
The accountability report sets out how NHS England meets key accountability requirements to Parliament and is comprised of three key sections:
The corporate governance report sets out how the organisation was governed during 2023/24, including membership and organisation of our governance structures and how they support achievement of our objectives. The report includes:
- directors’ report
- statement of accounting officer’s responsibility
- governance statement
The remuneration and staff report sets out our remuneration policies for executive and non-executive directors and how these policies have been implemented for the reporting period, including salary information and pension liabilities.
The parliamentary accountability and audit report brings together key information to support accountability to Parliament, including a summary of fees and charges, contingent liabilities and the Certificate and Report of the Comptroller and Auditor General to the Houses of Parliament.
Accountability to Parliament and the public
During 2023/24, NHS England has continued to work closely with the NAO in their work to test whether public bodies are delivering value for money. During this period, the Chief Executive and other senior leaders gave evidence to Public Accounts Committee hearings on Progress in improving mental health services in England, Access to UEC, the New Hospital Programme and NHS Supply Chain and efficiencies in procurement.
In 2023/24, the NAO published reports on Access to unplanned or urgent care, Progress with the New Hospital Programme, NHS Supply Chain and efficiencies in procurement and NHS England’s modelling for the NHS Long Term Workforce Plan.
In response to the PACs recommendations, NHS England has:
- set out targeted interventions, in the Long Term Workforce Plan, to grow and transform
the mental health workforce. These interventions will be delivered via partnership working across NHS England, DHSC, ICSs and wider - continued to work to tackle unwarranted variation in performance across secondary, primary and community care, and improve A&E waiting times and ambulance response times, with bespoke support for the most challenged systems
- continued to support the delivery of the New Hospital Programme including through procurement of a programme delivery partner and work to ensure the Programme’s modelling fits with regional and national modelling on the long-term infrastructure needs of the NHS
- continued to drive efficiencies in procurement through oversight of and support to NHS Supply Chain, including in the development of NHS Supply Chain’s modernisation programme
Corporate governance report
Directors’ report
The key responsibility of the Board is to provide strategic leadership to the organisation, including:
- setting the overall direction of NHS England, within the context of the NHS Mandate from government
- approving the business plan, which is designed to support achievement of our strategic objectives and monitor our performance against it
- holding the NHS Executive to account for this performance and for the proper running of the organisation (including operating in accordance with legal and government requirements)
- determining which decisions, it will make and which it will delegate to the executive or committee or sub-committee, via the Scheme of Delegation
- ensuring high standards of corporate governance and personal conduct
- monitoring the performance of the group against core financial and operational objectives
- providing effective financial stewardship
