
Introduction
This urgent and emergency care (UEC) acute patient flow clinical and operational improvement guide provides a range of change ideas for how UEC services can improve both patient care and productivity, with the 2 principal aims of:
- making care safer and patient experience better by increasing the adoption of evidenced best practice
- maximising the value of patients’ and clinicians’ time and the productivity of services by tackling waste and addressing inefficient processes
We know, for example, that patients who stay in the emergency department (ED) for more than 6 hours have a higher risk of dying within 30 days. A length of stay (LoS) of 10 days or more results in serious deconditioning and loss of muscle mass. With more than 1 in 10 patients in 2023/24 staying in ED for longer than 12 hours, and 20% of G&A beds consistently occupied by patients with a 21+ days LoS, improving flow is critical to improving the quality and safety of care.
The improvement ideas in this guide are intended to be supportive, particularly for winter planning. Those closest to delivering care should be supported with senior sponsorship to apply improvement methods to test, adapt and build on the ideas for your local context. Ensuring improvement work uses the 5 universal flow principles as the basis for making changes will help gain traction with teams and provide a framework through which to capture hearts and minds in this important work.
This guide identifies the current evidence of the most impactful interventions that can create greater value for patients and more productive services. However, we would invite teams and organisations to build on this guide with their own creativity and ideas.
The guide does not stand alone. It forms part of a suite of tools and interventions that will be released over the coming months to support clinical and operational teams. One such tool is improvement analytics that equip teams with the resources to diagnose issues and identify opportunities to improve care and to track improvement over time. The tool also includes dashboards to help people see how improvements are being realised over time and enable them to see how they compare to others.
The overall improvement work has two principle aims:
- make care safer and patient experience better by increasing the adoption of evidenced best practice
- maximise the value of patients and clinicians’ time and the productivity of services by tackling waste and addressing poor processes.
Universal flow principles
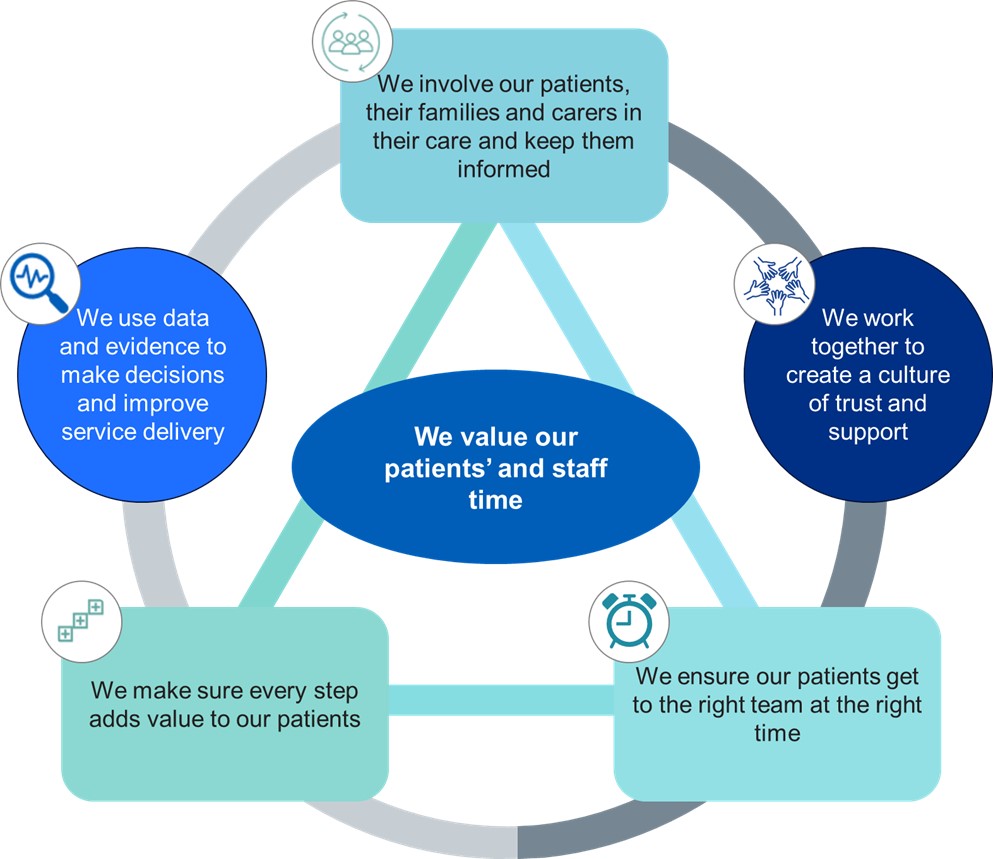
The diagram below describes the key principles of valuing patients’ and staff time in UEC flow.
- we involve our patients, their families and carers in their care and keep them informed
- we work together to create a culture of trust and support
- we ensure our patients get to the right team at the right time
- we make sure every step adds value to our patients
- we use data and evidence to make decisions and improve service delivery
- we value our patients’ and staff time
This guide is part of a suite of tools and interventions that will be released over the coming months to support clinical and operational teams. In particular, the improvement analytics tool in the Model Health System will bring together the tracking indicators referenced in this guide. These indicators cover a range of process, outcome and quality metrics that trusts and systems can use to diagnose issues, identify opportunities to improve care and to track improvement over time. The improvement analytics tool also includes dashboards to help you see how improvements are being realised over time and how you compare to others.
We want to understand how this guide works for you and your teams, and how we can further develop and improve it to make it as useful as possible to support local improvement programmes. Therefore, this is an interim guide – our intention is it will be refined, developed and updated as we learn what works through your teams. Please share your thoughts on the guide and your ideas to include in it – details on how to do this are at the end of this guide.
