
1. Introduction
The NHS dental quality improvement (QI) programme begins in April 2026 and is a structured 3-year programme. Taking part is voluntary, and each year focuses on a different nationally selected topic.
This guidance supports dental practices taking part in year 1 of the programme (from April 2026 until the end of March 2027).
It should be read alongside section 8 of the NHS dentistry: quality and payment reforms contractual guidance, which explains the formal requirements for taking part, including:
- eligibility
- how to sign up
- contractual requirements
- payment
This topic guide provides more practical detail on the programme. It includes examples of potential QI activities that may be especially helpful for practices with limited experience in this area. More experienced teams may choose to use their own preferred QI approaches.
The guidance in this publication is designed to support dental teams in understanding and carrying out QI activities. It does not constitute clinical guidance nor does it replace the need for individual clinical judgement.
Eligible dental contractors who wish to participate in year 1 of the QI programme must sign up by 6pm on Friday 8 May 2026, by completing the sign-up form on the Contract Management and Payment System. Dental contractors cannot join after the sign-up deadline date.
2. Quality improvement
Quality improvement (QI) is a systematic approach to solving simple or complex issues by involving those closest to them. It focuses on:
- understanding the issue deeply
- developing ideas to support improvement
- testing these out using rapid cycles, using data to learn and adapt
The aim is to improve care quality and support the implementation of evidence-based guidance through reflective and shared learning.
2.1 Year 1 topic
The topic for year 1 (2026/27 financial year) will focus on assigning dental recall intervals in line with the National Institute for Health and Care Excellence (NICE) guidelines.
2.2 Why this topic was chosen
The year 1 topic aims to support dental teams in making consistent, evidence-based clinical decisions about recall intervals that are tailored to each individual’s needs.
NICE guidelines on dental recall (2004) outline a risk-based approach, using information from a patient’s comprehensive oral health assessment and review.
For adults, NICE recommends a recall interval of between 3 months and 2 years, based on a risk assessment, integrating clinical expertise and risk factors relating to a patient’s oral and general health. Later studies, such as the INTERVAL trial, support this approach.
Data on recommended recall intervals in England has been collected on FP17 claims since 2022. Analysis suggests that nationally, between April 2025 and February 2026, only 13% of patients deemed to be at low risk of oral disease (identified by recent history of decay and a Basic Periodontal Examination of 0 to 1) were assigned a recall interval of 12 months or more. This suggests that a significant number of patients are being recalled more frequently than is clinically necessary, increasing costs and inconvenience for them and limiting appointment availability for others.
Evaluation of the Prototype programme suggests that improvements can be made. Practices participating in this programme demonstrated closer alignment with NICE guidance than non-prototype practices. For example, prototype practices recommended 12-month recall intervals to 47% of their low-risk patients, and 24-month intervals for 48%.
Adherence to NICE recall guidelines will help dental teams to:
- tackle health inequalities by focusing resources on those with more complex dental care needs
- support access for new patients
- reduce clinically unnecessary check-ups for those with lower oral-health risk
3. Overview of year 1 quality improvement programme
By taking part in the year 1 of the QI programme, dental teams will work through a series of activities to improve how recall intervals are assigned. This will support teams to:
- understand their current position by reviewing the data to see how closely their recall intervals align with NICE guidelines and how they compare to other practices
- explore the reasons behind current recall patterns through internal peer discussions
- identify opportunities to improve or maintain adherence to NICE guidelines within the practice
- design and test QI activities, aligning with best practice, develop a plan, using the national template provided to implement and test these changes, with consideration to improving patient understanding of dental recall intervals.
- consider the impact of the QI activities tested and review whether adherence to NICE guidelines has improved
- share and discuss learning within the dental team and with their external peer group
- produce a practice report, using the national template, to capture what quality improvement activities were tested, the results and learning
- agree how successful changes can be sustained within the practice
4. Quality improvement cycle
Quality improvement involves a systematic, co-ordinated approach to solving a problem, using specific methods and tools to achieve measurable improvement within a health care setting, as outlined by The Health Foundation.
