
Introduction
1. The 10 Year Health Plan sets the clear ambition for an NHS that delivers the 3 shifts:
- hospital to community
- analogue to digital
- sickness to prevention
Our new operating model provides the mechanism to realise this ambition through a simpler, more disciplined, rules‑based system in which expectations and consequences are clear. Success is met with greater freedoms, challenge with meaningful support, and persistent failure with fair but firm intervention. This replaces unnecessary bureaucracy with clarity and guardrails so leaders and staff can focus on improving care.
2. Under our new NHS operating model, each part of the system has a defined role:
- NHS England’s national teams and the Department of Health and Social Care (DHSC) set national outcomes and build shared platforms
- NHS England’s regional teams provide leadership with a single line of sight across performance and support
- integrated care boards (ICBs) become strategic commissioners, shifting resources into prevention and community capacity
- providers deliver high-quality and efficient services
- neighbourhood teams provide proactive, digitally enabled support to communities
3. The NHS Oversight Framework for 2026/27 is an integral part of our operating model providing clarity around accountability and our approach to oversight and intervention. Its objective is to bring fairness, proportionality, consistency, transparency and predictability to our oversight of NHS trusts and foundation trusts (collectively referred to as ‘providers’ in this framework) and ICBs.
4. In this context, the framework supports a value-based care approach, aiming to improve outcomes and experiences that matter to patients and communities, while making best use of public resources.
5. During 2025/26, we focused on embedding new operating arrangements and progressing provider capability assessments. Feedback from the service emphasised the importance of keeping the oversight model simple while ensuring it remained robust, data-driven and aligned with the priorities in the NHS Medium Term Planning Framework. This framework is designed to drive medium-term system transformation while maintaining operational performance tracking.
6. We are bringing together measures of access, quality, productivity, people and finance, and considering organisational capability as the basis for proportionate support and intervention. Publication of this information – including publicly available league tables – enables everyone to see how organisations compare and what follows next, with boards expected to use this insight to drive tangible improvement alongside wider metrics recommended in the Insightful board documents.
7. This update for 2026/27 is intentionally evolutionary, retaining the core architecture and oversight approach from the 2025/26 Oversight Framework. It has been updated to reflect the maturing operating model, introduces delivery segmentation for ICBs and clarifies the role of NHS England’s regional teams in overseeing performance.
8. Our intention is to be transparent and consistent in our oversight approach. We want the rules of engagement to be clearer, so boards know what to expect from us. This includes how we recognise capable, high-performing organisations and those that require structured support or intervention. The main changes from last year’s framework are:
- alignment of the approach to delivery segmentation for ICBs and providers
- clearer recognition of highly capable, high-performing providers, including those that are awarded advanced foundation trust status and benefit from lighter-touch oversight
- update oversight metrics aligned to the NHS Medium Term Planning Framework, including new metrics for mental health, community and ambulance trusts
- refinement of the delivery segmentation methodology, moving from a quartile-based approach to statistical thresholds, to make tracking of improvement easier
- establishing a stronger link between the oversight response model and delivery segmentation, organisational capability, and other considerations around engagement intensity, support, potential incentives and consequences
9. Over 2026/27, we will work with the service to develop an approach to our ICB capability assessments. This will include looking at the ICB’s role as a strategic commissioner, including for primary care services, and its alignment with the strategy for neighbourhood health.
10. This is a 1-year framework; we will review and update the framework for 2027/28. We are committed to continuously improving the oversight approach with annual updates. We actively welcome feedback on the framework from NHS organisations, stakeholders and the public. If you have any comments or questions about this framework, these can be shared with us at oversightandassessment@nhs.net
Roles and responsibilities in oversight
11. The Model ICB Blueprint and Strategic commissioning framework describe the role of ICBs as strategic commissioners, while the Model Region Blueprint defines how NHS England regions oversee and support ICBs and providers.
12. Oversight by the regions is the process of combining a wide range of information to form a rounded view of how well an organisation is delivering its statutory duties and agreed priorities. This determines the level of scrutiny and how NHS England directs incentives, resources, support and interventions.
Figure 1: Roles of NHS England regional teams as set out in the Model Region Blueprint

Figure description: A diagram showing the roles of NHS regions in providing leadership for a high-performing and sustainable regional health system.
Regional strategic leadership
Strategic leadership of regional health system to support delivery of reform, overseeing planning, investment and reconfiguration, supporting innovation and ensuring effective regional leadership strategy and talent pipelines.
Performance management
Holistic oversight of performance in line with national frameworks, including understanding board and leadership capability, understanding ‘early warning’ and managing risk.
Improvement and intervention
Regional approach to improvement, support and intervention to ensure high-quality and sustainable care, developing capability, addressing underperformance and overseeing regulatory interventions as required.
13. The specific responsibilities of NHS England, ICBs and providers in oversight are set out below.
Specific oversight responsibilities of NHS England, ICBs and providers
NHS England national teams
- setting overarching oversight policy
- ensuring consistency of implementation, including moderation of capability assessments
- calculation of oversight segments
- agreeing the use of support and intervention, including diagnostics, where this requires national resources
- co-ordinating cross‑boundary risks and issues that require a national view (for example, where risks span multiple systems or regions)
NHS regional teams
- leading day-to-day oversight of provider and ICB delivery
- making assessments of NHS organisational capability
- calibration of support and intervention based on analysis of regional risk profile
- escalating major issues where these constitute sufficient risk or complexity
- undertaking and co-ordinating annual assessments of ICB performance and capability
- enacting the use of enforcement powers in line with guidance and governance
ICBs
- contract-managing and assuring commissioned services (including those commissioned on behalf of NHS England) and using contractual levers to address non‑delivery
- self-assessing capability and performance
- operating a ‘no surprises’ approach and escalating potentially significant issues where these constitute sufficient risk or complexity
Providers
- ensuring high-quality and effective care for all patients and service users through effective quality governance, including learning and improvement following patient safety incidents in line with the Patient Safety Incident Response Framework
- setting strategic direction, ensuring the executive has appropriate capacity and capability to monitor and manage quality of care and operational delivery
- using prudent and effective controls to lead the organisation
- promoting and adhering to the organisation’s values
- ensuring all statutory and regulatory obligations and duties are met
- self‑assessing capability and performance, identifying issues and supporting continuous improvement
- maintaining a ‘no surprises’ approach with NHS England, escalating potentially significant issues
14. The roles and responsibilities set out above apply throughout this framework. Subsequent sections describe how these are exercised in practice through segmentation, capability assessment, monitoring and the oversight response.