UEC flow driver diagram
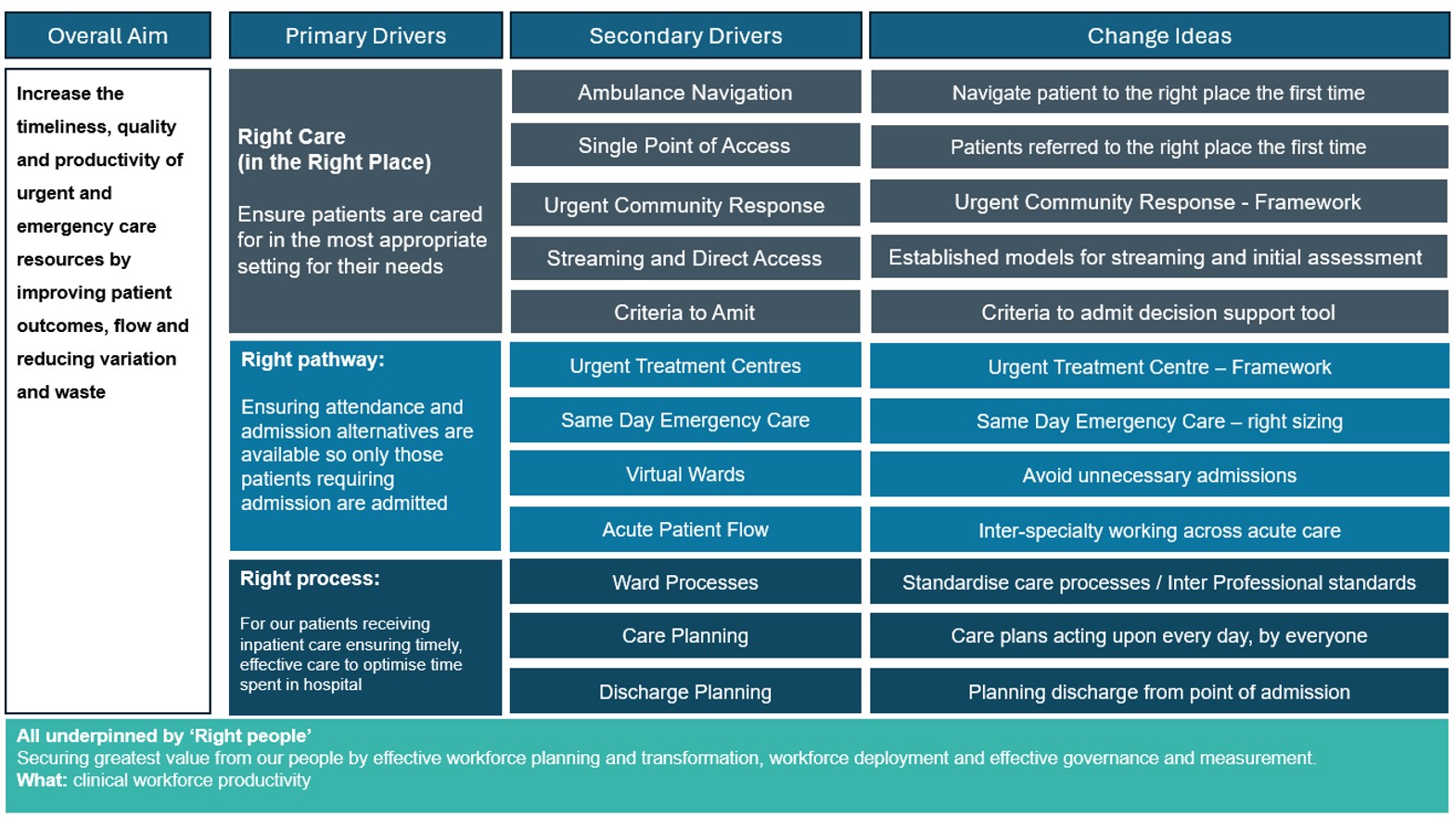
The driver diagram below set out the key elements that are needed to ensure patients are cared for in the most appropriate setting and have an appropriate plan in plan. As well as optimising processes and securing the greatest value from our people.
UEC driver diagram
Click here to access an accessible description of the driver diagram:
Overall aim
Increase the timeliness, quality and productivity of urgent and emergency care resources by improving patient outcomes, improving flow and reducing variation and waste.
Primary drivers
- Right care, right place: ensure patients are cared for in the most appropriate setting for their needs
- Right pathway: Ensuring attendance and admission alternatives are available so only those patients requiring admission are admitted
- Right process: Patients receiving inpatient care, ensuring timely, effective care to optimise time spent in hospital
- Right people: securing greatest value from our people
Areas of focus
- Keeping patients out of hospital that do not need admission: Ambulance navigation, single point of access, urgent community response, streaming and direct access and criteria driven approach regarding decision to admit
- Alternatives to admission: reduce reliance on admitted care by increasing the use and impact of alternative care models including urgent treatment centres, same day emergency care, virtual wards, patient flow initiatives
- Standardised process: increase the use and optimise the impact of Internal Professional Standards (IPS) 7-days a week, across all services and specialities
- Care and discharge planning: create and enact comprehensive care and discharge plans in partnership with patients and carers
- Workforce planning and deployment
- Workforce transformation
- Governance and measurement
Change ideas
- Navigate patients to the right place the first time
- Establish clear models for streaming and initial assessment
- Run Criteria to Admit as a live tool for confirming patient admissions
- Team job plans that support early review of patients by senior clinician
- Extend CTA to residents & other HCPs with senior oversight
- Ensure use of CTA by senior decision maker at the point of attendance
- Use CTA audits to confirm capacity required in alternatives to admission
- Run CTA for admitted patients at 24hr to determine fitness for discharge
- Implement 10 core components of the Virtual Wards Operational Framework
- Ensure virtual wards link with SPoAs/ICC, SDEC, UCR, 999/111, care homes
- Scale virtual ward capacity to deliver efficiencies and meet UEC demand
- Establish a virtual hub to manage referrals & outreach to specialist teams
- Local profiling of SDEC demand to ensure core service meets demand
- Establish acceptance criteria & include SDEC and VW on DoS
- Ensure job plans and resource support SDEC delivery
- Co-locate SDECs with the emergency department
- Use self-assessment tools to benchmark & address gaps in SDEC
- Establish, measure and hold to account IPS delivery
- Test IPSs during times of crowding and increased pressure in ED
- Implement changes to rostering and job planning to ensure the right resource
- Use telephone to refer allowing conversations rather than electronic referrals
- Ensure consistent access to diagnostics 7 days a week
- Minimise ward moves
- Deliver networked rotas to access speciality advice in low volume specialities
- Deliver 100% coverage of comprehensive care plans
- Ensure all appropriate patients can answer the four patient questions every day
- Deliver comprehensive discharge planning
- Implement criteria led discharge (CLD) with a focus on facilitating weekend discharge
- Implement reconditioning/get up get dressed initiatives
- Ensure a ‘home first’ approach
- Establish team job plans which support early review of all patients
- Implement best practice, evidence based clinical pathways
- Embed the flow principles throughout the patient pathway
- Maximise use of step-down virtual wards
- Job planning: e-job planning, job planning toolkit & demand / capacity planning
- E-rostering and e-job planning: as an enabler for flexible working
- Retention: deploy the national retention guide and toolkit
- Consider the establishment of a digital staff passport
- Use the nationally developed agency rules toolkit
- Workforce transformation: use best practice models like CLEAR & HEE tools
- Consider new roles: access workforce transformation case studies
- Deploy the national safe sustainable and productive staffing guidance
- Adopt the national e-rostering & e-job planning meaningful use standards
- Utilise national workforce measurement tools, including model hospital
Download the above diagram as a PDF file.
