
1. Development and Implementation
1.1 What happens if I decide to opt out?
Elements of the fit and proper person test (FPPT) assessment that relate to Care Quality Commission (CQC) Regulation 5 Fit and proper persons: board directors are required and will continue with no change.
If a board member seeks to opt out of all or part of the assessment (other than elements relating to CQC Regulation 5 Fit and Proper Persons: board directors, which are a requirement), the first step should be for the board member to have a discussion with the chair about their reasons.
The chair would consider this on a case-by-case basis and come to a judgement about the impact of this on the fit and proper person status for the individual concerned.
The underlying legal requirements in Regulation 5 of the 2014 Regulations cannot be opted out of.
1.2 Will we need to collect ‘old’ evidence for new elements of FPPT?
No, the new Framework is not being applied retrospectively. The new elements (in addition to those that are already in place under CQC Regulation 5) will begin in 2023/2024 and should be fully implemented in organisations by 31 March 2024.
1.3 How will you make sure that people and organisations comply?
The FPPT Framework is not statutory (other than CQC Regulation 5 Fit and Proper Persons: Board directors). Organisations and individual board members should be able to see the benefits of an effective FPPT assessment process and framework and the advantages of participating fully.
Once the Framework is live, NHS England will consider whether further levers are required, such as inclusion in the NHS Code of Governance and/or in the Provider Licence. Take-up and implementation of the Framework will be considered in the independent review which will be carried out September 2025 – November 2025.
1.4 What will happen if the FPPT means that people only apply to board roles at well-performing trusts and avoid challenged organisations as it could impact their FPPT status?
The FPPT assessment is undertaken on an individual basis, rather than in relation to the performance of a board or organisation as a whole. Aspirant board members who can demonstrate the characteristics described in the Framework should not be deterred from seeking to join the board of a more challenged NHS organisation.
1.5 Is the framework applicable to subsidiary companies of NHS foundation trusts? We would do the normal recruitment checks for individuals in a similar vein, but are the annual attestations and submissions to the regional team required for SubCo directors?
At this time, NHS England is suggesting that the FPPT Framework is only applicable to subsidiary companies where they are regulated by CQC. However, organisations may choose to extend the scope to include subsidiary boards, but this information would not be required to be included in the annual submission to the regional director.
1.6 What might be the definition of ‘something new comes to light’ in the guidance for chairs, to ensure a revised assessment is carried out?
The underlying legal requirements in Regulation 5 are such that organisations should be continuously keeping under review whether or not an individual director remains a fit and proper person.
An example may be where a board member’s current organisation receives an updated board member reference from their previous employer/appointing organisation with new information relevant to the FPPT assessment, for example, the conclusion of an investigation after the person left, or if an individual is convicted of an offence in-year.
2. Regulation
2.1 Why does the NHS regional director need to know about the FPPT status of board members in trusts and foundation trusts?
NHS England regional directors will ensure that individual NHS organisations are embedding the Framework by receiving the annual submission summarising the fit and proper person assessment outcomes for their boards.
2.2 What will the CQC want to see – will it be different; will we have to keep 2 sets of FPP information?
The CQC regulatory role in relation to Regulation 5: Fit and proper persons: directors will not change. NHS England has worked with CQC in developing the Framework and the new arrangements should provide for a more standardised approach from one organisation to another. There will be no need to keep two sets of fit and proper information for CQC and NHS England.
2.3 What happens when recruitment agencies are involved?
NHS organisations should be able to demonstrate that appointments of new board members are made through a robust and thorough appointment process. It will be important to ensure that responsibilities for the FPPT are clear between the recruitment agency and the NHS organisation.
No new appointments should be made to the post of board member unless the appointee concerned can demonstrate they have met the FPPT requirements as detailed in section 3.7 of the FPPT Framework, irrespective of how they were appointed. The standard board member reference should be completed, even where an agency is involved.
3. Annual submission and appraisals
3.1 How much information on training and development, education and qualifications is it reasonable to request? Can individual board members add what training they have done, as they may have done webinars, etc that we would not know about centrally?
NHS organisations need to have appropriate processes for assessing and checking that the candidate/board member holds the required qualifications and has the competence, skills and experience required.
Where NHS organisations consider that a board member role requires specific qualifications (for example, the chief financial officer being an accredited accountant, or the chief medical officer being a GMC-registered doctor), they should make this clear and should only appoint those candidates who meet the required specification, including any requirements to be registered with a professional body.
In assessing whether a board member has the competence, skills and experience to be considered fit and proper, the FPPT assessment will:
- not just consider current abilities, but also have regard to the formal training and development the board member has undergone or is undergoing
- take account of the NHS organisation (its size and how it operates), the role and the activities the board member should perform
Board members should update their own ESR record with relevant training that they have completed via ESR self-service.
