
Please note: This document is formal statutory guidance for NHS bodies designated as relevant bodies. It may also be helpful to other bodies, such as local authorities and combined authorities when jointly working with a relevant body.
This guidance supersedes previous guidance on delegation and joint working issued in September 2022. It provides an overview of the legislative changes set out in the Health and Care Act 2022, guidance on how to implement the new legislative options available to delegate and jointly exercise those functions and limits on the use of these powers.
Purpose of this guidance
1. This statutory guidance provides an overview of the new collaborative working arrangements that are possible between NHS organisations and local government following commencement of the Health and Care Act 2022 (the ‘2022 Act’), with further technical guidance in the supporting annexes.
2. The new legislation is generally permissive, allowing delegation and joint arrangements to develop and evolve in ways that best suit the needs of patients and the public. The guidance therefore explains what delegation and joint working arrangements are permitted by the legislation, and when these can be used. This enables organisations to sense check that their proposed delegation or joint exercise of any statutory functions is done lawfully and in accordance with the principles of good governance, and is consistent with recommendations and expectations set out in this guidance in relation to delegation or joint exercise.
3. This guidance is issued under new section 65Z7 of the National Health Service Act 2006 (the 2006 Act), inserted by the 2022 Act. NHS England, integrated care boards, NHS trusts and foundation trusts must have regard to this Local authorities and combined authorities may also find this guidance helpful when working jointly with a relevant body.
4. The guidance should be read alongside the National Health Service (Joint Working and Delegation Arrangements) (England) Regulations 2022 as amended last year (the ‘2022 Regulations’), which list the functions that should never be delegated or jointly exercised. These restrictions are covered further at Annex E of this guidance, which also sets out the additional recommendations/expectations that organisations must have regard to when deciding whether to delegate or jointly exercise a function.
5. Considering the additional potential complexity of integrated care board (ICB) to provider delegation, associated risks, and the significant operational and financial pressures facing systems in 2024/25, NHS England continues to expect that ICBs not seek to use these powers in financial year 2024/25. This hold does not apply to other joint working or delegation arrangements under Section 65Z5 of the 2006 Act. Relevant bodies should refer to Annex G of this guidance for further information on the hold.
6. Entering into new collaborative working arrangements can have a significant impact on the decision-making of organisations involved in those arrangements. It requires careful consideration and preparation for the changes in responsibility and resource – ensuring proper governance arrangements are in place that set out clearly how the arrangement will work, and how they will meet their organisation’s financial obligations.
Background
7. The health and care landscape is evolving – moving towards ever-increasing integration and joint working between different organisations to deliver better care and value for patients and the taxpayer. To meet this challenge, the way that NHS services are delivered needs to change – to improve the quality of care and health outcomes for populations, reduce health inequalities, enhance productivity and value for money, support broader social and economic development and improve the experience for patients.
8. Some of these changes have been happening for some time – including from their experience of responding to the COVID-19 pandemic – organisations across the NHS (and with local authorities) are implementing collaborative arrangements across a variety of However, some arrangements rely heavily on goodwill and/or the adoption of complex workarounds, as organisations have been legally constrained in the extent to which they can work together across their functions.
9. NHS England has recommended Parliament make a number of legislative changes to support integration of care. These give organisations more flexibility to work together to improve people’s health and wellbeing and reduce health inequalities. The intent of the 2022 Act – and the sections to which this guidance relates – is to make collaborative working between those involved in planning, purchasing and delivering care easier at a national, system level and place level, as well as accelerating progress in meeting our most critical health and care challenges.
Overview of relevant legislative changes
10. The 2022 Act introduces new sections 65Z5-65Z7 to the 2006 Act. These changes will give organisations greater flexibility to collaborate in exercising their statutory functions, either through delegation or joint exercise of those functions – enabling better integration of their services to improve outcomes for patients, and facilitating the best use of resources across care pathways at system and place level.
11. Section 65Z5 of the 2022 Act provides new powers for statutory NHS It creates a defined list of relevant bodies, which are:
- NHS England
- Integrated care boards (ICBs)
- NHS trusts, and
- NHS foundation
12. The section allows those relevant bodies to delegate their functions to each other, and to local authorities (LAs) and combined authorities (CAs). It also allows the Department of Health and Social Care (DHSC) to set out in regulations other organisations that may in the future become a relevant body.
13. Section 65Z5 also enables these relevant bodies to jointly exercise their functions with each other and/or with LAs and CAs; and to form joint committees and pool funds to do so (under s65Z6). However, these relevant bodies cannot use these provisions to delegate to, or form joint exercise arrangements with, any organisations other than those within the scope of s65Z5.
14. LAs and CAs are not defined as relevant bodies in s65Z5, and therefore cannot enter into collaborative arrangements using that provision in respect of their own functions. Instead, they should continue to use existing provisions in s75 of the 2006 Act and the associated partnership arrangements regulations for any delegation/joint exercise of health-related LA or CA functions to/with health See Annex C for more information on s75 partnership arrangements.
15. The legislation allows significant flexibilities, but it does not specify circumstances where organisations should delegate or jointly exercise any particular function – it is for the relevant bodies to decide how they exercise their own functions. However, the new flexibilities are not completely unfettered. The 2022 Regulations set out certain restrictions. In addition, some functions should not be delegated as they are central to the governance of relevant bodies and therefore should remain under its direct control. The hold on ICB to provider delegation – as set out in Annex G – does not apply specifically to delegation to local authorities. However, the use of the ICB powers to delegate to local authorities should be considered alongside rather than separately from Section 75 partnership arrangements, and within the scope of s75 restrictions.
16. The ‘2022 Regulations’, made under s65Z5, set out functions that are excluded from the scope of the powers in sections 65Z5 and 65Z6. This statutory guidance – published under section 65Z7 – also recommends some limits (and explains some other legal requirements) that safeguard the proper use of the new powers. This guidance should also be read alongside existing requirements elsewhere in law and guidance (eg around good governance).
17. The 2022 Act also inserts a new provision into s12ZA of the 2006 Act, in relation to arrangements made by NHS England and ICBs with NHS providers (NHS trusts and foundation trusts) for their delivery of services. The new power sets out that such arrangements ‘may confer discretions on a person with whom they are made in relation to anything to be provided under the arrangements’. The intention of this power is to confirm that NHS providers may lawfully take on wider population health activities relating to their contracted provision of services, for example. ‘Conferral of discretions’ is not a mechanism to achieve delegation – but it allows arrangements with providers to include identifying and deciding the services necessary to meet the needs of the population, within the scope afforded by the relevant contract, rather than just the logistics of service delivery. Therefore, commissioners and providers may wish to consider whether a contract conferring additional discretions on a provider is a suitable alternative to, or potential stepping-stone towards, the delegation of a function.
18. Any decisions by NHS organisations about delegation and joint exercise of functions should ensure alignment with the integrated care strategies developed by integrated care partnerships, joint health and wellbeing strategies, the five year joint forward plans of ICBs and partner trusts/foundation trusts, related system plans and other relevant national policy documents, including:
- Statutory guidance to integrated care boards on the preparation of constitutions
- Guidance on functions and governance
- Guidance on financial frameworks and contracting
- Guidance on provider collaboratives,
- Guidance on joint forward plans and the Better Care Fund
- Care Quality Commission of regulated services
- National framework for continuing healthcare and funded nursing care and
- The National Quality Board guidance on System Quality Groups
Future mechanisms for collaborative arrangements
19. All statutory NHS bodies have functions (duties and powers) conferred on them by legislation, which define their obligatory and permitted activities – a statutory body may only do what legislation requires or allows it to do. For example, NHS England has a range of regulatory, oversight and commissioning functions defined by statute.