- promoting effective dialogue between NHS England, government departments, partners, ICSs providers of healthcare and the communities served by the NHS.
The Board
In accordance with paragraph 2 of Schedule A1 to the 2006 Act (as also set out in section 4.1 of the Standing Orders), the Board comprises the chair, eleven non-executive directors and five executive directors including the chief executive.
Appointments
The chair and non-executive directors are appointed by the Secretary of State for Health and Social Care and executive directors are appointed by the chair and non-executive directors.
The appointment of the chief executive is subject to the Secretary of State for Health and Social Care’s consent.
Dame Emily Lawson was Chief Operating Officer from 1 November 2023 following the departure of Sir David Sloman on 3 September 2023, with an interim period covered by Sir James Mackey.
On 19 February 2024, Professor Sir Robert Lechler, Jane Ellison, Mark Bailie, and Professor Dame Helen Stokes-Lampard joined the NHS England Board as non-executive directors.
In February 2024, the Board approved the appointment of two associate non-executive directors; Suresh Viswanathan and Tanuj Kapilashrami.
Board members
Directors who served on the NHS England Board during the year are listed in the table below, along with their attendance. Biographical details may be viewed on our website.
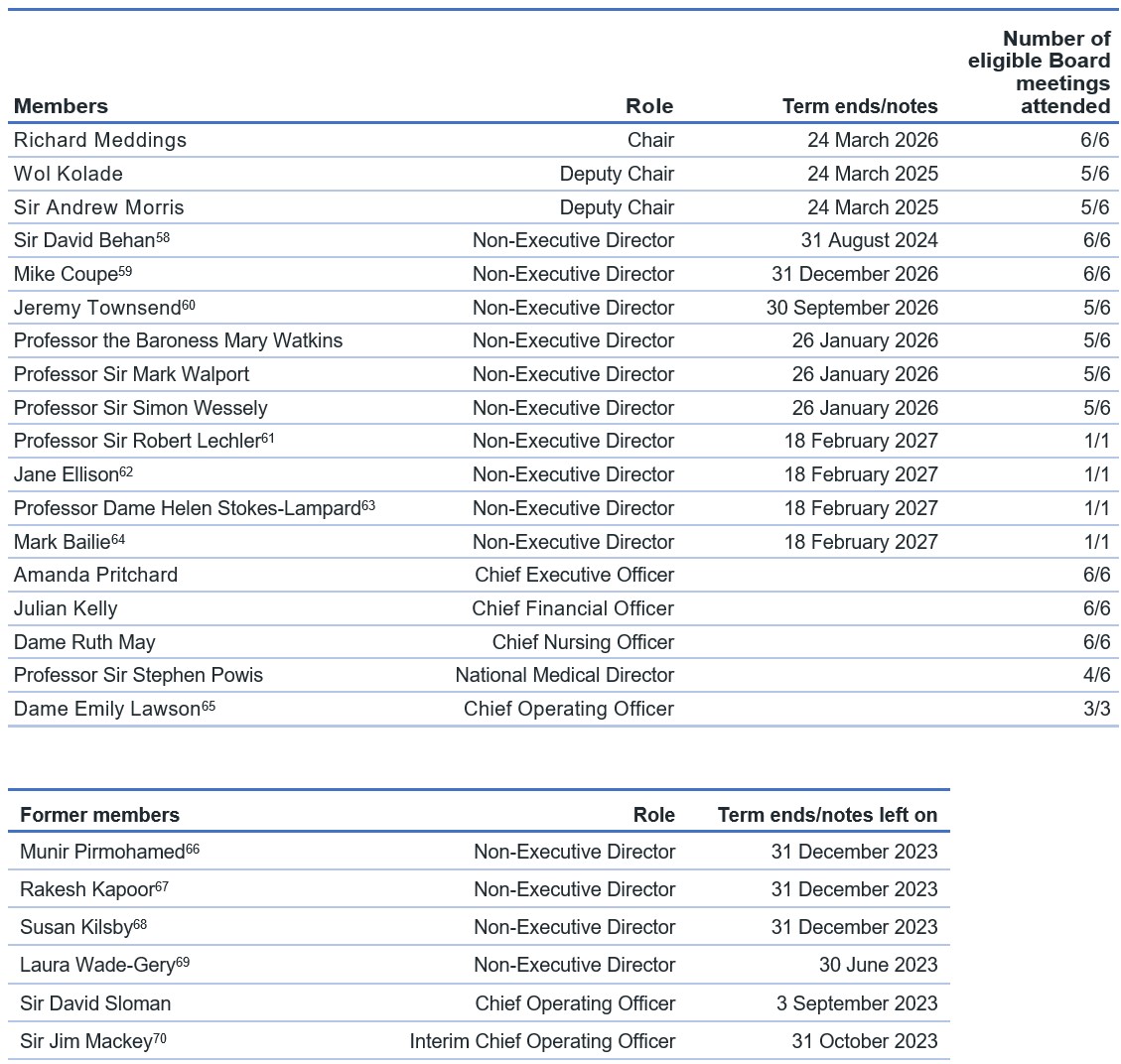
[58] Sir David Behan began his second term as non-executive director on 1 January 2024.
[59] Mike Coupe began his second term as non-executive director on 1 January 2024.
[60] Jeremy Townsend began his second term as non-executive director on 1 August 2023.
[61] Professor Sir Robert Lechler was appointed to the NHS England Board on 19 February 2024.
[62] Jane Ellison was appointed to the NHS England Board on 19 February 2024.
[63] Professor Dame Helen Stokes-Lampard was appointed to the NHS England Board on 19 February 2024
[64] Mark Bailie was appointed to the NHS England Board on 19 February 2024.
[65] Dame Emily Lawson was appointed as COO on 1 November 2023.
[66] Munir Pirmohamed’s term as non-executive director ended on 31 December 2023.
[67] Rakesh Kapoor’s term as non-executive director ended on 31 December 2023.
[68] Susan Kilsby’s term as non-executive director ended on 31 December 2023.
[69] Laura Wade-Gery’s term as non-executive director ended on 31 June 2023. [1] Sir Jim Mackey was Interim Chief Operating Officer from 3 September – 31 October 2023. He remains National Director of Elective Recovery and a member of the NHS England leadership team.
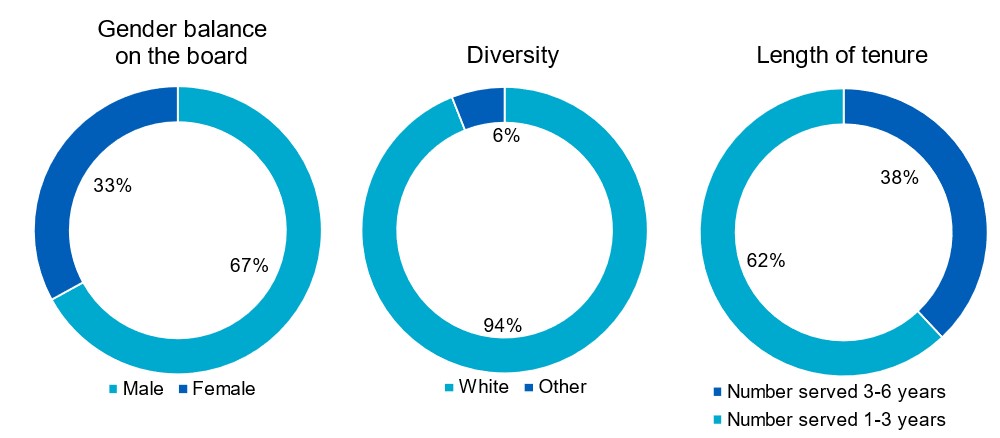
Board diversity
The charts below show the composition of the Board members by gender, diversity, and tenure as of 31 March 2024.
The governance structure
Following the merger of Health Education England with NHS England on 1 April 2023, NHS England strengthened its governance structure to include functions that transferred from Health Education England. An overview of the Board governance framework is shown on the next section and individual Board committee reports can be found in the board committees section of this report. A report detailing the business considered by the Board committees is provided to each Board meeting.
Board activity and administration
There were six NHS England Board meetings during the year, each including a public and a private session. The option for members of the public to attend public sessions in person was available throughout the year. Public sessions were live video streamed and published on our website along with the agenda, papers, and minutes.