Scope
15. The NHS Oversight Framework applies to ICBs and providers as statutory NHS entities. Other providers of NHS services are overseen through contractual and regulatory arrangements, as set out below.
- Independent providers of NHS services – ICBs are expected to ensure the quality and performance of these services through contract management and, where necessary, taking action and escalating concerns to the relevant regions. NHS England continues to oversee certain independent providers under the independent providers risk assessment framework (IPRAF) and NHS-controlled providers under either the IPRAF or this framework.
- Primary care providers – ICBs are responsible for primary care commissioning and population health. Consideration of how effectively an ICB is commissioning, assuring, and overseeing services, including primary care, in their strategic commissioning role forms part of ongoing ICB oversight, including annual assessments and future capability assessments.
- Provider collaboratives, groups and clustered ICBs – these groups are formed from legally distinct organisations and so are subject to this framework as distinct entities. Where collaboratives or groups have agreed delivery arrangements, regions may also consider group-level intelligence, but this does not replace entity-level oversight.
16. NHS England remains ultimately accountable for those services it has delegated responsibility for commissioning to ICBs. These include certain specialised services and all primary care services and the handling of associated complaints. NHS England holds ICBs to account for the performance of these services in their system through delegation agreements.
Components of oversight
17. As detailed in figure 2, NHS England’s oversight approach is composed of:
- delivery monitoring: we assess delivery against defined metrics and allocate a segment (1 to 4)
- capability monitoring: we assess leadership, governance and delivery capability
- oversight response: we combine segment, capability assessment and other considerations from ongoing monitoring to guide oversight intensity, potential incentives, support and (where necessary) intervention
Figure 2: Components of oversight
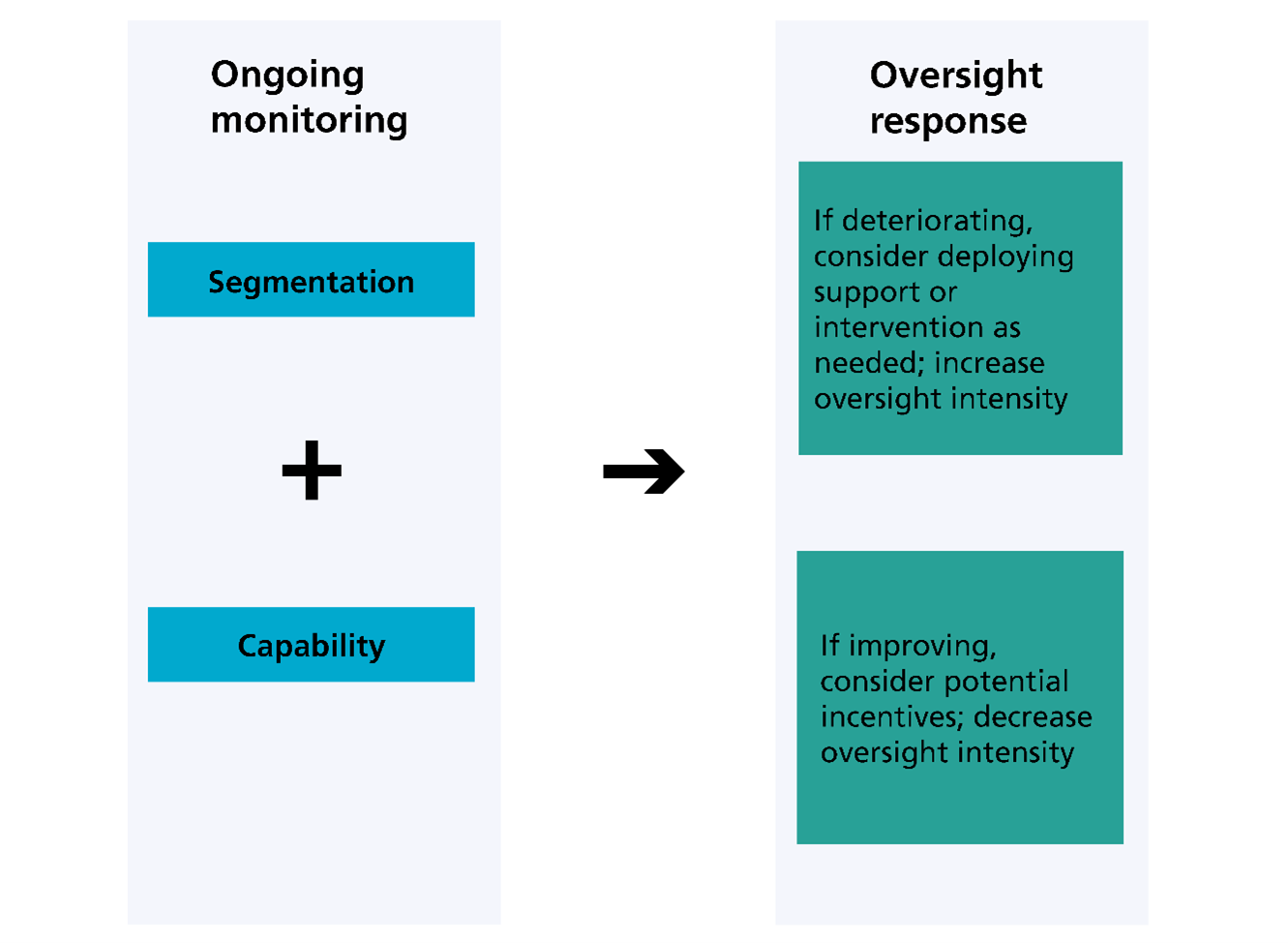
Figure description: This figure explains how NHS England decides its oversight response by considering segmentation and organisational capability together.
Ongoing monitoring looks at both:
- segmentation – identifying whether support or intervention is needed
- capability – judgement on how capable an organisation is to manage its support needs
These assessments inform the oversight response:
- if segmentation and/or capability is deteriorating, consider deploying support or intervention as needed; increase oversight intensity
- if segmentation and/or capability is improving, consider potential incentives; decrease oversight intensity
18. Alongside our oversight approach, where real-time intelligence or operational information indicates that an organisation’s delivery or quality may decline rapidly, we may undertake performance management activities to secure improvement. For providers with serious performance concerns, regional teams will undertake performance management activities, supported by rapid access to time-limited, expert improvement support as determined by need.