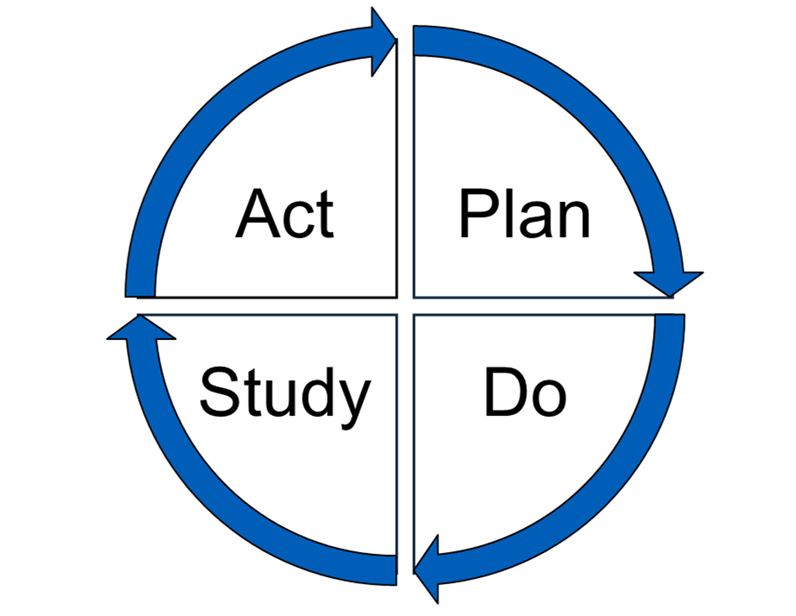
PDSA (Plan, Do, Study, Act) cycles are a helpful tool for improvement and provide a structured process. It is a 4-step, iterative, trial-and-learning method used to test, refine and implement changes for continuous quality improvement.
Step 1 – Plan
Identify the idea or change to be tested. Develop a plan for implementing the change(s) that you want to put in place, identify who will do what, and when and where the change will be implemented.
Step 2 – Do
Implement your plan and test the change(s).
Step 3 – Study
Analyse the data, comparing it with previous data and the expected outcomes and goals.
Step 4 – Act
Determine the next steps based on the results. Adjust the plan, scale up the test, or implement the change fully.
Figure 1: PDSA (Plan, Do, Study, Act) cycle
The requirements within the QI programme are designed to align with and run as a PDSA cycle across the QI year. The following sections have been developed to guide dental teams through each step of the cycle. A suggested timeline for the actions in each step has been provided in Appendix 1.
5. Step 1 – Plan
The first step of the QI cycle is to identify what you want to improve and how you will test those changes during the QI year. Develop a plan, using the national template provided in Annex 1, for how your practice will do this and measure improvement.
5.1 Identify a QI lead
Each dental practice must nominate a QI lead. They must be:
- based within the practice
- understand the QI programme requirements and timescales
- able to engage team members who support delivery of NHS dental care relevant to the QI topic and support shared learning
The QI lead does not need to be a clinician. However, if the QI lead does not have clinical experience, then at least one clinical representative from the dental practice should also attend the external peer meetings to provide clinical representation in these discussions (see section 6.2).
5.2 Establishing the baseline and measuring improvement
Measuring improvement involves:
- establishing a clear baseline
- defining specific and actionable metrics
- tracking data over time
There are 2 metrics for year 1 that measure recall intervals for patients assessed as low risk (metric 1) and high risk (metric 2) of oral disease.
Metric 1: low risk of oral disease
The NICE guidelines recommend that recall intervals for patients aged 18 years and over who have repeatedly demonstrated that they can maintain oral health, and who are not considered to be at risk of oral disease, may be extended over time up to an interval of 24 months.
Metric 1 therefore considers recall intervals assigned to patients identified as having a low risk of oral disease, with an assigned recall interval of 12 months or more. Low risk is defined as adults receiving routine care who have both:
- no evidence of new decay
- a Basic Periodontal Examination (BPE) score of 0 or 1
How metric 1 is calculated
Numerator: the number of FP17s for patients aged 18 years and over with no evidence of new decay and a BPE score of 0 or 1 who have a recorded routine dental recall of 12 months or more.
Denominator: the total number of FP17s for patients aged 18 years and over with no evidence of decay and a BPE score of 0 or 1 who have a recorded routine dental recall.
Metric 2: high risk of oral disease
The NICE guidelines recommend that patients at higher risk of oral disease are recalled at intervals of no longer than 12 months. This timing allows the dental team to reinforce preventive advice, monitor risk and support behaviour change.
