
Context
This specification supports the planning and delivery of new-build neighbourhood health centres. It is not a detailed technical rulebook, but a tool for consistent planning and design by providing a common starting point for local systems to develop designs that reflect community needs while remaining aligned with national policy.
It sets out shared principles to guide design, rather than prescribing a single model. While developed for purpose‑built facilities, the principles can also be applied, where appropriate, to refurbishments, extensions and repurposed buildings, including health‑on-the-high street models.
While the aim of this specification is primarily to support new-build neighbourhood health centres, it is explicitly intended to enable and encourage refurbishment, repurposing and extension of existing estate as a primary route to delivery. In many locations, adapting existing buildings will offer the fastest, most affordable and most appropriate way to establish neighbourhood health centres, applying the same core principles proportionately.
Neighbourhood health centres should be co-designed with local communities, including people with lived experience and specific health needs such as a learning disability, to ensure services and spaces genuinely reflect local priorities and needs.
Status and intended use
The document is for integrated care boards (ICBs), local authorities, providers, design teams and delivery partners when developing proposals and briefs. It should be read alongside the accompanying neighbourhood health centre guidance for regions and integrated care boards and relevant NHS technical guidance; health building notes (HBNs) and health technical memoranda (/HTMs). It should also be read alongside relevant planning policy and guidance, including the National Planning Policy Framework.
How to interpret language
The specification does not introduce new burdens or compliance mechanisms. ‘Must’ is stipulated only where there is an existing legal or regulatory requirement. Beyond this, it sets common principles and aspirations that local systems should follow, adapting to local contexts as necessary.
These principles are intended to be applied proportionately and pragmatically, recognising that high-quality neighbourhood health centres can be delivered through refurbishment, repurposing or extension of existing estate, as well as through new-build schemes.
Definition and primary objective
Delivering on neighbourhood health, as set out as part of the broad transformative vision in the 10 year Health Plan, will involve bringing together a wide range of health and healthcare services. Where feasible, neighbourhoods will also align with a wider range of public services through proactive cross-government working and co-design, consistent with the government’s place-based approach to public service reform.
The ambition within the 10 year Health plan for neighbourhood health centres is that they may:
- be based in every community (defined as a population of around 50,000), focused on places where healthy life expectancy is lowest
- be a ‘one stop shop’ for patient care, and recognised as the place to go for the majority of health needs
- be based around general practices, co-locating community care and bringing traditionally hospital-based services such as diagnostics, post operative care and rehabilitation into the community
- be a place from which multidisciplinary teams operate
- ideally, co-locate a wider range of local government and voluntary sector services to help create an offer that meets population need holistically: for example, through offering services like social welfare advice (covering issues such as debt and housing), employment support and smoking cessation or weight management services
- help ensure, through co-location, convenient access to services, particularly for those with complex needs, and support more integrated working by professionals
- shift outpatient care from hospitals into the community
Neighbourhood health centres are intended to form part of an asset-based neighbourhood approach, building on existing community strengths, services and infrastructure. They are designed to support prevention, integration and place-based working by connecting health services with wider networks of support, community activity and health promotion, rather than operating as standalone clinical facilities, contributing to a wider ecology of care that supports people throughout their lives.
The neighbourhood health centre
Neighbourhood health centres are integrated primary and community care facilities, designed to support prevention and bring more care closer to home, reducing pressure on acute services.
A core neighbourhood health centre is typically built around co‑located general practices and may bring together several practices serving the same locality. It provides space for primary care, community services and some secondary care clinics, supporting more joined‑up working while remaining convenient and accessible for local people.
Core+ centres include additional space for services such as family support and healthy child development, primary care‑led mental health provision and minor injuries or walk‑in services. Core++ centres also include diagnostic space and 24‑hour phlebotomy provision, supporting local need and, where appropriate, acute services. All models are designed to accommodate mobile diagnostic units.
Neighbourhood health centres are designed around adaptable, shared spaces rather than fixed, service‑specific rooms. This allows a wide range of services, such as physiotherapy, occupational therapy, community nursing, diagnostics, social care and voluntary sector support, to operate from the building in response to local need. These services are delivered in standard consultation and treatment rooms, therapy and group spaces, team bases and flexible community rooms, enabling efficient use of space and supporting multidisciplinary working over time.
Mental health provision within neighbourhood health centres focuses on primary care‑led and early intervention support, integrated with general practice services. This is distinct from community based mental health centres, which bring together community and crisis mental health teams with local authority and voluntary sector partners to support people with more complex or acute needs. Community based neighbourhood mental health centres complement, rather than replace, neighbourhood health centres and the person’s named GP, ensure continuity of care and co-ordinated support across neighbourhood teams.
Where possible, neighbourhood health centres should be connected to existing community pharmacy provision, particularly in high street or town centre locations. Co‑location with nearby pharmacies is preferred, supporting accessibility, local regeneration and efficient use of space. Fully embedded pharmacies are not expected as standard due to their space and operational requirements but may be considered where there is a clear local need and service rationale.
Best Start Family Hubs and Network Sites form part of the wider neighbourhood offer. Local authorities, ICBs and partners should ensure that they complement, rather than duplicate, neighbourhood health centres, while retaining their own identity and national branding. Neighbourhood Health Centres should work collaboratively with Best Start Family Hubs as part of a joint network so that families can easily find and navigate the help they need. Best Start Family Hubs and Healthy Babies Guidance for Local Authorities emphasises the importance of Best Start Family Hubs delivering services through ‘network sites’ (other trusted community locations such as Neighbourhood Health Centres) wherever possible – to ensure services reach families where they are and deliver the greatest impact.
Neighbourhood health centres are designed to provide a physical setting and a digital hub for:
- integrating primary and community health and social care
- localising ambulatory and diagnostic services
- partnering with the third sector and local authority services where appropriate.
The centres will:
- embody the shift from reactive to proactive care, moving services, wherever appropriate, from settings in hospitals or isolated general practice premises to integrated local centres
- be simple, adaptable and non-specific ‘long life, loose fit’ buildings that can flex and change throughout their life
- meet the Net Zero Building Standard and provide exemplars for low carbon construction and operation, with an aspiration to achieve Passivhaus standards where appropriate
- be healthy buildings, providing well-tempered and well-designed environments with alignment to strategies such as BREEAM or the WELL Building standard, or similar
- contain standard rooms and standard systems of assembly
- be designed, manufactured and assembled in accordance with the principles of modern methods of construction (MMC)
- achieve improved rates of utilisation of space
Archetypes and space utilisation
Archetypes
Recognising that different geographies will be starting from different points, we have identified 4 potential archetypes (configurations) through which the neighbourhood health model can broadly be delivered:
- hub-and-spoke model
- repurposed community or civic spaces
- cohort-specific hubs
- purpose-built neighbourhood health centres
These archetypes are not intended to be restrictive. Local partners may develop variations or hybrid models where these meet service needs and align with the principles set out in this specification.
The archetypes described below relate to components of the wider neighbourhood health model and network within a place. Together, they create a flexible network that brings care closer to where people live while maintaining a coherent neighbourhood offer.
They distinguish between locations that function as neighbourhood health centres and other hubs or settings that support specific population groups as part of the wider neighbourhood health system. Not all the archetypes represent places that can be designated as neighbourhood health centres in their own right. 2 of the archetypes – the hub-and-spoke model and new neighbourhood health centres – function as the primary neighbourhood health centre setting, providing a central base for integrated care. The other 2 – repurposed community or civic spaces and cohort-specific hubs – operate as supporting neighbourhood health services, extending reach into high street, community and specialist settings.
Neighbourhood health centres operate as anchors within a wider neighbourhood health network, supported by digitally connected cohort‑specific and community‑based hubs. All archetypes are therefore expected to operate as digitally-enabled and connected components of a wider neighbourhood network, with digital infrastructure acting as a key enabler to integrate services, co-ordinate activity and connect centres across a place, in line with the digital requirements set out later in this specification.