20. Therefore, relevant bodies within the scope of the new s65Z5 powers will have three options for ‘exercising’ (carrying out) their functions under the new legislation. They will be able to:
- carry the function out themselves, on their own as they have been able to do previously – including through ‘internal’ delegations to individuals and committees
- delegate responsibility to one or more organisations to carry out functions on their behalf, and/or
- carry out their functions jointly (jointly exercise) with one or more other organisations, potentially by forming joint committees and pooling funds to do
21. Annexes A and B give more detail on the different ways for organisations to delegate and jointly exercise their functions – including who is able to make decisions about functions, between (and within) organisations.
22. The 2022 Act provides more flexibility for different NHS bodies to come together to carry out their functions, and to delegate their responsibility for making decisions. Further, this collaboration could be at any level – nationally, regionally, system or place – and relate to individual services or broad categories, such as services for older people.
23. This increased flexibility means that NHS organisations need to consider carefully what they want to achieve and how – taking into account the integrated care strategy produced by the integrated care partnership (ICP) and when they and their partners will be ready to do so – not least because they will likely have more than one way to achieve their objectives in future. For example, although organisations could set up a joint committee arrangement under the new s65Z6 so that partners can collectively make decisions at place level, they might better achieve their aim by an internal delegation of their decision to a place-level committee of the ICB.
24. The use of these new powers can lead to a step change in the way that organisations’ arrangements are planned and delivered making it easier to drive rapid and sustained improvements of care, so they better meet the health needs of local populations. However, arrangements for the delegation and joint exercise of functions will have a significant impact on the governance of the organisations involved in those arrangements.
25. Organisations must therefore carefully consider the potential benefits from collaboration – taking into account the duty of cooperation and, for ICBs, the duty to promote integration and how they can be continually assured that these benefits are being realised; and how all organisations recognise that the models of collaboration best suited to local circumstances may change over time – before they enter into such arrangements.
26. All organisations involved in these collaborative arrangements should fully prepare for the changes in responsibility and resource – including by working with partners to set clear objectives and a strategy, so that they can determine which mechanism would be most appropriate for delivery; and by ensuring proper governance arrangements are in place to assure their agreed delegation/joint exercise model.
Summary of mechanisms
27. Table 1 below summarises the key legislative mechanisms that will enable collaborative working across organisations in future – further details are given in Annexes A to C.
Table 1: Key legislative mechanisms for collaborative working
| Mechanism for collaboration | Organisations whose functions are involved | Description of mechanism |
|---|---|---|
| Section 65Z5 delegation (see Annex A) |
NHS England, ICBs, NHS trusts and foundation trusts | This is a voluntary arrangement whereby NHS organisations listed under s65Z5 delegate responsibility for carrying out specific functions to other listed NHS organisations and/or to LAs and/or to CAs. There are some constraints on what functions can be delegated and how these delegations are made, which are set out in the 2022 Regulations and in Annex E and G of this statutory guidance.NHS organisations cannot delegate their functions to non- statutory, non-public organisations (that is, independent or voluntary sector providers). LAs and CAs cannot delegate their functions to statutory NHS organisations using this mechanism – although they can receive delegated responsibility for the functions of NHS organisations under s65Z5 arrangements. For delegation of LA functions, see s75 arrangements below. |
| Sections 65Z5 and 65Z6 joint exercise arrangements (see Annex B) |
NHS England, ICBs, NHS trusts and foundation trusts | Two or more NHS organisations within the scope of s65Z5 can choose to come together (including via a joint committee) to make legally-binding decisions and pool funds across agreed functions. Any constraints on how these arrangements are made and which functions can be part of them are set out in the 2022 Regulations and in Annex E and G of this statutory guidance.LAs and CAs can be part of these arrangements – but they cannot include their own functions in any joint decision- making using this mechanism. Joint working between LAs and NHS organisations, including for LA functions, can be achieved using s75 and s65Z5 arrangements. |
| Section 75 partnership arrangements (see Annex C) |
NHS England and/or ICBs with LAs and/or CAs NHS trusts and/or foundation trusts with LAs and/or CAs |
Section 75 partnership arrangements are a longstanding collaboration mechanism under the 2006 Act. These enable collaborative working between at least one NHS organisation (NHS England/ICB or NHS trust/foundation trust) and at least one LA to exercise or delegate a range of the NHS organisation’s functions and the LA’s health-related functions. Any delegation/joint exercise of health-related LA functions to/with NHS organisations will continue to be achieved using the powers in s75 of the 2006 Act and the associated partnership arrangement regulations. The 2022 Act requires ICPs to consider the use of section 75 arrangements in preparing their strategy for their system. |
| Trust joint working arrangements |
NHS trusts and foundation trusts |
FTs and NHS trusts have their own powers to exercise their functions jointly with other bodies. If a Trust agrees to exercise functions jointly with another Trust and they want to exercise functions through a joint committee, they can use s65Z6 arrangements to set up the committee. |
| Conferral of discretions
|
NHS England, ICBs, NHS trusts and foundation trusts |
This provision has been included to make clear the lawful scope of contractual arrangements between commissioners and providers. It confirms that a commissioner can lawfully give providers a wide degree of latitude as to the services they provide under a contract, both in terms of which services are delivered and how they are delivered, so as to resolve any doubt on this issue. The commissioner will still set the broad scope of what the provider is expected to achieve (clinical outcomes, for example) under a contract. A contract that confers discretion on a provider in respect of some or all services under the contract may be a useful alternative or precursor to delegation to trusts or foundation trusts under s65Z6. |
28. Organisations may find the flowcharts in Annex D helpful when considering adopting delegation arrangements in respect of their functions. These flowcharts are not an exhaustive statement of what could be achieved but an example of how a delegation arrangement could be considered.
Managing conflicts
29. An issue that will arise – particularly initially in both delegation and joint working arrangements with ICBs – is the effective management of conflicts. The guiding principle for NHS organisations in dealing with these conflicts will be that decisions must be made in the public interest, avoiding any undue influence from other interests. Our Guidance to Clinical Commissioning Groups on the ICB Constitution sets out seven principles for the safe and effective management of conflicts of interest in ICBs. The significant NHS provider involvement within each ICB’s membership will require any conflicts of interest to be assessed on a case-by-case basis, in line with these principles.
30. Under s65Z5, delegation and joint exercise of functions arrangements can only be made between relevant bodies, LAs and/or CAs. NHS organisations convening joint committees will be able to determine the membership of committees – which organisations are represented and on what basis. Committees could include individuals who are not employees of the ‘convening organisations’. For example, the joint committee could include a clinician who has expertise relevant to matters delegated to the committee but who is not an employee of any of the bodies participating in the joint committee. As with any internal committees of an ICB, a joint committee should ensure the appropriate management of conflicts of interest relating to any of its members.
31. For example, an individual from a social enterprise that provides mental health services may give a reasoned and evidence-based opinion that a certain type of online therapy is better for supporting people who experience anxiety – but it might also be that the social enterprise is currently the only provider of that service in the ICS footprint. This should not mean that individual’s contribution is discounted – but their conflicting interests should be recognised and taken into account when considering the final decision.
32. FAQs for chairs have been published which clarify the role of individuals (including those from non-statutory providers) in these joint exercise arrangements. This will reiterate the seven principles of public life – as they are as relevant to the good governance of any collaborative arrangements as to decisions within ICBs.
Options for collaborative arrangements
33. The new legal flexibilities, associated regulations and statutory guidance came into force on 1 July 2022. Additional restrictions on the use of those powers to delegate Continuing Health Care Functions of ICBs came into force on 10 April 2023.
Arrangements between NHS England and ICBs
34. NHS England previously had the power to delegate functions to clinical commissioning groups (CCGs), and used it successfully to delegate the commissioning of primary medical services (PMS).
35. Building on this approach, delegated responsibility for PMS shifted from CCGs to ICBs at the point when ICBs became statutory bodies. NHS England also delegated arranging primary dental services, primary ophthalmic services and pharmaceutical services to some ICBs on 1 July All ICBs took on these functions by 1 April 2023, although some took them on earlier.
36. In addition, as approved by NHS England’s board on 7 December 2023, NHS England will delegate 59 specialised services plus others to ICBs on 1 April 2024 for some regions and from April 2025 in the remaining regions.
