
Publication reference: PR2040
Background
Commissioning is described by NHS England as “the continual process of planning, agreeing and monitoring services. Commissioning is not one action but many, ranging from the health-needs assessment for a population, through the clinically based design of patient pathways, to service specification and contract negotiation or procurement, with continuous quality assessment”. This description reflects the broad range of skills and knowledge required by those who perform these functions – whether based in integrated care systems, provider collaboratives, NHS England, or another structure.
We also know that commissioning care for autistic people and people with a learning disability can be more complex than commissioning care for other population groups. Rather than commissioning episodic care, block/bed-based services, or treatment, these groups of people often need a ‘whole life approach’ which is flexible, personalised and based on enabling each person to become and be recognised as a valued citizen.
To reflect the complexities of commissioning for people with a learning disability and autistic people, there is now a specific training offer to support people who commission services for autistic people and people with a learning disability. This training has been well received by people who have completed it and this guide is intended to supplement the training offer.
Through the training we have been made aware of several scenarios which the guide will help to address:
- New commissioners (or people who are newly undertaking these functions) who have taken up these responsibilities following the introduction of ICSs.
- People undertaking commissioning functions who do not recognise themselves as commissioners therefore may have had limited support or training resources.
- Experienced commissioners who have recently begun working in the area of autism and learning disability, who have a wide knowledge of commissioning but not for people with a learning disability and autistic people.
The introduction of integrated care systems has resulted in a shift in the health and social care landscape, and a change to roles and responsibilities across a range of areas. Commissioning is a function which has been impacted by these changes.
This guide draws together a number of resources and provides a one stop shop for professionals who put in place services and approaches to support children, young people and adults who have a learning disability or who are autistic to lead healthier, happier lives.

This is a Venn diagram showing three interlinking, and overlapping, circles. The image is taken from the National Service Model which was published in 2015. Each circle describes a type of commissioning function.
Circle one shows individual, or micro, commissioning where support is commissioned at an individual or patient level. Examples of people involved in this type of commissioning are shown as the person, their family, the social worker, and a nurse.
Circle two shows strategic commissioning where support is commissioned at a population level. Examples of people involved in this type of commissioning are shown as a clinical commissioning group, a local authority, NHS England, joint commissioners and health and wellbeing boards. Since the National Service Model was published, integrated care systems have replaced clinical commissioning groups.
Circle three shows operational commissioning where support is commissioned for a specific client group. Examples of people involved in this type of commissioning are shown as local commissioners, and contract and procurement officers.
The model
In 2015, NHS England, Association of Directors of Adult Social Services and the Local Government Association published a national plan to develop community services and close inpatient facilities for people with a learning disability and autistic people who display behaviour that challenges, including those with a mental health condition.
Although terminology has changed, the principles within this model to improve community services for autistic people and people with a learning disability still stand.
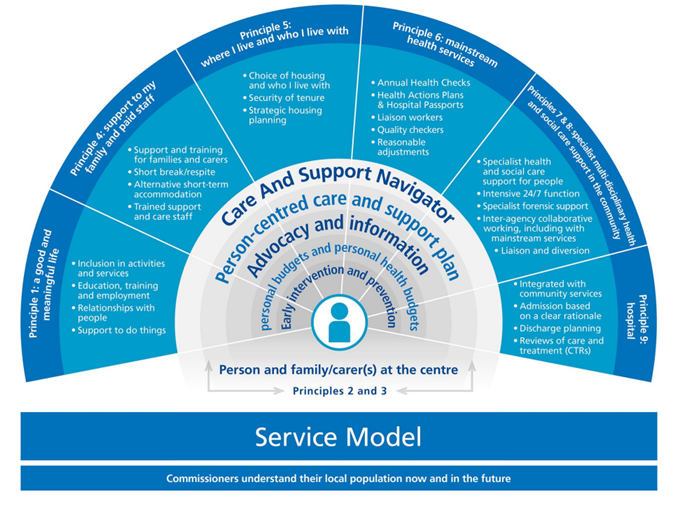
This image has been adapted from the Building the right support guidance published by NHS England in 2015. It visually shows the National Service Model. The image is of an arc with nine principles.