This specification, including the supporting schedules of accommodation and layout plans , applies primarily to the new-build archetype. However, the underlying principles, including flexibility, high utilisation, inclusive design, net zero alignment and digital connectivity, should be applied, where feasible, to refurbishment, extension and repurposing schemes, as well as health-on-the-high street models.
Archetype 1: Hub-and-spoke/upgrade, repurpose or extend existing NHS estate
Upgrading or reconfiguring existing general practice, community or other NHS buildings is typically the quickest and most affordable way to establish a neighbourhood health centre. It is appropriate where existing high-quality estate can be extended or complemented by ‘spokes’ such as mobile or small satellite sites to provide the right neighbourhood health service offer.
Archetype 2: Repurposed community or civic spaces
Adapting high street premises, libraries, leisure centres or other civic assets to host neighbourhood health services brings care closer to where people live and can be delivered at pace and comparatively low cost. While these facilities will often not be able to provide the full range of services expected from a neighbourhood health centre, they can form a valuable part of the local offer.
Archetype 3: Cohort-specific hubs
Existing hubs that provide health or care services in the local community for particular groups, such as women’s health hubs, Best Start Family Hubs, community based mental health centres or respiratory hubs, and can be integrated into the wider neighbourhood health offer. These hubs will not always be physically located within a neighbourhood health centre, but should complement, align with and, where it makes sense locally, be co-located or rationalised with neighbourhood health centres.
Archetype 4: Purpose-built neighbourhood health centres
New-build centres that are designed specifically for multidisciplinary teams, co-located services and strong digital integration. These will be delivered through a mix of public capital and a new public private partnership model in areas where current estate cannot readily be repurposed to deliver convenient access for patients to the full range of neighbourhood health services.
Utilisation of space
Key utilisation assumptions for neighbourhood health centres are:
- 30,000 general practice population (core)
- 50,000 community care population (core+)
- 100,000 ‘other’ for example diagnostic (core++)
- rooms are shared between services on a timetabled basis delivering an integrated service model
- all services operating at 80% utilisation of spaces
- open 6 days a week.
- open 12 hours
- spaces out of hours available for community activities
These assumptions are intended to support flexibility and shared use of space. They should be applied alongside realistic modelling of workforce growth, service expansion and evolving primary care roles over time.
A high level of space utilisation is expected to be achieved primarily with longer operating hours, shared use of rooms across multiple services and improved co-ordination of activity across the day, rather than intensifying individual clinical sessions.
Neighbourhood health centres are designed to support extended opening hours and multiple, co-ordinated sessions within the same room across a broader range of providers. This represents a shift from traditional models where rooms are occupied for limited, fixed sessions within a longer opening day, towards a more flexible, system‑wide approach to scheduling and use of space.
The activity modelling tool we used to derive the accompanying schedules of accommodation and layouts is provided alongside this specification for local providers to use.
In their operation neighbourhood health centres are expected to be highly flexible and adaptable facilities that can alter their space allocations to match changing provider demand, not ones that preserve exclusivity and ‘ownership’ of space over long periods of time. This ambition is supported by the proposed centre funding, ownership and occupation models.
Where spaces are made available outside core operating hours, this is expected to support targeted health, wellbeing and social prescribing activity that aligns with neighbourhood priorities, not general commercial hire, and will be subject to local operational, security and cost considerations.
Integrated and unintegrated operating models
In considering space utilisation, this specification distinguishes between unintegrated and integrated operating models, reflecting different approaches to the use and management of space.
In an unintegrated model, services typically operate independently, with rooms and spaces allocated to individual organisations, teams or clinicians. Space is sized and planned to meet the peak needs of each service, and rooms are often occupied for fixed sessions within a wider opening day. While this model provides a high degree of ownership and familiarity, it can result in lower overall utilisation and reduced flexibility as service needs change.
In an integrated model, space is shared across services and sized to support a broader range of activity over the course of the day. Rooms are booked and used flexibly by different providers and teams, supported by co-ordinated scheduling, extended operating hours and shared operating models. This approach enables higher levels of utilisation, reduces duplication of space and supports multidisciplinary working and more seamless care for patients.
Neighbourhood health centres are designed to support the integrated model, with adaptable rooms, shared booking systems and operational arrangements that allow space to respond dynamically to changing demand and service mix, rather than being tied to single users or fixed patterns of use.
Location
Neighbourhood health centres should be located at the heart of the communities they serve. Sites should be places people already visit regularly, with good public transport and local infrastructure, to avoid creating high‑quality but under‑used buildings.
When identifying sites, systems should consider location, accessibility, footfall, social value and regeneration together. Existing community focal points, such as high streets and town centres, are often well recognised, accessible and well served by amenities. While such locations may mean higher land or rental costs, their visibility and accessibility can improve use, support regeneration and deliver better long‑term value.
Neighbourhood health centres should act as community anchors, supporting wider social value and the broader determinants of health. Sites should therefore be selected in collaboration with local authorities to align with local planning priorities, regeneration strategies and wider public service provision. With local input, each centre should reflect local need, identity and pride in place.
Locating a centre away from an established community focal point should be approached cautiously and only where there is clear evidence of future population growth, such as committed large‑scale housing development. Information about such developments is available from local authorities and on the STRATA platform (previously branded SHAPE).
Site selection and design should align with NHS England’s Building for health principles, supporting accessibility, wellbeing and integration with the surrounding place.
Key principles for location are:
- social value
- regeneration
- accessibility
- footfall
- community
Inclusive by design
Neighbourhood health centres should function as accessible, practical community facilities, supporting access to services, advice and prevention activity.
The design approach should prioritise usability, dignity and safety, informed by established guidance rather than bespoke or experimental solutions, for people to use these centres with confidence.
The design should provide clear layouts, allow ease of movement and create environments that reduce confusion and unnecessary stress. Natural light and views to the outside should be maximised where possible. Waiting and shared areas should be calm, clearly organised and appropriately scaled.
Dementia-friendly design is a core requirement and should be embedded from the outset. This includes clear and intuitive wayfinding, consistent colour cues, simple circulation routes and the avoidance of glare, visual clutter and confusing patterns.
Designs should take account of a wide range of physical, sensory and cognitive needs. This includes step‑free access, suitable seating, clear entrances and environments that support people with sensory sensitivity, including those living with dementia, autism, a learning disability or mental health condition. Public areas should feel familiar and non‑institutional, supporting use by a wide range of people and services.
Design teams are encouraged to draw on emerging good practice, including the sensory‑informed design principles set out in HBN 00‑03: Clinical and clinical support spaces and relevant professional guidance on design development, such as the inclusive design overlay to the RIBA plan of work, adapting these principles proportionately to local context and service need.
Where appropriate, provision may be made for quiet or multi‑faith spaces. Engagement with local communities should inform design choices, proportionate to the scale and context of the scheme.
Key principles for inclusive design are:
- dementia-friendly design
- accessibility
- sensory comfort
- wayfinding
- natural light and biophilia
- community wellbeing
Brief
Defining service requirements
Neighbourhood health estate will enable long-term flexibility in clinical service delivery. Clinical briefing and patient flow improvements are key priorities for the NHS and should be embodied in the development of all schemes.
All systems considering a neighbourhood health centre will establish a clinical brief. This brief will:
- be based on the identified services that are present in a core neighbourhood health centre through to the larger core++ version
- appropriately define and model currently acknowledged population health needs and outcomes, and identify the preferred service mix to improve outcomes and reduce inequalities. From this process, space requirements and improved patient flow can be understood and developed
- clearly state expected benefits and key performance indicators for added value, including socio-economic, health outcomes and local regeneration
Rather than adopting traditional approaches to healthcare planning in primary care, neighbourhood health centres will be modelled on bookable rooms and flexible floor space to achieve occupancy rates of 80% during opening hours (at least 72 hours a week).
