
- Lithuania: ZZ99 7SZ
- Luxembourg: ZZ99 2EZ
- Malta: ZZ99 5BZ
- Netherlands: ZZ99 4EZ
- Norway*: ZZ99 2AZ
- Poland: ZZ99 4YZ
- Portugal: ZZ99 4JZ
- Republic of Ireland: ZZ99 3AZ
- Romania: ZZ99 4ZZ
- Slovakia: ZZ99 5YZ
- Slovenia: ZZ99 5UZ
- Spain: ZZ99 4HZ
- Sweden: ZZ99 2CZ
- Switzerland*: ZZ99 4PZ
Notes on EU arrangements
- France includes the departments of Guadeloupe, Martinique, Guyane (French Guiana) and Réunion.
- Spain includes the Balearic Islands, the Canary Islands, Ceuta and Melilla
- Portugal includes the Azores and Madeira.
- The territory of Denmark excludes the Faroe Islands and Greenland, although Faroese residents are covered by a separate healthcare arrangement
- Andorra, Monaco, San Marino and Vatican City are not part of the EU or EEA.
Non-EEA reciprocal arrangement countries as listed in DHSC/NHS guidance and pseudo postcodes from ONS.
- Anguilla: ZZ99 6RZ
- Ascension: ZZ99 6UZ
- Australia: ZZ99 6GZ
- Bermuda: ZZ99 6RZ
- Bosnia and Herzegovina: ZZ99 5NZ
- British Virgin Islands: ZZ99 6RZ
- Cayman Islands: ZZ99 6RZ
- Falkland Islands: ZZ99 6UZ
- Faroe Islands: ZZ99 4WZ
- Gibraltar: ZZ99 5AZ
- Guernsey: ZZ99 3EZ
- Isle of Man: ZZ99 3BZ
- Israel: ZZ99 9AZ
- Jersey: ZZ99 3FZ
- Kosovo: ZZ99 9SZ
- Montenegro: ZZ99 9SZ
- Montserrat: ZZ99 6RZ
- New Zealand: ZZ99 6HZ
- North Macedonia: ZZ99 5QZ
- Pitcairn Islands (including Henderson, Ducie and Oeno Islands: ZZ99 6JZ
- Serbia: ZZ99 9SZ
- St Helena: ZZ99 6UZ
- Tristan da Cunha: ZZ99 6UZ
- Turks and Caicos Islands: ZZ99 6RZ
Further codes are available in the Country names and pseudo country postcodes file, available from the ODS ONS file section.
Appendix I – Commissioner Assignment Method Flow Chart
Commissioner assignment method 2024/25.
Appendix J – Commissioned Service Category Codes
Please see separate Commissioner assignment method supporting tables spreadsheet 2024/25, for the list of commissioned service category codes.