
Introduction
The NHS provider licence was introduced in 2013 for foundation trusts and independent providers of NHS-funded services. Much has changed since then, so we wrote to the sector in October 2022 setting out our proposals to update the licence conditions and align them with current statutory and policy requirements, including new legislation requiring NHS trusts to hold a licence from 1 April.
These changes were designed to support the development of effective system working, enhance our oversight of key services provided by the independent sector and help address climate change. We also proposed a number of technical changes to align the licence with our regulatory framework and reduce burden.
The proposed changes were subject to a statutory consultation from 28 October to 9 December 2022.
This document summarises the changes we proposed to the licence conditions, the feedback we received, any changes we have made to the final licence in response, and the next steps.
This document should be read alongside the final modified provider licence. The amended licence will come into effect on April 1 2023.
Consultation feedback
We received 72 responses via an online consultation webpage and by email and held two roundtables with trusts and integrated care boards (ICBs) organised by national partners.
In addition to feedback on each of the individual proposed changes, we also received more cross-cutting feedback on the use of the licence in general. We address this first before setting out the feedback received on each individual area.
The full breakdown of responses by organisation and question is outlined in Annex A.
1. Cross-cutting feedback on the use of the licence
Many respondents asked questions about compliance and enforcement, in particular how judgements around compliance with specific conditions would work in different local contexts and operating environments. These comments were made to varying degrees across most of the proposed changes but were particularly focused on the proposals to support system working.
The licence forms part of and supports the operation of NHS oversight arrangements by providing the legal basis for NHS England to provide mandated support to our most challenged providers in line with the principles and procedures outlined in the NHS Oversight Framework and operating framework.
The proposed modifications reflect existing statutory and policy requirements and so build coherence across national legislative, policy and regulatory frameworks. NHS England does not routinely monitor and assess compliance against each of the individual licence conditions. While providers should periodically self-assess, the changes reflect existing requirements and so in the majority of cases compliance can be assured through reference to existing plans/strategies. Should specific information come to light requiring support, we would consider this through our broader oversight and regulatory functions, working constructively with systems and providers to support improvement.
2. Supporting system working
Reflecting expectations around collaboration and cooperation
Proposal
A new condition: WS1 Cooperation – which requires NHS trusts, foundation trusts and NHS controlled providers to consistently cooperate with ICBs, Local Authorities and other organisations that deliver NHS care when developing and delivering system plans, delivering NHS services, improving NHS services, delivering system financial plans and delivering system workforce plans.
Feedback and response
Respondents welcomed this new condition, noting that it is a prerequisite for system working, financial sustainability, and fair and equitable access to skills and expertise across the local workforce. 88% of responses agreed or strongly agreed with the condition. All trusts and foundation trusts who responded to the question agreed/strongly agreed with the specific references to consistent cooperation for the purposes of delivering system financial and workforce plans.
Respondents told us that they prefer the term ‘collaboration’ to ‘cooperation.’ To some, ‘cooperation’ suggests a lower threshold of participation than the ongoing commitment to the design and delivery of shared plans at the heart of this condition. We have used the term ‘cooperation’ to reflect the statutory duty to cooperate as set out in sections 72 and 82 of the NHS Act 2006. However we consider ‘cooperation’ to be synonymous with our understanding of the illustrative (non-exhaustive) minimum behaviours we outline for provider collaboration in our Guidance on good governance and collaboration. In response to your feedback, we have added a definition of ‘cooperation’ to the provider licence linked directly to the collaboration expectations defined in guidance.
Respondents also asked how to account for the impact of different operating environments, priorities, and levels of system maturity across England on collaborative approaches, especially where relationships break down. Section 3 of the collaboration guidance outlines a stepped approach in determining local approaches to support collaboration, taking into consideration local contexts including health inequalities and system relationships.
Finally, respondents noted they would like to see reciprocal expectations placed on a wider range of system partners including large scale community interest companies and local authorities. Local authorities are key members of the integrated care board and integrated care partnerships in ICSs and play a crucial role in enabling integration and collaboration. However, it is not under NHS England’s remit to place expectations on local authorities. Many independent providers suggested that they should be included in system workforce plans by default, whilst others noted potential conflict between requirements to cooperate and their commercial and charitable sensitivities. At this time the duty set out in legislation only applies to statutory organisations and we have not extended the condition to them.
Outcome
We have included this condition in the final modified licence with added clarification about cooperation/collaboration. We have not extended the condition at this time to independent providers.
Reflecting the Triple Aim and health inequalities
Proposal
A new condition: WS2 The Triple Aim – which requires NHS trusts, foundation trusts and NHS controlled providers to have regard for and consider the likely effects of their decisions on the Triple Aim and have regard to related guidance.
Feedback and response
There was strong support from ICBs, trusts and foundation trusts for the condition. 77% of those who responded to the question agreed or strongly agreed with the condition, including 89% of trust and foundation trust respondents. One representative body disagreed on the basis that there was currently limited guidance for the condition.
The Triple Aim is a key element of the Health and Care Act 2022 and was intended to ensure the legislative framework supports local health and care organisations to work together in the interests of the populations they serve.
Respondents sought clarity about how to meet the Triple Aim’s expectations in the context of local circumstances. The triple aim requires organisations that plan and deliver healthcare services in a local area, including ICBs, NHS Trusts and foundation trusts, alongside NHS England, to consider the likely effects of their decisions on the shared goals – better health for everyone, better care for all patients, and efficient use of NHS resources – and therefore work together to achieve them both for their local system and for the wider NHS. How best to achieve this will depend on the context and what needs to be done. NHS England will keep under review whether developing further guidance would help support progress in this area.
Three respondents also recommended the condition wording should have a greater focus on collaboration as a means to meet the Triple Aim. We support and encourage providers to work with system partners to deliver the Triple Aim and note that in addition to the requirements in the Cooperation condition, the reframed Integrated Care Condition also requires all licensees to integrate and cooperate with wider health-related services for the purposes of reducing inequalities of access and outcomes.
During the consultation we asked whether elements of this proposal should be extended to the independent sector. 58% of independent sector providers who responded supported the extension of the Triple Aim condition to their sector. However, at this time the duty set out in legislation only applies to statutory organisations and we have not extended the condition to independent providers.
Outcome
We have included the proposed condition WS2: The Triple Aim in the final modified licence for NHS trusts, foundation trusts and NHS controlled providers. We have not at this time extended the condition to independent providers.
Reflecting digital obligations to enable system working and promote digital maturity
Proposal
- A new condition: WS3 Digital Transformation – which requires NHS trusts, foundation trusts and NHS controlled providers to comply with the information standards of section 250 of the Health and Social Care Act 2012 and with guidance related to digital maturity as they pertain to cooperation and the Triple Aim.
- A new requirement in NHS2: Governance arrangements paragraph 3(c) and CP1: Governance arrangements for NHS controlled providers paragraph 3(c) to have systems and processes in place to meet guidance on digital maturity.
Feedback and response
Respondents were generally in favour of these proposed modifications, noting that digital transformation is central to system working and delivering integrated care. 74% of those who responded agreed or strongly agreed with the inclusion of a digital condition, including 92% of responding trusts and foundation trusts; 83% of responding trusts and foundation trusts also agreed or strongly agreed with adding digital maturity to the NHS2/CP1 governance conditions.
Respondents consistently highlighted that digital maturity varies; moreover, several areas do not yet have interoperable systems in place. Some respondents also highlighted concerns with the delays in rolling out planned digital maturity assessments to support organisational improvement, which led to one trust and one representative body disagreeing with the proposals.
Respondents also raised the risk of burden in meeting information standards and wider digital requirements. Trusts and an advisory panel of digital leaders both highlighted the significant capital investment and access to an appropriately skilled workforce required to meet these expectations.
We discussed these issues further with digital leaders across the NHS. Many agreed with the policy intent, noting that reflecting existing digital expectations in the licence would support senior discussions about digital capabilities and priorities. They also welcomed further guidance to support engagement with trust and system leaders. We are setting up a working group of provider digital leaders to co-develop this supporting guidance in 2023/24.
Furthermore, a minimum of £500m funding for 2023/24 will be available to ICSs to meet minimum digital foundations in accordance with What good looks like. This will be allocated in line with the levelling-up agenda and with planning guidance. Funding has also been provided to ICSs to support the digital and data planning process with priorities outlined in the operational planning guidance. Consistent cooperation around the delivery of system plans should also provide expertise across systems, especially to providers at the start of their digital transformation.
In response to feedback, we have also added clarification to the digital maturity requirements in NHS2, noting that it is specifically governance and/or corporate systems and processes that are expected to be in place.
During the consultation we asked whether elements of this proposal should be extended to the independent sector. Most independent provider respondents did not support extending the licence conditions to all licence-holders. Respondents raised concerns that they do not qualify for NHS funding to support digital transformation. They also highlighted that the current variation in provider IT systems across the NHS poses a challenge when investing in interoperable systems. Independent providers also told us they are held to necessary minimum digital standards in both their CQC registration and the NHS Standard Contract and must also meet the s250 information standards set out in law.