19. Oversight and performance management are closely linked but serve different purposes. Oversight is the enduring, proportionate relationship between NHS England and an organisation, informed by segmentation, capability, and other considerations from ongoing monitoring. Performance management is often issue‑specific and employs intensive scrutiny and engagement with an organisation to secure rapid improvement where there is a material risk to patients, staff, quality, access, or financial sustainability, or where performance is deteriorating quickly.
20. Performance management can be initiated at any point in the year and is limited to the time period required to resolve the concern. Where performance management activity indicates that risks are broader or sustained, we may review and adjust our oversight response for an organisation to ensure the overall approach remains proportionate and joined‑up.
21. In summary, oversight sets the overall relationship between NHS England and an organisation, while performance management is a targeted tool used to address specific, time‑critical risks.
Example – performance management alongside oversight
Through daily situation reports, NHS England becomes aware of emerging issues with ambulances being delayed outside a provider’s A&E department. This is creating unacceptable downstream risk of delay in ambulances reaching patients requiring urgent care in the community.
Regardless of the provider’s delivery segment or capability rating, we may decide to undertake time-limited performance management to support the provider in resolving these issues by agreeing to short-term actions to facilitate timelier patient handover.
Should these issues be difficult to resolve through performance management alone, we may decide, during the provider’s regular oversight review, that a more structured response is needed. This may involve deploying resources to support more detailed diagnostics and solution management.
22. NHS England’s oversight does not replace or duplicate the role of other regulators. We work closely with bodies such as the Care Quality Commission (CQC) and professional regulators, sharing intelligence and considering regulatory findings as part of our overall assessment of risk, performance and capability.
23. This framework sets out how NHS England oversees delivery and capability; it does not replace statutory duties, licence obligations or board accountability for delivery. Annex A summarises the oversight activities over an annual cycle.
Delivery segmentation
24. Each organisation is assigned a segment between 1 and 4 (see table 2). This is based on data and provides a high‑level view of the breadth of challenges it faces. Organisations in segment 1 likely have a narrow range of issues, while those in segment 4 have the broadest.
25. While segmentation is not a judgement of leadership quality or improvement potential, it indicates where delivery risk lies and informs the scale and nature of the oversight response when considered alongside capability and other intelligence.
Figure 3: How metrics determine the delivery segment, including the financial deficit override where applicable
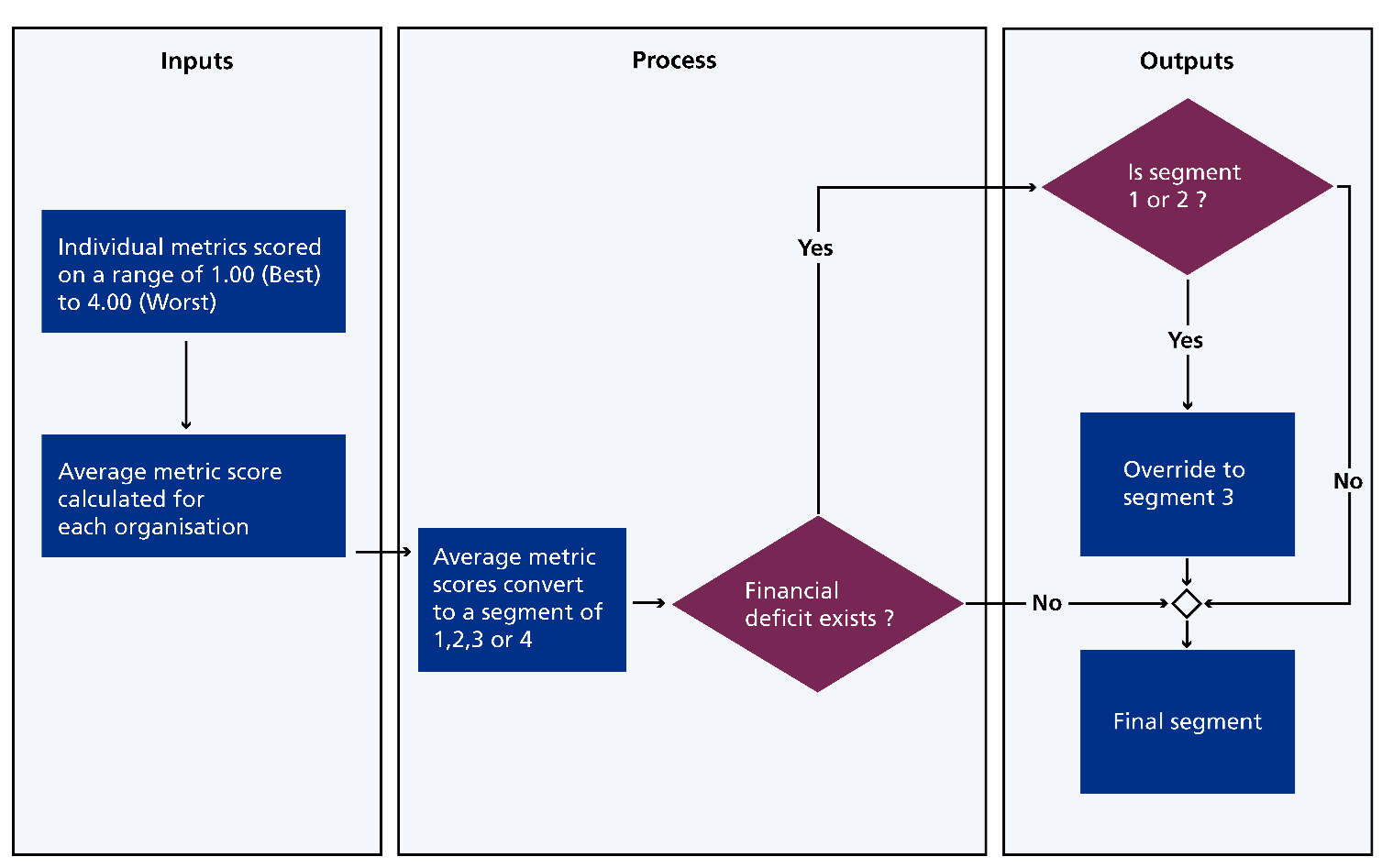
26. The process for determining segmentation (shown in Figure 3 above) is set out in full in the NHS Oversight Framework methodology manual. In summary, the process is as follows:
- calculation of an average metric score: each organisation receives a score for its delivery against a range of metrics. Each metric has an agreed scheme for scoring between 1 and 4. The individual metric scores are then averaged to produce an overall score for each organisation
- segmentation: each organisation’s overall score is then benchmarked against the rest of the country using defined rules to translate the score into a segment of 1, 2, 3, or 4
- overrides: there is a single override within the segmentation methodology. Any organisation determined to be in financial deficit is automatically prevented from being allocated to segment 1 or segment 2 until the deficit has been satisfactorily resolved
Table 2: Description of delivery segments
|
Segment |
Description |
|
1 |
The organisation performs highly across most areas and any challenges have a narrow focus. |
|
2 |
The organisation performs better than average across most areas but may have some areas of challenge to address. |
|
3 |
The organisation performs below average across multiple areas and may require more co-ordinated responses. Or, the organisation’s delivery segment has been overridden due to finance concerns. |
|
4 |
The organisation performs significantly below average in a range of areas and is likely to require a co-ordinated response and potential intervention. |
27. The segmentation process scores each organisation objectively against national standards and priorities set out in the 10 Year Health Plan and the NHS Medium Term Planning Framework. Metrics are reported under a set of standard domains (see table 3) tailored to reflect the organisation’s role within a standardised structure for the health and care system.