In addition to the six formal meetings, the Board held three Board strategy sessions and various subject-specific workshops and deep dives.
Key items considered by the Board during the year were:
Strategy
- a review of technology and innovation in the NHS
- working in partnership with people and communities
- Federated Data Platform
- New Hospital Programme
- NHS efficiency and productivity programme
- multi professional education and training investment plan
- long term infrastructure strategy project
- Primary care future strategy
- revised NHS Oversight Framework
- NHS Long Term Workforce Plan
Performance
- regular operational and financial performance updates
- learning from COVID-19
- the delivery plan for recovering access to primary care
- annual report on NHS England’s work on healthcare inequalities and the NHS Race and Health Observatory
- learning disability and autism programme
- specialised commissioning 2024/25 – delegation to ICBs
- mental health, learning disability and autism inpatient quality transformation
- delivery plan for recovering UEC services
- NHS England’s 3-year delivery plan for maternity and neonatal services.
Governance and risk
- annual board effectiveness review (2022/23)
- risk appetite and risk governance
Review of Board effectiveness and performance evaluation
In May 2023, the Board received the findings of the 2022/23 NHS England Board governance effectiveness review and endorsed the recommendations and actions. The review identified a number of areas that had improved, including the operation of the Board and its committees, the effectiveness of NHS England’s governance framework and internal control arrangements, and information flows to the Board. Recommendations for improvement were made in relation to the balance of operational and strategic business at the Board, risk reporting and assurance processes, and the quality of papers.
NHS England has implemented most of the recommendations and actions during 2023/24 and the Board will consider a report on the success of the implementation later in 2024.
Board committees
Audit and Risk Assurance Committee (ARAC)
Role of the committee
The committee’s primary role is to provide assurance to the Board about the integrity of NHS England’s financial statements and the comprehensiveness, reliability and integrity of its internal control, risk management and governance processes.
Committee members
The committee met six times and the following table details membership, and the number of meetings attended by each member during the year:
| Members | Number of eligible meetings attended | Comment |
| Jeremy Townsend | 6/6 | Non-Executive Director, Chair |
| Wol Kolade | 4/6 | Non-Executive Director |
| Mark Bailie[72] | 1/1 | Non-Executive Director |
| Mike Coupe | 6/6 | Non-Executive Director |
| Jane Ellison[73] | 1/1 | Non-Executive Director |
| Rakesh Kapoor[74] | 1/4 | Non-Executive Director |
| Gerry Murphy | 4/6 | Non-executive Chair of DHSC’s Audit Committee (non-voting member) |
[72] Mark Bailie joined the committee as a member from 19 February 2024
[73] Jane Ellison joined the committee as a member from 19 February 2024
[74] Rakesh Kapoor left the committee membership on 31 December 2023
Attendees
Additional attendees are invited to attend meetings to assist with committee business. For 2023/24 these included the Chief Delivery Officer, Chief Executive Officer, Chief Financial Officer, Director of Corporate Governance, Director of Financial Control, as well as representatives from the external auditors the National Audit Office (NAO) and the internal auditors Deloitte LLP. The committee can meet with the internal and external auditors without management when required, and the auditors have direct access to the Board Chair and to the committee chair to support independence.
Principal activities during the year
As part of ensuring the integrity of the organisation’s financial statements, systems of internal control and risk management processes, the committee:
- approved the internal audit plan and considered regular progress reports from the internal auditors and the annual Head of Internal Audit Opinion
- considered risk management governance within NHS England and reviewed NHS England’s risk register
- reviewed several risk deep dives including NHS Estates and maternity and neonatal
- received updates on information security and cyber risks, including updates from the Cyber Security and Risk Committee (CSRC), a sub-committee of the ARAC
- received the Counter Fraud strategy and updates
- approved changes in accounting policies and reviewed areas of significant estimation or judgement
- assessed the integrity of NHS England’s financial reporting
- approved NHS England’s 2022/23 Annual Report and Accounts
- received details of losses and special payments
- considered NAO reports and management letters and received an update on the status of the NAO Value for Money Programme.
External audit
During the year, ARAC has worked constructively with the NAO Director responsible for the NHS England audit and their team. The work of external audit sits outside our governance arrangements but independently informs our consideration of control, compliance, governance, and risk. The work of external audit is monitored by the ARAC through regular progress reports. These include summaries of the value for money work that is either directly relevant to our work or may provide useful insights to the committee.
Data, Digital and Technology Committee (DDAT)
Role of the committee
The role of the committee is to consider and make recommendations on the digital and technology strategy (including cyber strategy) to the NHS England Board and oversee its implementation. It advises on the development of data and technology architecture and assures the Board on the discharge of data functions, including overseeing and scrutinising how the functions are exercised, the steps taken by NHS England to follow the statutory guidance on NHS England’s protection of patient data, and how NHS England protects confidential patient information.