Outcome
We have included the proposed condition WS3: Digital Transformation and the digital maturity requirements in NHS2: Governance arrangements in the modified licence. We have not extended these digital requirements to independent providers at this time.
Reframing integrated Care as a positive obligation to integrate service provision and reduce health inequalities
Proposal
To reframe: IC1 Provision of Integrated Care – as a positive obligation that all providers take steps to integrate services and enable cooperation with other services to improve quality and reduce inequalities of access and outcomes.
Feedback and response
Responses were highly supportive of the proposal to reframe this condition. 90% of those who responded to the question agreed or strongly agreed with the reframing of the Integrated Care Condition as a positive obligation on all licence holders. Two independent providers disagreed.
Feedback from providers and a representative body indicated that the condition as drafted allowed for different interpretations of integration due to the range of services delivered (including non-NHS services) within and across providers and local contexts. Respondents expected that these differing views could affect how providers work together to deliver integrated care.
The condition is intentionally drafted broadly to account for the wide range of services delivered across the NHS and is supported by established good practice and the standard NHS contract; providers and systems are supported in meeting expectations through a number of resources for integrated care and clear guidance addressing health inequalities through Core20PLUS5.
Some respondents also noted concerns around commercial or charitable sensitivities and potential for conflict in meeting this obligation alongside those in competition law. We do not intend this condition to require constitutional changes to businesses or charities. We have therefore amended paragraph 4 of the condition in the final modified licence to note that: “Nothing in this licence condition requires the licensee to take action or share information with other providers of health care services for the purposes of the NHS if the action or disclosure of the information would materially prejudice its commercial or charitable interests”.
Outcome
We have included the modified IC1: Provision of Integrated Care condition in the final modified licence with the noted clarification to paragraph 4.
Reflecting the importance of personalised care
Proposal
To expand: IC2 Personalised care and Patient Choice – to require providers to support the implementation and delivery of personalised care by having regard for relevant guidance and legislation, offering people control to manage their own health and wellbeing.
Feedback and response
89% of respondents agreed or strongly agreed with the expansion of the patient choice condition to include requirements around personalised care.
Feedback from across all respondent types supported the principle and felt it aligned with central aims of providing high quality care. Some providers asked for greater clarity on how to deliver personalised care given resourcing and operational constraints.
ICBs will need to consider how to incorporate personalised care alongside other priorities included in operational planning guidance and the Long Term Plan. The Universal Personalised Care guidance, co-produced with key stakeholders including people with lived experience, can support providers to offer personalised care, including supporting patients to have better control over their own healthcare budget. Furthermore, the Personalised Care Institute has provided a range of quality assured workforce development programmes to support implementation.
Outcome
We have included the modified IC2: Personalised care and Patient Choice condition in the final modified licence.
Removing the competition condition
Proposal
To remove Choice and Competition Condition 2: Competition Oversight.
Response
There was strong support for the removal of the competition oversight condition. 91% of respondents agreed or strongly agreed with the proposal, including 97% of trusts and foundation trusts and 79% of independent providers who responded to the question.
The 2022 Act did not transfer enforcement authority for competition oversight to NHS England as part of the dissolution of Monitor, however general competition law will still apply to prevent against anticompetitive practice.
Outcome
We have removed the competition condition from the final modified licence.
3. Broadening oversight and support of key services provided by the independent sector
Broadening the range of providers where continuity of services (CoS) conditions will apply
Proposal
- To remove redundant clauses from General Condition 9 (now G8)
- To allow NHS England to determine and apply continuity of service conditions to Hard to Replace Providers
- To amend relevant CoS conditions to reference Hard to Replace Providers.
This includes a mechanism added to G8 (Application of section 6 (Continuity of Service)) which sets out that the Continuity of Service conditions shall apply to licensees subject to a contractual obligation as CRS, or as determined by NHS England to be a Hard to Replace provider. CoS3 (Standards of corporate governance and financial management), Cos6 (Cooperation in the event of financial stress) and CoS7 (Availability of resources) will also be amended to refer to Hard to Replace Providers.
Feedback and Response
73% of respondents supported modifying the Continuity of Services (CoS) conditions to include a new category of Hard to Replace Provider. Trusts, ICBs, national stakeholders, and several independent providers were highly supportive, highlighting how important the changes were for ensuring stability of these essential services across the NHS.
21% of responding independent providers disagreed or strongly disagreed with the proposals as did a representative body. There are fewer than 10 providers who are not currently CRS but would be likely to come under the new ‘Hard to Replace’ definition. Of these, two responded to the consultation; both were in favour of this proposal.
Independent providers told us they would like more clarity on the definition of a Hard to Replace Provider and whether this would apply to individual services or to the provider as a whole.
NHS England consulted separately from 25 January to 22 February 2023 on the definition and designation approach for a Hard to Replace Provider through a consultation on changes to the Risk assessment framework for independent providers (IPRAF). Changes to the IPRAF include a definition of ‘Hard to Replace’ which will be applied to the provider where their services may be of sufficient scale or complexity nationally or regionally that NHS England considers that their unavailability, due to the provider’s insolvency or quality issues, would impact on patients.
Respondents were also concerned that additional regulatory burden would affect the viability of their business, particularly where there were financial pressures. Some suggested that the risk of ‘Hard to Replace’ designation may affect commercial decisions to enter or remain in the market for the provision of NHS services, including concerns they could be required to run an unviable service indefinitely via this designation. The continuity of service conditions are not intended to require providers of Hard to Replace services to run them indefinitely and providers of Hard to Replace services will not be subject to the CoS1 condition which requires CRS providers to offer a continuity of service over a defined period whilst the service is replaced, unless these services are also denoted as CRS.
Any action we take with providers under the CoS conditions will be proportionate, supportive and should protect, not interfere with, the provision of services. There are no planned changes to the way we undertake financial oversight of providers. Based on the experience of providers of CRS since the initial licence was published in 2013, we do not consider that being placed under the CoS conditions creates a high amount of regulatory burden.
88% of all respondents agreed that NHS England was the correct authority to decide who should be a Hard to Replace Provider, however three independent providers disagreed. From the comments received, disagreement was largely based on a wish for local systems to be involved in decision making.
Local systems already have a method to designate services at a provider as a Commissioner Requested Service and this would be the appropriate route to use for a provider who is essential for the continuity of access locally. However, we are introducing a category of ‘Hard to Replace’ because we know that some independent sector providers that either have no or very few services designated as CRS by a commissioner would be ‘Hard to Replace’ due to the scale of services they provide regionally or nationally. It is therefore necessary to view these providers on a national or regional scale and NHS England is best placed to do this. We will publish details when a provider is designated ‘Hard to Replace’.
A provider expecting to be designated as ‘Hard to Replace’ brought to our attention that the reference to Hard to Replace Providers was missing from CoS3 in the draft licence and parts of the consultation document. We wrote to independent providers on 9 February to clarify the position for the avoidance of doubt. We invited further feedback to adding ‘Hard to Replace’ to CoS3 but did not receive further feedback.
We will make this revision to CoS3 in the final modified licence. We have also updated G8 to refer to section 6 (Continuity of Service) in line with the section numbering in the modified licence.
Outcome
We have included these provisions in the final modified provider licence due to the importance of ensuring that NHS England has regulatory powers to intervene where the loss of a national, multi-regional or large regional provider would significantly reduce capacity across the NHS and impact access to patients.
Expanding the scope of CoS conditions to include quality governance standards
Proposal
To amend CoS 3 and CoS 6 to include standards of Quality Governance for Commissioner Requested services and Hard to Replace Providers and provide reasonable safeguards against the licensee being unable to deliver services when standards of quality governance have fallen below expectations.
Feedback and response
Responses were positive, with 83% agreeing or strongly agreeing to the addition of standards of quality governance to the CoS conditions. Respondents stressed the importance of a close working relationship between NHS England and other regulators, e.g. the Care Quality Commission (CQC).
Four out of 14 independent provider respondents disagreed or strongly disagreed with the proposal. Their disagreement was driven by concerns of duplicate regulation overlapping with the CQC. Respondents, including those in favour of the proposal, also sought further clarification around the assessment of quality governance standards.
Further details on our approach to quality governance oversight were consulted on as part of our consultation into the Risk assessment framework for independent providers.
We have worked closely with other regulators to develop these proposals and to ensure the approach does not duplicate inspection or oversight activities already undertaken. We will work with these organisations, using the intelligence gathered to ensure they offer high quality patient care to users of NHS services by offering support and, if necessary, taking the requisite regulatory action. Our approach to identifying risk at providers will be based on intelligence gathered from CQC as well as from local and regional stakeholders, with a starting position that providers are low risk unless intelligence suggests otherwise.
Outcome
We have included these provisions in the final modified licence given the importance of ensuring that NHS England can intervene as a regulator in the interest of patients.