28. ICBs and providers are scored against the domains set out below, with specific metrics reflecting their respective responsibilities. For ICBs, the second domain is ‘allocating resources’, reflecting their role as strategic commissioners. For providers, it is ‘access’, reflecting their role as service providers. For providers, each domain includes a range of appropriate metrics for each provider type (acute, mental health, community and ambulance trusts). Each domain is scored from 1 to 4 to evaluate the performance across specific areas at organisational level.
Table 3: ICB and provider domains and sub-domains for delivery segmentation
ICB domains | Provider domains |
|
Population health and inequalities
|
Population health and inequalities
|
Allocating resources
|
Access
|
|
Effectiveness of care
|
Effectiveness of care
|
|
Experience of care
|
Experience of care
|
|
Patient safety
|
Patient safety
|
|
Finance, productivity and innovation
|
Finance, productivity and innovation
|
|
People
|
People
|
Due to small numbers of metrics for the 2026/27 financial year the population health and effectiveness of care domains will be reported as a single “effectiveness of care and population health” domain for providers.
29. Delivery metrics are classed as scoring or contextual. Scoring metrics are robust, comparable and are used in the calculation. Contextual metrics are informative but not comparable or not yet sufficiently mature; they are used to support how NHS England responds to segmentation rather than informing the calculation itself. Annex B lists the 2026/27 scoring and contextual metrics by domain. Contextual metrics should form part of other governance information that boards monitor, as set out in the Insightful board guidance.
30. Segmentation data is also used to rank organisations relative to others of the same type in a published league (see the league table process for how we translate segmentation data into league tables). League tables allow organisations and the public to understand performance relative to appropriate peers, both overall and across a range of specific areas.
31. Where organisations are undergoing transactions, including mergers, any adverse impact on delivery from taking on challenged services will continue to be reflected in segmentation. Segmentation will not be adjusted to offset the effects of transactions. Instead, the acquiring organisation’s capability to manage and improve those services will be considered through their capability assessments and wider regional judgement as part of the oversight response (see capability and oversight response sections).
32. ICBs are currently undergoing structural reforms, with some working temporarily in clusters while mergers and boundary adjustments are completed. ICBs that merge into statutory organisations in April 2026 will be subject to segmentation for the first time in quarter 1 2026/27. Clustered ICBs that have not merged by 1 April 2026 will remain segmented as separate legal entities rather than clusters.
Publication of data
33. As part of our commitment to openness and transparency, we publish a range of information related to segmentation and league tables on a public dashboard. This gives patients, the general public, system partners, and NHS organisations a single shared picture of each organisation’s delivery, including individual metric results, domain scores, segments, and league table rankings. While contextual metrics do not appear on the public dashboard, they are available to NHS organisations through internal tools.
Capability assessments
34. Capability assessments provide NHS England with a structured view of an organisation’s leadership, governance and ability to deliver sustained improvement. They consider how effectively boards set direction, manage risk, use data and insight, engage with partners and translate plans into delivery.
35. Capability assessments complement delivery segmentation by focusing not on what an organisation has delivered, but on its capacity to improve, and are used alongside delivery information and other considerations from ongoing monitoring to determine the appropriate oversight response. Capability assessments are conducted annually, with quarterly reviews and may be revised in-year in light of new or emerging information.
ICB capability
36. For 2025/26, our statutory annual assessment of each ICB’s performance will be conducted in line with the ICB annual assessment guidance for 2025/26. The annual assessment provides our view on how well an ICB has met its statutory functions, performed its strategic commissioning role, worked with system partners, and commissioned and assured services on behalf of NHS England for which it has delegated responsibility, such as primary care and associated complaints handling and some specialised services.
37. During 2026/27, we will work with ICBs to develop an approach to assess capability, reflecting their central role as strategic commissioners and system leaders, including for primary care services, and aligned with the strategy for neighbourhood health. From 2027/28, we anticipate that formal ICB capability assessments will be incorporated into the annual assessment, alongside a delivery score derived from the ICB’s average segment in the preceding year.
38. In the meantime, the 2025/26 annual assessment will provide the primary qualitative view of ICB leadership, governance and strategic commissioning readiness. Regions will use this alongside segmentation and other considerations from ongoing monitoring to calibrate the oversight response and agree proportionate support or intervention, recognising that ICBs are evolving their operating model during this period of change.
Provider capability
39. Providers receive annual capability ratings in line with the guidance on assessing provider capability. The process consists of:
- a self‑assessment completed by the provider board against a range of expectations across the 6 domain areas of the Insightful provider board
- a regional team review of this self-assessment, the evidence behind it, the region’s own views of the board, the provider’s track record and the views of any relevant third parties
40. Following this, the region assigns a capability rating to the provider. This rating reflects not only how the board is overseeing the organisation, but also how well it is supporting system working and collaboration. Ratings are moderated for consistency and confirmed through the relevant NHS England governance route. Providers with high capability are rated ‘green’, those for which we have significant concerns are rated ‘red’, and those in between are rated ‘amber-green’ and ‘amber-red’ depending on the level of issues identified.