Metric 2 therefore considers recall intervals assigned to patients identified as at high risk of oral disease, where the assigned recall interval is less than 12 months. High risk is defined as adults receiving routine care who have both:
- evidence of decay
- a Basic Periodontal Examination (BPE) score of 3 or 4
How to metric 2 is calculated
Numerator: the number of FP17s for patients aged 18 years and over with evidence of decay and a BPE score of 3 or 4 who have a recorded routine dental recall of less than 12 months.
Denominator: the total number of FP17s for patients aged 18 years and above with evidence of decay and a BPE score of 3 or 4 who have a recorded routine dental recall.
5.2.1 Data packs
National data packs reporting on these metrics will be provided to dental teams. This data will support discussions in internal meetings (see section 5.3) and in external peer groups (see section 6.2).
These data packs are produced using information submitted by dental practices to the NHS Business Services Authority (NHSBSA).
The first data pack will be provided in March 2026 and will include 2025/26 data. This will provide the baseline data. The first pack will cover the period 1 April 2025 to 28 February 2026, with an update in April to include full 2025/26 data up to 31 March 2026.
During 2026/27, the data packs will be updated monthly. This allows practices to:
- monitor changes in performance against the 2 QI metrics
- review how recall intervals are being assigned
- regularly monitor and measure the impact of the QI plan
- prepare for both internal peer review and external peer group discussions
Further information on using the data pack and suggested discussion points for internal practice meetings is provided in sections 5.2.2 and 5.3 below.
Further information and suggested discussion points for external peer meetings are provided in section 6.2.
5.2.2 Using the data pack
The data pack will be located within the Contract Management and Payment System.
For each of the 2 metrics (detailed in section 5.2 above) the data pack will provide:
- the number of patients (defined as the number of FP17s) with each of the 2 risk groups (those assessed as being low risk and high risk of oral disease as defined in the section 5.2)
- data on the recall intervals assigned by your practice for each risk cohort (presented as numbers and a percentage)
- a comparison of your practice recall rate for each cohort with the integrated care board (ICB), regional and national rates
- an anonymous view of your practice data broken down by individual performers within your practice
The data pack will be provided in a downloadable Excel format with separate tabs, including a guidance tab to explain what data is included and support on how to use the pack.
5.3 Internal practice discussion
The dental practice should hold an internal meeting to discuss recall intervals using the data pack provided to consider their patient cohort and assigned recall intervals. It is recommended as a minimum that attendees include:
- the QI lead
- other members of the dental team that support delivery of NHS dental care relevant to the QI topic
- the dental contractor(s), where possible
The internal peer discussion may consider:
- whether the recall interval data shows alignment with the NICE guidelines, and if not, why this may be the case
- whether the data reflects what members of the dental team had expected, and why
- whether any variation in recall intervals can be seen between individuals in the dental team, and if so, discuss why this might be the case. For example:
- does this align with certain patient cohorts?
- are there any default system prompts that impact recall intervals?
- are the recall intervals the same for different oral health risk groups?
- how the dental team are currently using the NICE guidelines to support recall interval decisions and whether there are any differences in approach between members of the dental team
- whether the data identifies any opportunities for improvement
- how the practice data compares to other practices locally and nationally
In addition to analysing the data pack, dental teams may find it helpful to identify and discuss real examples for each of the 2 metrics for the QI topic (detailed in section 5.2) at their meeting.
Example clinical scenarios for recall interval selection can also be found in Appendix G (pages 100 to 118) of the NICE dental recall guidance.
Regular internal peer meetings should be held throughout the year to revisit the monthly data packs and discuss whether the quality improvement plan is having an impact (see section 7, Step 3 – Study).
5.4 The aim (what are you trying to achieve?)
Once dental teams have reviewed and understood their baseline position, best practice is to identify a clear aim and use this to measure improvement.
The year 1 aim should be an aspirational goal specific to your practice. This recognises that participating practices will start from different baseline positions. For example, the percentage of adults identified as being at low risk of oral disease who have a recorded recall interval of 12 months or more may range from less than 5% to over 60%.
When setting the aim, dental teams may want to consider whether they need to improve or maintain their current practice. It can be helpful to consider wider evidence to help with this benchmarking.