4. Addressing climate change
Tackling climate change and delivering Net Zero
Proposal
A new requirement in: NHS2 Governance arrangements paragraph 3(b) and CP1 Governance arrangements for NHS controlled providers paragraph 3(b) – to ensure NHS trusts, foundation trusts and NHS Controlled Providers have regard to guidance on tackling climate change.
Feedback and response
73% of respondents, including 83% of trusts and foundation trusts, agreed or strongly agreed with the proposed addition of these requirements. Only 6% of trusts/foundation trusts disagreed. Respondents supported the principles of tackling climate change but raised concerns about the practicalities of meeting this condition, including cost.
The 2022 Act places duties on NHS bodies to reduce their environmental impact and reach net zero by 2045. Transferring the associated legal and policy requirements over to the licence does not affect the cost of meeting these requirements, but supports coherence across legislative, policy and regulatory frameworks and allows us to provide support where policy requirements are not being met.
The NHS has secured over £650 million in funding through the Department for Business, Energy and Industrial Strategy for providers to utilise towards meeting Net Zero and climate change obligations, with a further £220 million expected during 2023/24. Further funding has also been distributed to support improvements in electrifying ambulance fleet and LED lighting. A range of smaller grant funding is also available through other government schemes. To support research and innovation, NHS England’s Small Business Research Initiative has awarded £7 million for net zero clinical innovations, including £6 million awarded in February 2023.
During the consultation we asked whether elements of this proposal should be extended to the independent sector. 75% of independent providers opposed the introduction of a comparable licence condition for independent providers, noting that the statutory duties in relation to climate change only apply to trusts and foundation trusts. Providers also noted that climate change requirements already sit in the NHS Standard Contract.
Outcome
We have included the modified NHS2: Governance arrangements paragraph 3(b) and CP1: Governance arrangements paragraph 3(b) in the final modified licence. We have not extended the condition to independent providers.
5. Technical amendments
Shifting the focus of the costing conditions to support integration and improvement
Proposal
- To replace Pricing Condition 1 with new Costing Condition 1: Submission of costing information
- To replace Pricing Condition 2 with new Costing Condition 2: Provision of costing and costing related information
- To replace Pricing Condition 3 with new Costing Condition 3: Assuring the accuracy of pricing and costing information.
Feedback and response
68% of respondents agreed or strongly agreed with the modifications related to costing conditions 1 and 2.
63% agreed or strongly agreed with replacing Pricing Condition 3 with the new Costing Condition 3. One foundation trust disagreed with the proposals.
Some respondents raised concerns about the resources required to provide accurate and timely costing data. We are working closely with providers to understand how best to support this. Additionally, the new assurance process will provide trusts and foundation trusts with tools and support to improve the accuracy of data before and after it is utilised in the costing process. We understand this is a shift in approach but expect this should improve patient care and outcomes by embedding data reviews into business as usual. This supports the use of quality-assured costing data in ongoing decision-making. We also expect this to remove the burden currently felt when preparing for a specific costing audit once data reviews become part of ongoing practice.
Some independent providers questioned whether they would be expected to meet the same requirements as trusts and foundation trusts. We expect independent providers to meet the same basic costing requirements to achieve value, consistency, and better patient outcomes. Any work to extend the collection of costing information to independent providers will be co-developed. This would include assessing the granularity and complexity of required data to ensure it is reasonable and providers can complete it from their own records as far as possible.
Outcome
Given the need to bring the conditions related to costing up to date, we have included the proposed Costing Condition 1: Submission of costing information, Costing Condition 2: Provision of costing and costing related information, and Costing Condition 3: Assuring the accuracy of pricing and costing information in the final modified licence.
Amending the pricing conditions to reflect changes to national policy
Proposal
- To update Pricing Condition 4 (renamed as Pricing Condition 1) – to apply the rules and methods of charging for the provision of NHS services as set out in the NHS Payment Scheme.
- To remove Pricing Condition 5 (local modifications) from the licence.
Feedback and response
Respondents were in favour of these pricing condition changes, noting that the conditions need to reflect changes to policy and legislation to be effective. 63% agreed or strongly agreed with the proposed wording change to Pricing Condition 4 and 70% agreed or strongly agreed with the proposed removal of Pricing Condition 5. The remaining respondents were neutral.
Some independent providers queried whether this may apply to them in the future and others questioned whether there should be more local system input to pricing. Legislation requires NHS England to consult affected providers and ICBs about changes to the NHS payment scheme. There will always be an opportunity for providers to comment on specific proposed pricing changes before this condition would be extended to independent providers.
Outcome
We have included the modified Pricing Condition 4 and this will become Pricing Condition 1 in the final modified licence. Pricing Condition 5 (local modifications) will be removed.
Streamlining reporting requirements
Proposal
To remove reporting requirements from General Condition 6 (Systems for compliance), which requires licensees to self-certify against the licence, and Foundation Trust Condition 4/Controlled Provider condition 1, which requires foundation trusts to report on past and future compliance with the licence and to prepare a Corporate Governance Statement.
Feedback and response
Responses were in favour of these proposed modifications. 79% of respondents agreed or strongly agreed with the proposed removal of paragraphs 3 and 4 from General Condition 6 of the existing licence. No respondents disagreed with the proposal. 73% agreed or strongly agreed with the proposed removal of the Corporate Governance Statement requirements for NHS trusts, foundation trusts and NHS controlled providers, including 81% of trusts and foundation trusts who responded. 10% of trusts and foundation trusts disagreed or strongly disagreed.
There was broad consensus that these proposals would streamline requirements and reduce burden. However, some respondents noted the usefulness of the Corporate Governance Statement in focusing Board attention to governance processes and compliance issues and would continue this process internally.
Many respondents also noted the range of other reporting mechanisms that would continue, such as the annual report, annual governance statements and through any CQC well-led review. These will require Boards to continue to assess their compliance with corporate governance standards, and evidence of this compliance will continue to be considered as part of well-led assessments. However, removing this requirement would mean providers will no longer have to make statements on anticipated future compliance. On balance, there was a consistent view that any reduction in duplication and regulatory burden was welcome.
Independent providers will continue to self-certify through the Risk Assessment Framework, pending consultation.
Outcome
We have removed the reporting requirements from the final modified licence.
Applying conditions to NHS trusts and updating language to reflect the current statutory framework
Proposal
- To amend the licence to apply relevant existing conditions to NHS trusts and to extend the existing foundation trust conditions to NHS trusts excluding specific legislative requirements which relate only to foundation trusts
- To remove all references to Monitor or NHS Commissioning Board and replace them with ‘NHS England’, and to amend references to commissioning to reflect the new role of Integrated Care Boards and of bodies which may hold delegated commissioning functions.
Feedback and response
81% agreed or strongly agreed with applying all core conditions to NHS trusts (including the general conditions, integrated care conditions, costing and pricing conditions and continuity of service conditions, if applicable) and to extend the foundation trust conditions to NHS trusts. The remaining respondents were neutral to the proposal. 87% of respondents agreed or strongly agreed with the proposed wording changes to ensure the provider licence accurately reflects the names of the statutory NHS organisations.
Outcome
These modifications will be retained in the final modified licence.
Removing obsolete conditions
Proposal
To remove the following conditions:
- General Condition 3: Payment of fees to Monitor
- Foundation Trust Condition 2: Payment to Monitor in respect of registration and related costs
- Foundation Trust Condition 3: Provision of information to advisory panel.
Feedback and response
81% of respondents agreed or strongly agreed with the proposed removal of General Condition 3 from the licence. 57% of respondents agreed or strongly agreed with the proposed removal of Foundation Trust Condition 2 from the licence. 70% agreed or strongly agreed with the proposed removal of Foundation Trust Condition 3 from the licence.
Outcome
These conditions will be removed from the modified licence.
Amending the Fit and Proper Persons condition
Proposal
To accept the changes to licence condition G4: Fit and Proper Persons as per the consultation run by Monitor in February-March 2021.
Feedback and response
NHS England held a 5-week consultation into changes to the Fit and Proper persons requirements in early 2021. The responses demonstrated broad support for the proposal, and during the period of the consultation only 1% of all licence holders objected, which did not meet the objection threshold that applied at the time. The licence holders who objected held 3% of the share of supply in England, meaning the ‘share of supply percentage’ also did not meet the threshold.
We have reconsulted on this to ensure that any new licensees would have a chance to respond to the proposed modifications as well. All respondents to this question agreed with the previously consulted upon technical amendment to modify condition G4 to align it with Regulation 5 of the Fit and Proper Persons Regulations.
Outcome
The changes to Fit and Proper Persons Regulations will be transferred to the modified licence.
6. Wider feedback on the provider licence
We invited respondents to share further comments on the NHS provider licence. Several responses asked about the foundation trust model, noting the additional cost burden related to foundation trust governing bodies that NHS trusts do not face. Two other respondents asked about exemption regulations and suggested the licence was an unnecessary burden for independent providers not subject to the continuity of service conditions. We have taken note of these comments.
We also received suggestions that the licence should refer to organisational responsibilities regarding evidence-based practice, conducting meaningful equality impact assessments, and scrutiny and oversight over patient safety initiatives and clinical negligence costs. These responsibilities form part of the NHS2 governance arrangements condition around corporate systems and processes and do not need to be explicit.