The image shows that the person and their family carer(s) should always be at the centre. It shows enablers to this as being a care and support navigator, person –centred care and support plans, advocacy and information, personal budgets and personal health budgets, and early intervention and prevention.
Underpinning the arc are two key principles – that commissioners understand their local population now and in the future, and that there is sufficient workforce capacity. This is described as ‘the right people with the right values, behaviours, skills, capacity and capability to deliver high quality care and support for people with a learning disability and autistic people’.
The principles and support services within the arc are:
- I have a good and meaningful life.
- Support to my family and paid staff.
- Where I live and who I live with.
- Mainstream health services.
- Specialist multidisciplinary teams and social care support in the community.
To support provision being delivered in line with this model, this guide includes 11 sections – the top ten essentials and a section for useful resources. These sections are:
- Citizenship and human rights
- Language
- Use the expertise of the people with lived experience – involvement and coproduction
- Commissioning for people’s lives and not just a service
- Commissioning skills and capability – national support
- Know your population
- Housing: getting a home
- Workforce
- Market shaping and community capacity
- Commissioning oversight
- Useful resources
1. Citizenship and human rights
Citizenship
Children and adults with a learning disability and autistic children and adults are entitled to live fulfilling lives with dignity and respect, empowered and enabled to make their own choices by commissioners who understand the unique qualities needed to commission ‘for living life’. Simon Duffy’s Seven keys to citizenship are a useful resource for understanding what citizenship means. Duffy says that there are seven keys: love, freedom, life, meaning, home, money and help.
Human rights
Systems must offer access to high quality, effective housing, care and support, which meets the personal choices, expectations and aspirations of children and adults with a learning disability, and autistic people, and their families and carers.
Impact on commissioning practice
Commissioning therefore should be about:
- Enabling the right to life, a life with purpose, relationships and aspirations.
- Enabling personal choice, the right to say ‘no’.
- Enabling liberty, and freedom from inhuman or degrading treatment.
- Treating everyone with fairness and respect.
Further Information
Information about human rights can be found on the British Institute of Human Rights website.
Information about the Seven keys to citizenship is available on the Citizen Network website.
2. Language
The words we use matter – a lot!
We often use different words to describe disabled people and the services that they use.
Words like ‘cohort’, ‘placement’, ‘accessing the community’ or ‘unit’.
These words are not commonly used to describe how non-disabled people live their lives.
Words like these come about by often looking through a narrow service lens.
People with lived experience tell us that they feel trapped in ‘Service Land’ which makes it really hard to be a citizen, be seen as equal to non-disabled people and be described like everyone else.
Challenging Behaviour
‘Challenging behaviour’ is not acceptable language. It does not consider the function or reason for the person behaving as they are and puts the blame on the person. It is shorthand for lots of different things, so it is not always clear what the phrase means.
All behaviour is communication and so it is important to understand if someone is distressed or in pain and is communicating that.
If someone is a risk of hurting themselves, say that.
If someone is distressed, say that.
People are not service users, clients, patients, beds, LD or numbers – labels are for clothes, people are just people.
Further Information
Advice on words to use and words to avoid can be found on our website.
3. Use the expertise of the people with lived experience – involvement and coproduction
Nothing about us, without us
Since the publication of Valuing people (2001) and reports that have followed, the phrase ‘Nothing about us, without us’ has been a key principle when delivering services for people with a disability and more broadly. Inclusion of people when commissioning services is key in ensuring the right provision is developed, and that it is working well.
Putting it into practice
Make sure the housing, care and support that is put in place is what is needed by the people it is for. Listen to all the people who are being supported with housing, care and support to make sure you get things right.