Integration of social care within neighbourhood health centres
Neighbourhood health centres are designed to enable the integration of social care services through flexible, shared and non‑clinical spaces rather than fixed, single‑purpose accommodation. Social care functions may be delivered through a combination of interview rooms, group rooms, shared workspaces and community support rooms, co‑located alongside health and voluntary sector services.
This approach supports joint working, warm handovers and multidisciplinary collaboration, while allowing the scale and form of social care presence to respond to local commissioning arrangements, workforce models and population need. Social care integration is therefore enabled by adaptable space, shared operating models and digital connectivity, rather than by prescribing specific room types or layouts.
We have based the development of the activity modelling tool (in Excel), provided alongside this specification, on agreed population definitions and utilisation for healthcare only services at this stage. It can be adapted to input social care parameters at briefing stages to reflect local requirements.
Training and education opportunities
System‑owned and system‑controlled assets provide opportunities to accommodate medical, nursing and other training programmes. These requirements should be considered when developing the clinical brief and schedule of accommodation. Neighbourhood health centres should support shared training environments for the wider neighbourhood workforce, enabling team‑based learning across primary, community, mental health, social care and voluntary sector partners.
Local educational institutions, including deaneries, should be contacted to understand training needs, recognising that flexible occupation and standard room types can often be used for more than one function. In addition to providing training opportunities for NHS staff, neighbourhood health centres may also support the education needs of the local community. Training provision should recognise the growing scale and diversity of the primary and community care workforce and support multidisciplinary learning within neighbourhood teams.
Flexible spaces in neighbourhood health centres may provide:
- clinical training rooms
- educational debriefing rooms, which can be multipurpose with general meeting rooms
- neighbourhood work facilities with IT equipment to replace traditional ‘staff library’ facilities
Operational principles
It is important that all providers co-locating and integrating into a neighbourhood health centre building understand the fundamental change in approach away from traditional commercial models of estate ownership and occupancy.
This programme proposes an alternative way of occupying space to drive greater efficiency, promote system and partnership working and facilitate genuine integration between the NHS and other services. There are vital underlying principles for occupying and operating within a neighbourhood health centre to maximise opportunities to address the wider determinants of health and social care;
- co-location of multiple services within the same building to promote the health and wellbeing of local populations, grounded by general practice services as an ‘anchor tenant’
- primary occupancy for all users is via bookable and shared space
- use of an effective electronic room booking system
- monitoring and measuring ongoing utilisation
- working together to use the space to its full capacity
- applying a greater level of flexibility and adaptability to meet the changing needs of service delivery and local population health
- strategic alignment with local authority regeneration and place‑based plans, ensuring neighbourhood health centres support wider ambitions for town centre renewal, accessibility, social value and sustainable community development
- working in partnership with other health, care and community settings within the neighbourhood to ensure services are aligned, complementary and shaped around people’s lives, rather than organisational boundaries, for example through effective collaboration between neighbourhood health centres and cohort‑specific hubs such as Best Start family hubs – to support early identification, prevention and targeted early intervention. This could include co-location of services, or co-ordinated referral pathways for babies, children and their families.
Co‑location is intended to support, but not substitute for, integrated working, which is enabled through shared operating models, digital connectivity and multidisciplinary team collaboration across physical and virtual settings.
Occupancy will be through the use of short to medium term flexible leases and licence agreements, allowing services to change and adapt over the life of the neighbourhood health centre to meet the strategic objectives and vision for place-based services responding to population health needs and social determinants of health.
This ethos behind the centres is more than a ‘lift and shift’ of activity. The facility will enable new ways of system working brining benefits for:
- managing the cost for services that improve local population health by ICBs or relevant boards of integrated health organisations
- removing personal liabilities and responsibilities associated with ownership and management of facilities by the integrated care system (ICS)
- removal of unnecessary commercial and administrative barriers that limit flexibility and integration
- creation of a more sustainable model of adaptability and flexibility (long life, loose fit)
These identified early benefits will free up providers from dealing with estates and facilities management issues, allowing them to better focus on delivering clinical services and promoting health and wellbeing.
The operational principles set out in this specification will be supported by clear, consistent frameworks for cost allocation, data reporting and performance management, to be applied across owners and occupiers and aligned with national guidance.
Managing utilisation and avoiding void space
Neighbourhood health centres are intended to operate as managed system assets, with a single, co-ordinated approach to room booking and space allocation. Responsibility for the day-to-day management of rooms, including booking, utilisation monitoring and reallocation of space, should sit with the organisation responsible for operating the building, supported by the centre manager the neighbourhood health centre employs to oversee the smooth and efficient operation of the building. The centre manager co-ordinates and chairs the building user group and is responsible for the measurement, reporting and delivery of the agreed benefits of neighbourhood health centres.
Smart building technology will monitor the utilisation and efficiency of the building and provide regular reports to the centre manager and building user group.
All bookable rooms are expected to be managed through a shared electronic booking system, providing visibility of availability across services and enabling space to be allocated dynamically in response to demand. Individual organisations or services will not have exclusive control over rooms unless this is explicitly agreed as part of the operating model.
All centre occupants will have access to the electronic booking system to book the space for the delivery of clinical, social care or other appropriate services as determined by the ICS and relevant stakeholder groups. They will co-operate with each other to develop and implement proposals to improve the utilisation of the building, which include:
- agreeing the principles of understanding and obligations for occupying and maximising space use
- surrendering excess space that is found not to have been used
- varying the rights and reservations of any occupancy agreement
- sharing occupation with others that provide health and care or complementary services
- carrying out utilisation studies or surveys to inform proposed use and room allocation
The centre manager, working with the building user group, is responsible for resolving booking conflicts, identifying under‑utilised capacity, and enabling space to be reallocated or shared where appropriate. This ensures that rooms are used efficiently across the day and that the building can respond flexibly to changes in service delivery, workforce patterns and population need.
In multi‑occupant neighbourhood health centres, active management of space is essential to avoid under‑utilisation and void space, and to ensure the building operates effectively as a shared system asset.
Digital check-in and reception functions will be designed to streamline access and reduce waiting times. Each centre will provide self-service digital check-in points, integrated with the NHS App and shared care systems, enabling patients to register their arrival quickly and independently. A single, shared reception desk will support all services within the building, offering face-to-face assistance and safeguarding oversight and inclusive support for those who require or prefer personal interaction. This unified approach ensures a consistent welcome, improves operational efficiency and reinforces the neighbourhood health centres role as an integrated, co-ordinated point of access.
Local systems may adopt a range of commercial and funding mechanisms to incentivise efficient use of space, reflecting local ownership and contractual arrangements. The specification does not prescribe a single commercial model, but all models should align accountability for utilisation with responsibility for the cost and operation of the building.
Long-life, loose-fit: sizing a neighbourhood health centre
Healthcare planners are encouraged to support conversations that arrive at the new way of working for flexible space allocation, the effectiveness of which will depend on an effective room booking system and building monitoring system.
The activity modelling tool provides a structured basis for NHS service planning and should be complemented locally by qualitative and place‑based approaches to sizing shared community, local authority and voluntary sector spaces.
From the start of proposal development, the activity modelling tool should be used to aid in determining the number of patient facing rooms required with the parameters set for opening hours and utilisation.
The calculator encourages users to think of rooms as flexible spaces that can be utilised by multiple different professionals and services throughout the day and over an extended period, not for a single purpose.
The supporting schedules of accommodation, which have been tested for better utilisation for core through to core++ centres, can be used as a basis to adjust the building size to suit the local need.