Next steps
We are grateful to all who worked with us to co-develop the proposed licence modifications and for the engagement with this consultation. A modified final licence has been published alongside this response.
NHS trusts who have not previously been issued licences will receive their licences via registered mail throughout April. A digital copy of the licence can be found on our website here.
Annex A: quantitative analysis of responses received via the NHS England Citizen Space survey
We received 72 responses to the consultation via the Citizenspace page or email. Respondents included:
- 41 trusts and foundation trusts
- 14 independent providers
- 4 integrated care boards
- 9 national organisations or representative bodies[1]
- 3 provider collaboratives
- 1 individual not representing an organisation
Quantitative breakdown by question
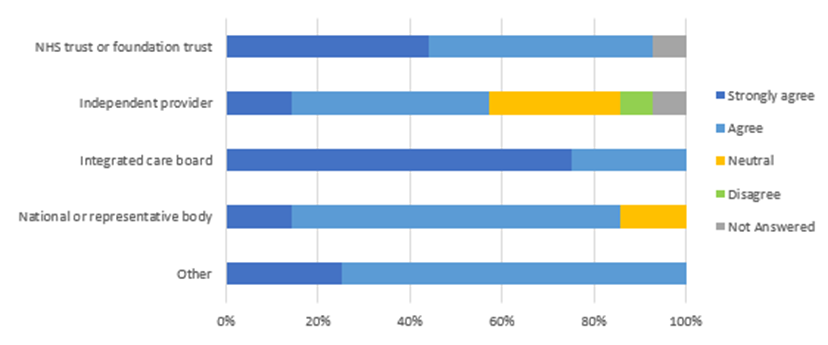
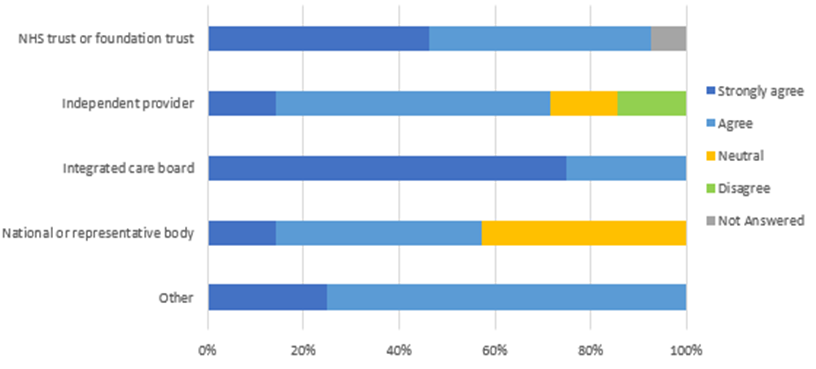
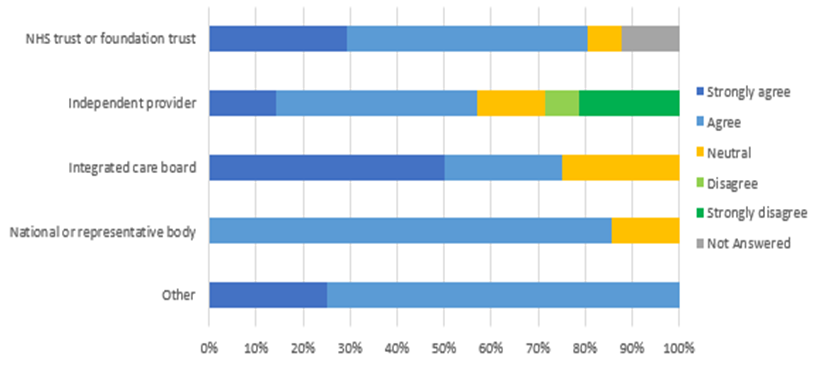
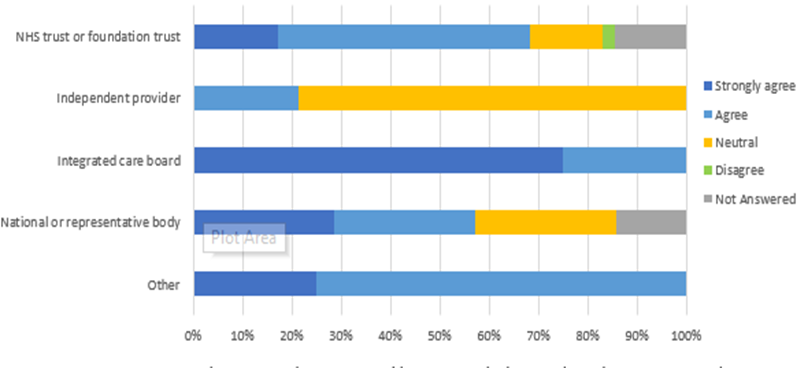
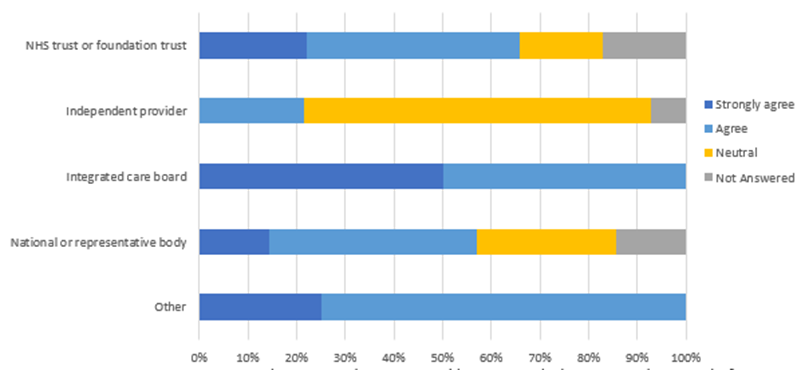
Q1. To what extent do you agree/disagree with the proposed new cooperation licence condition for the purposes of developing and delivering system plans, delivering NHS services and improving NHS services?
|
Respondent |
Strongly agree |
Agree |
Neutral |
Disagree |
Not answered |