41. Provider self‑assessments are completed annually; however, capability ratings may be revised in‑year where new information emerges. The capability ratings and any subsequent changes are moderated and approved by the relevant NHS England governance group. The capability rating for each provider is published alongside its segment and league table position.
Other considerations
42. While our oversight response is based on segmentation and capability, other factors from our ongoing monitoring are also considered, including internal information such as progress against plans and external sources such as escalations from NHS organisations or other regulators. We use a mix of qualitative and quantitative data across several areas to support our oversight. This includes:
- information provided by ICBs and providers as part of routine interactions, including via contract monitoring
- progress against agreed plans and key performance indicators in line with the commitment in the Medium Term Planning Framework that operating plans should be scrutinised as part of routine oversight arrangements
- information from official performance management or improvement programmes, including enhanced national support arrangements
- intelligence shared through system and regional quality groups in line with the National Quality Board guidance on quality risk response and escalation in integrated care systems and reports from organisations such as the CQC, Health and Care Professions Council, General Medical Council, Nursing and Midwifery Council, and the Office for Standards in Education, Children’s Services and Skills (Ofsted)
- third-party information, for example, whistleblowing, 360-degree feedback, peer reviews, complaints, formal publications or assessments, internal and external audit reports, and police and coroner reports
43. We expect all organisations to promptly escalate any issues and risks that are or may potentially significantly affect delivery, finance or quality to their relevant regional team as part of a ‘no-surprises’ approach. The section below explains how we bring together such escalations with segmentation, capability and other considerations from ongoing monitoring to agree a coherent response.
Oversight response
44. NHS England’s regional teams lead the oversight of ICBs and providers, and the intensity of oversight is informed by both an organisation’s delivery segment and its capability, ensuring a proportionate and joined‑up approach to improvement and risk. This relationship may also be informed by other relevant information from ongoing monitoring or escalation.
45. Organisations in higher segments and with lower capability are likely to receive the most intensive oversight and support or intervention. By contrast, organisations in lower segments with higher capability are likely to benefit from lighter-touch oversight arrangements and be potential candidates for greater freedoms and incentives.
46. The section below illustrates typical oversight relationships. It does not replace regional judgement, which will take account of organisational context and risk.
NHS England’s oversight response
This illustrates typical oversight relationships based on organisational profile. It does not replace regional judgement, which will take account of organisational context and risk.
Segment 1 or 2 with green or amber-green capability
How we drive improvement
The organisation has a narrow range of issues and is therefore expected to be able to diagnose challenges, tackle issues and clearly explain any support needs.
Support from NHS England is not normally expected unless problems are particularly deep or intense.
The organisation is expected to take a leadership role in developing and sharing best practice and improvement initiatives in areas where it excels.
The organisation is most likely to be eligible for additional freedoms, such as advanced foundation trust status or certain capital freedoms.
How we intervene
Intervention is minimal and, where required, is highly targeted using specialist resources. In exceptional circumstances, enforcement powers can be used if necessary, but this is not expected.
Segment 2 with amber-red or 3 with amber-green capability
How we drive improvement
Regional teams agree the organisation’s support needs based on its individual areas of strength and challenge, which is usually delivered through:
- local support offers
- defined national support programmes
- bespoke regional interventions
The organisation receives increased scrutiny, likely targeted at improving performance in challenged areas.
Where the delivery segment is driven by a financial deficit override, targeted activities are expected from the organisation to identify how sufficient improvement can be made to no longer meet the override condition.
How we intervene
Interventions may be applied, or the organisation may be required to act in specific areas of low performance. This may involve the use of enforcement powers, particularly where performance concerns persist.
Segment 3 or 4 with amber-red or red capability
How we drive improvement
The organisation is subject to the most intensive level of scrutiny until its delivery and/or capability improves and it can demonstrate that this improvement can be sustained.
How we intervene
Enforcement powers are highly likely to be used, and this is agreed through the relevant NHS England governance group.
Support may be mandated as part of an improvement plan that NHS England is involved in developing, drawing on experts as necessary.
Very senior manager (VSM) pay restrictions or limits applied to operational freedoms.
47. Our oversight response is designed to be flexible and dynamic rather than prescriptive. It is therefore not anticipated to change automatically in response to every change in circumstances. While the oversight response is expected to be reviewed every quarter, it is likely to remain stable with any changes based on sustained trends, capability and risk rather than single data points.
Advanced foundation trusts
48. Advanced foundation trusts will benefit from proportionate, risk-based oversight. This includes a time‑limited period (up to 6 months) to resolve non‑urgent issues without escalation. Where serious concerns arise (for example, a 2‑segment fall or a ‘red’ capability rating over 2 quarters), the oversight response is adjusted accordingly. Advanced foundation trust status may also be reviewed in line with the criteria set out in the forthcoming advanced foundation trust guidance.
Incentives, support, and consequences
49. NHS England’s oversight approach is designed to recognise and reward strong delivery and capability, and to apply fair but firm consequences where delivery or capability is persistently low. The incentives, support and consequences set out below are applied through clear national and regional governance arrangements, described in the next section.
50. Incentives: organisations that consistently demonstrate strong delivery and effective leadership benefit from greater freedoms and incentives. This may include eligibility to apply for advanced foundation trust status, access to additional capital flexibilities in line with capital planning guidance and lighter‑touch processes for taking on responsibility for NHS Property Services estates, where appropriate, in line with NHS property guidance. These organisations are also expected to play a leading role in supporting improvement across the system, including sharing good practice in the areas where they excel.
51. Support: where organisations face challenges in delivery and/or capability, NHS England will increase scrutiny and provide proportionate, targeted support to help secure improvement. For providers, this includes bespoke support from regional teams, where appropriate, as well as access to improvement support offers such as the Get It Right First Time (GIRFT) programme, alongside NHS IMPACT and the GIRFT Academy, which are available to all organisations to strengthen improvement capability.