The sizing of shared community and non‑clinical spaces will require locally informed judgement, co‑design and iteration, recognising that demand may not be defined by activity data alone.
Sizing a neighbourhood health centre
Determining the size of a proposed neighbourhood health centre will require reference to the range and scope of services provided by the partners involved.
Demand and capacity modelling in healthcare planning seeks to process clinical activity data by applying a range of agreed growth and defined operational parameters for neighbourhood health centres. Sizing will be an iterative process, with early assumptions refined in the schedule as local needs, service models and pathways are confirmed.
The factors that need to be considered when estimating size are:
- population growth estimates
- access rates by age demographic
- adjusted access rate by ethnicity
- any proposed services relocating from hospital to community
- care pathways and model of care that support improving population health management priorities
- mode of appointment applicable to access rates and clinical model, such as proportion of home visits and face-to-face, telephone and video appointments
- appointment lengths for each mode of appointment
- setting needed for each mode of appointment
- open plan administration requirements alongside work spaces and remote working
- an increase in digital care models
Where proposals support the transfer of services from acute to community settings, systems should consider the full affordability and estate impact, including how income flows with activity and how any vacated estate is repurposed, reconfigured or released. This supports sustainable implementation and avoids creating unintended financial or operational pressures.
Neighbourhood health centres will achieve a target room occupancy rate of 80% during operational hours.
The activity modelling tool consists of functional content projections based on the aggregated clinical activity across all partners within the building, including:
- consultation and examination rooms
- treatment rooms
- interview and counselling rooms
- multidisciplinary team and group rooms
- imaging and diagnostic rooms
- virtual consultation rooms
Building design principles
Net zero by design
Neighbourhood health centres are conceived as next generation; future-proofed community assets designed from the outset to support a net zero NHS. They will be local exemplars of low carbon public infrastructure.
Each centre is delivered as a highly efficient, all-electric, net-zero energy building that meets or exceeds the NHS Net Zero Building Standard, regardless of scheme scale or capital value, with an aspiration to achieve Passivhaus standards where appropriate. The design approach prioritises exceptional building fabric performance, smart ventilation, smart energy control and modern low carbon heating systems, ensuring consistently low energy demand and a healthy internal environment.
Where relevant, schemes should consider heat network zoning regulations and any requirements or opportunities to connect to local heat networks, working with local authorities and other partners to understand, plan for and future‑proof designs for potential connection, where this supports wider place‑based energy strategies.
Wherever feasible, neighbourhood health centres should have on-site renewable generation, solar-ready roofs, smart energy systems and the capability to integrate with local microgrids and energy infrastructure. Whole life carbon is assessed from concept through to operation, with modern methods of construction (MMC), circular materials and design-for-disassembly forming the baseline expectation. To maintain performance long after handover, each centre will have a structured soft landings process, seasonal commissioning, ongoing energy monitoring and verification, and transparent reporting aligned with NHS sustainability obligations.
The relevant distribution network operator (DNO) should be engaged early to confirm grid capacity and connection requirements, recognising that constraints may affect feasibility, phasing and cost.
The key design principles are:
- concept and modelling
- MMC and low carbon materials
- construction (reduced embodied carbon)
- operational optimisation
- end-of-life reuse and disassembly
Buildings resilient to severe weather
Neighbourhood health centres are designed with resilience at their core, recognising that flooding, overheating and extreme weather events are becoming more frequent and are already disrupting access to healthcare, particularly for those in deprived and vulnerable communities.
Each centre is designed to protect access to essential care as well as provide safe, stable and supportive spaces during climate-related events; with safe access routes, alternative entry points and the ability to maintain essential operations if surrounding conditions deteriorate. In doing so, they help protect the most vulnerable communities and reduce health inequalities driven by environmental risks.
By including flood mitigation, heat resilience and operational continuity among their core design principles, neighbourhood health centres will form a national network of climate ready assets for now and well into the future, helping secure the NHS’s ability to serve communities, especially the most deprived.
Schemes should undertake a climate change risk assessment at an early stage, informed by the NHS England climate adaptation framework, to identify and mitigate risks to access, operation and service continuity.
Flood risk and continuity of access
From the earliest stage of site appraisal, every neighbourhood health centre assesses and mitigates flood risk, incorporating measures that protect both the building and the people who rely on it. This includes raised thresholds; resilient ground floor layouts; sustainable drainage systems; rainwater attenuation; and landscape features designed to slow run off and reduce local flood pressure. Mechanical, electrical and digital infrastructure is positioned and protected to ensure that services remain operational even during severe weather.
Overheating, heat stress and healthy internal environments
Overheating is now a serious and predictable risk for public buildings and the populations they serve. Each neighbourhood health centre is designed to build out heat stress primarily through passive design measures including high performance insulation and glazing, external shading, optimised building orientation and controlled solar gain, and natural ventilation strategies.
Internal environments will be monitored and regulated to maintain comfortable conditions throughout the year, supporting clinical delivery and wellbeing for patients and staff.
Mechanical cooling systems should only be introduced where the risk of overheating cannot be adequately mitigated through passive measures alone and where they are clinically required to support safe care delivery. Those that are installed must be highly energy efficient, use low carbon technologies and designed to minimise operational energy demand and associated emissions.
Recognising the increasing prevalence of overheating in existing housing, particularly in poorly insulated or densely occupied homes, neighbourhood health centres may also act as community cooling spaces during extreme heat. Their accessible, welcoming and climate-controlled environments provide a safe refuge for residents at greatest risk, strengthening the role of the centres as local anchors that protect health, wellbeing and social resilience.
Social value: community hubs that strengthen place and wellbeing
Neighbourhood health centres are designed as anchors of social value, supporting healthier, more connected and more resilient communities. They do far more than host clinical services: each centre provides accessible, welcoming spaces where people can meet, learn, socialise and access wider support that shapes health, education and opportunity.
Larger centres include flexible community rooms, spaces for group activities and places where voluntary and community organisations can convene and collaborate. Centres may also host local social enterprises, such as advice services, community cafés and local arts, sport and wellbeing groups, creating pathways into employment, training and prevention while keeping value circulating within the local economy. Centres may also co-locate with leisure and wellbeing facilities to bring multi-purpose health provision and support under an integrated neighbourhood health service umbrella.
Where enterprise or commercial space is provided, priority should be given to local businesses and social enterprises, particularly those rooted in or supporting more deprived communities.
Outdoor areas are designed as active, inclusive public spaces that promote physical and mental wellbeing. This may include outdoor gyms, walking loops, gardens, children’s play areas and seating that encourages social interaction, making the centres welcoming places to spend time, not simply places to receive care. Thoughtfully designed landscapes help connect the centre to its neighbourhood and support everyday physical activity.
Where located on or near high streets, neighbourhood health centres can play a key role in revitalising town centres by increasing footfall, supporting local businesses and reinforcing the high street as a focus for community activity.
Information, digital access points and signposting hubs provide residents with tools to navigate issues that influence health – from housing and benefits to family support, education and employment. By embedding these functions within a trusted local setting, neighbourhood health centres help reduce inequalities and create lasting social value across generations.
Together, these features make each centre a vibrant asset for the community, strengthening social networks, supporting local enterprise and contributing to the wider social, economic and environmental wellbeing of the neighbourhood it serves.
Infection prevention and control: flexible and resilient design
Infection prevention and control (IPC) is essential for safe, resilient and flexible service delivery within neighbourhood health centres and is embedded in the design approach from the outset.
The design of centres supports a move away from fixed, infection‑defined spaces towards adaptable, capability‑led environments, where clinical function is aligned to environmental capability and supporting infrastructure. Standardised rooms and building services enable spaces to flex between uses as service demand and infection risk change, while ensuring that activities are only undertaken in environments that meet the appropriate clinical and IPC requirements.