37. Further guidance relating to delegation to integrated care boards is set out in Annex E and G.
Arrangements between ICBs
38. ICBs will have powers to delegate functions to other ICBs and make decisions jointly. This could be across bigger population footprints (that is, covering multiple ICBs) or at place-level across their ICB footprint; and will enable those ICBs with particular expertise in service of specialty to take the lead in making arrangements on behalf of other ICBs.
39. For example, it may be that an ICB determines that the best option for arranging ambulance services for its population is to delegate this responsibility to another ICB, through a lead commissioner arrangement – that is, the first ICB delegates responsibility to the second ICB to arrange the provision and contract for ambulance services on its behalf.
40. In deciding the form of any future arrangements, ICBs should consider the following questions:
- Is working together (at scale, place, or on behalf of the other) likely to have a positive impact on the health and wellbeing of the population; support improvements in quality; and/or improve efficiency and sustainability whilst protecting quality of care in the use of NHS resources (in line with their new triple aim duty)?
- Does establishing a pooled fund enable a more flexible use of resource?
- Does one of the ICBs in the arrangement have a workforce with particular capacity, skills and experience in the area of commissioning concerned?
41. If ICBs decide to use s65Z5 powers, they must have processes to provide ongoing assurance that the arrangement is effective.
42. Further guidance relating to arrangements between integrated care boards is set out in Annex E and G.
Arrangements between NHS providers, and with NHS England and ICBs
43. The legislative changes will create a new way for statutory NHS providers (that is, NHS trusts and foundation trusts) to work together, and/or with NHS England and ICBs – either by delegating responsibility for functions to, or jointly exercising functions with, each other. See Annexes A and B for more details.
44. For example:
- NHS trusts and foundation trusts that want to collaborate will be able to use delegation to reinforce existing lead provider arrangements and other collaborative models – if they so choose.
- Provider collaboratives may decide that they want to use s65Z6 joint committee arrangements to agree plans and carry out their cross-population delivery.
- NHS providers may choose to replace their ‘committees-in-common’ arrangements to work together in joint committees at system or place
45. These powers also allow NHS England and ICBs to delegate their functions to statutory NHS providers. This kind of delegation is new, and its use should be carefully targeted to situations where there is a clear rationale for allowing individual (or groups of) statutory NHS providers to carry out certain NHS England or ICB commissioning functions – that is, where (and when) the organisations involved feel that this approach best serves their population needs, and best enables the system to meet its objectives (see Annex E).
46. As set out in Annex G, NHS England recommends a hold on use of these powers, and expects ICBs not to delegate to NHS providers in 2024/25, but the following information is provided to assist systems who may want to consider such arrangements in future.
47. In some circumstances, an ICB may want to work with an NHS provider or group of NHS providers to allow these provider(s) to take on responsibility for commissioning/arranging (exercise of ICB’s functions) a range of services in addition to providing services they are contracted for. It is important to note that under such an arrangement, a provider cannot be responsible for both arranging and providing the same services. We also do not recommend that a provider is formally delegated ICB responsibility for determining population needs in relation to particular services where that provider intends to seek selection as the provider of those services, as this could create a conflict of interest.
48. In these cases, the ICB would need to have both an agreement in place that sets out the terms of delegation for the services to be commissioned, including any scope for onward delegation, and a separate contract covering the services the provider was to deliver itself. This would need to comply with the provider selection rules to ensure provider(s) are selected to deliver services fairly and lawfully. All contracts for healthcare services should be awarded by following the new NHS Provider Selection Regime (PSR), irrespective of whether any delegation of functions takes place.
49. If an ICB wants an NHS provider to be responsible for certain services, but have discretion as to whether it provides those services itself or contracts with a third party to do so, that can be delivered through existing contracting and sub-contracting arrangements (as in lead provider arrangements).
50. Section 65Z5 arrangements are voluntary, so organisations can choose whether and how to use them. As NHS providers have not had responsibility for specific commissioning functions before, it may take some time to establish a strong rationale and basis (capacity and capability) for such delegation. Systems will need to undertake substantial strategic planning and preparatory work to gain assurance that all parties are fully prepared, before delegating such functions.
51. If in future an ICB agrees to delegate certain function(s) to one or more NHS provider(s), it would need to set out the governance for the s65Z5 arrangement in advance, through a delegation agreement – which may form part of a contract for the relevant services with the provider. The s65Z5 arrangement must be reflected in:
- ICB and individual providers’ governance documentation (eg their scheme of reservation and delegation, and functions and decisions map). This includes setting out governance arrangements where two or more NHS providers will jointly exercise any ICB-delegated function(s), and
- the provider’s service contracts, where the provider will also deliver aspects of the service for which it has delegated responsibility.
52. The statutory duties which apply to ICBs when commissioning – including those under the Standing Rules, such as the duties to use the NHS standard contract and those relating to patient choice waiting times, and compliance with the NHS Payment Scheme – will extend to NHS providers when they are exercising delegated commissioning functions. ICBs should ensure that delegation agreements make it explicit that the NHS provider must comply with those duties.
53. To build capability in the system as an interim step to delegation (or even as an end-point in itself), ICBs could award to or vary a contract with an NHS provider or contracts to or with a number of NHS providers, either during the annual contracting round or in year, under which they could choose to give the provider or providers latitude to develop and delivery service models at their discretion, to meet outcomes or objectives specified by the ICB by a conferral of discretion (using the power to confer discretion in contracts with providers).
54. Further guidance relating to delegation to providers is set out in Annex E and G.
Arrangements involving local and combined authority functions
55. Under new s65Z5, relevant bodies (NHS England, ICBs, NHS trusts and foundation trusts) will be able to delegate to, or exercise their statutory functions jointly with, LAs and/or CAs.
56. However, as LAs and CAs are not relevant bodies, they cannot make arrangements under s65Z5 in respect of their own functions. If an LA or CA intends to jointly exercise health-related LA or CA functions with health bodies – eg commissioning or provision of sexual health service – it will need to do this using the powers in s75 of the 2006 Act and the associated partnership regulations.
57. Section 75 partnership arrangements are a longstanding and widely-used mechanism to support key integration initiatives such as the Better Care Fund. However, there are limits on the scope of the health (or health-related) functions that NHS organisations and local authorities can include in s75 partnership arrangements – see Annex C for further details. In addition, the s75 regulations impose a requirement that organisations must ensure that they can demonstrate this arrangement is ‘likely to lead to an improvement in the way that those functions are exercised’.
58. The new provisions under the 2022 Act, used in combination with current s75 partnerships arrangements with LAs, could consolidate arrangements for collaboration between NHS bodies and LAs. For example, for LA functions to effectively be part of an s65Z5 joint committee arrangement and for LAs to be part of decision-making requires an s75 partnership arrangement to be used, with:
- the LA delegating its functions within the scope of the s75 regulations to an NHS body, via an s75 partnership arrangement
- that NHS body then forming a joint committee with the LA (and potentially other relevant bodies) to exercise the function jointly.
59. If using the s65Z5 and s75 arrangements in this way, partner organisations must ensure the governance and oversight arrangements are clear – including demonstrating that the arrangements improve delivery of the function.
60 .Section 65Z5 should not be used as a tool to circumvent the constraints in the section 75 partnership regulations, to jointly exercise functions that are currently excluded.
Annex A – delegation and joint exercise
Different ways of delegating functions
61. There are three ways in which statutory bodies can delegate authority for making decisions about the exercise of their functions:
Internal organisational delegation
62. By default, overall responsibility for exercising most functions conferred on a statutory body usually rests with the board of that organisation. Some functions are conferred by legislation directly, for example, on a chief executive or remuneration committee, but this is the exception rather than the norm.
63. In accordance with the organisation’s scheme of delegation, decision-making for functions not reserved to the board can be ‘delegated’ to committees and sub- committees of the organisation established by the board, or to individuals (board members or employees) – giving them the delegated authority to exercise their organisation’s functions. For example, the Chief Finance Officer of NHS England has delegated authority to approve and sign certain contracts made by NHS England.