National priorities and constitutional standards
Key metrics in each guide will have an overall impact on UEC national priorities and a return to constitutional standards.
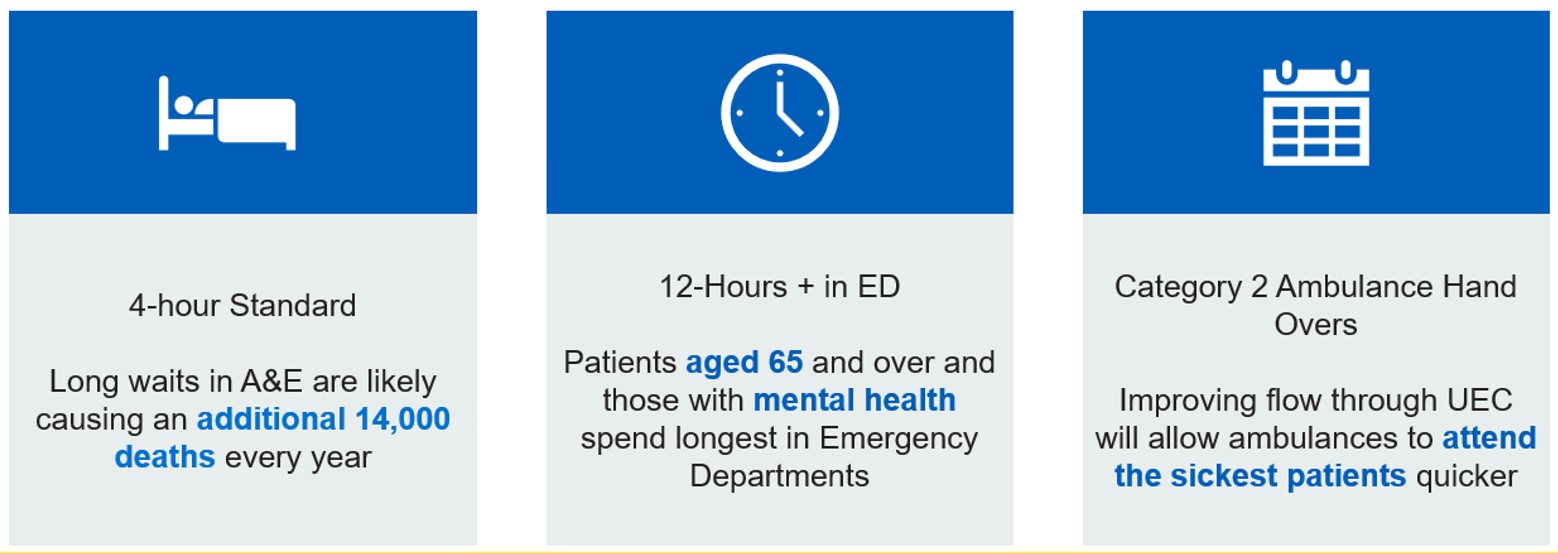
Urgent and emergency care national priorities
Click here to access an accessible description of the diagram above:
4 hour standard:
- Long waits in A%E are likely causing an additional 14,000 deaths every year
12 hours + in an emergency department (ED):
- Patients gaged 65 and over and those with mental health spend longest in emergency departments
Category 2 ambulance handovers:
- Improving flow through UEC will allow ambulances to attend the sickest patients quicker
Key measures should include:
Outcome measures:
- patients spending 12-hours + in ED
- number of non-elective admissions
- time spent on wards after discharge ready date
Balancing measures:
- re-attendance at ED within 7-days
- readmission rates at 30-days
Right care right place
How to ensure patients are cared for in the most appropriate setting for their needs and identifying those patients who may not need to be admitted to hospital.
Ambulance navigation
Ambulance services act as a front door and can correctly navigate patients to the right place first time. They can reduce unnecessary dispatches & conveyances, focussing resource on the sickest patients.
Change ideas
Hear and Treat:
- Increase the number of calls clinically navigated and validated prior to ambulance dispatch; including all category 3, category 4 and a proportion of category 2 calls.
- Implement the revised approach to category 2 segmentation (modified principles).
- Increase appropriate community referrals through to SPOA/navigation hubs/community providers using pre-determined pathways and clinical validation.
- Invest in technical infrastructure to safely refer patients through to community pathways using push/pull models and automation.
See and Treat:
- Increase ‘See and Treat’ through effective call before convey pathways, improve use of alternative pathways’
- Make use of lower acuity approved transport options, where it is safe and appropriate to do
- Community providers profiled on Directory of Service (DoS)
Other initiatives:
- Increase C3 and C4 validations in 111 including those with ED dispositions to reduce the validation taking place in 999.