Learning from the Covid‑19 pandemic has informed a design approach that supports service continuity during periods of heightened infection risk. Centres are planned to enable the operational separation of patient pathways where required, including through direct access from public zones to clinical areas and the ability to cohort patients, and the flexible reconfiguration of space without disrupting routine preventative, diagnostic and community‑based care.
This approach supports a scalable response to surges in demand, maintaining a positive patient experience, protecting staff and service users and ensuring that IPC requirements are met without unnecessarily restricting service delivery.
Digitally-enabled, networked and operationally intelligent centres
Digital infrastructure is fundamental to the neighbourhood health centre model. Each neighbourhood health centre is designed as a digitally mature, interoperable and data intelligent facility that is seamlessly connected to shared care records, the NHS App and system-wide digital platforms. Crucially, every centre is digitally linked with all other neighbourhood health centres in its locality, creating a networked estate where space, activity and service availability are collectively visible and intelligently managed across the neighbourhood.
This connectivity means that each centre spans far beyond its physical footprint. Real-time utilisation and occupancy data flows across the whole neighbourhood health centre network enable dynamic space sharing, co-ordinated scheduling and cross site service optimisation. Patients can be directed to the right place first time; staff can work flexibly across multiple centres; and ICSs can actively manage capacity, throughput and extended hours using live operational intelligence.
Smart building technologies – including occupancy analytics, environmental sensors and interoperable room booking systems – provide continuous insight into how space is used and how services are delivered. This supports more efficient deployment of multidisciplinary teams, reduces bottlenecks and ensures that every centre and every room across the network contributes to the overall productivity of neighbourhood care.
Digitally-enabled clinical models, including virtual consultations, mobile diagnostics, community monitoring and shared team spaces, are supported by standardised, plug and play technology across all bookable environments. Where appropriate, digital twins and common data environments enhance lifecycle performance, enabling predictive maintenance, asset optimisation and ongoing reductions in energy use and carbon. This data environment also creates opportunities to support learning health system approaches over time, enabling continuous improvement in how and where care is delivered.
Together, this creates a digitally connected, operationally intelligent neighbourhood platform, where the estate actively supports integrated working, modern care pathways and the NHS’s long-term productivity and sustainability ambitions, enhancing productivity, sustainability and patient and staff comfort.
Design guide
External spaces
Patients, staff and visitors to neighbourhood health centre will make their first impression of it from the building’s façade and external space. Their appearance, therefore, needs to be well maintained and welcoming.
To accommodate the requisite number of services that make up either a core neighbourhood health centre or the larger core+/core++ models, all are likely to be 2 storeys in height. They could be standalone developments or form the base of much higher mixed-use developments.
The centres entrance level will contain public shared spaces and community spaces that will become an internal part of the public realm, and clinical spaces that need privacy and will be shielded from public view. This sets up a need to design external spaces that can create a public and a private area(s) inside and outside the centre.
External layouts should also allow for the safe access, positioning and servicing of mobile diagnostic units, where deployed, ensuring these can be integrated without compromising public realm quality, accessibility or operational safety.
The therapeutic value of external spaces, such as gardens and courtyards, as physical and, as importantly, visual amenities is a proven component in creating healthy buildings for patients and staff. Every neighbourhood health centre is also expected to contribute positively to community development and local biodiversity.
The role of the centres as essential community assets will be strengthened by developing participatory landscapes for play, exercise, education, creative (for example, activities for example, art) sport and gardening or contribute towards townscape spaces. Cost savings achieved by delivering a programme ‘at scale’ using standard components will be reinvested into such landscapes.
Schemes should maintain and enhance local biodiversity following local planning policy and, where applicable, meet statutory biodiversity net gain (BNG) requirements, using high‑quality landscape design to deliver both ecological and health benefits. Business cases should ensure sufficient provision is made within the cost plan to achieve and maintain landscape quality throughout the project lifetime. Nature‑based solutions should be prioritised wherever possible to deliver health, biodiversity and climate resilience benefits.
Key components for external spaces are:
- gardening
- sport
- creativity
- art
- education
- exercise
- play
Travel and access
Neighbourhood health centres will be planned to promote sustainable travel choices and enable convenient access for all members of the community. Site selection and design should prioritise strong public transport links, safe and direct pedestrian routes, and high-quality cycling infrastructure, including secure cycle storage and facilities that support active travel. Centres should be easy to reach without a car wherever possible, reducing reliance on private vehicles and encouraging healthier, low-carbon modes of travel.
Parking provision will be informed by local planning policy and the available public transport in the area, recognising the differences between inner-city locations with good public transport access and rural or suburban settings with limited connectivity. Parking should be sensitively integrated into the site and offer affordable electric vehicle charging facilities. Designs should avoid isolating the building behind extensive surface parking and incorporate landscaping to create a welcoming, accessible environment.
Travel and external access arrangements must be developed in partnership with a disability reference group, including people with sensory, physical and cognitive disabilities, to ensure that routes, drop-off points and building entrances are inclusive and intuitive. Opportunities to share parking or travel infrastructure with neighbouring organisations should also be explored early in the design process.
Bulidings
Neighbourhood health centres are based on a library of repeatable rooms and room clusters that can be assembled in different functional configurations to meet the clinical brief.
The adaptability of these centres throughout their 50+ year planned life and beyond is essential and every project will consider how the building will need to change over time.
Neighbourhood health centres will accommodate known NHS models of care from the outset but have the flexibly to adapt to new models throughout their operational life. Designers should consider whether the space could be converted, in part or whole, to other potential uses such as housing or commercial.
Each neighbourhood health centre will have a shared entrance space that acts as the focal point for welcome and orientation and the front door for access to all services operating in the building. This public zone will have digital check-in, a single shared reception desk and clear signposting, creating a simple and consistent experience for all visitors. From this shared space, people will move into the clinical areas and the wider community facilities, including spaces such as group rooms and community support rooms.
The proposed form of tenure, will enable a ‘neutral’ public zone, providing the accommodation for all public functions such as welcome, information, waiting and public toilets. Tenure and ‘plug in, plug out’ adaptability will mean that the public zone will be separate from the clinical, social and third party clusters.
Layouts and wayfinding strategies recognise that neighbourhood health centres are public buildings with public responsibilities yet contain mainly private functions. Patients and staff will be able to move around the building, and find their way easily and enjoyably, understanding how the centre works and gaining a sense of control.
Healthcare buildings will have qualities that reflect and promote a healthy lifestyle for patients, staff and visitors:
- well-tempered environments that provide patients, visitors and staff with those elements that are essential to our health, such as fresh and gently moving air, well balanced temperatures, good acoustics, high levels of day light penetration, sunlight without glare and the use of contrasting and changeable levels of lighting
- materials and finishes that have a zero or very low volatile organic compounds content and low embedded carbon
- healthy environments, wherever possible, that assist us in our daily lives to maintain a healthy lifestyle, for example, good food, social interaction, access to sunshine, nature, exercise and the arts
The building is constructed using good materials and finishes that maintain their quality. A level of detail in the design communicates that care and thought have gone into making the building fit for the patients and the staff.
Neighbourhood health centres provide a collaborative environment in which staff can work and learn together in multidisciplinary teams in safety, while also supporting their morale. The relationship between workplace design and wellbeing is an essential component in improving productivity, recruitment and retention.
Planning principles
New-build neighbourhood health centres will be planned on a standardised structural grid. This enables the clustering of rooms in an interchangeable configuration to maximise adaptability – the ‘long life, loose fit’ approach to their design, and offers opportunities for MMC, off-site manufacture and the development of standard product and mechanical, electrical and plumbing (MEP) assemblies.