|
NHS trust or foundation trust |
41% |
44% |
2% |
0% |
12% |
|
Independent provider |
7% |
57% |
29% |
7% |
0% |
|
Integrated care board |
75% |
25% |
0% |
0% |
0% |
|
National or representative body |
14% |
57% |
29% |
0% |
0% |
|
Other |
50% |
50% |
0% |
0% |
0% |
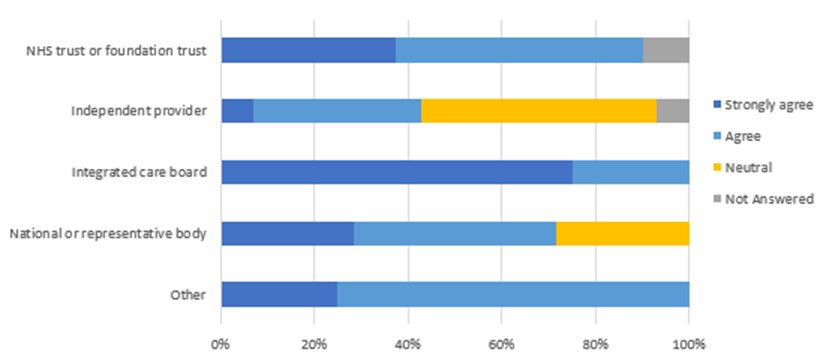
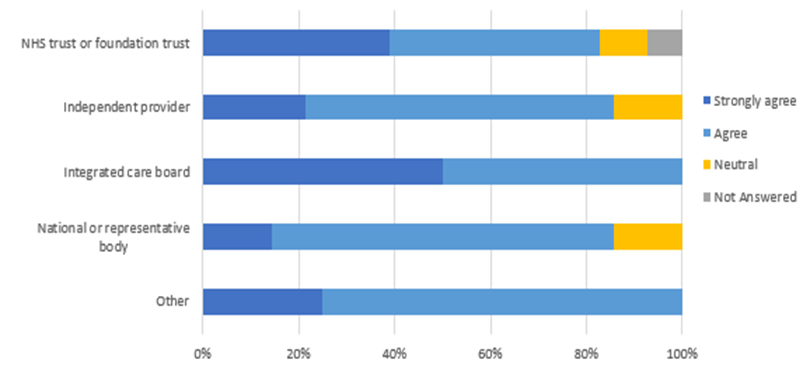
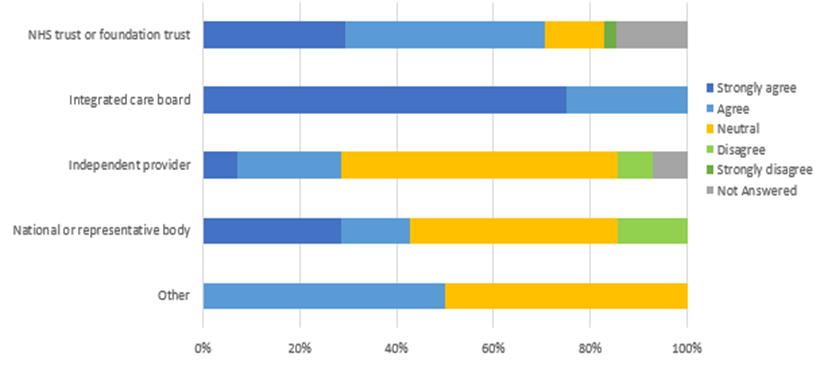
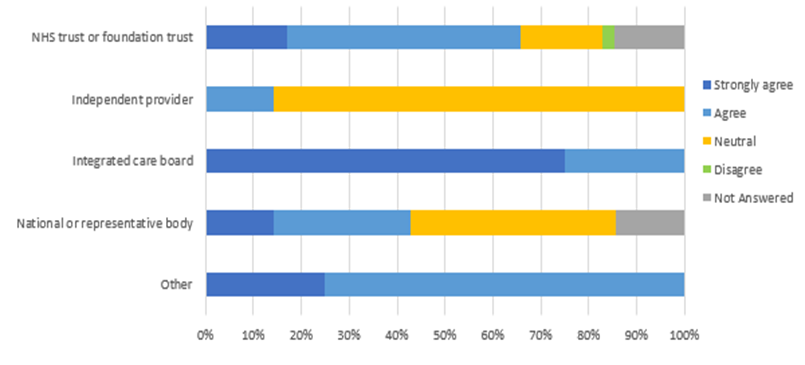
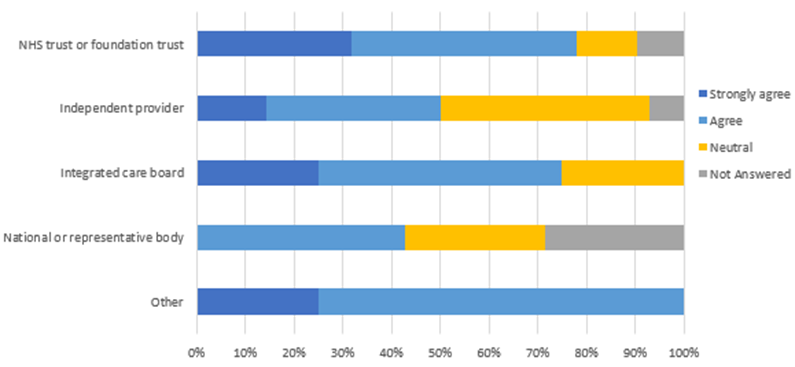
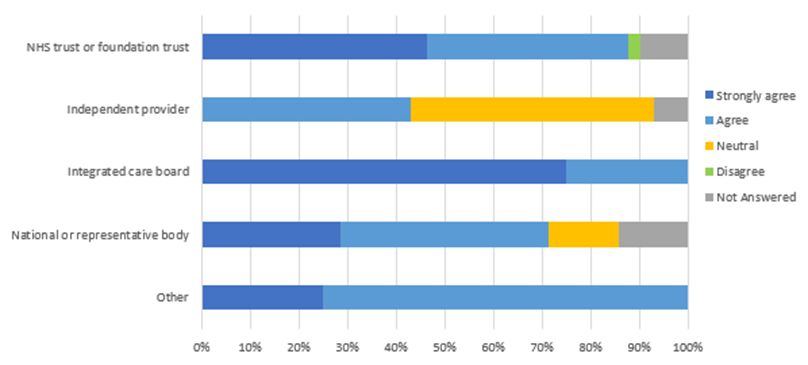
Q2. To what extent do you agree/disagree with the inclusion in the proposed licence condition of the requirement to consistently cooperate for the purpose of delivering system financial plans?
|
Respondent |
Strongly agree |
Agree |
Neutral |
Not answered |
|
NHS trust or foundation trust |
38% |
53% |
0% |
10% |
|
Independent provider |
7% |
36% |
50% |
7% |
|
Integrated care board |
75% |
25% |
0% |
0% |
|
National or representative body |
29% |
43% |
29% |
0% |
|
Other |
25% |
75% |
0% |
0% |
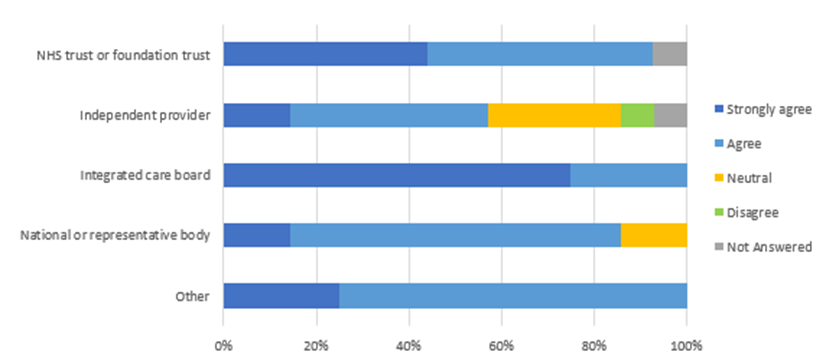
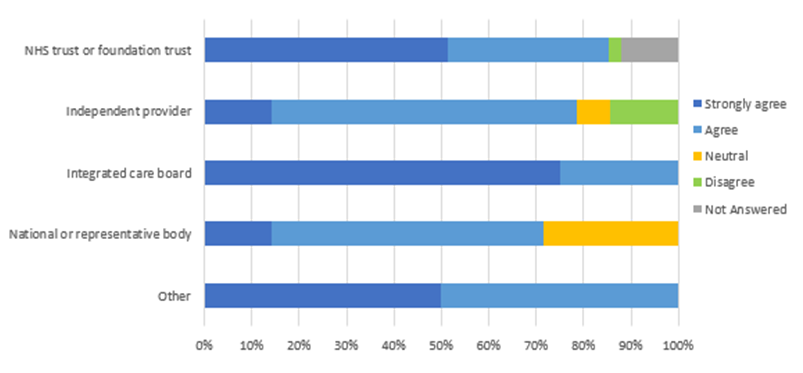
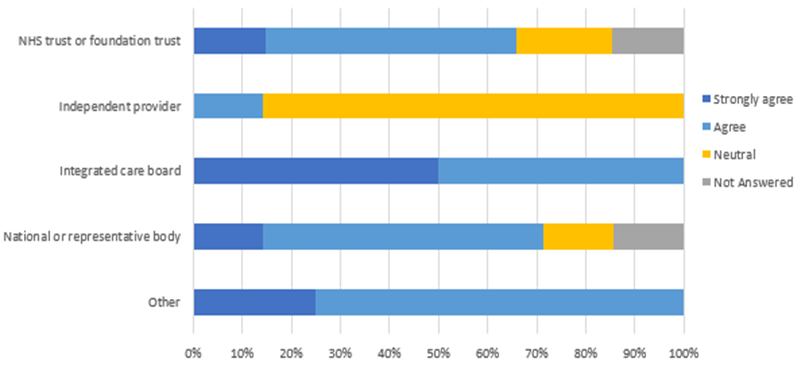
Q3. To what extent do you agree/disagree with the inclusion in the proposed licence condition of the requirement to consistently cooperate for the purpose of delivering system workforce plans?