Tracking indicators
In addition to local process measures linked to your change ideas, include the following measures:
- Hear and Treat rates
- See and Treat rates
- Onward referrals to community providers including breakdown of successful referrals and rejection rates
- Hospital handover delays
- Clinical staff within EOC
- Proportion of Cat 2 Segmentation calls clinically validated
- Ambulance response times with a particular focus on Category 2
Resources
- Urgent and Emergency Care Improvement Guide
- Winter 2024 letter
- NHS England » Urgent community response and ambulance referral resource
- UCR and Ambulance Referral Blueprint – Examples of 999 and Urgent Community Response (UCR) pathways
- Single Point of Access (SPoA) – Out Of Hospital Urgent and Emergency Care (UEC) – FutureNHS Collaboration Platform
- NHS England » Single point of access (SPoA)
Single point of access (SPOA)
SPOAs are multidisciplinary teams intervening early in the patient pathway to ensure a patient is seen by the right person for the first time. This results in better care for patients where the hospital is not the best place, and an alternative service may be available. Patients being supported by SPOA can be referred to an alternative service avoiding ambulance dispatch or following a face-to-face assessment by an on-scene clinician to prevent conveyance to ED.
SPoA can prevent unnecessary attendances to ED, reducing patient harm and prevent deconditioning in hospital. This supports the left shift to community-based services – both by diverting demand away from hospitals and reducing ambulance dispatch and conveyances.
Change ideas
- Increase category 3/4/5 pre dispatch (refer) for core patient groups
- Increase call before conveyance when paramedic on scene
- Increase conveyance to other community professional (GP, UCR, VW, NH MDT, social care)
- Appropriate referral processes and care pathways for care home residents to provide alternatives to ambulance dispatch and conveyance.
- Agreed common approach/ MVP for all SPoAs in the ICB/ system
- Agreed standardised pathways for key services e.g. end of life, falls, delirium
Tracking indicators
Define patient cohort who could be managed via a SPoA, for example: features of frailty, complex category 3-5 and key receiving services (UCR, virtual ward, SDEC). Could include category 2 outcomes as part of a segmentation approach.
- Volume of activity for these patients before and after (dispatch and conveyances for this cohort) once a SPoA is in place
- Capacity and opening hours of referred to services.
- Number of cases automatically transferred (pushed) to the SPoA from the EOC for onward referral.
- Number of contacts from the EOC for clinical advice (hear and treat and refer)
- Number of contacts to the SPoA from paramedics on scene with a patient and referrals
- Cases rejected by receiving services and why
Systems are encouraged to use the example data collection template and guidance, plus national data sets (ADS or local ambulance collection, Virtual Ward MDS, UCR CSDS, SDEC).
Resources
- Single Point of Access (SPoA) – Out Of Hospital Urgent and Emergency Care (UEC) – FutureNHS Collaboration Platform
- NHS England » Single point of access (SPoA)
Urgent community response (UCR)
Robust UCR services ensure patients are treated in the right place, avoiding unnecessary secondary care attendance and or admission, and when possible enabling patients to remain at home.
Change ideas
- Local review of UCR provision to meet demand 7 days a week
- Job plans and resource to support UCR delivery – ICB focus on efficient workforce & patient outcomes
- Standardised criteria (by exclusion) for accessing UCR
- Standardisation of service profiling on service finder / Directory of Services (DoS)
- ICB plans include system wide engagement for direct referral and use of Single Point of Access (SPOA) into UCR
- Communication strategies and OPEL planning include access into UCR
- UCR services collaborate with Primary Care, SDEC, virtual ward, ED/UTC and ambulance services to support patient flow across community and secondary care.
- Self-assessment tools to benchmark UCR and address gaps
- ICB process in place for effective feedback for referrals that are not suitable (inc. referral source breakdown)
Tracking indicators
In addition to local process measures linked to your change ideas, include the following measures:
- Increase rate of referral per 100,000 population
- Availability of UCR services including opening hours, accessibility and conditions responded to
- Achieve and/or exceed the minimum threshold of reaching 70% of 2-hours crisis response demand within 2 hours (Balancing metric)
Community Services Data set (CSDS) should be used in conjunction with ECDS /ADS opportunity reviews.
Resources
- B1406-community-health-services-two-hour-urgent-community-response-standard.pdf – All Documents
- Community Health Services – FutureNHS Collaboration Platform
- Urgent Community Response – Community Health Services – FutureNHS Collaboration Platform
Streaming and direct access
Establish models for streaming and initial assessment so that patients are seen in the right place the first time, improving patient safety and flow through UEC.
Change ideas
- Standardise streaming/ initial assessment and acuity/triage recording
- Clinical streaming at the front door of the ED/UTC as part of initial assessment (This may vary pending the model)
- Clinical resource for initial assessment and streaming for effective decision making
- Interprofessional standards to support shared risk across the whole hospital from arrival at the front door
- Pathways internally understood and accessible
- Agreed criteria for internal streaming
- DoS profiling of community services
- Digital enablers to support moving the patient to the right place for their healthcare needs as timely as possible
- Missed opportunities audits for continuous improvements of pathways through ED (A-tED)
Tracking indicators
- Proportion % of ED/UTC attendances that are streamed/redirected
- Proportion of patients streamed/initially assessed within 15 minutes of arrival
- Identifying patient cohorts suitable for streaming to other areas of the hospital
- Accurately recording acuity (triage acuity) to support patient selection
- Minimum pathways open to initial assessment clinicians
- DoS/Service finder being populated with the right services to avoid referral/conveyance to ED/UTC
Resources
- B1406-community-health-services-two-hour-urgent-community-response-standard.pdf – All Documents
- Community Health Services – FutureNHS Collaboration Platform
- Urgent Community Response – Community Health Services – FutureNHS Collaboration Platform
Criteria to admit
Consistent use of the CTA decision support tool can help identify those patients that would not benefit from admission and identify suitable alternatives. It minimises variation in decisions to admit, by ensuring only patients who need acute hospital beds are admitted, thus reducing delays and waste. Used retrospectively, it can help identify gaps in service provision and areas of opportunity.
The Criteria to Admit (CTA) decision support tool is an algorithm which helps clinicians check that an admission is required and identify potential alternatives to admission. It does not replace or override the senior clinician’s decision to admit.