For example, learning from the Prototype programme suggests that where a practice’s baseline is low, a reasonable aim would be to improve:
- the assignment of recall intervals in line with NICE guidelines by 20%, based on the 2025/26 practice contract baseline for the percentage of patients identified as being at low risk of oral disease with a recorded recall interval of 12 months or more
Where practice baselines are higher, the focus may be on maintaining good practice or a modest increase.
While measurable improvements are expected as a result of QI activities, it is recognised that not all quality improvement activities will be successful or lead to measurable impact. Where individual practices do not observe measurable improvement against their aim, this should not be viewed as a negative; learning from these outcomes can still inform future improvement activities.
5.5 Identifying areas for improvement (how to meet the aim)
Having considered the data, next identify areas for improvement that will work towards your overall practice aim (covered in section 5.4 above).
Below are suggested examples of QI activities your dental team may want to consider. However, the decision about what to include in your QI plan should be based on priorities identified through the internal data review and peer discussion.
In either case, consider tangible actions that individuals or the dental team can undertake to support risk-based recall in line with NICE guidelines.
Knowledge and application of the NICE guidelines
- Is the dental team familiar and confident in applying the following NICE guidelines when determining dental recall intervals:
- Consider the NICE dental recall guidance checklist (page 101 of appendix G). Does this align with your practice approach for risk assessment? Is there any learning which can be adopted within your practice?
Standardised approach to recall interval decision-making
- Is there a dental practice standard operating procedure (SOP) or clinical policy to support a standardised approach to recall interval decision-making?
- Are recall intervals considered again at the patients’ next oral health review in line with the NICE guideline?
Patient communications
- Consider the approach across the dental team for discussing recommended recall intervals with patients. For example, how are changes to recall intervals communicated to patients?
- Is the whole dental team confident in communicating recall intervals to patients, in line with their role?
Consider what communication tools are available or may be needed to support patient information on recall intervals (for example, patient leaflets or posters).
Appointment systems
- Is there a default approach to scheduling recall appointments? If so, how does this align with a personalised risk-based approach to dental recall?
- Can any default approach be amended or removed to better support individual clinical risk-based recall?
Case studies
- Consider how other dental teams have effectively implemented the NICE guideline to balance NHS routine and unscheduled dental care. Is there any learning that could be adopted?
- Case study example: Park View Family Dental in Gateshead.
Skill mix
- Consider how skill mix is supporting or could be used more widely to support adherence to the NICE guideline.
5.6 Developing the quality improvement plan
Once the improvement activities your practice will test have been identified, they should be developed into your practice QI plan, using the national template provided in Annex 1.
The QI plan should focus on 2 or 3 key objectives and actions.
These objectives and actions should be SMART (specific, measurable, achievable, relevant, and time-bound) and should be able to be implemented during the 2026/27 QI year (see below).
- Specific – clearly define the actions that the dental team wants to achieve.
- Measurable – set out how you are going to measure progress and success of the actions.
- Achievable – ensure the actions (what you hope to achieve) are feasible within the resources and time available and are agreed by the dental team.
- Relevant – ensure the actions can be achieved and support the aim of improving or maintaining clinical recall intervals in line with NICE guidelines.
- Time-bound – ensure the actions can be implemented and monitored during 2026/27.
The QI plan should be agreed with:
- the QI lead
- relevant members of the dental team
- the contractor(s)
6. Step 2 – Do
Once your QI plan has been agreed, step 2 is about putting it into practice.
6.1 Implement your improvement plan
The dental team should begin carrying out the QI actions set out in their plan.
To maximise learning, it is recommended that, where possible, the whole dental team providing NHS care to patients engage in the implementation. As a minimum:
- the QI plan should be shared with the whole dental team
- those involved in testing the changes should be clear about the agreed approach and timescales
- the QI lead should oversee progress and communicate regularly with the dental team throughout implementation
The monthly data pack should be used to monitor the impact of changes during and after the implementation of the QI activities (see section 7).
6.2 External peer review
A key benefit of QI is peer review. It allows practices to share learning. It also provides a structured process to:
- discuss strengths and weaknesses
- explore different approaches to clinical risk-based recalls in day-to-day care
- identify barriers to aligning with the NICE guideline
- share approaches to patient communication
- discuss how appointment systems may support or hinder risk-based recalls
Participating dental practices are to determine the membership of their external peer group. Details on how the external peer groups should be set up are outlined in the contractual guidance (section 8). Once agreed, the dental practices should notify the commissioner in writing of the membership of their peer review group. This must be done no later than 31 May 2026.