|
Respondent |
Strongly agree |
Agree |
Neutral |
Disagree |
Not answered |
|
NHS trust or foundation trust |
44% |
49% |
0% |
0% |
7% |
|
Independent Provider |
14% |
43% |
29% |
7% |
7% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
|
National or representative body |
14% |
71% |
14% |
0% |
0% |
|
Other |
25% |
75% |
0% |
0% |
0% |
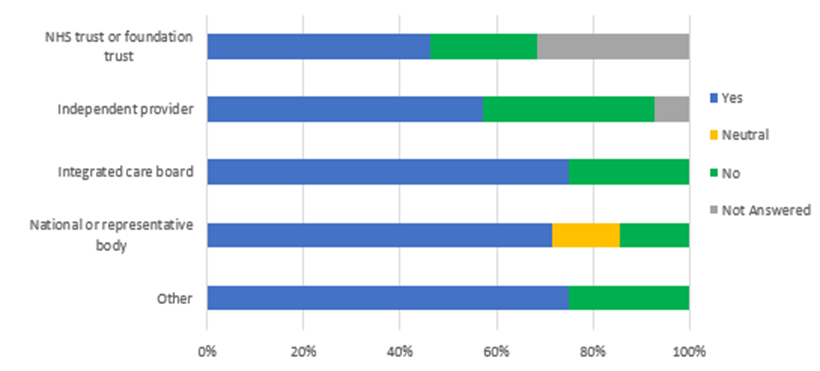
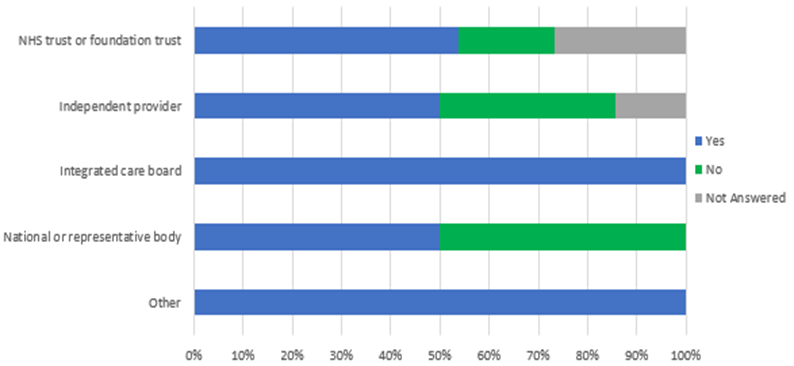
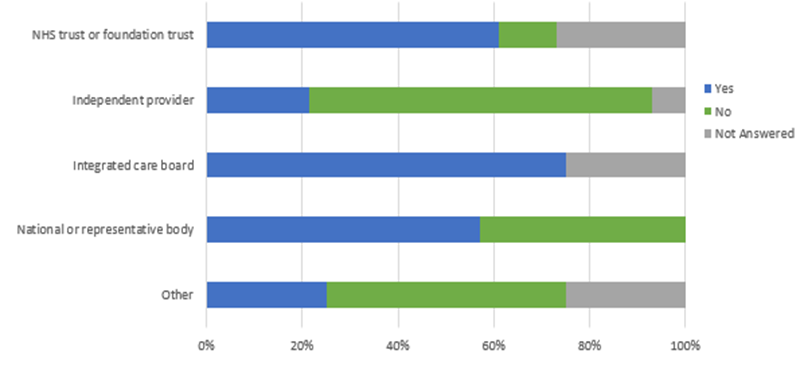
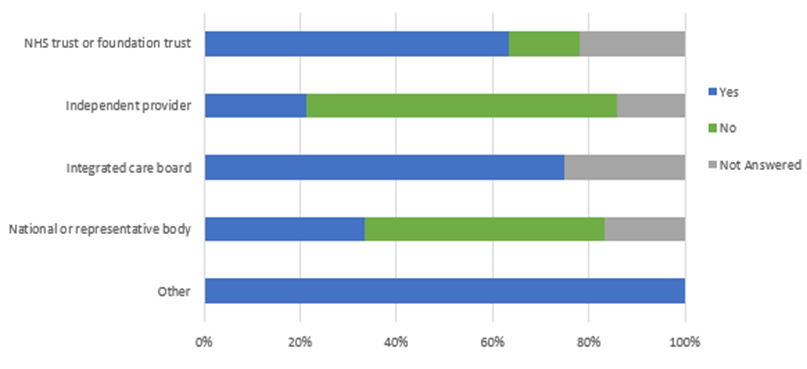
Q4. Are there elements of this proposed cooperation condition that should be extended to independent sector providers?
|
Respondent |
Yes |
No |
Neutral |
Not answered |
|
NHS trust or foundation trust |
46% |
22% |
0% |
32% |
|
Independent Provider |
57% |
36% |
0% |
0% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
|
National or representative body |
71% |
14% |
14% |
0% |
|
Other |
75% |
25% |
0% |
0% |
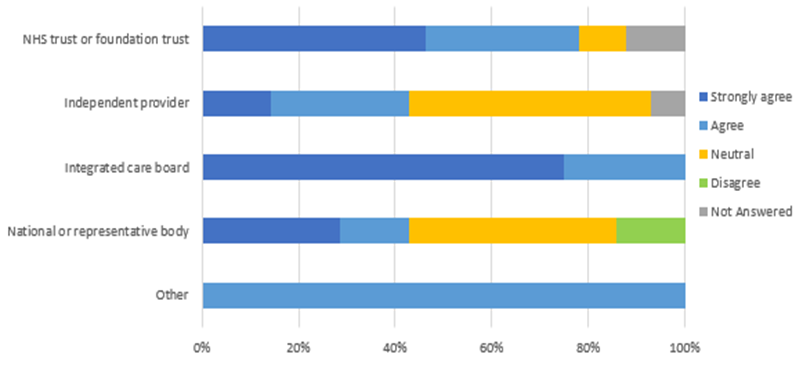
Q5. To what extent do you agree/disagree with the reframing of the Integrated Care condition as a positive obligation on all licence holders?
|
Respondent |
Strongly agree |
Agree |
Neutral |
Disagree |
Not answered |
|
NHS trust or foundation trust |
46% |
46% |
0% |
0% |
7% |
|
Independent Provider |
14% |
57% |
14% |
14% |
0% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
|
National or representative body |
14% |
43% |
43% |
0% |
0% |
|
Other |
25% |
75% |
0% |
0% |
0% |
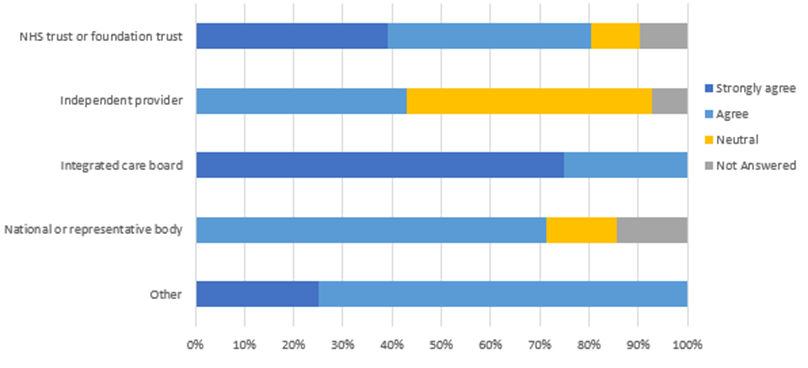
Q6. To what extent do you agree/disagree with the expansion of the patient choice condition to include requirements around personalised care?
|
Respondent |
Strongly agree |
Agree |
Neutral |
Not answered |
|
NHS trust or foundation trust |
39% |
44% |
10% |
7% |
|
Independent Provider |
21% |
64% |
14% |
0% |
|
Integrated Care Board |
50% |
50% |
0% |
0% |
|
National or representative body |
14% |
71% |
14% |
0% |
|
Other |
25% |
75% |
0% |
0% |
Q7. To what extent do you agree/disagree that the choice and competition condition 2: competition oversight should be removed from the provider licence?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Not Answered |
|
NHS trust or foundation trust |
51% |
34% |
0% |
2% |
12% |
|
Independent Provider |
14% |
64% |
7% |
14% |
0% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
|
National or representative body |
14% |
57% |
29% |
0% |
0% |
|
Other |
50% |
50% |
0% |
0% |
0% |
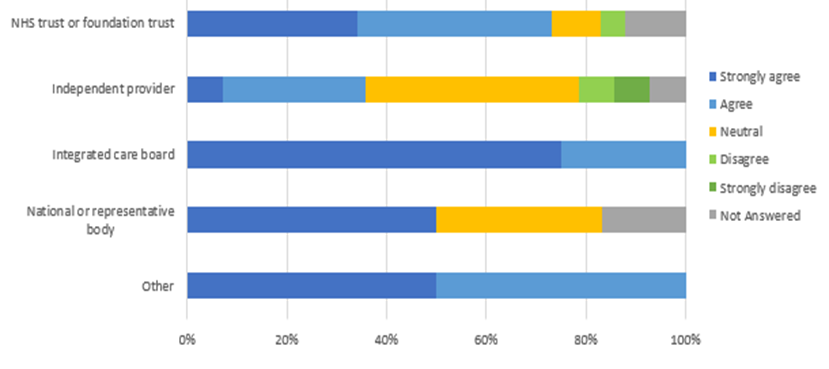
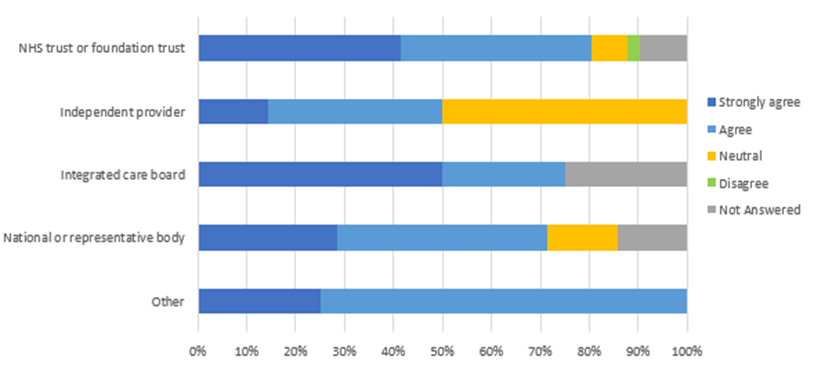
Q8. To what extent do you agree/disagree with the proposed inclusion of the Triple Aim, as set out in the 2022 Act, in a new licence condition for NHS trusts, NHS foundation trusts and NHS controlled providers?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Not Answered |
|
NHS trust or foundation trust |
46% |
32% |
10% |
0% |
12% |
|
Independent Provider |
14% |
29% |
50% |
0% |
7% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
|
National or representative body |
29% |
14% |
43% |
14% |
0% |
|
Other |
0% |
100% |
0% |
0% |
0% |
Q9. Are there elements of this proposed Triple Aim condition that should be extended to independent sector providers?