Committee members
The committee met six times and the following table details membership, and the number of meetings attended by each member during the year:
| Members | Number of eligible meetings attended | Comment |
|---|---|---|
| Richard Meddings | 6/6 | Chair of NHS England |
| Mark Bailie[75] | 1/1 | Non-Executive Director |
| Daniel Benton | 6/6 | Non-Executive Committee Member |
| Mike Coupe | 5/6 | Non-Executive Director |
| Laura Wade-Gery (Chair)[76] | 1/1 | Non-Executive Director |
| Rakesh Kapoor[77] | 1/4 | Non-Executive Director |
| Sir Robert Lechler[78] | 1/1 | Non-Executive Director |
| Mark Walport | 4/6 | Non-Executive Director |
| John Noble | 6/6 | Non-Executive Committee Member |
| Steve Woodford | 4/6 | Non-Executive Committee Member |
[75] Mark Bailie was appointed as Non-Executive Director and Committee member on 19 February 2024
[76] Laura Wade-Gery was Non-Executive Director and Committee member until her end of term on 30 June 2023
[77] Rakesh Kapoor was a Non-Executive Director and Committee member until his end of term on 31 December 2023
[78] Sir Robert Lechler was appointed as Non-Executive Director and Committee member and on 19 February 2024
Attendees
Additional attendees are routinely invited to attend meetings to assist with committee business, including the National Director of Transformation, Chief Information Officer, Chief Operating Officer, Chief Strategy Officer, Head of the NHS England/DHSC Digital Policy Unit, Chief Delivery Officer, Director of Privacy and Information Governance, Chief Data and Analytics Officer and National Advisor to the Data Digital and Technology Committee.
Principal activities during the year
Matters considered by the committee included:
- the Federated Data Platform
- cyber resilience
- the Accelerating Access to GP Data programme
- NHS technology workforce
- frontline digitisation
- the vision for and functionality of the NHS App
- the digital therapeutics programme
- proposals for productivity through transformation
- digital workforce plan
- the terms of reference for the Advisory Group for Data
People and Remuneration Committee
Role of the committee
The committee’s role is to provide the Board with assurance on the management of NHS England workforce risks, and to oversee all aspects of strategic people management and organisational development for NHS England as an employer. The committee’s work includes reviewing the organisation’s gender pay gap and ensuring NHS England develops policies and actions to reduce it; reviewing progress in increasing black and minority ethnic (BME) representation at senior levels in the organisation; and initiatives relating to diversity and inclusion.
The committee ensures that NHS England has an effective remuneration policy that is in line with DHSC Executive and Senior Manager (ESM) Pay Framework for arm’s length bodies (ALBs). The committee considers and approves remuneration, benefits, and terms of service for senior executives covered by this pay framework before submission to DHSC for approval.
The committee also exercises the organisation’s powers to approve the appointment, suspension, and termination of ICB chairs, NHS trust chairs and non-executive directors.
The committee has delegated certain functions to the Executive HR Group and to the Regional Appointments and Approvals Committee. The committee receives regular reports from the group and the committee on cases considered and approved.
Committee members
The committee met nine times during the reporting period and the following table details membership and attendance:
| Members | Number of eligible meetings attended | Comment |
|---|---|---|
| Sir David Behan (Chair) | 9/9 | Non-Executive Director |
| Susan Kilsby[79] | 3/7 | Non-Executive Director |
| Richard Meddings | 6/9 | Chair of NHS England |
| Sir Andrew Morris | 6/9 | Non-Executive Director |
| Jeremy Townsend[80] | 0/5 | Non-Executive Director |
| Laura Wade-Gery[81] | 0/3 | Non-Executive Director |
| Professor the Baroness Watkins[82] | 7/9 | Non-Executive Director |
| Jane Ellison[83] | 1/1 | Non-Executive Director |
[79] Susan Kilsby’s directorship ended on 31 December 2023.
[80] Jeremy Townsend stepped down from the People and Remuneration Committee in October 2023.
[81] Laura Wade-Gery’s directorship ended on 30 June 2023.
[82] Professor the Baroness Watkins was appointed as a member of the People and Remuneration Committee on 1 April 2023.
[83] Jane Ellison was appointed as a Non-Executive Director and a member of the People and Remuneration Committee on 19 February 2024.
Attendees
Additional attendees are invited to meetings to assist with committee business. For 2023/24 these included the Chief Delivery Officer, the Director for Staff Experience and Leadership Development and the Director of Human Resources and Organisation Development.
Principal activities during the year
Matters considered by the committee included:
- the approach to improving equality, diversity, and inclusion within NHS England
- updates on Creating the New NHS England programme and the approach to hybrid working for the new NHS England
- approved the Fit and Proper Person Test Framework and the Leadership Competency Framework for implementation across the NHS
- management and leadership development in NHS England
- internal NHS England Freedom to Speak Up arrangements, and themes from staff feedback
- NHS England staff survey results and related actions
- approval of the revised policy for the appointment, suspension and termination of NHS trusts chairs and non-executives and ICB chairs
- approval, in line with DHSC pay framework, of the remuneration and appointment of several senior executives
- approval, in line with DHSC recommendation, of annual salary increases for ESM and medical colleagues on local pay arrangements
- approval of the appointment, remuneration, suspension, and termination of ICB chairs, with approval of the Secretary of State for Health and Social Care, and chairs of NHS trusts
Nominations Committee
Role of the committee
The committee oversees the succession plans for the NHS England Board and senior management, board composition and board evaluation.
Committee members
The committee met three times during the reporting period and the following table details membership and attendance:
| Members | Number of eligible meetings attended | Comment |
|---|---|---|
| Richard Meddings (Chair) | 3/3 | Chair of NHS England |
| Sir Andrew Morris | 3/3 | Deputy Chair, NHS England |
| Wol Kolade | 3/3 | Deputy Chair, NHS England |
| Michael Coupe | 3/3 | Non-Executive Director |
| Amanda Pritchard | 3/3 | Chief Executive Officer |
Attendees
The Director of Human Resources and Organisational Development is invited to attend meetings to assist with committee business.