3.2 Is the FPPT assessment just part of recruitment and then a once-a-year assessment, what happens if something crops up at other times?
The FPPT assessment is an ongoing assessment. There are assessments both on recruitment and on an annual basis. However, should anything come to light at any time that is relevant to the FPPT, the latest assessment should be revisited and updated appropriately.
3.3 Why is the six-year history for training included?
A six-year training history is included to provide evidence that board members have relevant skills and qualifications for their roles as described in the person specification for the role and that the training record is up to date as appropriate.
3.4 When is the annual submission required?
The first annual submission to regional directors should be sent by June 2024.
All organisations should have adopted the FPPT Framework by 31 March 2024.
The FPPT Framework asks organisations, from the end of quarter 1 in 2024/2025, to incorporate the Leadership Competency Framework (LCF) into annual appraisals of all board directors. Where the FPPT Framework refers to appraisal, it means the annual performance appraisal.
In future years, the appraisal/LCF and FPPT assessment should all align..
3.5 Why are 360-degree assessments not included?
We received feedback from stakeholders that it would not be appropriate to include 360-degree assessments as there is no consistency of approach from one organisation to the next, and that they are open to greater subjectivity. NHS England agreed with these comments.
4. Board member reference (BMR) and data quality
4.1 Why are you proposing to retain leaver BMRs career-long?
By completing a BMR whenever a board member leaves whether or not there has been a request from another organisation and retaining the BMR career-long, there will be a reference available for individuals who may have left the NHS for a time and then return, rather than moving straight from an NHS board role to another NHS role.
All NHS organisations in scope should establish, implement and maintain adequate policies and procedures to comply with data protection law and the NHS Records Management Code of Practice.
The NHS Records Management Code of Practice sets out expectations in relation to retaining actual staff documents/records for a period of six years. However, NHS organisational case documents/records may be retained for longer than the standard six years, based on the facts of the case. This will be a local decision for each NHS organisation.
4.2 Why are you including a question on discontinued or ongoing complaints and investigations in the board member reference – the response will not be based on fact until the case is concluded and could be unfair?
Discontinued investigations are included in the board member reference request to identify potential issues around serious misconduct and mismanagement. The fact that there has been a discontinued investigation does not automatically render a director unfit. However, it is a piece of evidence which may need to be taken into account in assessing whether a director is fit.
The reason for discontinuing (including not starting) an investigation should be recorded, including whether an investigation was not started or stopped because a compromise, confidentiality or settlement agreement was then put in place, again recognising that such an agreement is not necessarily a conclusion that someone is not fit and proper for the purposes of the FPPT.
4.3 How will data quality be assured and when does the ESR FFPT database need to be updated?
The ESR FPPT data fields need to be maintained to ensure information about serving board members is current. This includes for existing board members and new appointees. It also includes whenever there has been a relevant change to one of the fields of the FPPT information held in ESR. In addition, chairs should confirm annual completion of FPPT.
It is the responsibility of each NHS organisation to ensure that ESR remains current and is updated for relevant changes in a timely manner. As a minimum it is expected that each NHS organisation conducts an annual review to verify that ESR is appropriately maintained.
5. Disclosure and barring service (DBS)
5.1 What level DBS check should organisations apply to board members?
A DBS check in line with their local policy requirement. Each NHS organisation should outline within their local policy the relevant DBS check (basic, standard, enhanced or enhanced with barred lists) required for each individual board member role. In defining the required DBS level, NHS organisations should identify those board roles that fall within the definition of a ‘regulated activity’, as defined by the Safeguarding Vulnerable Groups Act 2006, as required barred list checks.
DBS guidelines are set out on the UK Government Disclosure and Barring Service website. Please also refer to the Care Quality Commission’s frequently asked questions on fit and proper person requirement and DBS. This provides guidance on which the criteria of the DBS levels would be required for the roles.
5.2 Regarding DBS checks – if the DBS is updated by 31 March 2023 and then the individual signs up to the DBS Update Service, is this sufficient for maintaining an up-to-date DBS at all times? Would the DBS still need to be ‘renewed’ every 3 years?
DBS checks should align with the organisation’s local policy (see Section 3.7.1 of the guidance). A 3-year review is recommended as good practice but is not a mandatory requirement unless specified by local policy. Where the individual has signed up to the DBS Update Service, this would be sufficient depending on organisational policy.
Organisations may want to explore the DBS update service at secure.crbonline.gov.uk/crsc/check?execution=e1s1 (see question 8.1 below).