Improving flow can impact on length of stay, and clinical outcomes, with a reduction in bed occupancy to facilitate flow and the number of non-elective (NEL) admissions
The CTA tool is one way of assessing if a patient will benefit from an inpatient stay. It can be used as:
- a live tool to determine or confirm a patient’s admission
- an audit and learning tool to determine:
- bed days utilisation
- bed days that would have been saved, if the tool was used at point of attendance.
Admission is highly likely if any of the responses to the questions in the tool is ‘yes’. To note: there will be no need to use the tool if the MDT team is not considering a patient admission.
Change ideas
- Use CTA as a live tool for confirming patient admissions
- Team job plans to support early review of all patients by a senior decision maker
- CTA to residents and other HCPs with senior decision maker oversight
- Early use of CTA by senior decision makers in the patient journey at the point of attendance
- CTA audits for right capacity to meet the demand for alternatives to admission
- Review CTA for admitted patients after 24 hours to determine whether patients are fit for discharge
Tracking indicators
- Proportion of patients admitted with record of decision to admit review (data to be locally collected and audited)
- Conversion rate from ED attendance to NEL admission.
Systems should also seek to review input costs, particularly bank and agency spend to support corridor care and crowding in ED due to waits for inpatient beds.
Resources
- ECIST core resources on Criteria to Admit
- Criteria To Admit flow chart
- ECIST Bitesize Podcast Series – Criteria to Admit
- Criteria to Admit audit tool user guide
- Criteria to Admit audit tool
Right pathway
Ensuring attendance and admission alternatives are available so only those patients requiring admission are admitted.
Urgent Treatment Centres (UTCs):
UTCs provide a locally accessible, safe and convenient alternative to emergency departments. Standardised UTCs can reduce attendance at emergency departments and improve patient access, experience and care. All UTCs should aim to:
- See minor injuries and minor ailments for patients of all ages.
- Referral routes into SDEC and similar services for d-dimer and troponin testing direct from UTCs.
- Plain film X-ray provision as part of capacity and demand planning for all UTCs
- Accept appropriate ambulance conveyance including stretchers for fit2sit patients.
Change ideas
- Profiling of demand for UTC and adapting core opening hours to meet demand
- Review demand for both booked and walk in appointments to meet demand including links with other local services
- Access routes in place for patients to be booked into a UTC from NHS 111, Primary Care or streamed from ED
- Direct access from Ambulance
- Team job plans for consistent minor injury and minor illness offer
- Resource identified to deliver UTC services operationally and clinically
- UTC activity is recorded on ECDS as a type 3 attendance
- Basic consistent investigative and diagnostic offering on site (with clear protocols if not on site)
- Correct classification as UTC and is also designated as on
- Self-Assessment tools to benchmark and address gaps in UTC provision, improving the service and patient care.
Tracking indicators
- Decisions in 24/25 on the future function of existing services by designating as a UTC, becoming an alternative service (e.g. primary care centre) or closing.
- Provide assurance against the UTC Principles and Standards
- Report UTC activity as Type 3 on the emergency care data set meeting the required data standards.
Resources
- Urgent Treatment Centres – FutureNHS Collaboration Platform
- NHS England » Urgent treatment centres – principles and standards
- NHS England » Urgent treatment centres: frequently asked questions to support implementation of the standards and principles
- Emergency Care Data Set – FutureNHS Collaboration Platform
Same Day Emergency Care (SDEC):
SDEC should be in place 12 hours per day, 7 days per week (as a minimum) in every acute hospital with a type 1 ED in England.
SDEC allows specialists, where possible, to care for patients on the same day of arrival to hospital, as an alternative to an inpatient hospital stay, removing delays for patients requiring further investigation and / or treatment.
Enabling direct access from 999, 111, primary and community care will prevent overcrowding in EDs, improve the quality of care and patient experience.
Preventing SDEC estate being used as inpatient capacity will support flow from ED.
If every hospital were to meet the national mean of 42% of UEC activity for SDEC, over 100k bed days could be saved.
Change ideas
- Adapting core opening hours to meet demand
- Review of SDEC provision at weekends to meet demand
- Non-bedding SDEC overnight to maintain flow through
- Team job plans which support early review of all patients by a senior decision maker
- SDEC profiled on Directory of Service (DoS) to enable direct access
- Access criteria for direct ambulance referral
- SDEC activity recorded on ECDS to enable systemwide access to monitoring and evaluation of SDEC
- Co-locate SDEC services with specialties
- Self-assessment tools to benchmark and address gaps in SDEC provision
Tracking indicators
- Use of SDEC: SDEC activity, as recorded in the Emergency Care Dataset (T5)
- Size of the SDEC opportunity: volume of activity for patients with conditions that are amenable to SDEC (patients with an ‘SDEC Index’ diagnosis) that have a 1 day, 2 day or 3-day NE LOS
Systems should also start to record key input metrics including workforce, estate (e.g. square meterage), digital infrastructure, diagnostics, across all days of the week.
Resources
- SAMEDAY Strategy and framework for development and delivery of SDEC
- SDEC Index and SMARTool
- SDEC Case Studies
- SDEC Collaboration Platform
- SDEC Workforce Roles Toolkit – 2024
- SDEC Webinars
- Case Study Establishing an SDEC by Default approach in Oxfordshire – SDEC Collaboration Platform – FutureNHS Collaboration Platform
- Case study – Lancashire Teaching Hospital – SDEC Rapid Improvement Week – SDEC Collaboration Platform – FutureNHS Collaboration Platform
Virtual wards
A virtual ward (also known as hospital at home) is an acute clinical service with staff, equipment, technologies, medication, and skills that are usually provided in hospitals, delivered to selected people in their usual place of residence, including care homes, for up to 14 days. It is a substitute for acute inpatient hospital care.
The service can support admission avoidance (step-up care) and be accessed directly from home and via a range of services such as a GPs, single point of access (SPoA)/ Integrated Care Coordination (ICC) service, Urgent Community Response (UCR), 999/111, SDEC or an emergency department (ED).
It can also facilitate an earlier discharge or transfer from a hospital inpatient ward (step-down care), enabling individuals who are not medically optimised for discharge to continue to receive medical treatment, oversight and diagnostics at home.