Matters considered by the committee included:
- NHS England Board and board committee composition
- updates on non-executive director recruitment
- succession plans for national directors
Quality Committee
Role of the committee
The primary role of the committee is to support the Board in ensuring that areas concerning patient safety, the quality of care provided to patients and patient experience are continuing to improve and develop to meet the needs of patients in England. In doing so, the committee ensures strategies are continually improving quality, safety, and experience of care.
Committee members
The committee met five times in the reporting period and the following table details membership and attendance:
| Members | Number of eligible meetings attended | Comment |
| Professor Sir Munir Pirmohamed (Chair)[84] | 4/4 | Non-Executive Director |
| Professor Sir Simon Wessely (Chair)[85] | 4/5 | Non-Executive Director |
| Sir David Behan | 3/5 | Non-Executive Director |
| Dr Aidan Fowler | 5/5 | National Director of Patient Safety |
| Sir David Sloman[86] | 1/2 | Chief Operating Officer |
| Sarah Jane Marsh[87] | 2/2 | National Director of UEC and Deputy Chief Operating Officer |
| Sir Andrew Morris | 2/5 | Non-Executive Director |
| Mike Coupe[88] | 4/4 | Non-Executive Director |
| Dame Ruth May | 4/5 | Chief Nursing officer |
| Professor Sir Stephen Powis | 4/5 | National Medical Director |
| Amanda Doyle | 4/5 | National Director for Primary Care and Community Services |
| Vinod Diwakar | 1/3 | Medical Director for Secondary Care and Transformation |
| Charlotte McArdle | 3/5 | Deputy Chief Nursing Officer |
| Stella Vig[89] | 1/2 | Medical Director for Secondary Care and Transformation |
| Patient and Public Voice members | 4/4 |
[84] Professor Sir Munir Pirmohamed was Chair of the Quality Committee to 31 December 2023, when his directorship ended
[85] Professor Sir Simon Wessely was appointed as interim Chair of the Quality Committee from 1 January 2024
[86] Sir David Sloman left the organisation on 3 September 2023
[87] Sarah Jane Marsh was appointed as a member of the Quality Committee from 2 November 2023 following the departure of Sir David Sloman.
[88] Mike Coupe’s membership was transferred from the Quality Committee to the DDAT on 20 October 2023.
[89] Stella Vig was a member from November 2023 to March 2024
Attendees
Additional attendees are invited to attend meetings to assist with committee business. For 2023/24 these included the Chair of NHS England, Director of Health Inequalities, Director for Experience, Participation and Equalities, and the Head of Quality Strategy.
Principal activities during the year
Matters considered by the committee included:
- patient safety improvements
- utilisation of population health management within ICBs
- implementation of innovation strategies in life sciences
- work to improve maternity and neonatal services
- establishment of a National Children and Young Peoples’ Gender Dysphoria Research Oversight Board
- delivery plan for recovering access to primary care
- update on Martha’s rule
- update on healthcare acquired infections
The Quality Committee also held two informal roundtables to bring the clinical and service user voice into our board governance, and the outcomes of these roundtables were reported to the committee. The roundtables considered UEC and primary care patient safety.
Workforce, Training and Education Committee
Role of the committee
The committee’s role is to have oversight of all functions that ensure the NHS in England has a sufficient and inclusive workforce with the knowledge, skills, values, and behaviours to deliver compassionate, high-quality health and care to the people it serves.
Committee members
The committee was established on 1 April 2023 and met five times during the reporting period. The following table details membership and attendance:
| Members | Number of eligible meetings attended | Comment |
| Sir David Behan (Chair) | 5/5 | Non-Executive Director |
| Sir Andrew Morris | 1/5 | Non-Executive Director |
| Professor the Baroness Watkins | 5/5 | Non-Executive Director |
| Professor Dame Helen Stokes-Lampard[90] | 0/0 | Non-Executive Director |
| Professor Sir Mark Walport | 0/1 | Non-Executive Director |
| Dr Harpreet Sood[91] | 1/5 | Non-Executive Member |
| John Latham[92] | 5/5 | Non-Executive Member |
| Professor Andrew George[93] | 3/5 | Non-Executive Member |
[90] Professor Dame Helen Stokes-Lampard was appointed as a Non-Executive Director and committee member on 19 February 2024.
[91] Dr Harpreet Sood was previously a Non-Executive Director of Health Education England until 31 March 2023 and was appointed as a Non-Executive Committee Member of the Workforce, Training and Education Committee as of 1 April 2023.
[92] John Latham was previously a Non-Executive Director of Health Education England until 31 March 2023 and was appointed as a Non-Executive Committee Member of the Workforce, Training and Education Committee as of 1 April 2023.
[93] Professor Andrew George was previously a Non-Executive Director of Health Education England until 31 March 2023 and was appointed as a Non-Executive Committee Member of the Workforce, Training and Education Committee as of 1 April 2023.
Attendees
Additional attendees are invited to meetings to assist with committee business. For 2023/24 these included the Chief Workforce, Training and Education Officer, the Chief Delivery Officer, the Director for Staff Experience and Leadership Development and the Director of Operations and Oversight (Workforce, Training and Education Directorate) and the Deputy Chief Financial Officer – Strategic Finance.