6. FPPT good character assessment checks
6.1 Does financial soundness verification include credit checks or is only limited to information available on public domain?
The requirement to check certain financial soundness information is also a requirement of CQC Reg 5 and Schedule 4. Organisations and chairs should consider whether the checks that they have been carrying out previously for FPPT provide sufficient assurance. There are various websites available for these checks at a small cost, for example, www.trustonline.org.uk. It should not be necessary to undertake a credit check.
6.2 How can an organisation find out whether a person has been subject to any adverse finding or settlement in civil proceedings and employment tribunals? Is there a register?
There are various websites available for these checks at a small cost, for example, www.trustonline.org.uk.
Employment tribunal judgments are published online at https://www.gov.uk/employment-tribunal-decisions. Organisations may consider checking by previous organisations that the applicant has worked for to indicate any cases where that organisation was respondent and if so, the issue could be raised in discussion between the chair and the individual as to whether they were involved or not.
Other issues may be identified through the board member self-attestations and/or a direct discussion.
6.3 If information on how NHS England approaches social media checks could be shared, that would be extremely helpful
Due to the changing nature of social media, the NHS England approach to these checks is based on the individual applicant and to test for areas which would highlight any risks to an appointment in relation to FPPT.
7. Equality and diversity
7.1 How will equality, diversity and inclusion (EDI) data be collected?
EDI information is collated separately to the FPPT Framework through the NHS Workforce Race Equality Standard; and similarly for the NHS Workforce Disability Equality Standard.
As NHS England will not ask organisations to disclose protected characteristics of board members, Chairs should hold themselves accountable for reviewing this in line with their organisation’s broader responsibilities under equalities law.
8. Electronic staff record (ESR)
8.1 How can I see an FPPT dashboard report from ESR, and where is it located?
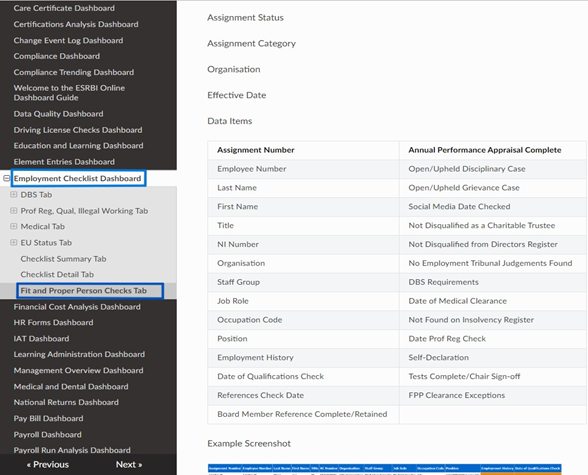
The NHS ESR Business Intelligence function includes an FPPT option within the NHS Employment Checklist Dashboard. Further information is provided in the accompanying FPPT ESR user guidance document located.
Screenshot below: The location of the FPPT Checks Tab can be located within the Employment Checklist Dashboard.
8.2 Why do we need to keep records as well as use ESR?
ESR only holds limited information. It should be used to record that the assessment has taken place and to download the FPPT dashboard. Detailed documentation which includes highly sensitive and confidential information, needs to be held locally as evidence of the assessment having taken place and any comments or mitigations required in reaching a conclusion.
8.3 I left the NHS six years ago and now I am applying to be a non-executive director (NED) – will someone be looking up my old ESR record?
No, the FPPT Framework will not be retrospective at the point of launch, that is, organisations will not be required to go back and build up records. It will be forward-looking from 1 October 2023, with a requirement for the first annual self-attestation to be undertaken by no later than 31 March 2024.
8.4 ICB boards have partner members; can you clarify where responsibility for the FPPT sits?
For an ICB, the chair should consider what level of assurance they need to conclude that members of their boards are fit and proper. The FPPT Framework provides guidance, and in summary:
- Where an individual is a partner member from a non-NHS organisation, the chair should seek a copy of the equivalent FPPT from their organisation where this is in place and consider whether it is sufficient.
- Where an individual is a partner member from an NHS organisation the chair should consider whether the FPPT assessment in their employing organisation is sufficient.
- where the FPPT assessment from the employing organisation is not sufficient – for example, where the role on the ICB board is different to the role on the individuals board, then the ICB chair should carry out an FPPT assessment for partner members.
- This would not necessarily need to be the full assessment if some elements were satisfactorily covered in the employing organisation’s assessment; the chair should use their discretion.
- The ESR ‘volunteer’ category can be used for those partner members who are not NHS employees or appointed board members.
Publication reference: PRN00870