Think about who you are not yet hearing from and link to organisations and people who can help you hear what they need. These are some of the ways to help connect with people:
|
Ways to involve people and families |
Resources |
|
Ask for feedback and act on concerns and complaints in services – use this in contract management | |
|
Run focus groups – go out and ask people what they think needs to change | |
|
Set up your own coproduction group and/or commission local groups to get involved to help shape services |
Links to local groups like parent carer forums and self-advocacy groups |
|
Employ people with lived experience to work with you. |
4. Commissioning for people’s lives and not just a service
Homes not hospitals
Traditional NHS commissioning is episodic – we are good at putting in place services to ‘fix’ people if they are unwell.
People with a learning disability and autistic people are not broken and don’t need fixing, but they may need care and support in order to live their life as a citizen.
There will be times when people may require care and treatment in a hospital setting. However, people are clear they want homes, not hospitals. And homes, jobs, relationships and ambitions can and will change as people go through life.
What do we need to do differently?
- Start with the person and their family or loved ones – personalised, person centred.
- Develop and maintain good conversations and relationships with the person and their family and loved ones.
- Ask what their hopes, dreams and aspirations are, as well as their needs, and work with them to try and make these happen.
- Make an effort to understand the person’s story, their past and how this has shaped their present.
- Enable maximum choice and control for the person and use personalised approaches.
- Ensure that you are providing the ‘least restrictive options’ and bear in mind that might mean dealing with some risks/worries but you should not be giving more service than people need or want.
- Work to create the conditions where advocacy can flourish so that people are enabled to have a voice.
- Make sure that people sort out problems so there is an environment where things can happen, rather than a focus on the problems.
- Aim towards supporting as normal a life as possible with room to grow and develop, especially at key transition times – life isn’t static.
5. Commissioning skills and capability – national support
Commissioning qualification
- The commissioning qualification is a funded opportunity for social care and health commissioners across England.
- It is specifically for people who commission services which support people with a learning disability and autistic people.
- Applications and access to frequently asked questions are available on the Skills for Care website.
Other support available
- Universal personalised care contains a range of tools, approaches and support for commissioners to enable choice and control.
- Commissioning services for autistic people – a cross-system framework for commissioning social care, health and children’s services for autistic people (Skills for Care, 2021)
- Commissioning services for people with a learning disability – a cross-system framework for commissioning social care, health and children’s services for people with a learning disability (Skills for Care, 2021)
- A shared commitment to quality: for those working in health and care systems (National Quality Board, 2021)
6. Know your population
Dynamic support registers (DSRs)
Dynamic support registers are essential to understanding your children, young people and adult population and their needs.
Registers must include:
- Children, young people and adults at immediate risk of admission (rated red).
- Children, young people and adults who will become at risk of admission without urgent intervention (rated amber).
- Autistic children, young people and adults in the categories above who do not have a learning disability and may not be known to traditional services.
- Children, young people and adults who are currently inpatients (rated blue).
Care (Education) and Treatment Reviews (C(E)TRs)
DSRs should also be linked to your Care (Education) and Treatment Reviews. There must also be a link between the registers and the key themes from community C(E)TRS and the use of children’s keyworkers. Further information about these reviews is available on our website.
Safe and wellbeing reviews
The outcomes from the individual safe and wellbeing reviews (2021/22) can also help you to have a better understanding of your population and the support that people may need.
Doing a needs analysis
Use information from a range of relevant local sources to help you ensure that you are basing your decisions about planning services and meeting needs on the best evidence/you can check that different sources are consistent with each other/you can identify any gaps in your analysis.
It is important to assess that the data is up to date/relevant/from a reliable source. You may have to commission some research if there are gaps in the data.
We suggest it is useful to look at the below data sources, where available to commissioners within confidentiality parameters. You may also be able also access other datasets relevant to people with a learning disability and autistic people.
- Local intelligence/reporting – including via contract management processes.
- Disabled children’s registers (a legal requirement that each local authority holds a register).
- Special Educational Needs and Disability (0-25 years) data – education, health and care plans, the local offer, those not in education or employment teams
- Local joint strategic needs assessments.
- Local housing needs assessment data.
- GP learning disability registers.
- Health, for example waiting list data
- Information from parent carer forums, self-advocacy groups, learning disability partnership boards, people’s Parliaments etc.