Delegation to other organisations
64. This situation is where one statutory body delegates responsibility for the exercise of any of its functions to another statutory The terms of this voluntary shift of responsibility are set out in a delegation agreement; which will need to be ratified by each organisation’s decision-makers (usually their boards), and reflected in their individual governance arrangements. For example, in recent years NHS England has used an existing mechanism under earlier legislation to delegate the arranging of primary medical services to CCGs, and has carried this forward with ICBs, using the powers in s65Z5.
65. Lead commissioner arrangements are also a form of this (external) delegation – one or more organisations delegate a function to another organisation to carry out, usually together with the recipient organisation’s own function. For example, a group of ICBs may wish to delegate arranging ambulance services to one ICB on their collective behalf. This will still be possible under the new legislative provisions.
Exercising functions jointly with other organisations
66. Two or more organisations (that is, relevant bodies, LAs and CAs) can come together to make joint decisions about functions of one or more of the relevant bodies. Although each organisation continues to have accountability and responsibility for the exercise of its delegated functions, it shares that responsibility with others. Therefore, as for delegation, the terms of the arrangement need to be set out, ratified by boards and reflected in the individual organisations’ governance arrangements. Joint working arrangements are often managed through the formation of a joint committee (see Annex B). The joint committee exercises the functions on the bodies’ behalf, and any decision is owned jointly by the convening member organisations.
67. This collective responsibility can be either an end in itself (eg an ICB and an NHS provider running a joint patient engagement consultation exercise) or a step to a full external delegation of a function (eg NHS England and some CCGs jointly exercised primary medical care functions before CCGs assumed full delegated responsibility for those functions).
Responsibility, accountability and liability in delegation and joint exercise arrangements
68. Three related but distinct concepts should be considered separately in the context of delegation to other organisations or joint exercise of functions. For the purposes of this document, they can be defined as follows:
- Responsibility – the obligation to carry out some or all aspects of a statutory function.
- Accountability – the obligation to explain how functions are being carried out, either by the organisation on which the function was initially conferred by legislation or by another organisation under a delegation or joint working arrangement, along with the obligation to ensure that any deficiencies are being addressed.
- Liability – the obligation to bear the legal consequences that result from a failure to carry out tasks within an organisation’s area of responsibility, or a failure to carry them out properly.
69. Accountability typically concerns being subject to arrangements for political or administrative oversight, whether locally such as by local authority health overview and scrutiny committees or nationally such as by NHS England, the Department of Health and Social Care, the Health Service Ombudsman or the National Audit
70. Liability is about responding to legal proceedings such as appeals or applications for judicial review. A party that is held liable must provide the remedy that is ordered by the court or Disputes that could result in legal proceedings, but which are settled by the parties, are within the scope of liability for the purposes of this document.
71. When an organisation simply exercises its own functions, then responsibility, accountability and liability are all held by that organisation. When arrangements for delegation to other organisations or joint exercise of functions are made, some of these may shift to, or be shared with, other organisations within the arrangement. These implications should be thought through when making arrangements and accounted for within agreements between the parties.
Delegating responsibility to another organisation
72. Under the new s65Z5, relevant bodies will be able to delegate their statutory functions to other relevant bodies, and to LAs and/or CAs – that is, make arrangements for one or more other relevant bodies to exercise (carry out) that function.
7.3 This enables organisations to take on delegated responsibility (individually or collectively) for functions that are not directly conferred on them by statute – but with a clear line of accountability between the organisation(s) exercising the delegated function and the one delegating it.
74. Following approval by each organisation’s board (or nominated decision-maker) and any relevant changes to each organisation’s governance arrangements (eg their schemes of delegation or constitutions), carrying out the function then becomes the responsibility of the recipient organisation; and they will bear any liabilities related to carrying out the functions. The ultimate accountability, including any potential liability for unlawful delegation for the function, remains with the delegating organisation.
75. The recipient organisation is operationally and legally responsible and liable for carrying out the function, for as long as both parties choose to sustain the agreement. It can take decisions about the exercise of the function without the day-to-day involvement of the delegating organisation – within the parameters set by legislation, statutory guidance and the terms of the delegation agreement.
76. For example:
- An NHS organisation determines that the best option for arranging services for its population is to delegate authority for securing community services to one of its place-based committees that has LA members. This could be achieved by an internal delegation within the ICB – but equally could be an s75 partnership arrangement, or
- NHS England and the ICBs agree that the ICBs should be responsible for NHS England’s direct commissioning of PMS. Subject to any requirements in their delegation agreement, ICBs can take decisions without needing sign-off from NHS England to do so. Therefore, ICBs are responsible for arranging the delivery of PMS, but to fulfil its statutory accountability NHS England must ensure it has appropriate oversight of the ICBs’ activity.
Delegation of NHS England functions to ICBs or NHS providers
77. To enable ICBs to commission end to end integrated services for their populations, NHS England has chosen to delegate some of its direct commissioning functions to and/or jointly exercise them with ICBs and other specified statutory bodies. There is currently a hold on ICBs delegating these functions further to NHS providers (see Annex G).
78. NHS England is also able to delegate its functions, including those related to arranging services, to NHS providers (NHS trusts and foundation trusts). As with ICB delegation, this enables NHS providers to take on legal responsibility both for making the arrangements for and delivering services. If NHS England were to do so, the same conditions and considerations would apply as where ICBs decide to delegate to providers – including any contractual arrangements and considerations of certain risks and duties (see Annex G).
79. The powers under s.65Z5 will allow the allocation of roles and responsibilities between NHS England and NHS providers to be flexibly applied giving NHS providers the scope to innovate and develop services to meet identified patient needs, and the formal responsibility for commissioning of services that is currently not permitted.
80. Table 1 of Annex D sets out a decision map for how NHS England might decide to delegate its functions.
Delegation of ICB functions to NHS providers
81. ICBs have the power to delegate their functions to NHS providers. NHS England’s position is that these powers should not be used for 2024/25 (see paragraphs 45-53, and Annex G).
82. In the future, in some circumstances an ICB may also want a provider or group of providers to take on commissioning functions for a type of service, while at the same time agreeing that the provider will deliver some aspects of the services themselves or will have discretion to decide to deliver some of the services themselves.
83. For example, an ICB may decide that it wants to give a trust discretion to design and implement services in which it has particular expertise, such as a range of mental health services. In the case of those services the ICB would adopt mutually agreed arrangements or outcomes- based approach to service specifications, oversight and assurance. An ICB may want to do this through a provider contract and the use of the power to confer discretion on a provider of services – and perhaps at a later date to go further and delegate responsibility for commissioning those services. Other services under the contract could be specified in greater detail by the ICB and be subject to a greater degree of input-based specification and oversight.
84. If in future an ICB wants an NHS provider to deliver a service while also exercising delegated functions related to it, it will need to ensure it selects the provider(s) in line with the relevant procurement and contracting rules to ensure the provider(s) is selected to deliver services fairly and lawfully. The delegation of a function cannot be used to circumvent the rules for provider selection, and delegation is not an alternative to contracting for the provision of healthcare services. ICBs must follow the NHS provider selection regime rules for selecting providers once this comes into force (and before that point, comply with current public procurement law). They will also need to award contracts to the selected provider(s) using the conditions and terms of the NHS Standard Contract or a primary care contract as appropriate to the commissioned service.
85. In these cases, the ICB would need to have an agreement(s) in place that sets out both the terms of delegation and the terms under which the provider would deliver some of the services or exercise discretion to deliver some services.
86. Table 2 of Annex D maps out how an ICB might decide the best mechanism for collaborative working.
87. NHS England will work with ICBs and NHS providers to provide further support to develop details on how such arrangements could be implemented.