Principal activities during the year
Matters considered by the committee included:
- development and implementation of the NHS Long Term Workforce Plan
- the approach to improving equality, diversity, and inclusion across the NHS
- developing the approach to management and leadership development across the NHS
- deep dives including medical expansion and retention
- quality of curriculum and training
- NHS staff survey
The New NHS England Committee
Role of the committee
The New NHS England Committee is a time-limited committee, to provide leadership and strategic oversight of the delivery of the New NHS England Programme.
Committee members
The committee met 11 times and the following table details membership, and the number of meetings attended by each member during the year:
| Members | Number of eligible meetings attended | Comment |
| Wol Kolade (Chair) | 10/11 | Deputy Chair, NHS England |
| Richard Meddings | 10/11 | Chair of NHS England |
| Sir Andrew Morris | 7/11 | Deputy Chair, NHS England |
| Sir David Behan | 11/11 | Non-Executive Director |
| Laura Wade-Gery[94] | 2/3 | Non-Executive Director |
| Amanda Pritchard | 6/11 | Chief Executive Officer |
| Julian Kelly | 5/11 | Chief Financial Officer |
| Steve Russell | 9/11 | Chief Delivery Officer |
[94] Laura Wade-Gery’s directorship ended on 30 June 2023.
Attendees
Additional attendees are invited to attend meetings to assist with committee business.
For 2023/24 this included the Director of Human Resources and Organisational Development and the New NHS England Programme Director.
Principal activities during the year
Matters considered by the committee included:
- overseeing delivery of the new NHS England Programme
- overseeing the high-level organisational design and priorities for the new NHS England, including ways of working and the approach to clinical integration
- considering and advising on organisational development and culture and equality, diversity, and inclusion for the new NHS England
- considering, approving, and receiving updates on the Filling of Posts Implementation process.
Board disclosures
Functional conflicts
NHS England maintains a policy on conflicts between functions, to comply with its duty under new section 13SB of the National Health Service Act 2006 (inserted by section 34 of the Health and Care Act 2022), to make arrangements to minimise the risk of conflicts between the exercise of the former Monitor regulatory functions and NHS England’s other functions, and to manage any conflicts that arise. The policy was revised and issued in July 2023 and, reflecting the statutory duty in section 13SB, contains arrangements for handling individual conflicts (notifiable to the Board Secretariat) and provides for formal escalation to a non-executive panel. The need to mitigate functional conflicts was considered as part of the setup of the Independent Patient Choice and Procurement Panel, where there are conflicts checks at each panel meeting and when panel members are allocated to cases. During 2023/24, the Board Secretariat were notified of no (zero) conflicts.
Register of Board members’ interests
Personal interests held by Board and committee members are managed in accordance with the NHS England Standing Orders and the Standards of Business Conduct policy. The organisation maintains a register of members’ interests to ensure that potential conflicts of interest can be managed appropriately. Board members and executives are also required at the beginning of each Board and committee meeting to declare any personal interest they might have in any business on the agenda and abstain from relevant Board or committee discussions as required. Where potential conflicts arise, they are recorded in the Board and committee minutes along with any appropriate action to address them. A copy of the register of interests is available on our website.
Details of related party transactions, where NHS England has transacted with other organisations during the year to which a Board or an executive is connected, are set out in Note 19.
Disclosure of personal data breach incidents
NHS England follows the Data Security and Protection Incident Reporting process guidance in the reporting of personal data breach incidents. This is in line with the UK General Data Protection Regulation (UK GDPR).
The guidance sets out the reporting requirements for NHS organisations where a potential or actual incident may lead to a personal data breach defined under UK GDPR. All organisations that have access to NHS patient data and systems must use the toolkit to provide assurance that they are practising good data security, and that personal information is handled correctly.
The scoring criteria reference the circumstances where notification to the Information Commissioner’s Office (ICO) may not be necessary.
In 2023/24, NHS England reported 233 personal data breaches to the DPO. Seven of these were reported to the ICO voluntarily or where they met the threshold for reporting under UK GDPR.
Directors’ third-party indemnity provisions
NHS England has the appropriate director’s and officer’s liability indemnity provided by NHS Resolution in place for legal action brought against, among others, its executive and non-executive directors. During 2023/24, there was one ongoing legal claim brought against NHS England during 2022/23 (disclosed in our prior year report), concerning alleged conduct of an NHS England director. This claim was indemnified by NHS Resolution.
Directors’ responsibility statement
The Annual Report and Accounts have been reviewed in detail by NHS England’s ARAC and Board. At each point it has been confirmed that the Annual Report and Accounts, taken as a whole, are considered to be fair, balanced, and understandable. They provide the information necessary for NHS England’s stakeholders to assess the business model, performance, and strategy.
Human rights
NHS England supports the Government’s objectives to eradicate modern slavery and human trafficking. The Board approved the NHS England Slavery and Human Trafficking Statement for the financial year ending 31 March 2024 on 17 April 2024. The statement for 2022/23, published in March 2022, is available on our website.
Statement of accounting officer’s responsibilities
Under the National Health Service Act 2006 (as amended), the Secretary of State for Health and Social Care (with the consent of HM Treasury) has directed NHS England to prepare, for each financial year, a statement of accounts in the form and on the basis set out in the Accounts Direction. The accounts are prepared on an accruals basis and must give a true and fair view of the state of affairs of NHS England and of its income and expenditure, statement of financial position and cash flows for the financial year.