7. Housing: getting a home
Many people can source their own housing solutions, sometimes with the help of their families. When this is not the case, commissioners may need to help the person, working closely with local housing partners. This section is designed to support commissioners to “ensure people get the help to find, adapt or maintain a home which is right for them”.
A true home (rather than a residential placement) can provide security, stability and promote health and wellbeing, preventing admissions to hospital and enabling people to be discharged from hospital into a home which is right for them.
Key messages on housing
What do we mean by housing? Many have observed that ‘every decision about health and care is a decision about housing’. However, helping people to get a home is not the responsibility of a single organisation or body, and many partners will be involved, including:
- local authority housing departments/strategic housing leads/housing options leads/housing benefit leads
- local authority planning teams (who prepare the local plan which sets planning policies in a local authority area)
- registered providers of housing/social housing providers, including specialist and supported housing providers
- occupational therapists who can advise people on equipment and adaptations to help them live as independently as possible, and voluntary organisations and housing providers who help to deliver home repairs and adaptations in the community
- more broadly, private landlords, construction industry.
Housing needs to be brought into the conversation about people’s needs at the earliest opportunity.
Commissioners need to do due diligence on housing providers as much as they would on care providers.
Local systems must explore sources of capital funding (actual or in kind) for housing, alongside revenue. This could include funding from the Affordable Homes Programme, private sources of funding via housing providers or local authorities, recycling of public land, funding generated via local planning obligations, and NHS England capital funding.
Housing timescales
Timescales for delivering quality affordable housing could be:
- at least six months for acquisitions and nearer nine to 12 months where work is required
- 12 to18 months for remodelling and refurbishment of empty properties
- Up to 24 to 30 months for new builds – from concept to delivery.
In order to meet people’s housing needs, a strategic housing needs assessment is essential. This is needed to support strategic planning for local housing needs, which is led by local authority strategic housing leads, working closely with local planners. Social care and NHS commissioners should work proactively with housing partners to help identify the housing need for autistic people and people with a learning disability, including those people in hospital, and co-develop a housing delivery plan to meet that need. This should be underpinned by an excellent understanding of people’s own housing aspirations, based on meaningful partnership with people and families. Other key local partners include housing providers, especially those with expertise in providing specialist or supported housing, and local authority housing benefit teams, who will be able to advise on whether proposed rent levels are judged to be reasonable (and thus can be covered by housing benefit). Key areas which will help to deliver housing solutions include:
- Support to increase knowledge and confidence around housing options
- Up front risk sharing (for example around voids) will help reduce the risk longer term.
- Relationships are key to delivering new sustainable housing solutions.
- Accommodation planning should start within 14 days of a person’s admission to a mental health hospital.
Further Information
Information, help and advice, including contact details for NHS England regional housing leads, can be obtained from the following locations:
- NHS England learning disability and autism housing pages
- NHS England/Local Government Association/Association of Directors of Adult Social Services joint guidance, Building the Right Home (2016).
- Housing LIN – housing and learning disability pages
- Local Government Association: Housing for people with a learning disability or autistic people
8. Workforce
Workforce is described as: “The right people, with the right values, behaviours, skills, capacity and capability to deliver high quality care and support for people with a learning disability and autistic people”.
Key workforce pointers
- Are there workforce plans in place? Local/system level, evidence?
- What is the workforce requirement (skills) to meet the required needs?
- What roles (may also include paid/unpaid) are required? Are these qualified, clinical, skilled? Can these meet the need?
- Is the workforce trained/skilled to do their job? Does this include agency workers? Do you have evidence of training?
- Are there appropriate and safe workforce levels (see the NHS improvement standards)
- Is the workforce representative/inclusive of the population, with sufficient cultural competency?
- Has the training been co-designed/co- produced?
- Is all training aligned to core capability frameworks, and do you have evidence of this?
- During the commissioning cycle there are contract review points – this presents an opportunity to collate any workforce transformation/risks amendments and take action/review next steps?
Trigger points which might make you want to look more closely at workforce
- High percentage of agency, high sickness/turnover, challenges attracting, recruiting and retaining people.