Delegation of NHS provider functions to other NHS providers
88. NHS providers (NHS trusts and foundation trusts) play a central role in collaborative working; for example, by working together in provider collaboratives, (whether to deliver clinical services or to deliver or purchase support functions), or by pooling monies with LAs to deliver prevention programmes or delayed transfer of care reduction programmes through s75 partnership arrangements.
89. In future, they will be able to work together and with ICBs, at both place and system level, in a way that was not possible previously. The new powers in s65Z5 give a statutory basis for collaborative working – offering NHS providers the scope they need to work together to innovate and integrate service delivery. These allow the establishment of a joint committee of NHS providers to manage the exercise of certain functions, or the formation of lead provider arrangements to exercise functions on behalf of other NHS providers. For example, a joint committee of NHS providers could provide a governance framework for the management of networked clinical services in support of the delivery of vulnerable services, or a group could choose to create a centre of excellence for procurement, hosted by one of the trusts which is given delegated powers to purchase goods and services on behalf of all.
90. There is no one-size fits all approach. NHS providers currently work together in a variety of other ways – for example provider collaboratives – including different mechanisms to form provider collaboratives and alliance agreements. So, it is important that organisations adopt the provider configuration that best delivers their system objectives.
91. Table 3 of Annex D sets out how an NHS provider might delegate its functions.
Annex B – joint working arrangements
92. Under the new s65Z5, relevant bodies are able to jointly exercise their statutory functions with other relevant bodies, and with LAs and/or CAs – that is, make formal decisions collectively about functions in scope of their joint working arrangements.
93. The new s65Z6 also allows relevant bodies to do so in a joint committee arrangement, and to pool funds.
94. As LAs and CAs are not relevant bodies for the purposes of these new legal provisions, they cannot make arrangements under s65Z5 in respect of their own functions – s65Z5 is a means of involving LAs and CAs in the exercise of NHS functions. Any joint exercise of health-related LA or CA functions with health bodies will continue to be achieved using the powers in s75 of the 2006 Act and the associated partnership regulations (see Annex C).
95. Although LAs cannot use the new provisions to delegate to or jointly exercise their own functions with NHS bodies directly, they can use the powers in s65Z5 in combination with current s75 partnership arrangements to create joint working arrangements between NHS bodies and LAs. This would require the following steps:
- The LA delegates its function within the scope of the s75 regulations to an NHS body, via an s75 partnership arrangement.
- The NHS body then forms a joint committee with relevant bodies – including the LA – to jointly exercise the function.
Joint committees
96. A joint committee provides a statutory basis for a group of NHS organisations to take collective responsibility for one or more of their statutory functions – enabling joint decision-making and risk-sharing approaches (including to financial management), whilst creating more transparency and clarity of accountability when organisations work together as systems. Organisations may also choose to pool funds across these functions, and manage the pooled spend through the joint committee. For example, ICBs and NHS providers may want to form a joint committee at place level to redesign a particular service, or to manage shared corporate services and the pooled fund that resources them.
97. Constituent organisations of a joint committee agree to abide by the decisions made jointly on a range of issues. These constituent organisations will determine the committee’s scope of work and governance arrangements – including setting out criteria, standards, principles or success measures to which the committee operates; and deciding how and when they will review the committee’s performance in respect of these.
98. NHS organisations convening joint committees will be able to determine the membership of committees – which organisations are represented and on what basis. Committees could include individuals who are not employees of the ‘convening organisations’. For example, the joint committee could include a clinician who has expertise relevant to matters delegated to the committee but who is not an employee of any of the bodies participating in the joint committee. As with any internal committees of an ICB, a joint committee should ensure the appropriate management of conflicts of interest relating to any of its members.
99. As with any NHS statutory body, joint committees will therefore need to adopt clear governance arrangements for making decisions, differentiating between those individuals who should be involved in the final, formal decision-making and those who contribute to committee discussions about, for example, service design that lead to that decision. These arrangements, and their application in particular instances, should be clearly documented.
Committees-in-common (CIC) arrangements
100. Although CIC arrangements are already used in the NHS as a governance mechanism for collaboration between organisations, the detail of how these arrangements work can vary from one case to another. In essence, they create a framework for aligned decision-making – they are an arrangement that promotes consistent decisions about the exercise of functions by all participant organisations, though those decisions are separately taken.
101. To form a CIC, each organisation in the arrangement delegates its decision- making for a particular function to an internal committee of that organisation. The committees of each of the organisations may have common membership, either entirely or in part hence the name ‘committees in common’. Individual committees then make decisions for their organisations – essentially simultaneously and following arrangements that maximise the chances of aligned decision making between the different organisations.
102. This mechanism has been used to good effect in the past for CCGs. However, it has limitations – it is not the same as making one binding decision on behalf of all the organisations involved; and requires careful governance of the decision- making process to ensure that the decision of each organisation’s committee is in line with its internal governance processes.
103. It is also possible for both NHS trusts and foundation trusts to establish CIC arrangements. For NHS trusts, their schemes of reservation and delegation allow delegation of decision-making to internal committees consisting wholly or partly of their directors, or wholly of people who are not directors of the trust. This means they can easily include members from other NHS trusts and foundation trusts.
104. However, legislation governing NHS foundation trusts only allows them to delegate their authority to make decisions about their functions to a committee of their directors or an executive director. This means that CIC arrangements between NHS foundation trusts (or with NHS trusts) often require directors to be jointly appointed across the NHS providers concerned, to achieve the necessary membership.
105. CICs do not provide a basis for delegating to other organisations – for example, in lead commissioning/provider arrangements; or in joint exercise of functions, and the associated establishment and maintenance of pooled funds. However, such arrangements can be useful as a precursor to adopting joint committee arrangements and/or in creating a decision forum for provider collaboratives.
Pooled funds
106. The 2022 Act provides a new mechanism for pooling funds to support collaboration arrangements, through s65Z6.
107. A pooled fund is a budget comprising contributions from one or more organisations in a joint working arrangement, which can be spent on activity/expenditure relating to the organisations’ joint responsibility for functions in scope of these arrangements.
108. The objective for pooling budgets is to apply resources more flexibly, improving services and outcomes for patients. This has been done in the NHS for a number of years – for example, the 2006 Act and previous legislation provides for the ability to pool budgets under an s75 partnership arrangement between NHS organisations and local authorities.
109. A pooled fund can be managed by one or more of the organisations, or by a joint committee (if they have established one for that purpose). Organisations in joint working arrangements that want to pool funds should ensure they specify what the pooled fund covers, who contributes to it and how decisions to spend it are made.
110. Where a pooled fund is created, there should be a written agreement covering matters including:
- the precise scope of functions to which the pooled fund relates
- the agreed contributions of each organisation, along with arrangements for dealing with overspends and underspends
- which organisation will host the pooled fund
- how payments from the pooled fund can be authorised
- reporting requirements to the organisations involved
- provisions allowing for the arrangements to be discontinued in an orderly way if necessary.
Annex C – section 75 partnership arrangements
111. Partnership arrangements made under s75 of the 2006 Act enable at least one NHS statutory body (ICBs/NHS England or NHS trusts/foundation trusts) and LAs to collaborate across a range of the LA health-related functions and NHS health functions as prescribed within the regulations. This includes creating a joint committee to manage the arrangement, and pooling funds to cover relevant expenditure. These arrangements should take into consideration the integrated care strategy which requires the integrated care partnership to consider the use of section 75 arrangements in preparing their strategy for their system.
112. Joint planning and commissioning of services enables the health and social care needs of the population to be taken into account simultaneously. Section 75 partnership arrangements allow health and social care commissioners to take decisions in a collaborative way and ensure that both parties implement the decisions taken. These arrangements help ensure that timely decisions are taken and avoid some of the bureaucracy that can be associated with other approaches.
113. Parties planning to enter into s75 arrangements must be able to demonstrate that the arrangements are likely to lead to an improvement in the way functions in the arrangement (both NHS and health-related LA) are exercised. In addition, the parties may only enter into the s75 arrangements if they have jointly consulted those ‘who appear to them to be affected by the arrangements’. The requirement to consult does not apply to s75 arrangements entered into for the purposes of the Better Care Fund.