We have chosen a grid of 8.1m x 7.2m as this size can accommodate a wide range of clinical and social functions. Local solutions may adapt the form of the building to suit site constraints, adhering to the building principles set out in this specification.
A standard set of room sizes from the revised HBN 00-03; Clinical and clinical support spaces (2026) can accommodate all required functions in various configurations, again to ensure long life adaptability and to maximise the advantages of assembling these buildings from a standard set of high-quality components. For the programme to benefit from scalability and repeatability, designs will use these standard room sizes wherever possible.
Within HBN 00-03; Clinical and clinical support spaces there are 2 sizes for consulting and examination rooms: 13.5 or 16 square metres. The latter can provide 3-sided couch access or, by aligning the couch against one wall, leave additional space in the room for escorts or family accompanying a patient or to place mobile equipment. When planning a centre, the appropriate ratio of 13.5 to 16 square metres sized rooms to meet the brief requirements should be considered, as well as how this fits efficiently within the chosen grid spacing.
To meet net zero carbon requirements and deliver the required percentage of MMC, an all-electric approach to the provision of building services is adopted. This increases the size of plant areas and primary distribution risers and horizontal runs. To provide sufficient depth for above ceiling services a repeatable floor to floor height of 4,000mm will accommodate floor to ceiling heights of circa:
- 2.55m in double loaded corridors
- 2.7m in consultation and examination and treatment rooms
- 3m in group and therapy rooms and single loaded primary circulation routes
Columns are standardised as a zone of around 450 millimetres square to allow for differences in structural methodologies, and layouts should be planned so that columns do not land within offices, consultation rooms or circulation areas, MEP zones and manufactured partitions. 150mm partition walls are used in the examples developed to meet acoustic, fire safety, robustness and MCC requirements. The walls around the stair and lift cores are at least 250mm to support consistent riser positioning, modular core walls and prefabricated structural/stability elements.
Riser positions should be consolidated into 2 to 4 major stacks, sized for prefabricated MEP riser frames. These should be in the centre of the race-track solutions (typically where support clinical rooms are located) to allow service distribution to the wings or quadrants without having cross-overs and maximise standardisation. 1,800mm corridor widths are included throughout to support MEP services distribution routes.
Adopting standardised assemblies for the shell and core design include but are not limited to:
- circulation cores; lifts and stair modules
- façade modules and assembles
- horizontal and vertical service zones
- defined allowance for future plant capacity
The incorporation of these strategies is reflected in the planning, circulation and engineering allowance percentage uplift in the schedule of accommodation.
Room assemblies
The standard rooms will be assembled to provide maximum flexibility of use in the clinical zone between general practice, community care and secondary care clinic rooms. Placing clinical rooms on an outside wall and the supporting rooms in a central core reduces the length of the clinical building zones.
These planning principles and room assemblies deliver a building that is inherently flexible, as the public circulation or waiting areas are ‘neutral’ under the landlord’s control, separated from the ‘plug in, plug out’ health, social care and community components that can agilely respond to change.
Figure 1 illustrates the indicative number of patient‑facing rooms by room type for a typical core, core+ and core++ model. The numbers within it are drawn from the published schedule of accommodation and show how spatial provision increases as the service offer expands. Rooms have been deliberately selected for multi‑use, with flexibility built in to maximise utilisation while remaining closely aligned to the types of services expected to operate within each space. This approach avoids unnecessary oversizing and ensures that rooms are proportionate, functional and fit for purpose. The diagram is intended to demonstrate the underlying rationale that services can be delivered via these typical rooms within the schedule of accommodation, timetabled on a sessional basis to increase utilisation of the rooms, rather than being owned full time by a particular service.
Figure 1 – indicative number of patient‑facing rooms by room type for a typical core, core+ and core++ model
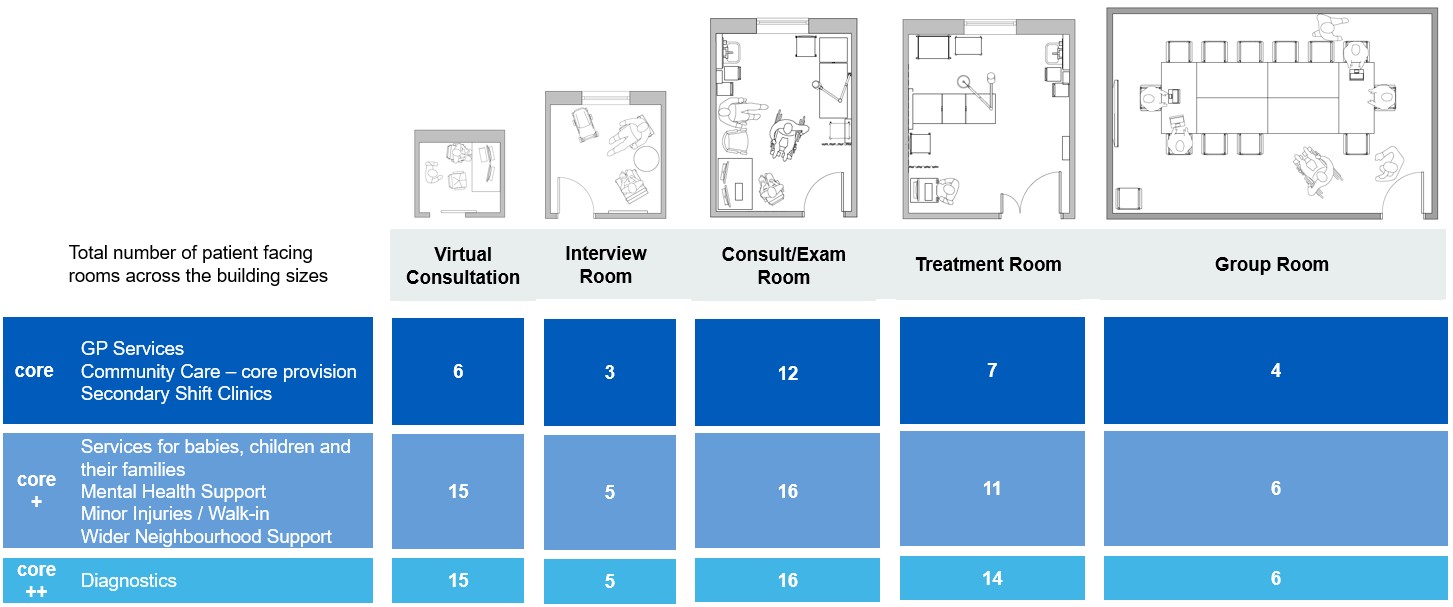
The image presents a table showing the indicative number of patient‑facing rooms across a neighbourhood health centre, broken down by room type and building size or service scope.
Across the top of the diagram are five room types, each illustrated with a simple floor‑plan icon:
- virtual consultation rooms
- interview rooms
- consult / examination rooms
- treatment rooms
- group rooms
Down the left‑hand side, the table is divided into three service levels, shown in progressively darker blue shades:
Core services
This level includes GP services, community care (core provision), and secondary shift clinics.
For this service mix, the building includes:
- 6 virtual consultation rooms
- 3 interview rooms
- 12 consult or examination rooms
- 7 treatment rooms
- 4 group rooms
Core+ services
This expanded level adds services for babies, children and their families, mental health support, minor injuries or walk‑in services, and wider neighbourhood support.
At this scale, the building includes:
- 15 virtual consultation rooms
- 5 interview rooms
- 16 consult or examination rooms
- 11 treatment rooms
- 6 group rooms
Core++ services
This level represents the largest and most comprehensive offer, with diagnostics added to the Core+ services.
At this scale, the building includes:
- 15 virtual consultation rooms
- 5 interview rooms
- 16 consult or examination rooms
- 14 treatment rooms
- 6 group rooms
Overall, the image shows how room numbers increase as service scope expands, particularly for treatment and diagnostic‑related spaces, while maintaining a consistent mix of consultation, interview, and group rooms.