Virtual wards can positively impact on NEL admissions and ED/SDEC attendances (step-up capacity) and reducing inpatient LoS and readmissions (step-down capacity).
Change ideas
- Delivering the 10 core components of a virtual ward outlined in the Virtual Wards operational framework
- Capacity adequately scaled with broad criteria to accept patients
- Link with SPoA/integrated care coordination (ICC) services to maximise access to step-up virtual wards
- Prioritise referrals from care homes and 999/111
- Virtual hubs staffed by dedicated teams which can take referrals from across hospital specialties
- Virtual wards considered as part of twice daily hospital ward rounds
- In-reach initiatives both in ED and inpatient wards to identify patients who could benefit from virtual ward care
- Closer working and linkage with community respiratory, heart failure and UCR to maximise use of the workforce
Tracking indicators
- Number of virtual wards ‘beds’
- Virtual ward occupancy percentage (of at least 80% in all virtual wards by the end of Q2)
Hospitals should also aim to improve the recording of key input costs for virtual wards, for example on workforce, digital infrastructure, diagnostics, medications and transport.
Resources
- GIRFT guide on making the most of virtual wards
- Pathways for acute respiratory illness, frailty and heart failure
- Access to diagnostics on virtual wards guidance
- A guide to setting up technology-enabled virtual wards
- Summary of South East evaluation
- Virtual Wards Network (on the FutureNHS platform)
Acute patient flow
Defined ways of working to help improve patient flow and patient experience, underpinned by an overarching principle that focuses on ensuring that patients receive care from healthcare professionals with the appropriate skills, regardless of their location in the hospital.
Standardising acute care in the first 72 hours avoids inappropriate use of direct admission to AMU pathways contribute to long waits in EDs (source: Society of Acute Medicine 2023)
Change ideas
- Urgent cross sectional (CT/MRI) imaging reported within 4 hours of request
- Core laboratory services available 24/7, turnaround times monitored regularly and reported monthly
- NEWS2 calculated for every patient
- Full assessment by competent clinical decision maker, within one hour
- Review by an expert clinical decision maker within six hours of decision to admit or of arrival on the assessment unit (whichever is earlier) from 08:00-20:00h or within 14 hours outside of these times
- Specialty team becomes responsible for patient care upon transfer from assessment unit to a non-medical ward
- Prioritisation for patients transferring out of critical care units (CCU, ICU, HDU, ECU) for inpatient bed allocation
- Expert/senior decision maker receive referrals and provide advice to community and hospitals every day
- Twice-daily consultant ward rounds in higher acuity areas, e.g. ICU, AMU, SSW, SAU, CCU, and other medical wards if possible.
- Patients aged over 65 presenting to hospital as an emergency assessed on arrival using the Clinical Frailty Scale (CFS) and 4AT tool for delirium.
Tracking indicators
- Reduction in 12 hour+ waits in the emergency department
- Reduction in LoS for common conditions (i.e. Chest pain, headache etc.)
- Reduction in bed occupancy
- Zero-day length of stay continues
Resources
Right process
Ensuring our patients receive inpatient care in a timely, effective care to optimise time spent in hospital.
Ward processes
Ward rounds play a crucial part in reviewing and planning patient care, however there is considerable variability. Addressing variation should improve clinical quality and length of stay. Intra-professional standards (IPS) that are shared, optimised and used consistently unpin effective and timely UEC care.
Change ideas
- Assessment by competent decision maker within 4h, ideally within 1h and an expert decision maker within 6h (14h if admitted out of hours)
- Local agreement on patient dispositions, determining which speciality should manage symptoms or conditions
- Consultant of the week model
- Twice daily consultant ward rounds in high intensity areas, daily in lower intensity areas, to include clear weekend reviews and discharge arrangements
- SHOP (SickHomeOtherPlan) principles
- Standardise the board rounds allowing time for discharge critical tasks to be completed rapidly
- Discharge supported by virtual ward
- Second ‘mop up’ board round in the afternoon with sick patients handed over and patients for discharge next morning have any outstanding discharge critical tasks completed
- Clinical Criteria for discharge plans, plus what to do when investigations are reported whether normal or abnormal
- Daily specialty liaison into admission areas (particularly Cardiology, Geriatrics and Respiratory) including telephone support, admission avoidance guidance and hot clinics including follow up of investigations done post-discharge
- All patients > 65 assessed for frailty using the Clinical Frailty Scale (CFS) and assessed for delirium using the 4AT
- Laboratory services available 24/7 with key results available within 1 h
- Urgent cross sectional imaging reports available within 4-hours
Tracking indicators
- Length of stay: 7, 14 and over 21 days
- Patients with no Criteria to reside, patients waiting for TTOs, speciality referrals, investigations or internal reasons
- Lengths of stay by speciality
- Percentage (and number) of patients discharged before 12 noon
Resources
- BGS/GIRFT Six steps for better care for older persons
- Hospital acute frailty pathway (GIRFT)
- NHS England Frailty resources
- SAFER bundle
- Red and green bed days
- BGS Joining the dots/proactive care
- RCP – Ward rounds in Medicine: principles for best practice
- RCP – Modern ward rounds
- RCN – Modern ward Rounds Best Practice: The process
Standardised care processes
Internal professional standards (IPS) state, in writing, the expectations on all clinicians and other staff in the delivery of care. They ensure there are agreed values, behaviours, response times and escalation chains for each specialty and service where processes are not followed, or standards not achieved. These work best when:
- every clinical service agrees IPS that are consistent and complement each other
- they contain an unambiguous description of the values and behaviours expected and set measurable standards for which everyone is accountable
- they centre on patient care, are written with clinicians and are championed by the executive team
- they operate 7-days a week across all services and specialties
Robust IPS designed collaboratively with staff lead to:
- safer, more effective, timely UEC services
- timely standards for key internal processes: for example, inpatient scans, specialty opinion, treatment
- consistency of response and turnaround times across all patient pathways
- reduced waste and delays, minimal clinical handovers and bed moves
- empowered clinical leadership
- increased clinical and operational collaboration
- improved visibility of performance and the factors that affect it
If the change ideas are adopted, a 5% reduction in the total beds occupied by patients admitted for 14 days or longer on a non-elective pathway is deliverable.