52. For ICBs, NHS England will provide support during 2026/27 to strengthen their role as strategic commissioners. This will be delivered through a structured development offer, focusing on commissioning capability, board leadership and the effective use of commissioning levers to support neighbourhood health and system transformation.
53. Consequences: where performance and/or capability remain persistently low, or where risks escalate, freedoms may be curtailed and formal consequences applied. This may include mandated improvement support and/or enforcement action. Where providers have long-standing financial and operational issues, they may be considered for entry into an intensive recovery programme. Other consequences may apply where appropriate, including ineligibility for very senior managers (VSM) pay awards in line with the VSM pay framework and enforcement action in line with NHS enforcement guidance (such as undertakings, discretionary requirements, additional licence conditions or other measures). This approach ensures proportionate intervention, supports improvement and safeguards public resources.
Oversight governance
54. Oversight decisions are made through a clear and proportionate governance model that balances national consistency with regional judgement. NHS England regions are responsible for leading day‑to‑day oversight of ICBs and providers, agreeing support and improvement plans, and where required, initiating performance management activity and the use of enforcement powers. Regions review the oversight response for each organisation at least quarterly in line with the refresh of segmentation data and bring together multidisciplinary teams to ensure oversight decisions are made consistently and take account of all relevant factors. Regional teams may make changes to oversight responses at any time to address emerging events.
55. Certain decisions require national moderation or approval to ensure consistency, the appropriate use of powers or access to national resources, including the approval of provider capability ratings. These decisions are taken through the relevant NHS England governance, informed by regional recommendations and supporting evidence. This approach ensures that oversight decisions are timely, proportionate and aligned with national expectations, while remaining responsive to local context and risk.
Annex A: Annual cycle of oversight activities
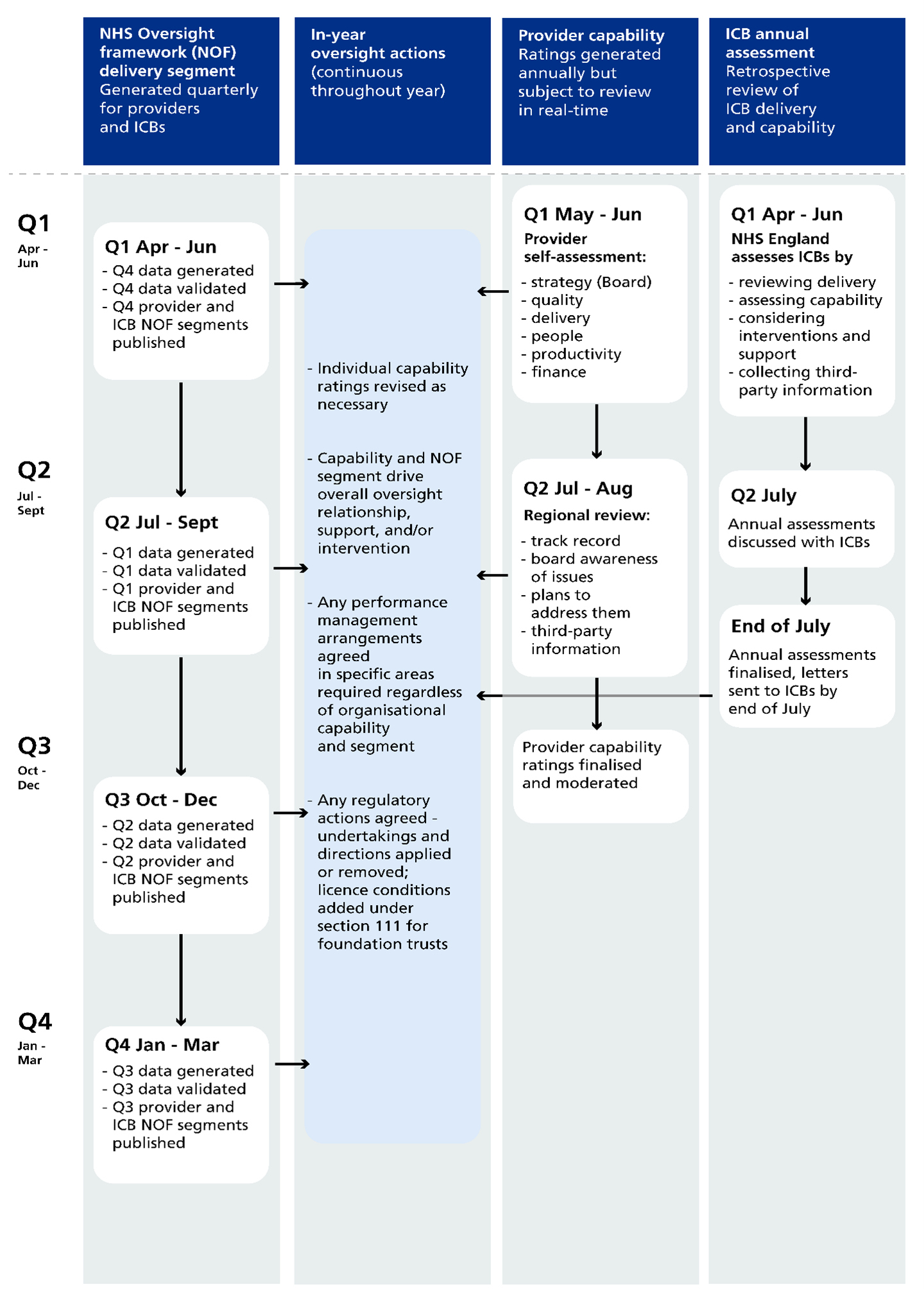
Image description: The image gives an overview of the annual cycle of NHS England oversight activities.
Oversight activity runs continuously throughout the year, with some elements updated quarterly and others annually. In‑year oversight actions may take place at any point in response to emerging issues.
The main components are:
- quarterly delivery segmentation for providers and ICBs
- ongoing in‑year oversight actions
- annual provider capability ratings, which can be reviewed at any time
- annual ICB assessments, carried out retrospectively
Quarterly delivery segmentation (providers and ICBs)
Delivery segmentation is generated every quarter using data from the previous quarter.
April to June (quarter 1)
Data from quarter 4 of the previous year is generated and validated. Quarter 4 provider and ICB delivery segments are published.
July to September (quarter 2)
Data from quarter 1 is generated and validated. Quarter 1 provider and ICB delivery segments are published.