114. Section 75 partnership arrangements allow a range of ICB or NHS provider health functions to be exercised collaboratively with health-related LA functions. However, the following NHS services are excluded from s75 arrangements:
- surgery, radiotherapy, termination of pregnancies, endoscopy, the use of Class 4 laser treatments and other invasive treatments
- s7A public health services
- primary dental services
- pharmaceutical services
- primary ophthalmic services
- emergency ambulance services.
Governance of s75 arrangements
115. Many s75 arrangements tend to be lead commissioner or lead provider arrangements – although they can also support joint working.
116. Whatever the configuration, s75 arrangements should be documented in a written agreement that details the precise scope of the functions to be exercised; that is, by the lead organisation. Partners in the arrangement should seek regular assurance that each one has the appropriate capabilities and resources to carry out the function effectively. This may include providing regular reports and management information to the partners.
117. Section 75 arrangements allow for the creation of a pooled fund. If organisations decide that this is something they want to use they should use the guidance at paragraph 111 above to ensure proper governance and management of that fund.
118. Section 65Z5 should not be used as a tool to circumvent the constraints in the section 75 partnership regulations, to jointly exercise functions that are currently excluded.
Annex D – flowcharts for delegation arrangements
Figure 1: NHS England functions – when to use delegation arrangements under s.65Z5
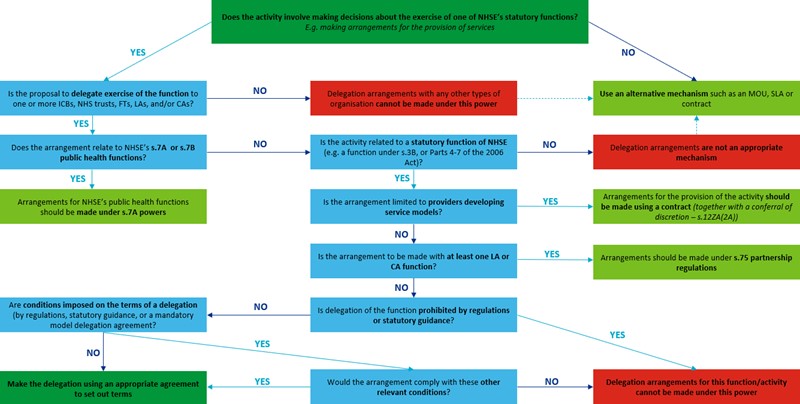
Note: this flow chart:
- Should be used when NHS England wants another organization to carry out activities that it would otherwise carry out itself
- Assumes that primary care transfer provisions have not been commenced
- References sections to the NHS Act 2006, as amended by the Health and Care Act 2022
- Is not an exhaustive statement of what can be achieved under s.65Z5
Image text: Top of the flowchart begins with the question:
Does the activity involve making decisions about the exercise of one of NHS England’s statutory functions? E.g. making arrangements for the provision of services
1. If ‘Yes’, then is the proposal to delegate exercise of the function to one or more ICBs, NHS trusts, FTs, LAs, and/or CAs?
If ‘Yes’ then does the arrangement relate to NHS England’s s.7A or s.7B public health functions?
If ‘Yes’ then agreements for NHS England’s public health functions should be made under s.7A powers.
If ‘No’ then is the activity related to a statutory function of NHS England (e.g. a function under s.3B, or Parts 4-7 of the 2006 Act)?
If ‘Yes’ then is the arrangement limited to providers developing service models?
If ‘Yes’ then arrangements for the provision of the activity should be made using a contract together with a conferral of discretion – s.12ZA(2A)).
If ‘No’ then is the arrangement to be made with at least on LA or CA?
If ‘Yes’ then arrangements should be made under s.75 partnership regulations.
If ‘No’ then is delegation of the function prohibited by regulations or statutory guidance?
If ‘Yes’ then delegation arrangements for this function/activity cannot be made under this power.
If ‘No’ then are conditions imposed on the terms of a delegation (by regulations, statutory guidance, or a mandatory model delegation agreement?
If ‘Yes’ then would the arrangement comply with these other relevant conditions?
If ‘Yes’ then make the delegation using an appropriate agreement to set out terms.
If ‘No’ then delegation arrangements for this function/activity cannot be made under this power.
If ’No’ then make the delegation using an appropriate agreement to set out terms.
If ‘No’ then delegation arrangements are not an appropriate mechanism. Use an alternative mechanism such as an MOU, SLA or contract.
If ‘No’ then delegation arrangements with any other types of organization cannot be made with this power. Use an alternative mechanism such as an MOU, SLA, or contract.
3. If ‘No’ then use an alternative mechanism such as an MOU, SLA, or contract.
Figure 2: ICB functions – when to use delegation arrangements under s.65Z5
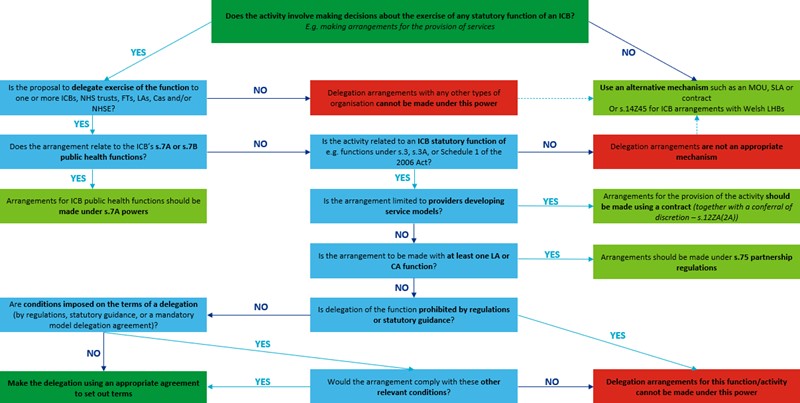
Note: this flow chart:
- Should be used when an ICB wants another organization to carry out activities that it would otherwise carry out itself
- Assumes that primary care transfer provisions have not been commenced
- References sections to the NHS Act 2006, as amended by the Health and Care Act 2022
- Is not an exhaustive statement of what can be achieved under s.65Z5
Image text: Top of the flow chart begins with the question:
Does the activity involve making decisions about the exercise of any statutory function, e.g. making arrangements for the provision of services?
1. If ‘Yes’ then is the proposal to delegate exercise of the function to one or more ICBs, NHS trusts, FTs, As, CAs, and/or NHS England?
If ‘Yes’ then does the arrangement relate to the ICB’s s.7A or s.7B public health functions?
If ‘Yes’ then arrangements for ICB public health functions should be made under s.7A powers.
If ‘No’ then is the activity related to an ICB statutory function of e.g. functions under s.3, s.3A, or Schedule 1 of the 2006 Act?
If ‘Yes’ then is the arrangement limited providers developing service models?
If ‘Yes’ then arrangements for the provision of activity should be made using a contract (together with a conferral of discretion – s.12ZA(2A))
If ‘No’ then is the arrangement to be made with at least one LA or CA function?
If ‘Yes’ then arrangements should be made under s.75 partnership regulations.
If ‘No’ then is the delegation of the function prohibited by regulations or statutory guidance?
If ‘Yes’ then delegation arrangement for this function/activity cannot be made under this power.
If ‘No’ then are conditions imposed on the terms of a delegation (by regulations, statutory guidance, or a mandatory model delegation agreement?
If ‘Yes’ then would the arrangement comply with these other mechanisms?
If ‘Yes’ then make the delegation using an appropriate agreement to set out terms.
If ‘No’ then delegation agreements for this function/activity cannot be made under this power.
If ‘No’ then make the delegation using an appropriate agreement to set out terms.
If ‘No’ then delegation arrangements are not an appropriate mechanism. Use an alternative mechanism such as an MOU, SLA, or contract or s.14Z45 for ICB arrangements with Welsh LHBs.
