
Overview of underpinning principles and key ideas
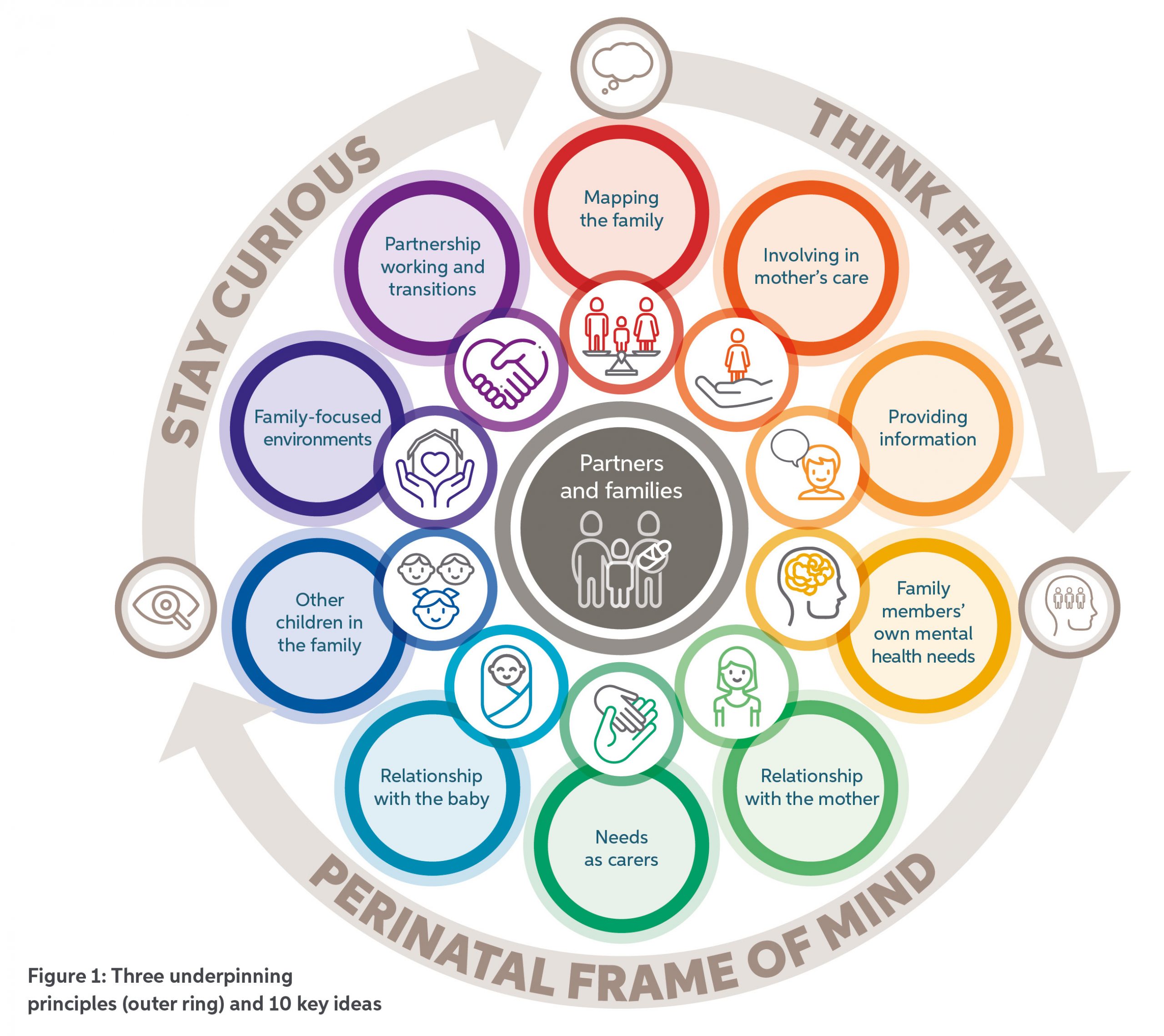
The good practice guide incorporates three underpinning principles and ten key ideas. These are shown in Figure 1.
The underpinning principles build on existing concepts for working with families, while the ideas have been developed through research as part of the development of this guide. The individual ideas are intended to be understood and actioned with these underpinning principles in mind, alongside compliance with local and national safeguarding procedures and NHS Trust information governance.
The ‘Think Family’ ethos needs to be embedded throughout services, with all members of the workforce adopting the Perinatal Frame of Mind. To ensure inclusivity and address inequalities, we need to ‘Stay Curious’.
Involving partners and other family members in a mother’s care must be respectful of the mother’s wishes and sensitive to the family’s individual culture. This is informed by mapping the family at early contacts and continuing to keep conversations open about who might be involved in her care. To adequately support partners and other family members, their multiple roles and relationships require recognition: their own mental health needs, their relationship with the mother, their relationship with the baby, and their needs as carers.
The needs of other children in the family also warrant identification and support. To deliver on meeting the needs of the wider family unit, and to provide interventions which target relationships and family systems as well as mothers’ individual mental health symptoms, it is important that specialist perinatal mental health services provide family-focused environments, work in partnership with other services and attend to continuity across critical transition points in the mother’s care.
A note on language
Language is powerful. Mental health services need to use language that is inclusive, non-stigmatising and not based on assumptions. In particular, the language used should recognise varied family forms, cultural considerations, and the multiple connections within families.
Within perinatal mental health services, a wide range of people may be involved and supported in relation to a mother and baby. For example, they may be involved as partners and as parents, as young carers and as siblings, and as parents’ parents or grandparents.
In this guide, we recognise the diversity of families using specialist perinatal mental health services. For simplicity this guide uses the following terms:
Mother
Refers to the ‘index’ patient of the specialist perinatal mental health service, who is pregnant or has given birth. This may include a trans man or non-binary person.
Partner
Refers to the person identified by the mother as their partner. This could be any co-parent including a father, co-mother or co-father.
Father
Refers to the person identified as the father of the baby, regardless of biological connectedness or parental responsibility. Much of the evidence base relates specifically to fathers and we use ‘father’ whenever we are describing this evidence.
Other family members
Refers to anyone else in the family network who is significant to the mother. This could for example be the baby’s grandparents, aunts, uncles, and siblings. It could also include close friends.