October to December (quarter 3)
Data from quarter 2 is generated and validated. Quarter 2 provider and ICB delivery segments are published.
January to March (quarter 4)
Data from quarter 3 is generated and validated. Quarter 3 provider and ICB delivery segments are published.
In‑year oversight actions (continuous)
Oversight actions take place throughout the year and are informed by delivery segmentation, provider capability and emerging risks.
These actions may include:
- revising individual provider capability ratings where necessary
- using capability and delivery segment information to shape the overall oversight relationship, including support and intervention
- agreeing performance management arrangements in specific areas, where required, regardless of overall organisational capability or delivery segment
- agreeing regulatory actions, such as undertakings or directions being applied or removed, or licence conditions added for foundation trusts under section 111 of the Health and Social Care Act 2012
Provider capability ratings
Provider capability ratings are generated annually but may be reviewed and updated at any time.
May to June (quarter 1)
Providers complete a self‑assessment covering:
- strategy (board)
- quality
- delivery
- people
- productivity
- finance
July to August (quarter 2)
Regional teams carry out a review, considering:
- track record
- board awareness of issues
- plans to address issues
- third‑party information
October (quarter 3)
Provider capability ratings are finalised and moderated.
ICB annual assessment
ICB annual assessments are retrospective and review ICB delivery and capability.
April to June (quarter 1)
NHS England assesses ICBs by:
- reviewing delivery
- assessing capability
- considering interventions and support
- collecting third‑party information
July (quarter 2)
Annual assessment outcomes are discussed with ICBs.
By the end of July
Annual assessments are finalised and letters are sent to ICBs.
Annex B: NHS oversight metrics for 2026/27
Summary
The metrics underpinning the NHS Oversight Framework are annually reviewed to ensure that they remain an accurate representation of NHS operating priorities.
They are intentionally designed to consider a broad range of subjects to enable a balanced judgement of the range of challenges each organisation faces as well as to allow an understanding of particular areas of challenge.
There are 86 metrics underpinning the NHS Oversight Framework; however, no organisation is assessed against all of them.
The summary table below provides an indicative view of how many metrics typically apply to each organisation type, noting that many organisations deliver more than 1 type of service and may therefore be subject to a broader set of metrics. Any trust that supplies data for a given activity will be scored on the corresponding metric unless an explicit exemption applies. These exemptions are set out in the technical annex.
|
Organisation type |
Total number of applicable metrics |
|
Integrated care board | 43 |
|
Acute trust |
35 |
|
Mental health trust |
24 |
|
Community trust |
19 |
|
Ambulance trust |
18 |
Scoring and contextual metrics
Each metric is defined status as scoring or contextual.
Scoring metrics are based on robust established data and are used to determine an organisation’s overall segment. Contextual metrics provide additional information but are not scored and do not form part of segmentation. This is usually because the data is not yet of sufficient quality to be used consequentially, cannot be used to make comparative judgements due to external factors (such as demographics) or the metric considers an area that is not fully within the organisation’s direct control.
Domain 1 – Population health, prevention and reducing inequality
|
Subject area |
Metric |
Applies to |
Status |
|
Population health |
Under 75s cancer mortality rate |
ICBs |
Contextual |
|
Population health |
Under 75s cardiovascular disease mortality rate |
ICBs |
Contextual |
|
Preventing ill health |
Cervical screening rate |
ICBs |
Scoring |
|
Preventing ill health |
Bowel screening rate |
ICBs |
Scoring |
|
Preventing ill health |
Breast screening rate |
ICBs |
Scoring |
|
Preventing ill health | MMRV (measles, mumps, rubella and varicella) uptake rate |
ICBs |
Scoring |
|
Preventing ill health |
% of eligible people supported by obesity prevention programmes |
ICBs |
Scoring |
|
Preventing ill health |
% of inpatients making a supported quit attempt with an in-house tobacco dependence treatment service |
Trusts |
Scoring |
|
Preventing ill health |
% of pregnant women who quit smoking |
ICBs |
Scoring |
|
Reducing inequality |
Deprivation gap in early cancer diagnosis |
ICBs |
Scoring |
|
Reducing inequality |
Deprivation and ethnicity gap in pre-term births |
ICBs |
Scoring |
|
Reducing inequality | Deprivation gap in lipid management |
ICBs |
Scoring |
| Reducing inequality | Deprivation gap in hypertension management | ICBs | Scoring |
Domain 2A – Allocating resources
|
Subject area |
Metric |
Applies to |
Status |
|
Elective care |
% change in overall waiting list size versus previous year |
ICBs |
Scoring |
|
Community care |
Level of growth in community care contacts |
ICBs |
Scoring |
|
Cancer care |
% of cancers diagnosed at stage 1 or 2 |
ICBs |
Scoring |
|
Mental health care | % of acute adult mental health admissions with no contact with community mental health services in the previous year |
ICBs |
Scoring |
|
Urgent care |
Occupied bed days per 100,000 head of population |
ICBs |
Scoring |
|
Primary care | % of clinically urgent appointments that happen on the same day |
ICBs |
Scoring |
|
Dental care | Units of dental activity delivered as a % of commissioned |
ICBs |
Contextual |
| Learning disabilities and autistic people | Percentage of people with a learning disability and autistic people in mental health hospital with the longest length of stay | ICBs | Contextual |
Domain 2B – Access to services
|
Subject area |
Metric |
Applies to |
Status |
|
Elective care |
% of patients waiting up to 18 weeks for care |
Trusts |
Scoring |
|
Elective care | % of cases waiting up to 18 weeks for care versus target |
Trusts |
Contextual |
|
Elective care |
% of patients waiting over 52 weeks for care |
Trusts |
Scoring |
|
Elective care |
% of patients waiting less than 18 weeks for community care |
Trusts |
Scoring |
|
Diagnostics |