If ‘No’ then delegation arrangements with any other types of organization cannot be made under this power. Use an alternative mechanism such as an MOU, SLA, or contract or s.14Z45 for ICB arrangements with Welsh LHBs.
If ‘No’ then use an alternative mechanism such as an MOU, SLA, or contract, or s.14Z45 for ICB arrangements with Welsh LHBs.
Figure 3: NHS provider functions – when to use delegation arrangements under s.65Z5
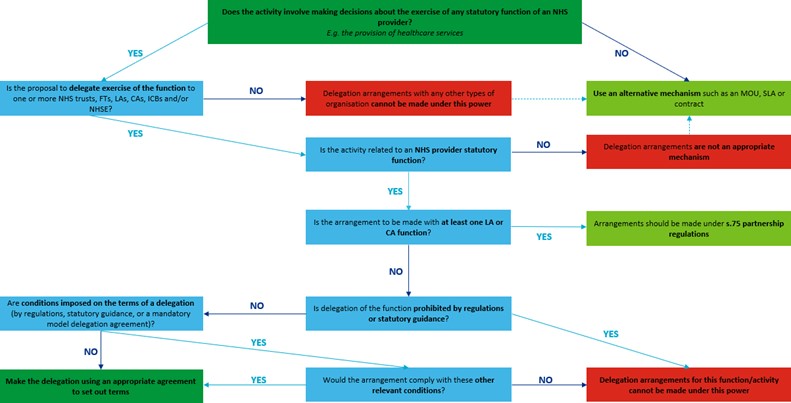
Note: this flow chart:
- Should be used when a provider wants another organization to carry out activities that it would otherwise carry out itself
- Assumes that primary care transfer provisions have not been commenced
- References sections to the NHS Act 2006, as amended by the Health and Care Act 2022
- Is not an exhaustive statement of what can be achieved under s.65Z5
Image text: Top of the flowchart begins with the question:
Does the activity involve making decisions about the exercise of any statutory function of an NHS provider? E.g. the provision of healthcare services.
If’ Yes’ then is the proposal to delegate exercise of the function to one or more NHS trusts, FTs, LAs, CAs, ICBs and/or NHS England?
If ‘Yes’ then is the activity related to an NHS provider statutory function?
If ‘Yes’ then is the arrangement to be made with at least one LA or CA function?
If ‘Yes’ then arrangements should be made under s.75 partnership regulations.
If ‘No’ then is delegation of the function prohibited by regulations or statutory guidance?
If ‘Yes’ then delegation arrangements for this function/activity cannot be made under this power.
If ‘No’ then are conditions imposed on the terms of a delegation (by regulations, statutory guidance, or a mandatory model delegation agreement)?
If ‘Yes’ then would the arrangement comply with these other relevant conditions?
If ‘Yes’ then make the delegation using an appropriate agreement to set out terms.
If ‘No’ then delegation arrangements for this function/activity cannot be made under this power.
If ‘No’ then make the delegation using an appropriate agreement to set out terms.
If ‘No’ then delegation arrangements are not an appropriate mechanism. Use an alternative mechanism such as an MOU, SLA or contract.
If ‘No’ then delegation arrangements with any other types of organization cannot be made under this power. Use an alternative mechanism such as an MOU, SLA, or contract.
If ‘No’ then use an alternative mechanism such as an MOU, SLA or contract.
Annex E – limitations on delegation and joint working
119. The powers in s.65Z5 of the Health and Care Act 2022 (the ‘2022 Act’) are generally permissive – conferring flexibility on organisations in making delegation and joint exercise arrangements.
120. However, there are some restrictions – the National Health Service (Joint Working and Delegation Arrangements) (England) Regulations 2022 as amended (the ‘2022 Regulations’) list the functions that must not be delegated or jointly exercised under these powers. In addition, this annex and accompanying functions table to the statutory guidance set out recommendations/expectations as to the limits to be applied when organisations are delegating or jointly exercising certain functions under these powers.
121. To preserve the ability for organisations to adopt delegation and joint exercise arrangements that suit their local system needs, the limitations set out in this guidance and 2022 Regulations are minimal, and aim to support organisations to exercise their s.65Z5 powers appropriately.
122. Relevant bodies must comply with the requirements set out in the 2022 Regulations and must have regard to this statutory guidance when making arrangements using s.65Z5 powers.
123. Should ICBs and/or NHS providers diverge from this guidance, NHS England may intervene, including consideration of the use of its power of direction under section 14Z61 of the 2006 Act – on the basis that organisations are not acting in the best interests of the health service and therefore are not discharging their functions properly.
Rationale for recommending limitations
124. The functions in scope of s65Z5 arrangements fall into different categories. Certain types of function are not suitable for delegation or joint exercise arrangements; or where they are suitable, they might require limits on how such arrangements should work – for example, in relation to their onward delegation.
125. The function types that are likely to be subject to exemption from, or conditional inclusion in, s65Z5 arrangements are as follows:
Regulatory, oversight and national co-ordination functions:
For these functions, it would be contrary to the intention underlying the function to delegate it or jointly exercise it with other organisations; for example, NHS England’s function under new s14Z57 to performance assess ICBs should not be delegated to ICBs or NHS providers under any circumstances.
Alternatively, there are circumstances where the function requires consistency; for example, the prices set for prescription cost reimbursement – where the value of local variation is outweighed by the benefit of a consistent, national approach across the NHS; or under section 4 where NHS England has a duty to make arrangements for high-security psychiatric services, working closely with another national body or government department (in this case, the Ministry of Justice).
Some of these functions should not therefore be within the scope of s65Z5 arrangements.
Functions central to the corporate governance of individual organisations
These functions assure the organisation’s leadership that it is functioning effectively, so must be retained if the organisation is to operate in its own right; for example, the requirement on each organisation to prepare consolidated annual accounts, or to have an audit committee.
Some of these are functions that are widely recognised as being essential to good governance and should not therefore be within the scope of s65Z5 arrangements.
Ancillary functions
Functions in the ‘ancillary’ category are statutory duties or powers, but which are primarily connected with exercise of a relevant body’s other substantive functions.
Ancillary duties may apply to all of an organisation’s substantive functions or a subset of them. Examples of substantive functions of relevant bodies include their commissioning or regulatory functions, which require or enable them to do something.
Ancillary functions include general duties which have wording such as ‘in the exercise of their functions, relevant bodies must have regard to…’ or ‘relevant bodies must exercise their functions having regard to…’. For example, the duty to co- operate with other bodies in the exercise of their functions or to have regard to reducing health inequalities.
In general terms, any duties which apply to how a substantive function is exercised should continue to apply when the substantive function is delegated. In some cases, the body to which a function is delegated may have equivalent duties which apply. Other ancillary statutory functions will normally be open to delegation and joint exercise to the extent necessary or appropriate for the exercise of the substantive function to which they relate (which the body may be exercising under a delegation agreement).
Commissioning functions
These functions cover the arranging of services or payments in respect of services.
These will usually be open to delegation (with the exception for 2024/25 of delegation of ICB commissioning functions to NHS providers – see Annex G), but as some of the powers are very broad, such as ‘to make arrangements for the provision of health services in England’, there may be expectations stipulating that delegation must only be partial – that is, in specific circumstances or for particular services, such as making arrangements for low acuity mental health services or maternity services. The delegating organisation would retain the responsibility for making arrangements for the remaining services.
126. The 2022 Regulations sets out a list functions that are “globally” exempt from inclusion in s65Z5 arrangements – irrespective of specific circumstances, or the organisations delegating or receiving those functions.
127. The table of functions at Annex F to this statutory guidance sets out any other required or recommended limitations for each function – in particular as to whether it can or should be delegated, or as to how it should be exercised for each NHS England, integrated care board and NHS provider function.