This work will also help reduce 12-hour+ stays in ED.
Change ideas
- Where IPS do not exist or are not complete for all services, undertake executive-sponsored collaborative work to create and implement them, and make the core service standards explicit.
- After reviewing current compliance with existing IPS, assess the performance of each specialty and make the measurable time standards, for example diagnostic turnaround time, more explicit or more challenging. Consider implementing the standards in the GIRFT acute patient care standards.
- Designate an executive as IPS sponsor with a remit for holding the organisation and teams to account, as well as managing escalations and unblocking any issues identified.
- Undertake a thorough review of demand and capacity, considering UEC flow from ED and elective/cancer/diagnostic demand and capacity; ensure capacity is in place to meet IPS.
- Test IPS during times of overcrowding and increased pressure in ED; particularly the escalation process, which will involve medicine and surgery reaching into ED to support decision-making, flow and referrals.
- Implement changes to rostering and job planning to ensure the right resource to support delivery of IPS (see Right people section).
- Implement agile referrals to specialties – allowing, for example, conversations by telephone or secure messaging rather than electronic or paper referrals – or move to a full trusted assessor model.
- Review and standardise respiratory and cardiology pathways to reduce variation in specialty LoS.
- Ensure consistent access to diagnostics 7 days a week.
- Deliver networked rotas to access advice from low volume specialties and, out-of-hours, from high volume specialties.
- Minimise ward moves during an inpatient stay; get the patient to the right team first time.
Tracking indicators
These should be determined in line with the time standards you record locally: for example, the proportion of requests for specialty input actioned within 30 minutes.
Note: We do not advise looking at mean LoS as this is an overly simplistic measure that will be more sensitive to the ‘right place’ change actions for NEL admissions.
Resources
- GIRFT acute patient care standards
- ECIST rapid improvement guide
- NHS England Admitted Pathways Programme
- GIRFT 6 to help fix
Care planning
If Internal Professional Standards (IPS) are how the UEC pathway works at an organisational level, care plans are the patient-level equivalent: how patients move through their care in a way that meets their individual needs. Consistent and standardised hospital processes are crucial to ensure everyone delivers care plans every day. Achieve this by:
- a senior clinical decision-maker carrying out a review within 12 hours of the patient being in the hospital, supported by shared decision-making conversations between the senior clinical decision-maker and patient
- developing a comprehensive care plan, with input from clinical teams, allied health professionals, discharge teams, patients (where they have the capacity to do so) and their careers and families, using the 4 patient questions, with set clinical criteria for discharge and an estimated discharge date within 14 hours of admission
- completing daily board rounds and starting ward rounds by 10am with a senior clinical decision-maker, senior nurse and members of the wider MDT, and an afternoon huddle to ensure all actions have been or are being delivered and, if not, to ensure these actions are escalated to the right colleagues or teams to urgently address them.
- continuously reviewing and updating care plans, supported by clear escalation processes.
Optimise care and discharge planning
Having comprehensive care and discharge plans, with input from patients, their careers and families, that are delivered every day minimises waste and delays in patient care, reducing length of stay and the harm associated with it.
If change ideas are adopted, a 5% reduction in the total beds occupied by patients admitted for 14 days or longer on a non-elective pathway is deliverable.
Note: We do not advise looking at mean LoS as it is overly simplistic and will be affected by changes to NEL admissions generated by the ‘right place’ change actions.
Change ideas
- Ensure 100% of patients have comprehensive care plans. These plans are always developed by a consultant with the patient and their carer/family within 14 hours of admission.
- Ensure all patients can answer the 4 patient questions every day.
- Deliver comprehensive discharge plans, from the point of admission, for all patients. These must include the estimated discharge date and clinical criteria for discharge (clinical and physiological criteria with clear parameters for each, plan and follow up action as a minimum). Ensure patients requiring referral to care transfer hubs, and social care for those with more complex needs, are identified early.
- Implement criteria led discharge (CLD)
- Implement reconditioning/get up get dressed
- Embed a ‘home first’ approach in board and ward rounds and minimise decisions made about people’s long-term care needs when they return home, outside of their usual environment.
- Establish team job plans which support the early review of all patients by a senior decision maker and 7-day ward and board rounds (see Right people section).
- Where they exist, implement best practice, evidence based clinical pathways including #NOF, STEMI and stroke.
- Embed the flow principles throughout the patient pathway to eradicate overcrowding. This will involve making the best use of automated bed systems and embedding the principles of 7-day working.
- Maximise use of step-down virtual wards and hot clinics to reduce the time patients spend in hospital.
- Undertake weekly multi-disciplinary long length of stay reviews.
- Reduce variation in exit pathways between teams and days of the week and time of the day.
Tracking indicators
- In addition to local process measures linked to your change ideas, the following can be used:
- number of beds occupied by patients with 14+ days LoS
- proportion of emergency admissions with 21+ days LoS
- patient reviews by senior decision-maker (local audit)
- proportion of comprehensive care plans in place where the 4 patient questions can be answered by patients or their carers / family members (local audit)
Resources
- NHS England Admitted Pathways Programme
- The 4 patient questions
- RCP modern ward rounds
- Hospital discharge and support guidance
- NHS England UEC pathway maturity self-assessment
- NHS England Universal Support Offer 2023
Discharge planning
The average length of delay for delayed patients in January 2025 was 6.1 days amounting to an estimated 324,000 bed days lost.
Change ideas
- Discharge planning starts at the point of attendance – clinical and functional criteria for discharge, discharge ready date data collection
- Identify frailty and embed a supported home first philosophy
- If a person requires admission aim to prevent deconditioning while having acute treatment
- Once clinical criteria for discharge embedded begin to implement criteria led discharge
- Minimise delays within the TTO process – transcription to patient collection
- Plan for predictable events; weekends, public holiday discharges
- Aim for high maturity for Care transfer hubs and managing transitions of care with partner organisations
- Accurate, up to date and effective discharge pathway demand and capacity planning (BCF link)
- Effective use and flow through Intermediate Care beds
- Create real time reporting on a shared data platform with all partners
Tracking indicators
In addition to local process measures linked to your change ideas, the following measures feature in the improvement analytics:
- Proportion of people discharged on their discharge ready date
- Average length of delay (discharge ready to discharge date)
- Residential care home admissions (ASCOF)
- Proportion of acute bed base occupied by people experiencing a 7, 14 and 21day length of stay.