Peer review meetings can be held within smaller peer groups who meet separately, or as larger ICB-wide peer review meetings with all participating dental practices.
Participating dental practices must attend at least 2 peer review meetings during the QI year. External peer meetings will be facilitated by a nominated clinical lead.
The QI lead for each Dental Practice should attend the external peer review meetings. Where the QI lead does not have clinical experience, at least one clinical representative from the dental team should also attend to ensure clinical representation for the Dental Practice in these discussions.
6.2.1 Roles and responsibilities for peer review group
The role and responsibilities for the group members are to:
- participate in at least 2 meetings in each QI year
- be an active participant in the group and contribute to discussions
- be open to sharing experiences and learning, including sharing the findings of internal practice discussions and current practice with the peer group
- be open to new ways of working and approaches, implementing changes within their own practice to improve service quality
The role and responsibilities of the clinical lead are to:
- produce an agenda for the meetings, guided by the topic guidance and circulate it to the group in advance
- keep a record of attendance for all meetings
- help the group members achieve the objectives identified for each meeting
- aid the discussion, ensuring the group members have explored the key points
- encourage and support the group members to contribute to the discussion
6.2.2 Meeting 1
The first external peer group meeting should ideally be held between June and September 2026.
This meeting usually focuses on:
- sharing what each practice learnt from reviewing their data pack
- understanding where there is variation across the group
- exploring possible reasons for differences in recall patterns
Suggested discussion points:
- What did each dental practice learn from the internal data review? Did the data show what was expected?
- Are there differences in recall intervals between practices in the group? If so, what might explain this variation?
- How is each dental practice in the group currently using the NICE guideline in day-to-day recall decisions? Is there any learning which can be shared?
- What opportunities for improvement have dental practices in the group identified? How could these be implemented?
- What actions have dental teams included in their QI plan?
- How are QI leads involving others in their practice team in the QI programme? What approaches are helping build engagement?
Example external peer group scenario
- Dental Practice 1 has a recall interval rate of 47% of low-risk patients with a record recall interval of 12 months and over.
- Dental Practice 2 has a recall interval rate of 7% of low-risk patients with a record recall interval of 12 months and over.
- Dental Practice 3 has a recall interval rate of 62% of low-risk patients with a record recall interval of 12 months and over.
- Dental Practice 4 has a recall interval rate of 16% of low-risk patients with a record recall interval of 12 months and over.
Questions
- Are there obvious reasons for the variations in the recall rates between the practices in the group?
- Ask dental practices 1 and 3 to share their approach for assigning recall intervals. What are the differences? Do these differ from other practices in the group?
- Is there any learning which can be shared and adapted across the practices?
7. Step 3 – Study
Step 3 focuses on reviewing the results of testing. This involves monitoring progress and evaluating the impact of QI activities.
7.1 Internal practice review and discussion
Use the monthly data pack to monitor progress during the testing phase (Step 2) and to determine whether your QI activities are having the intended impact. The results of testing should be discussed at an internal practice meeting.
Suggested discussion points:
- How did the implementation and testing of the QI activities go?
- What does the updated data pack show? Has anything changed compared to your baseline? If so, is this a positive or negative change? Is this what you expected to see?
- Do you have other data or feedback, and what does this show?
- Are any specific activities having a noticeably greater positive impact?
- Are there any further activities the practice may wish to try? This may not be relevant depending on outcomes.
7.2 External peer review meeting 2
The second external peer group meeting should ideally be held between February and March 2027.
This meeting would usually focus on sharing:
- the actions each dental practice has taken
- the changes or outcomes
- main learning points
Suggested discussion points:
- What actions has each dental practice taken? How were these implemented, and how were other team members involved?
- What results have been seen by each dental practice so far? Consider the updated data packs and any changes or outcomes identified in the practice, such as feedback from dental team and patients.
- Which actions had a greater or least impact, and why? How will any successful changes be embedded and sustained in future?
- What learning would be useful to share with the external peer group? Are there examples that could be shared more widely (for example, as a case study shared by the commissioner across the ICB or region)?