128. In addition to the conditions or limitations set out in the 2022 Regulations and this guidance, organisations may choose to impose their own conditions on the delegated or joint exercise of their functions. For example, NHS England’s 2022/23 delegation agreement with ICBs excluded the onward delegation of any delegated primary care functions without prior consent from NHS England. This condition extends to NHS England’s delegation of primary dental services, pharmaceutical services, primary ophthalmic services and specialised commissioning services where they are delegated.
129. Although this guidance does not currently impose conditions on functions where their delegation or joint exercise gives rise to inherent conflicts of interest that cannot be managed, individual organisations should consider carefully whether this is an issue in their specific circumstances and make appropriate arrangements for their management.
130. This situation is most likely to arise where the delegation or joint exercise of functions could compromise decisions that need to be made in the interests of patients. For example, ICBs’ duties to ensure patient choice and determine Continuing Healthcare eligibility; NHS England’s determination of ICBs’ eligibility for quality payments; and delegating to NHS providers the NHS England and ICB functions of arranging personal health budgets and decisions about individual funding In these areas, NHS providers have legitimate interests relating to value and delivery, but NHS England and ICBs could determine that their duty to protect and promote patient interests are best promoted by reserving certain aspects of those functions.
Delegation from ICBs to NHS providers
131. Although the relevant sections of the 2022 Act have commenced, NHS England expects integrated care boards not to delegate their functions to NHS trusts and foundation trusts in the coming financial year (2024/25). Further details on this hold on delegation are set out in Annex G.
Guidance regarding NHS Continuing Healthcare and NHS-funded Nursing Care
132. ICBs assumed responsibility for NHS Continuing Healthcare (CHC) and NHS- funded Nursing Care (FNC) from 1 July 2022. In exercising their functions under or by virtue of sections 3, 3A or 3B of the NHS Act 2006, insofar as they relate to NHS Continuing Healthcare and NHS-funded Nursing Care, a relevant body (in this case ICBs or NHS England in some limited circumstances*) must comply with the requirements set out in the National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) Regulations 2012, whilst having regard to the National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care. Relevant bodies should work jointly with local authorities insofar as is reasonably practicable.
133. NHS England, ICBs, NHS Trusts, and Foundation Trusts (the “relevant bodies” set out in the 2022 Act) must have regard to this guidance for Delegation and Joint Working Arrangements. In addition, in relation to CHC and FNC, the 2022 regulations (as amended) preclude ICBs and NHS England from delegating decisions as to whether or not an individual is eligible for CHC or FNC to any other body. It also precludes NHS England from delegating the function of arranging for the review of CHC eligibility decisions to any other body. The amendment does not apply to individuals who may have a primary health need arising from a rapidly deteriorating condition, who may be entering a terminal phase. For this cohort of individuals, there is a ‘Fast-Track’ pathway to determining eligibility for CHC.**
134. This means that NHS England and ICBs must comply with these regulations and must not delegate their final decision-making functions on eligibility for CHC or FNC to any other organisation. ICBs and NHS England are able to delegate their assessment and commissioning functions, in relation to CHC and FNC to appropriate organisations set out in s65Z5 of the NHS Act 2006.
135. For further information on the process to assess for CHC and FNC eligibility, please see the National Framework for NHS Continuing Healthcare and NHS- funded Nursing Care.
Table of functions
136. This table at Annex F sets out functions of NHS England, ICBs and NHS providers relevant to s65Z5 arrangements – and the expectations on their inclusion in such arrangements. For completeness, it also lists those functions excluded via the list in the 2022 Regulations.
137. Relevant bodies should pay particular attention to the functions table when considering potential delegation of a function or placing it in a joint working arrangement, to see whether this is permitted. If it is, relevant bodies should then consider any further guidance on the delegation of that function (such as proposed limitations or restrictions), which they must take into account.
* The duty on NHS England to arrange for the review of CHC eligibility decisions is set out at Regulation 23 of the National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) Regulations 2012.
** Their eligibility for CHC is, in substance, determined by an appropriate clinician, in accordance with regulation 21(8) and (9) of the Standing Rules. That is because there is no discretion afforded to an ICB or NHS England in determining whether an individual on the Fast-Track pathway is eligible for CHC. Rather, they must find the individual eligible for CHC if an appropriate clinician has found such an individual to have a primary health need where the Fast Track Pathway Tool has been completed in accordance with regulation 21(8) of the Standing Rules.
Annex F – list of statutory functions to be considered for delegation and joint working arrangements
This spreadsheet sets out functions of NHS England, ICBs and NHS providers relevant to s65Z5 arrangements – and the expectations on their inclusion in such. For completeness, it also lists those functions excluded via the list in the 2022 Regulations.
Annex G – hold on the delegation of integrated care board (ICB) statutory functions to NHS trusts and foundation trusts into financial year 2024/25
Background
138. NHS England welcomes the development of more collaborative approaches that systems are adopting towards assessing population needs, service design, and commissioning, including greater flexibility and responsibility being given to providers for the delivery of system priorities, including through provider collaboratives.
139. The intention behind the Health and Care Act 2022 was to enable these and broader forms of collaborative arrangements. To this end, the Act introduced a range of new flexibilities and powers, including the ability for ICBs to delegate statutory functions to, NHS providers (ie NHS trusts and foundation trusts).
140. NHS England has worked closely with systems and providers to understand the opportunities and risks relating to formal ICB to provider delegation. Our engagement suggests appetite for the use of these powers in the coming financial year is limited, and that system plans can be supported through one or a combination of simpler existing mechanisms (a list of which can be found in Appendix 1) and therefore do not require formal delegation.
141. Given the additional potential complexity of delegation arrangements and the associated risks, and the significant operational and financial pressures facing systems in 2024/25, NHS England continues to expect that ICBs do not seek to use these powers in financial year 2024/25. NHS England remains supportive of collaboration and innovation, and will consider exemptions where local proposals can demonstrate both substantial benefits for patients and communities alongside robust assurance arrangements. Proposals will be subject to a risk based assurance review by NHS England. In such cases, NHS England will first consider the case for change and the strategic benefits to both the ICB and patients of delegation. If this shows sufficient merit, NHS England would then need to assure itself of providers’ ability to carry out the functions and the robustness of systems in place to manage associated risk (financial, quality and execution).
142. This hold only applies to delegation of ICB statutory functions to NHS providers. It does not apply to delegation from NHS England to ICBs (eg primary care commissioning functions), or ICBs delegating to one another. The hold does not apply specifically to delegation to local authorities. However, as indicated earlier in this guidance, the use of ICB powers to delegate to local authorities should be considered in conjunction with Section 75 partnership arrangements and within the scope of s75 restrictions.
143. If you have concerns about the hold impacting on your plans for 2024/25, or would like to discuss potential proposals, please contact your NHS England regional team.
Appendix 1 – existing mechanisms to enable more collaborative approaches to commissioning
Outcomes-based commissioning: Contract sets broad scope of what provider is expected to achieve, rather than the means of achievement.
Lead provider models: Single NHS trust or foundation trust takes on contractual responsibility for an agreed set of services, on behalf of a provider collaborative, and then subcontracts to other providers as required.
Conferral of discretions: Commissioning contract gives provider discretion in relation to the services provided under the contract; e.g. as to the allocation of resources between different services under the contract, and how those services are provided or subcontracted. A key part of lead provider models.
ICB committee or subcommittee including members from providers: An ICB board delegates exercise of certain ICB functions to one of its committees or sub-committees and appoints executives or nonexecutives from providers to membership of the committee or subcommittee exercising those functions. (Note – this must be in line with the ICB’s constitution and other governance arrangements, including in respect of conflicts of interest).
Joint committees between ICBs and providers or solely between providers: A joint committee of an ICB and NHS trust(s)/foundation trust(s) could exercise functions those bodies have agreed to exercise jointly through the committee, allowing binding shared decisions. A joint committee solely of trusts and foundation trusts could similarly exercise trust functions which the trusts have agreed to exercise jointly, which may for example form part of lead provider or other contracting models.
These mechanisms are not mutually exclusive, and some can be used in combination.
Publication approval reference: PRN0152