In preparing the accounts, the Accounting Officer is required to comply with the requirements of the Government Financial Reporting Manual (FReM) (HM Treasury, June 2024) and in particular to:
- observe the Accounts Direction issued by DHSC, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis
- make judgements and estimates on a reasonable basis
- state whether applicable accounting standards, as set out in the Government FReM, have been followed and disclose and explain any material departures in the financial statements
- prepare the financial statements on a going concern basis
- confirm that the Annual Report and Accounts are fair, balanced, and understandable, and take personal responsibility for the Annual Report and Accounts and the judgements required for determining that they are fair, balanced, and understandable
The National Health Service Act 2006 (as amended) schedule A1 paragraph 15(4) states that the Chief Executive shall be the Accounting Officer of NHS England.
The responsibilities of the Accounting Officer, including responsibilities for the propriety and regularity of the public finances for which the Accounting Officer is answerable, for keeping proper records and for safeguarding NHS England’s assets, are set out in Managing Public Money (HM Treasury, July 2013, as amended May 2023).
As the Accounting Officer for NHS England, I have taken the steps that I ought to have taken to make myself aware of any relevant audit information and to establish that NHS England’s auditors are aware of that information. So far as I am aware, there is no relevant audit information of which the auditors are unaware.
Governance statement
This governance statement covers NHS England, its system leadership role of the NHS, directly commissioned health services, and oversight and assurance of the commissioning system.
As Accounting Officer, I have responsibility for the system of internal controls supporting and enabling the achievement of NHS England’s aims and objectives, while safeguarding public funds and the assets for which I am personally responsible in accordance with Managing Public Money and as set out in my Accounting Officer appointment letter.
This includes assurance of several organisations which are part of the wider commissioning system, including those organisations hosted by NHS England.
My responsibilities in relation to the oversight of ICBs are set out below.
Board arrangements
Information on our Board and its committees is set out in the board committees section.
Freedom to Speak Up
Our report on whistleblowing disclosures made by NHS workers is published on our website.
Government functional standards
Functional standards set out what needs to be done, and why, for different types of functional work and were mandated for use in Governmental departments and their ALBs from the end of March 2022. The extent to which these standards are adopted across NHS England varies, and certain elements of the standards are not applicable to the organisation.
Governance arrangements and effectiveness
Governance framework
The Governance Manual brings together all key strands of governance and assurance, including Standing Orders, Standing Financial Instructions (SFIs), Scheme of Delegation, Standards of Business Conduct Policy, Risk Management Framework and the three lines of defence model.
Assessment against the Corporate Governance in Central Governance Departments: Code of Good Practice 2017 Compliance Checklist
As part of implementing best practice, an assessment is undertaken each year against this checklist from HM Treasury. NHS England is compliant* against the provisions of the code, with the following exceptions:
| Ref | Code provision | Exception |
|---|---|---|
| 4.7 | Through the Board Secretariat, the Department provides the necessary resources for developing the knowledge and capabilities of Board members, including access to its operations and staff | This responsibility is shared between the Chair, the Chief Executive’s private office and the Board Secretary |
| 4.11 | The Board Secretary’s responsibilities include arranging induction and professional development of Board Members | This responsibility is shared between the Chair, Chief Executive’s private office and the Board Secretary |
| 5.5 | The Head of Internal Audit is periodically invited to attend Board meetings, where key issues are discussed relating to governance, risk management, or control issues across the department and its ALBs | The Head of Internal Audit routinely attends ARAC meetings |
*It should be noted that the following provisions in the code do not apply to NHS England: Sections 1, 2.3, 2.11, 3.3a, 3.3b, 3.3c, 3.6e, 3.7, 3.8, 3.9, 3.14, 3.19, 4.9, 4.12, 4.13, 4.14, 5.7, 5.8 and 6.
Corporate assurance
The NHS England corporate assurance framework, set out below, helps to provide assurance on organisational stewardship and the management of significant risks to organisational objectives.
| Assurance activity | How does it add value? |
|---|---|
| Organisational change framework Guidelines for assessing and implementing major changes across the organisation. | The framework provides a consistent approach to thinking about the impact of organisational change, including on people, infrastructure, financial and legal issues. |
| Risk management framework Our approach to managing risk, including tools and methodologies for identifying, assessing, documenting and reporting risk. | The framework enables a consistent approach to be taken across the organisation, allowing identification of cross-directorate risks and challenges. It provides a mechanism for managers to identify risks with a route of escalation to those accountable. |
| SFIs, Scheme of Delegation and Standing Orders These documents protect both the organisation’s interests and officers from possible accusation that they have acted less than properly. | Together, these documents ensure that our financial transactions, accountabilities and responsibilities are carried out in accordance with the law and government policy in order to achieve probity, accuracy, economy, efficiency and effectiveness. |
| Programme management framework The policies, tools, methodology and resources that provide an approach to managing, controlling and assuring the delivery of projects and programmes in the organisational portfolio. | Provides staff with a framework to manage, control and deliver projects and programmes. Provides the organisation with consistency of reporting and monitoring, confidence of delivery of outcomes to enable decision-making and better resource control. |
| Third-party assurance framework Guidelines for the assurance required for managing third-party contracts. | Ensures directorates responsible for major contracts assign a contract manager and put arrangements in place to monitor supplier performance. Obtains assurance over the services provided. |
| Corporate policy framework The methodology and approach for creating, maintaining and amending policies. | Provides an approach to help ensure policy documents are not developed in isolation, so they are balanced against the priorities of the organisation. |
We work with the support of both our internal and external auditors to strengthen and embed our assurance framework. All directorates and regions have designated leads with responsibility for ensuring that risk management, implementation of internal audit actions and other key assurance activities are properly carried out, including regular reporting and escalation.