Resources
- High impact change model
- BCF Demand and Capacity
- Optimising discharge medication RIG
- Weekend discharge RIG
- Criteria led discharge
- Active hospitals
- Connected digital systems
- Principles for acute patient care
- Planning for predictable events
- HomeFirst principles
- Intermediate care framework
- Seven days services clinical standards
- Hospital acute care frailty pathway
Right people
Utilising your workforce more effectively through high quality operational workforce planning and deployment will help improve staff experience and retention, support service improvement and further improve productivity by optimising the skills and capacity of your workforce.
Optimising the valuable skills and capacity of clinical workforces
Good quality workforce planning and deployment is about optimising the valuable skills and capacity of our clinical workforce by ensuring the right people are in the right place at the right time to deliver high quality, efficient patient care. It is about supporting the development of staff and services and providing the visibility of clinical capacity required to plan services effectively and match valuable clinical capacity to patient need.
Improvement requires targeted action on workforce planning and transformation, workforce deployment, governance and measurement.
Follow the resources on clinical workforce productivity on FutureNHS. In particular, we recommend the following resources for each of the 3 pillars of excellence, which are workforce planning and deployment; workforce transformation; and governance and measurement.
Workforce planning and deployment
Workforce planning and deployment resources
- e-job planning and e-rostering for effective planning and deployment of all staff:
- the Advancing levels of attainment handbook and related resources: helps organisations establish what their e-rostering and e-job planning levels of attainment are and what is required at each level to progress, based on local need and current position
- the e-job planning toolkit and e-rostering toolkit: provide a step-by-step guide to optimising system usage and embedding effective associated processes and governance
- e-rostering as an enabler to flexible working: provides resources to support team leaders working in clinical areas to develop ways to roster their staff more flexibly, thereby improving work-life balance and experience at work for staff. The case studies showcase the innovative initiatives that are being implemented and their impacts on staff wellbeing and retention
- medical consultant job planning improvement guide
- demand and capacity planning: provides resources to support service and system-level demand and capacity planning, including modelling tools and approaches, case studies, webinars and e-learning
- digital staff passport: enables NHS employees to use their smart phone to share employment, education and training, and occupational health details with hospitals 24/7, to support their moves between those hospitals
- agency toolkit: supports organisations to reduce their agency staff bills and encourage workers back into substantive and bank roles
Retention resources
- improving staff retention guide: supports line managers and employers to consider the key areas that affect workforce retention
- international retention toolkit: actions employers can take, such as mapping skillset and qualifications and setting up pastoral support, to ensure internationally recruited staff will want to stay, thrive and build lasting careers in the NHS
- NHS Emeritus: an initiative that connects recently retired and peri-retired clinicians across England with NHS providers of acute care who need the help only experienced clinicians can offer
Workforce transformation
Workforce transformation resources
- Clinically-Led Workforce and Activity Redesign (CLEAR) programme: supports clinicians and organisations to deliver transformation and workforce redesign projects to enhance patient care, by equipping frontline staff with skills in data analysis, innovation and leadership
- Star: accelerating workforce redesign: a model and workshop for workforce transformation, enabling you to explore workforce challenges, develop bespoke action plans and use resources in the Star online directory
- Roles explorer: provides resources for workforce redesign, such as introducing new roles or innovative adaptations to existing roles within a service or system
- Calderdale Framework: an evidence-based workforce transformation tool used in acute and community settings to rapidly identify skill sets required by services and their populations in acute, sub-acute and rehabilitation phases
Governance and measurement
Governance resources
- National Quality Board (NQB): safe sustainable and productive staffing guidance (2016): an improvement resource that builds on the NQB’s 2013 expectations and framework within which organisations and staff should make decisions about staffing that optimise productivity and efficiency while maintaining focus on improving quality
- e-rostering and e-job planning meaningful use standards: support hospitals to implement and use e-job planning and e-rostering software to its full potential, which includes the use of board reporting and metrics for improvement
Measurement resources
- care hours per patient day: guidance on the principal measure of nursing, midwifery and healthcare support staff deployment on inpatient wards
- Model Health System: data-driven improvement tool that enables NHS health systems and hospitals to benchmark quality and productivity
- Workforce Productivity Diagnostic Tool: supporting systems and hospitals to understand and benchmark their workforce productivity
Change ideas
Collect workforce data to understand your workforce capacity:
- capture and review data for all staff who work in urgent and emergency care on a permanent or temporary basis. Include data from/on ESR, temporary spend, recharge, recruitment and retention rates, turnover, sickness absence, age profile and demographics
- review your consultant-level capacity (including direct clinical care and supporting professional activity time)
Understand your retrospective and prospective activity:
- collect activity data and review any service plans that may impact on future activity levels (such as work transferring from location or changes in mode of delivery)
- this review should include key hours of operation
Undertake a systematic review of your workforce requirements:
- map your pathway and consider which staff are required at each stage
- review the roles, skills and capacity required to meet your expected activity. Consider whether any new roles are required or would improve productivity
- review your pay spend run rates and compare these to your budget
- consider recruitment, training and retention needs, including specific equipment or specialty training requirements
Review national policy when building your establishment and optimising deployment:
- Developing workforce safeguards: Supporting providers to deliver high quality care through safe and effective staffing
- GIRFT guidance
- appropriate Royal College guidance
Please share your ideas and feedback with us
Thank you for engaging with this guide.
Please share your ideas and feedback with us. There are 2 ways you can do this:
- by emailing us at england.improvementdelivery@nhs.net
- by feeding back through your local Learning and Improvement Network. Details on the networks are on the FutureNHS platform
Publication reference: PRN01435_iv (interim version)