- Are practices planning to test or adopt any further changes?
- What successes can be celebrated? Which key changes and improvements should be recognised?
8. Step 4 – Act
The fourth step is Act. In this step, you should decide what actions to implement based on what you learnt in Step 3. This is where practices:
- review the results
- identify gaps between actual and desired outcomes
- modify the solution if necessary
The goal is to ensure continuous improvement and learning in the problem-solving process.
Further resources are available on NHS IMPACT (Improving Patient Care Together)
8.1 QI Report
Participating dental practices will need to complete a QI report at the end of the quality improvement year. A reporting template is provided in Annex 2.
The quality improvement report should capture:
- the outputs from the dental practice’s internal review
- the actions tested
- the outcomes and changes observed
- learning identified and shared in the team
The QI report should be shared and discussed within the dental team, ideally with an opportunity for team members to contribute.
The Dental Practice must be able to provide a copy of the QI report when requested by the Commissioner for the purpose of post-payment verification.
9. QI year-end process
A declaration for the Dental Practice must be submitted by the dental contractor, for the 2026/27 QI year, by 6pm on 31 May 2027. Declarations cannot be submitted after this date. Non-submission of the declaration will result in full financial recovery of UDAs attributed to QI and an adjustment to the Dental Contractors delivered activity.
This should be submitted using the declaration form on the Contract Management and Payment System. This declaration is to confirm that all QI programme requirements and actions described in the dental practice’s quality QI plan have been completed.
Commissioners have the discretion to check compliance and can request evidence to confirm completion of the QI requirements. This may include reviewing the QI report and written evidence of attendance at external peer review meetings, either directly or through the Contract Management and Payment System, where available.
Appendix 1: Suggested timings for the 2026/27 quality improvement topic
This appendix provides timings to support dental practices in planning the quality improvement requirements during the year.
These timings are illustrative and flexible, except for the contractual deadlines for sign up and self-declaration at year-end.
March 2026
Dental practice actions
- Sign-up period opens week commencing 23rd March 2026.
- 2025/2026 national data pack will be made available in the Contract Management and Payment System. The national data packs will be provided in March 2026 and monthly thereafter.
Commissioner actions
- Commissioner to write to eligible dental contractors to confirm the sign-up period.
May 2026
Dental practice actions
- Sign-up period closes on 6pm Friday 8 May 2026. Dental contractors will be unable to sign up after the deadline date.
- Participating dental practices to identify a QI lead for their practice (Step 1).
- Dental practice review of national data pack and internal peer discussion to identify opportunities for improvement (Step 1).
- Dental practices to notify the commissioner in writing of the membership of their external peer review group. This must be done no later than 31 May 2026.
Commissioner actions
- Review the list of dental contractors who have signed-up for 2026/27 and confirm in writing to the dental contractor by 6pm on 29 May 2026 their eligibility to participate.
- Issue contract variations.
June to September 2026
Dental practice actions
- Meeting 1 of the external peer group to be held (Step 2).
- Begin development of practice improvement plan and, if applicable, any refinement post meeting 1 of the external peer group.
Commissioner actions
- Provide support, as required, for meeting 1 of the external peer group(s).
August 2026 to March 2027
Dental practice actions
- Implementation and monitoring of the improvement plan using monthly national data packs.
February and March 2027
Dental practice actions
- Meeting 2 of the external peer group.
- Complete quality improvement report. Share and discuss the findings and the report with the dental team.
Commissioner actions
- Provide support, as required, for meeting 2 of the external peer group(s).
February and March 2027
Dental practice actions
- Meeting 2 of the external peer group.
- Complete quality improvement report. Share and discuss the findings and the report with the dental team.
Commissioner actions
- Provide support, as required, for meeting 2 of the external peer group(s).
May 2027
Dental practice actions
- Dental contractor to complete and submit year-end declaration for the 2026/27 QI year by 6pm on 31 May 2027. Declarations cannot be submitted after this date.
Annex 1: Quality improvement plan template
Annex 2: Quality improvement reporting template
The QI report must be completed at the end of the 2026/27 quality improvement year. The Dental Practice must be able to provide a copy of the QI report when requested by the Commissioner for the purpose of post-payment verification. Please see the Quality improvement topic guidance for further information.