- Areas of concern linking to Care Quality Commission’s (CQC’s) five key questions and specifically question five: Are they well-led? “By well-led, we mean that the leadership, management and governance of the organisation assures the delivery of high-quality and person-centred care, supports learning and innovation, and promotes an open and fair culture” (CQC 2022).
- Unable to demonstrate talent and succession planning pipeline and no evidence of training needs assessment for the workforce.
Assurance
- Are you assured that the correct workforce is in place, with the right values and skills?
- How and where are workforce transformation and risks reported, escalated and managed?
- How and where are feedback/quality outcomes linked to workforce needs and how are changes implemented and monitored?
9. Market shaping and community capacity
How to support the provision of creative community options and develop and shape markets
Cross system conversations with partners are the best way to develop a cross system strategy where we are all working towards developing and shaping health, housing and social care markets locally and nationally.
Things that can help:
- Ensure there is a full understanding of all providers from all sectors in the locality and what they are able to offer.
- Engage with people with lived experience to fully understand what services are wanted and needed.
- Explore how gaps in the market may be addressed, have conversations with providers on how they may be able to address these gaps.
- Think differently: how can individual service funds and personal budgets be used to best support person centred care?
- Explore how small/micro providers can support diversity in market provision.
- Look at things like market position statements and wider market development to understand how you can influence what sort of provision is needed.
National support available
Small Supports: A programme designed to grow small, person centred organisations to support people with ‘hefty reputations’ live in the community. Over the last three years this programme has also established a network of existing and emerging small supports organisations and a commissioner network.
Peer reviews and intensive support: Based on sector led improvement methodology used in local government. A team of people with a range of experience (including those who have lived experience of receiving care and support) are invited into a local system as critical friends, to hold up the mirror and identify strengths and areas of improvement including shaping and developing services to support their community. Intensive support can then be offered to an area to help them implement any changes.
10. Oversight
Commissioners are responsible for ensuring oversight of the quality and safety of any care and support that they commission provided for people with a learning disability and autistic people. For those people in who are in a mental health inpatient care setting, there is specific guidance which sets out the responsibilities of commissioners in terms of quality oversight.
Host commissioner arrangements
Host commissioner guidance supports quality and patient safety where inpatient care is delivered. The host commissioner arrangements are based around the locality of the inpatient unit and are the mechanism to oversee and co-ordinate local activity relating to quality oversight, setting out responsibilities for co-ordinating any responses to serious concerns. These arrangements are key in underpinning system wide collaborative working in respect of quality oversight and promoting excellence in care. A host commissioner forum has also been set up to enable commissioners to share good practice.
Commissioner oversight visits
Commissioner oversight arrangements with supporting guidance sets out a framework for regular visits that will help to ensure commissioners are engaged with the people for whom they commission care, are checking to make sure that the care is of good quality and is beneficial to the person, and are able to work towards effective assessment and treatment and a more rapid discharge back into the community. People and their families are at the heart of these arrangements, with their input being a key part of the feedback and continued discussion relating to the care being received, and future-plans for discharge.
Care, (Education) and Treatment reviews (C(E)TRs)
Commissioners are responsible for C(E)TR’s taking place, in line with the guidance, at various points – both pre-admission and whilst a person is in an inpatient setting. Ensuring the CETR takes place is the responsibility of the person commissioning the care of the person in hospital, or of the integrated care board if the person is living in the community. There is guidance in place to support commissioners to put in place CETRs, and which sets out the responsibilities of all partners who are involved.
11. Useful resources
NHS policy documents
- Building the right support (2015)
- Building the right home (2016)
- National service model (2015)
- Service model specifications (2017)
- NHS Long Term Plan (2019) – learning disability and autism
- Government Plans Building the right support action plan (2022)
Health improvement resources
- NHS Improvement (2018): The learning disability improvement standards for NHS trusts
- Learning from lives and deaths – people with a learning disability and autistic people (LeDeR) annual report 2021
Workforce and training
- Health Education England star and star user guide
- Guidance for the production of transforming care partnership workforce plans
- How can we build the right workforce
- Skills and competency frameworks