|
Respondent |
Yes |
No |
Not Answered |
|
NHS trust or foundation trust |
54% |
20% |
27% |
|
Independent Provider |
50% |
36% |
14% |
|
Integrated Care Board |
100% |
0% |
0% |
|
National or representative body |
50% |
50% |
0% |
|
Other |
100% |
0% |
0% |
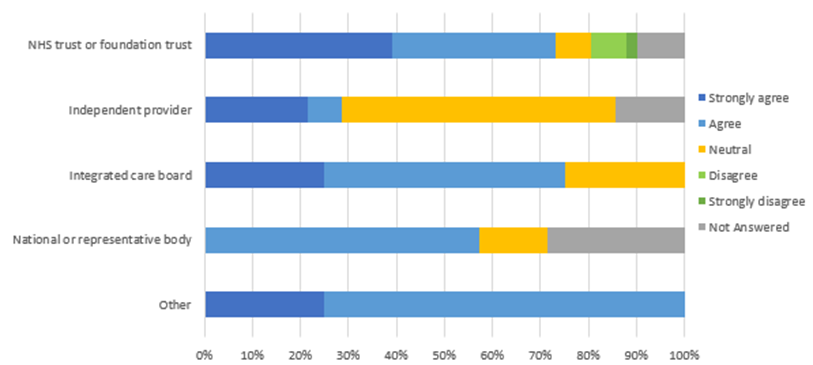
Q10. To what extent do you agree/disagree with the application of continuity of services conditions to Hard to Replace Providers?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Strongly Disagree |
Not Answered |
|
NHS trust or foundation trust |
15% |
56% |
15% |
0% |
0% |
0% |
|
Independent Provider |
7% |
50% |
21% |
7% |
14% |
0% |
|
Integrated Care Board |
25% |
50% |
0% |
0% |
0% |
25% |
|
National or representative body |
14% |
71% |
0% |
14% |
0% |
0% |
|
Other |
|
|
|
|
|
|
Q11. Do you agree that NHS England should have the ability to determine who is a Hard to Replace Provider?
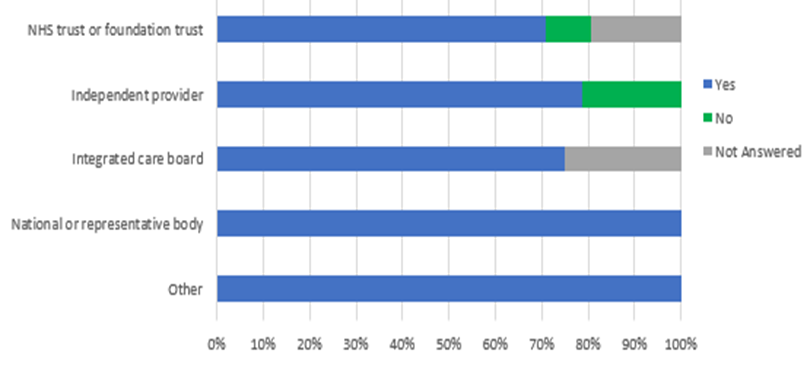
|
Respondent |
Yes |
No |
Not answered |
|
NHS trust or foundation trust |
71% |
10% |
20% |
|
Independent Provider |
79% |
21% |
0% |
|
Integrated Care Board |
75% |
0% |
25% |
|
National or representative body |
100% |
0% |
0% |
|
Other |
100% |
0% |
0% |
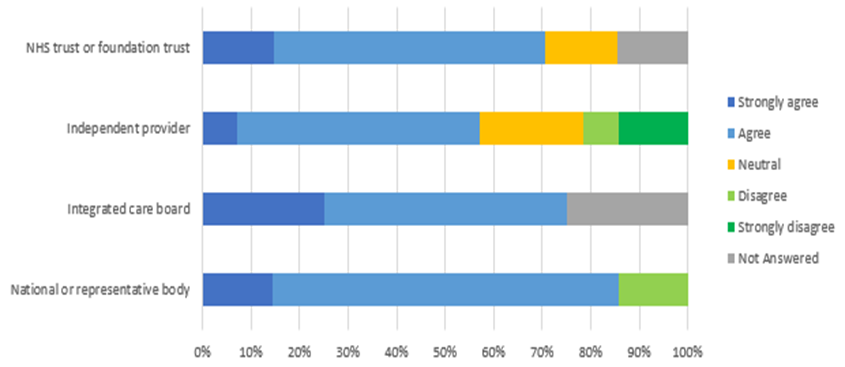
Q12. To what extent do you agree/disagree with the proposed new requirements for quality governance for independent sector providers that are subject to the continuity of services conditions?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Strongly Disagree |
Not Answered |
|
NHS trust or foundation trust |
29% |
51% |
7% |
0% |
0% |
12% |
|
Independent Provider |
14% |
43% |
14% |
7% |
21% |
0% |
|
Integrated Care Board |
50% |
25% |
25% |
0% |
0% |
0% |
|
National or representative body |
0% |
86% |
14% |
0% |
0% |
0% |
|
Other |
25% |
75% |
0% |
0% |
0% |
0% |
Q13. To what extent do you agree/disagree with a proposed new licence condition reflecting compliance with relevant digital information standards and digital maturity for the purposes of cooperation and meeting the Triple Aim?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Strongly Disagree |
Not Answered |
|
NHS trust or foundation trust |
34% |
49% |
5% |
0% |
2% |
10% |
|
Independent Provider |
7% |
29% |
50% |
7% |
0% |
7% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
0% |
|
National or representative body |
29% |
14% |
43% |
14% |
0% |
0% |
|
Other |
0% |
50% |
50% |
0% |
0% |
0% |
Q14. To what extent do you agree/disagree with the proposed amendment to the NHS governance condition and the NHS Controlled Provider condition reflecting the need for systems and processes to meet digital maturity expectations?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Strongly Disagree |
Not Answered |
|
NHS trust or foundation trust |
29% |
41% |
12% |
0% |
2% |
15% |
|
Independent Provider |
7% |
21% |
57% |
7% |
0% |
7% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
0% |
|
National or representative body |
29% |
14% |
43% |
14% |
0% |
0% |
|
Other |
0% |
50% |
50% |
0% |
0% |
0% |
Q15. Are there elements of these proposed digital conditions that should be extended to independent sector providers?
|
Respondent |
Yes |
No |
Not Answered |
|
NHS trust or foundation trust |
61% |
12% |
27% |
|
Independent Provider |
21% |
71% |
7% |
|
Integrated Care Board |
75% |
0% |
25% |
|
National or representative body |
57% |
43% |
0% |
|
Other |
25% |
50% |
25% |
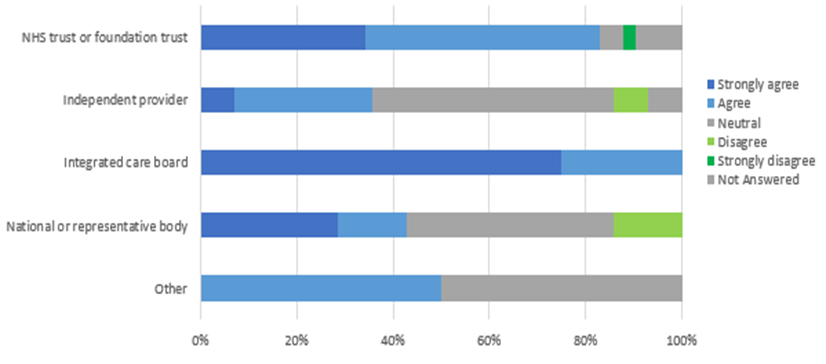
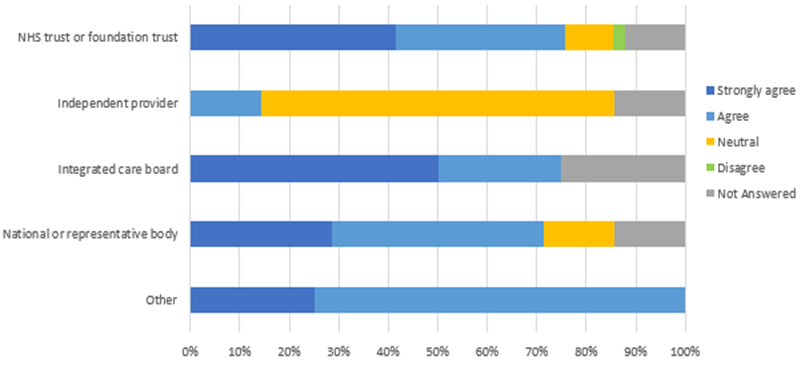
Q16. To what extent do you agree/disagree with this proposed addition of having regard to guidance on delivering net zero as a requirement of the NHS2/CP1 (previously FT4) and the NHS Controlled Providers condition?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Strongly Disagree |
Not Answered |
|
NHS trust or foundation trust |
34% |
39% |
10% |
5% |
0% |
12% |
|
Independent Provider |
7% |
29% |
43% |
7% |
7% |
7% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
0% |
|
National or representative body |
50% |
0% |
33% |
0% |
0% |
17% |
|
Other |
50% |
50% |
0% |
0% |
0% |
0% |
Q17. Are there elements of this proposed condition that should be extended to independent sector providers?