Product assemblies
In new-build schemes, a standardised kit of parts underpins consistent internal layouts and operational efficiency across the programme, while providing sufficient flexibility for the building form and external envelope to be locally designed in response to environmental conditions, urban context and community identity.
The ProCure Framework (on the Futures collaboration platform; login required) product range will be the starting point but will require continuous review and continuous refreshing to minimise embedded carbon and eliminate volatile organic compounds in products as a pass or fail approach to materials.
Facilities management
Strong facilities management practices will be built into the programme to support the digital and smart building strategy. These practices will be enabled through the NHS digital toolkit and the buildings digital asset management solution, which will provide a consistent way to manage building and asset information from design through to day‑to‑day operation.
This approach will avoid teams working in silos. Instead, it will encourage joined‑up, evidence‑based decisions that focus on practical outcomes and long‑term performance.
The main design team should be supported by asset management (digital) specialists, operational estates and facilities management (EFM) teams and building information management (BIM) experts. This wider team will ensure buildings are designed to be operated, not just designed and handed over, reducing risk and improving long-term value.
Neighbourhood health centres will have a single point of day-to-day control, providing both real-time visibility and strategic insights into overall performance across the building, estates, facilities and engineering teams’ activities and business processes.
Neighbourhood health centre teams, including the building contractor, will provide a detailed commissioning strategy prior to practical completion of the building works. The plan will adequately evidence commissioning, sign-off processes and training; handover of quality documentation; ensure minimal defects and later disruption to the service via an early agreed soft landings approach; and identifying specifics that need to be introduced to the FM teams, centre manager and end users.
As part of scheme development and operation, neighbourhood health centre teams should consider proportionate security and counter‑terrorism measures appropriate to the scale, use and risk profile of the site. While many centres may fall below the statutory thresholds of the Terrorism (Protection of Premises) Act, schemes should be informed by relevant national guidance and undertake appropriate risk assessment, including consideration of safe access and egress, public zone management, physical mitigation measures where appropriate, and operational procedures to support preparedness and response.
This approach will maximise the reliability and availability of critical building assets by integrating with other key control systems, exploiting data to automate workflow, optimise internal and external ‘resources’ and drive compliance and reporting.
Fire safety
Neighbourhood health centres will be designed to ensure the safety of all users. Compliance with the functional requirements of the Building Regulations 2010 (as amended) may be demonstrated using HTM 05 02: Fire safety in the design of healthcare premises, read alongside Approved document B (Fire Safety), volume 2. Buildings other than dwellings. It is acknowledged that based on the patient dependency not all aspects of the HTM guidance may be applicable to all neighbourhood health centres and so reference to both will be required.
Each neighbourhood health centre must have a site-specific fire strategy, prepared by a competent person such as an independent expert adviser (AE), authorised person (fire projects – see HTM 05-01: Managing healthcare fire safety) or fire engineer if fire engineering is involved (see HTM 05-03, part J: Guidance on fire engineering of healthcare premises). The fire strategy will be robust and flexible enough to ensure safety at all times.
As a minimum, this strategy must reflect or address:
- the level of patient dependency. This will significantly influence the fire strategy: for example, where patients may be given local anaesthetics, that may impinge or their mobility and means of escape
- any local fire hazards such as the use of medical gases or the risk of arson
- space adjacencies, compartmentation, detection and alarm requirements, means of escape
- business continuity in case of fire
- ongoing maintenance of fire elements and the fire performance of the building fabric
The strategy will be robust and flexible enough to ensure safety at all times. Each neighbourhood health centre will provide an individual, site specific, fire strategy report which considers the patient dependency, local fire hazards, adjacencies, compartmentation, alarm requirements and fabric performance requirements.
The Building Safety Act 2022, and particularly the classification of a “Higher Risk Building” may apply to these buildings if forming the base of a residential development. Refer to NHS Estates Technical Bulletin (NETB) No. 2024/2, Building Safety Act (2022) – application to healthcare buildings for guidance.
Standalone 2storey healthcare buildings are typically not higher risk buildings, but the building safety act (BSA) duty holder competence and strengthened building control requirements still apply.
Area zoning: public spaces
The civic nature of neighbourhood health centres means that their ‘public’ areas will provide much more than basic clinical waiting and circulation space. There will be active, flexible spaces that promote ‘wellness’ and community activity rather than purely functional content. Public zones will provide:
- welcome meet and greet space
- check in and reception
- vertical and horizontal circulation
- waiting areas
- patient toilets
- changing places or toilets
- interview rooms
- multifunctional group rooms
- gardens
The public zone can also be used to support wider place making ambitions, and organisations should consider how this space could accommodate locally appropriate community uses. For example, entrance areas could be designed to host social enterprise cafés, community kitchens, informal gathering spaces or small education or digital access points. While these elements are not included in the core schedule of accommodation, local partners may choose to incorporate such features so public spaces maximise shared value for the benefit of the neighbourhood and support community outcomes.
A principal feature in neighbourhood health centres is connecting these spaces in both tenure and socially, recognising that these centres will be a focus within their communities for a wide range of activities. These design principles support the ambitions to address the social determinants of health through fostering strong community cohesion and empowerment.
The entrance itself will be easily identified, accessible and present positive first impressions for patients and staff, with a priority given to the provision of green spaces viewed from circulation and waiting areas.
Discrete areas can be secured when not in use while allowing other areas to be used as normal without enhanced security measures.
Consideration will be given to colour palettes and the user experience of these areas. They will be welcoming, calming and attractive places, shaped by the community, and not overly clinical in appearance.
Rooms that are multifunctional, including for use as a meeting space, group therapy room or education space, can be located in the public zone and may be designed for community use outside normal working hours. There is scope in the accompanying layouts to open up the group rooms to create a larger hall that the community can use.
The public will be able to easily access all spaces within the public zone. Access control to all spaces in the public zone will be minimal to allow their easy access by the public, but the capability to keep these spaces under active and passive surveillance is important.
Area zoning: clinical spaces
Clinical areas will be organised to optimise flexible use between tenants. Access to distinct clinical areas will be through the public zone and not through another clinical area to maintain future building flexibility and effective patient flow. Clinical zoning and circulation strategies should support the operational separation of patient cohorts where required, without constraining routine service delivery.
Direct access into a clinical ‘hot zone’ enables several rooms to be physically separated for the consultation and treatment of patients suspected of having contagious diseases. For information on building these principles into projects at briefing stages, refer to the Pandemic Preparedness Strategy: building our capabilities. The layouts show consideration for direct access into the family services spaces and mental health support rooms on the ground floor where this is required locally.
Clinical spaces within neighbourhood health centres include:
- clusters of consultation and examination, treatment and interview rooms
- diagnostic rooms, such as phlebotomy
- counselling and group therapy spaces
- multidisciplinary team rooms (team bases)
- therapy spaces
Clinical spaces in the larger models may also include
- imaging rooms: for the core++ example provided these are simple diagnostic rooms such as for ultrasound and utilising mobile x-ray equipment. Local activity modelling may adjust this to suit the modality required for site-specific needs
- enhanced procedures or minor operation suites
The use of remote consultation is increasing, and current sizing assumptions are based on a third of consultations being delivered virtually. This proportion should be confirmed locally using existing evidence and realistic future ambition. When sizing a neighbourhood health centre, teams should plan for a minimum of a third of consultations being remote unless partners agree a higher proportion.
The key considerations for accommodating digital consultation are that:
- it must not result in an overall increase in the space required for digital or physical consultation and examination
- the provision of digital consultation rooms must not reduce the quality of the working environment for clinical staff
The inclusion of digital consultation rooms or dedicated e-consultation pods will enable virtual appointments to take place on site without occupying rooms designed for face-to-face care.