% of diagnostic referrals waiting over 6 weeks |
Trusts |
Scoring |
|
Cancer care | % of cases meeting the 28 day faster diagnosis standard |
Trusts |
Scoring |
|
Cancer care | % of cases treated within 62 days of referral |
Trusts |
Scoring |
|
Urgent care |
% of patients admitted, discharged or transferred within 4 hours |
Trusts |
Scoring |
|
Urgent care |
% of patients spending over 12 hours in department |
Trusts |
Scoring |
|
Urgent care |
Mean response time to category 2 calls |
Trusts |
Scoring |
|
Urgent care |
Mean 999 call response time |
Trusts |
Scoring |
|
Mental health care | % of total children and young people’s mental health waits for help that are over 104 weeks |
Trusts |
Scoring |
|
Mental health care | % of people discharged from community mental health services with a paired outcome score recorded (all ages) |
Trusts |
Scoring |
Domain 3 – Experience of care
|
Subject area |
Metric |
Applies to |
Status |
|
Experience |
CQC inpatient survey satisfaction rate |
Trusts |
Scoring |
|
Experience |
CQC community mental health survey satisfaction rate |
Trusts |
Scoring |
|
Experience | % of patients rating their experience of GP access as easy |
ICBs |
Scoring |
|
Experience |
% of patients with a preferred general practice professional able to see that professional |
ICBs |
Scoring |
|
Experience |
NHS staff survey advocacy rate |
All trusts |
Scoring |
|
Experience |
% of complaints open beyond 6 months |
ICBs |
Scoring |
|
Patient flow | 12 month adult admission rate for people with a learning disability and autistic people |
ICBs |
Contextual |
|
Patient flow |
Number of patients cared for in corridors |
Trusts |
Contextual |
|
Patient flow | % of ICB commissioned adult inappropriate out of area placement bed days as a proportion of all ICB commissioned bed days |
ICBs |
Scoring |
|
Patient flow | Mean length of stay for adult acute mental health and psychiatric intensive care unit patients |
Trusts |
Scoring |
|
Patient flow | Mean length of stay for older adult acute mental health patients |
Trusts |
Scoring |
|
Patient flow |
% of intermediate care beds occupied by patients without criteria to reside |
Trusts |
Scoring |
|
Patient flow |
Average number of days between discharge ready and actual discharge date |
ICBs |
Scoring |
Domain 4 – Effectiveness of care
|
Subject area |
Metric |
Applies to |
Status |
|
Outcomes |
Summary Hospital Mortality Indicator |
Trusts |
Scoring |
|
Outcomes |
Rate of pregnant women with a delayed planned induction per 1,000 deliveries |
Trusts |
Scoring |
|
Outcomes |
% of NHS Talking Therapies patients completing a course of treatment and achieving reliable recovery |
ICBs and Trusts |
Scoring |
|
Outcomes |
% of incidents managed via hear and treat or see and treat |
Trusts |
Scoring |
|
Outcomes |
% of people with 3 or more emergency admissions in the last 90 days of life |
ICBs |
Scoring |
|
Outcomes |
% of acute and rehabilitation adult discharges followed up within 72 hours |
Trusts |
Scoring |
|
Outcomes |
Over 65s bed days per 100,000 head of population |
ICBs |
Scoring |
|
Effective discharge |
30-day readmission rate band |
Trusts |
Scoring |
|
Effective discharge |
Mental health 14-day readmission rate |
Trusts |
Scoring |
|
Managing long term conditions |
% of patients who receive all 8 diabetes care processes |
ICBs |
Scoring |
|
Managing long term conditions |
Number of patients with GP recorded cardiovascular disease whose cholesterol is managed to NICE guidance |
ICBs |
Scoring |
|
Managing long term conditions |
Number of patients with GP recorded hypertension whose blood pressure is managed to NICE guidance |
ICBs |
Scoring |
|
Managing long term conditions |
% of patients on GP severe mental illness registers to receive a full physical health check in the last 12 months |
ICBs |
Scoring |
|
Managing long term conditions |
% of patients over 14 years old on GP learning disability registers to receive a full physical health check and action plan in the last 12 months |
ICBs |
Scoring |
Domain 5 – Patient safety
|
Subject area |
Metric |
Applies to |
Status |
|
High quality care |
Breadth and depth of clinical audit outliers |
Trusts |
Scoring |
|
High quality care | Urgent crisis response within 24 hours |
Trusts |
Scoring |
|
Safe practice |
Percentage of children aged 9 and under prescribed antibiotics |
ICBs |
Scoring |
|
Safe practice |
Crude rate of restrictive interventions per 100,000 bed days |
Trusts |
Contextual |
|
Safe outcomes |
Number of cases of MRSA in the last 12 months |
Trusts |
Scoring |
|
Safe outcomes |
Rate of e-coli |
Trusts |
Scoring |
|
Safe outcomes |
Rate of c-difficile |
Trusts |
Scoring |
|
Safe outcomes |
Number of neonatal deaths and stillbirths per 1,000 total births |
ICBs |
Scoring |
|
Safe outcomes |
Rate of inpatient falls that cause harm |
Trusts |
Contextual |
|
Safe outcomes | % of patients to acquire a new grade 3 or 4 pressure ulcer |
Trusts |
Contextual |
|
Safe outcomes | % of safety incidents resulting in harm |
All trusts |
Contextual |
|
Safe culture |
NHS staff survey raising concerns sub-score |
All trusts |
Scoring |
Domain 6 – Finance, productivity and innovation
|
Subject area |
Metric |
Applies to |
Status |
|
Finance |
Planned surplus or deficit |
All organisations |
Scoring |
|
Finance |
Variance to plan year-to-date |
All organisations |
Scoring |
|
Productivity |
Relative cost difference (National Cost Collection Index) |
All trusts |
Scoring |
|
Productivity |
Implied productivity growth |
All organisations |
Contextual |
|
Innovation | % of clinical trials set up within 90 days |
All organisations |
Scoring |
|
Innovation |
Data Quality Maturity Index |
All trusts |
Scoring |
Domain 7 – People
|
Subject area |
Metric |
Applies to |
Status |
|
People and culture |
Sickness absence rate |
All organisations |
Scoring |
|
People and culture |
NHS staff survey engagement theme score |
All organisations |
Scoring for trusts
Contextual for ICBs |
|
People and culture |
National education and training survey satisfaction rate |
All trusts |
Scoring |
|
People and culture |
NHS staff standards score |
All trusts |
Scoring |
|
People and culture |
Healthcare worker flu vaccination rate |
All trusts |
Scoring |
|
Workforce |
GP headcount per capita |
ICBs |
Scoring |
|
Workforce |
Temporary staffing cost relative band |
All trusts |
Scoring |
Publication reference: PRN02437