|
Respondent |
Yes |
No |
Not Answered |
|
NHS trust or foundation trust |
63% |
15% |
22% |
|
Independent Provider |
21% |
64% |
14% |
|
Integrated Care Board |
75% |
0% |
25% |
|
National or representative body |
33% |
50% |
17% |
|
Other |
100% |
0% |
0% |
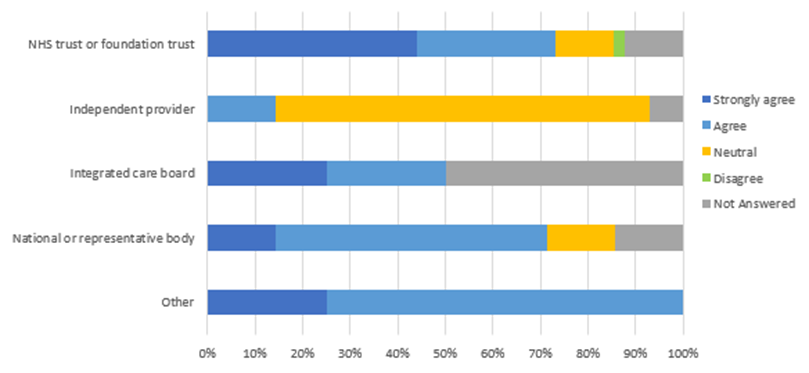
Q18. To what extent do you agree/disagree with the wording changes required to reposition pricing conditions 1 and 2 as the new costing conditions 1 and 2?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Not Answered |
|
NHS trust or foundation trust |
17% |
51% |
15% |
2% |
15% |
|
Independent Provider |
0% |
21% |
79% |
0% |
0% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
|
National or representative body |
29% |
29% |
29% |
0% |
14% |
|
Other |
25% |
75% |
0% |
0% |
0% |
Q19. To what extent do you agree/disagree with replacing Pricing Condition 3 with the new Costing Condition 3: assuring the accuracy of pricing and costing information?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Not Answered |
|
NHS trust or foundation trust |
17% |
49% |
17% |
2% |
15% |
|
Independent Provider |
0% |
14% |
86% |
0% |
0% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
|
National or representative body |
14% |
29% |
43% |
0% |
14% |
|
Other |
25% |
75% |
0% |
0% |
0% |
Q20. To what extent do you agree/disagree with the proposed wording change to Pricing Condition 4?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Not Answered |
|
NHS trust or foundation trust |
15% |
51% |
20% |
15% |
|
Independent Provider |
0% |
14% |
86% |
0% |
|
Integrated Care Board |
50% |
50% |
0% |
0% |
|
National or representative body |
14% |
57% |
14% |
14% |
|
Other |
25% |
75% |
0% |
0% |
Q21. To what extent do you agree/disagree with the proposed removal of Pricing Condition 5 from the provider licence?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Not Answered |
|
NHS trust or foundation trust |
22% |
44% |
17% |
17% |
|
Independent Provider |
0% |
21% |
71% |
7% |
|
Integrated Care Board |
50% |
50% |
0% |
0% |
|
National or representative body |
14% |
43% |
29% |
14% |
|
Other |
25% |
75% |
0% |
0% |
Q22. To what extent do you agree/disagree with the removal of paragraphs 3 and 4 from General Condition 6 of the existing licence?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Not Answered |
|
NHS trust or foundation trust |
32% |
46% |
12% |
10% |
|
Independent Provider |
14% |
36% |
43% |
7% |
|
Integrated Care Board |
25% |
50% |
25% |
0% |
|
National or representative body |
0% |
43% |
29% |
29% |
|
Other |
25% |
75% |
0% |
0% |
Q23. To what extent do you agree with the proposed removal of Paragraph 8: requirements to submit a Corporate Governance Statement within FT4 for NHS trusts and foundation trusts (renamed NHS2 in proposed draft licence) and CP1 for NHS controlled providers?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Strongly Disagree |
Not Answered |
|
NHS trust or foundation trust |
39% |
34% |
7% |
7% |
2% |
10% |
|
Independent Provider |
21% |
7% |
57% |
0% |
0% |
14% |
|
Integrated Care Board |
25% |
50% |
25% |
0% |
0% |
0% |
|
National or representative body |
0% |
57% |
14% |
0% |
0% |
29% |
|
Other |
25% |
75% |
0% |
0% |
0% |
0% |
Q24. To what extent do you agree/disagree that we should apply all core conditions to NHS trusts (including the general conditions, integrated care conditions, costing and pricing conditions and continuity of service conditions, if applicable) and to extend the foundation trust conditions to NHS trusts?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Not Answered |
|
NHS trust or foundation trust |
39% |
41% |
10% |
10% |
|
Independent Provider |
0% |
43% |
50% |
7% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
|
National or representative body |
0% |
71% |
14% |
14% |
|
Other |
25% |
75% |
0% |
0% |
Q25. To what extent do you agree/disagree with these proposed wording changes to ensure the provider licence accurately reflects the names of the statutory NHS organisations?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Not Answered |
|
NHS trust or foundation trust |
46% |
41% |
0% |
2% |
10% |
|
Independent Provider |
0% |
43% |
50% |
0% |
7% |
|
Integrated Care Board |
75% |
25% |
0% |
0% |
0% |
|
National or representative body |
29% |
43% |
14% |
0% |
14% |
|
Other |
25% |
75% |
0% |
0% |
0% |
Q26. To what extent do you agree/disagree with the proposal to remove General Condition 3 from the provider licence?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Not Answered |
|
NHS trust or foundation trust |
41% |
39% |
7% |
2% |
10% |
|
Independent Provider |
14% |
36% |
50% |
0% |
0% |
|
Integrated Care Board |
50% |
25% |
0% |
0% |
25% |
|
National or representative body |
29% |
43% |
14% |
0% |
14% |
|
Other |
25% |
75% |
0% |
0% |
0% |
Q27. To what extent do you agree/disagree with the proposal to remove Foundation Trust Condition 2 from the provider licence?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Not Answered |
|
NHS trust or foundation trust |
41% |
34% |
10% |
2% |
12% |
|
Independent Provider |
0% |
14% |
71% |
0% |
14% |
|
Integrated Care Board |
50% |
25% |
0% |
0% |
25% |
|
National or representative body |
29% |
43% |
14% |
0% |
14% |
|
Other |
25% |
75% |
0% |
0% |
0% |
Q28. To what extent do you agree/disagree with the proposal to remove Foundation Trust Condition 3 from the provider licence?
|
Respondent |
Strongly Agree |
Agree |
Neutral |
Disagree |
Not Answered |
|
NHS trust or foundation trust |
44% |
29% |
23% |
2% |
12% |
|
Independent Provider |
0% |
14% |
79% |
0% |
7% |
|
Integrated Care Board |
25% |
25% |
0% |
0% |
50% |
|
National or representative body |
14% |
57% |
14% |
0% |
14% |
|
Other |
25% |
75% |
0% |
0% |
0% |
Q29. For licensees who received their provider licence after March 2021: do you agree/disagree with the previously consulted upon technical amendment to modify condition G4 to align it with Regulation 5 of the Fit and Proper Persons Regulations?
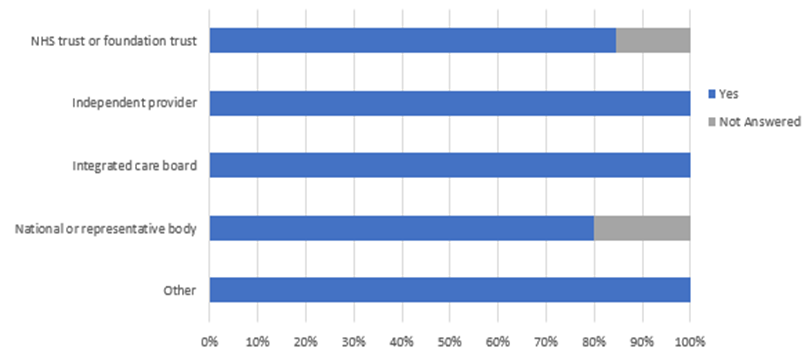
|
Respondent |
Yes |
Not Answered |
|
NHS trust or foundation trust |
85% |
15% |
|
Independent Provider |
100% |
0% |
|
Integrated Care Board |
100% |
0% |
|
National or representative body |
80% |
20% |
|
Other |
100% |
0% |
[1] Two national or representative body organisations submitted letters in response to the consultation content but did not respond to any of the individual questions in the survey. They have been excluded from the quantitative analyses.