Our ambition is for all clinical spaces, wherever possible, to benefit from natural light and views to nature.
Centralised waiting areas will be as close to the clinical area as possible to minimise and simplify the patient journey. The space metric for the waiting area allows for a variety of seating arrangements and seating types to support seating choice and allow seating to be incorporated specifically for those who may need assistance. Given the diversity of individuals, medical conditions and family group dynamics, no single type of seat or seating configuration can accommodate everyone who uses a waiting area.
Clinical support areas will be distributed throughout the building so that they can be used flexibly, where appropriate, between clinical units. These will include the following functional content:
- dirty utilities
- clean utilities and stores
- general storage
- specimen toilets
Area zoning: staff spaces
The integration of health, community and social care services and neighbourhood teams within neighbourhood health centres will make them an optimal location for the creation of robust multidisciplinary teams, providing integrated services and combined care pathways.
Staff accommodation is designed to support flexible, integrated ways of working, enabling teams to operate in small, functional neighbourhoods within the wider neighbourhood health centre, rather than fixed organisational silos. These work neighbourhoods support multidisciplinary collaboration, shared ownership of space and proximity to clinical and community settings, while retaining the flexibility to adapt as service models evolve.
Staff areas will consist of the following types of space:
- modern, flexible workspace areas
- small meeting rooms, interview rooms and quiet spaces within open plan neighbourhood workspaces
- remote consultation rooms
- training and development rooms, identified as part of the clinical brief (though there is scope for meeting rooms to fulfil this function)
- social spaces providing kitchen, dining and welfare facilities
- toilets and showers
- locker space and sufficient storage, which is critical to ensuring the building’s flexibility and that personal belongings are not left in clinical or other bookable spaces
- refreshment facilities and staff toilets in clinical areas
Office areas will be shared between organisations and co-located as much as possible, in flexible open plan configurations with some limited enclosed offices or pods for privacy or senior management. Agile working spaces that provide the following functionality will be provided: touchdown workstations for peripatetic staff, spaces for socialising, spaces for collaborative working and quiet working, and informal meeting facility.
Social spaces will be centralised and shared, creating a welcoming atmosphere that can be used for informal working arrangements and meetings as well as staff dining and rest.
To achieve these aims the neighbourhood health centres will look carefully at the serviced office model, which invests in a high quality shared social space for all the tenants and:
- provides a meeting place for rest and refreshment, informal working, meetings and interviews
- enables the dynamic chance encounters between disciplines
- sets the users and the staff on an equal footing
Area zoning: engineering and facilities management spaces
Consider the requirement for facilities management (FM) and engineering areas and ensure that they are tied in with an in-depth FM strategy. FM and engineering spaces include:
- cleaners rooms, including stores
- waste stores
- receipt and dispatch areas and technical areas; how and when goods/waste are distributed/collected around the building in a discreet manner will be considered as part of the operational principles and policies
- centre management and security facilities
- comms and server rooms
- risers and plant room
Providers should refer to the wider suite of NHS technical guidance when developing or adapting clinical spaces. This includes the relevant Health Building Notes and Health Technical Memoranda, the NHS Net Zero Building Standard and requirements linked to the Terrorism (Protection of Premises) Act. These documents offer detailed design and engineering expectations that sit alongside this specification and should be used to inform safe, resilient and future-ready neighbourhood health facilities.
Refurbishment schemes
Refurbishment schemes offer an important route for systems to expand neighbourhood health provision by making better use of existing estate. While the constraints of inherited layouts, structural arrangements and building condition will inevitably shape what is achievable, all refurbishment projects should apply the core principles of the neighbourhood health centre model to the fullest extent feasible. Refurbishment proposals should also consider opportunities to preserve and respond sensitively to the historic environment and local cultural heritage where relevant.
Considerations that should guide any redesign or reconfiguration of existing facilities are:
- utilisation and operating model
- digital connectivity
- net zero planning
- flexible and multi-use space
- clinical spaces and practical constraints
- inclusive by design
Utilisation and operating model
Refurbished centres should operate to the same utilisation expectations as new-build facilities. This includes extended operating hours and planning to achieve 80% utilisation of bookable spaces, supported by shared rooms, flexible scheduling and service models that maximise occupancy patterns.
Digital connectivity
All refurbishment schemes must ensure that facilities are digitally-enabled and fully connected to other neighbourhood health services, shared care records and system-wide digital platforms. Digital infrastructure should support the same core functions as new-build centres, including interoperable room booking systems, virtual consultation capability and participation in network-wide operational intelligence.
Net zero planning
Refurbishment projects should be supported by a credible plan to achieve net zero by 2040, with clear steps towards reducing operational and embodied carbon. Where full building fabric upgrades are not immediately viable, schemes should identify and implement practical near-term measures such as modernising building services, improving insulation and airtightness, upgrading lighting and ventilation systems, and planning for future integration of low carbon heating.
Flexible and multi-use space
Space in refurbished centres should be designed to be multi-use, adaptable and capable of supporting a range of clinical and non-clinical functions. Flexibility is crucial for longevity and allows the building to remain effective as service needs change. Wherever possible, layouts should be rationalised to create simple, legible and reconfigurable spaces that support a bookable room model.
Clinical spaces and practical constraints
It is acknowledged that full reconfiguration of clinical zones may not always be possible or cost effective in refurbishment settings due to structural and engineering constraints. However, all projects should seek to optimise clinical flow and flexibility in line with the principles of the neighbourhood health centre model. Providers are advised to refer to HBN 00-03: Clinical and clinical support spaces, which outlines appropriate space parameters and standardised room types that support adaptability, quality and long-term efficiency.
When planning refurbishment or reconfiguration, providers will need to understand how their existing rooms and layouts compare with the functional requirements of a neighbourhood health centre. To support this process, Table 1 below illustrates how current spaces can be mapped against the recommended schedules of accommodation. This will help identify where existing rooms align well with the model, where adaptation is feasible and where alternative solutions may be required to deliver safe, flexible and efficient clinical environments.
Refurbishment schemes should, where feasible, support flexible infection prevention and control arrangements that enable service continuity during periods of increased infection risk.
When planning refurbishment or reconfiguration, providers will need to understand how existing rooms and layouts compare with the functional requirements of a neighbourhood health centre. To support this process, the table below illustrates how current spaces can be mapped against the recommended schedules of accommodation.
The example in table 1 is based on extended opening days and hours, together with an assumed 80% utilisation of rooms, to deliver the annual number of appointments for a service using the activity modelling tool. This approach supports an objective assessment of whether existing accommodation aligns with the model and helps identify where adaptation, reconfiguration or extension of the building may be required to deliver safe, flexible and efficient clinical environments.
In the example shown, it has been assumed that the existing building does not include pods or dedicated virtual consultation spaces. Where this assumption does not hold, or where there is sufficient flexibility within the wider building, some of these functions may be accommodated within flexible work areas. This can enable integrated team working, supported by access to small meeting rooms, interview spaces and quiet rooms.
| Existing building room types (example only) | Existing number of rooms | NHC (core ++) Room requirement | Future need of rooms |
| Virtual consultation | 0 | 15 | +15 |
| Interview | 4 | 5 | +1 |
| Consultation and examination | 10 | 16 | +6 |
| Treatment room | 5 | 14 | +9 |
| Group room | 3 | 6 | +3 |
Inclusive by design
Refurbishment schemes should adopt inclusive, approachable and dementia-friendly design principles, recognising the needs of an ageing population and the central role of neighbourhood centres in frailty pathways. This includes intuitive wayfinding, accessible entrances, supportive lighting and acoustics, clear colour cues, and the creation of calm, welcoming environments that reduce anxiety and support people with sensory or cognitive impairments.
Publication reference: PRN02455