
Metacarpal wrong site surgery – inconsistent terminology used to describe anatomy
Through its review of recorded patient safety events, the National Patient Safety Team identified issues where the wrong joint was operated on due to inconsistencies in how finger digits were described and site marked.
The team reviewed a Serious Incident report describing a patient where the wrong carpometacarpal joint was operated on because the terminology used to describe the digits of the hand are not consistent nationally. The nomenclature for fingers is complex as there are different ways of identifying a finger digit, for example by name or by number. There are also several joints in a hand and there are many different types of procedure that can be carried out on these bones and joints. There is no national guidance to provide clarity around consistent terminology that should be used when site marking fingers and toes before surgery.
As a result, the British Society for Surgery of the Hand (BSSH) has agreed to add a section in the BSSH Framework on the nomenclature and site marking of digits in relation to consent and best practice. Finger digits should be identified by name not number followed by the individual bone or joint, for example, ‘ring finger metacarpal’. It has also been agreed that this should be shared with the British Orthopaedic Foot and Ankle Society so that similar guidance can be developed for toe surgery. Consistency in nomenclature should reduce the potential for confusion during surgery.
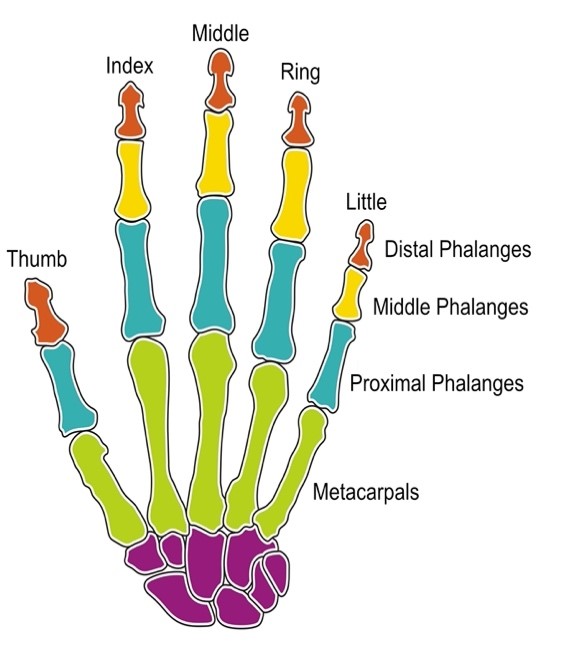
Illustration of bones in the hand.
About our patient safety review and response work
The recording and central collection of patient safety events to support learning and improvement is fundamental to improving patient safety across all parts of NHS healthcare. The National Patient Safety Team identify new or under recognised patient safety risks, which are often not obvious at a local level. It does this through its core work to review patients safety events recorded on national systems, such as the National Reporting and Learning System (NRLS), the new Learn from Patient Safety Events service (LFPSE), and other sources.
In response to any newly identified risks, we develop advice and guidance, such as National Patient Safety Alerts, or work directly with partners as in the example above, to support providers across the NHS to take the necessary action to keep patients safe.
You can find out more about our processes for identifying new and under recognised patient safety issues on our using patient safety events data to keep patients safe and reviewing patient safety events and developing advice and guidance web pages.
You can also find more case studies providing examples of this work on our case study page.