During 2023/24, the corporate governance and compliance team worked with teams across the organisation to embed controls and underpin processes including by:
- ensuring that officers undertook staff declarations in line with the standards of business conduct policy, which was updated on 1 January 202485
- developing refreshed strategic and operational risk registers
- carrying out targeted interventions with teams to ensure the timely completion of actions arising from internal audit reviews
Management assurance
Throughout 2023/24, the Board has been provided with regular performance updates on the implementation of the priorities and programmes committed to in the NHS Long Term Plan and NHS England’s business plan.
Board reporting integrates performance against constitutional standards, NHS Long Term Plan commitments and workforce and quality metrics.
Individual programme boards and oversight groups, each with responsibility for delivery of their programme, meet frequently, with representatives from national and regional teams.
Assuring the quality of data and reporting
The Board has agreed the information it requires to carry out its duties. The Board is confident that performance reports have been through appropriate management review and scrutiny, and that reporting continues to evolve to meet changing organisational needs.
Risk governance
The Board sets the organisation’s risk appetite and oversees the organisational risk profile to ensure key risks are mitigated within the agreed appetite level. A review and refresh of the Board’s risk appetite commenced in 2023/24 and Board approval and subsequent implementation was scheduled from May 2024. The Board discusses the most significant risks and actions identified to mitigate their likelihood and impact.
ARAC is responsible for reviewing the establishment and maintenance of an effective system of governance, risk management and internal control covering NHS England’s activities. The committee holds the organisation to account on the effectiveness of risk management processes and evaluates the effectiveness of the risk management framework.
To ensure robust oversight of transferred key risks following mergers with NHS Digital on 1 February 2023 and Health Education England on 1 April 2023, a CSRC was established as a sub-committee of ARAC, and a Workforce, Training and Education Committee was established as a committee of the Board.
The Executive Risk Group is responsible for assuring ARAC about how risks across the organisation are being managed. ARAC oversees implementation of NHS England’s risk management framework. The NHS Executive also periodically reviews the organisation’s most significant risks and, when appropriate, undertakes in-depth review.
The Chief Executive Officer, supported by senior management, provides leadership, and articulates their continued commitment to risk management through the organisational risk management framework.
The executive team collectively owns the Strategic and Operational Risk Registers and has nominated a responsible officer for each of the risks that are included within them. Individual executives are responsible for managing risk at a directorate and regional level. Each directorate holds its own risk register and is required to review its risks on a regular basis.
Principal risks
The Strategic and Operational Risk Registers contain over 40 risks to the organisation. The SRR considers the principal risks that could impact delivery of NHS England’s strategic objectives. NHS England’s risk profile adapts throughout the course of the year in response to events and emerging priorities. NHS England’s considers its most significant risks to be those which have received the highest pre-mitigation impact and likelihood scores. The six risks detailed below were NHS England’s most significant risks in 2023/24. The mitigation plans for each extend to 2024/25 or 2025/26 and remain under regular review through NHS England’s risk management governance framework:
| Risk | Key mitigations delivered in 2023/24 |
|---|---|
| Demand and capacity: Risk of failure to create additional capacity that meets demand, which would have an adverse impact on patients’ outcomes. | A redesign of the Elective Recovery Fund was introduced in the planning guidance to incentivise additional activity in the most impactful areas and minimise unnecessary activity. Capacity was increased across a range of services, including: general and acute beds; £1 billion of revenue funding and £250 million capital funding were devolved to deliver an additional 5,000 beds in winter virtual wards: 10,000 extra virtual beds were created Ambulance hours on the road were expanded by 7% Step-down capacity and Care Transfer Hubs; these are now in place in every acute provider Additional winter surge plans for UEC |
| Workforce capacity: The NHS workforce is not sufficiently skilled or resourced to meet the immediate or future needs of the population | In 2023/24 workforce capacity was further impacted by industrial action An Incident Management Team was established, and workforce contingency plans were developed to manage its impact. NHS England engaged with the DHSC and Trade Unions to support the development of non-pay options for negotiations The NHS Long Term Workforce Plan seeks to address the imbalance between population health needs and the extent and nature of medical/clinical training and work opportunities, via a number of actions over a 15-year period. Whilst the delivery of the plan is tied into a number of national levers, it presents an opportunity to right size and right skill the NHS workforce The commitment to recruit 50,000 nurses was delivered six months ahead of schedule; 72% of nursing international recruitment target was achieved by September 2023 and the annual turnover rate had reduced to 11.5% in October 2023 |
| Quality of care: There is a risk to care quality (safety, effectiveness and experience) for patients, carers and families if NHS England does not satisfactorily deliver its statutory functions; commissioning and regulatory duties; implement national policy and strategy that cover assurance, improvement and planning functions. | NHS England has been supporting ICSs with the development of System Quality Groups, quality strategies and wider quality requirements Good Quality monitoring and intelligence sharing systems have been implemented at regional and ICB level Good Quality risk escalation processes are in place from ICB to NHS England regional teams and regional to national teams, and vice versa NHS England is developing an Operating Model for Quality, to further integrate the focus on quality across corporate reporting in the new organisation |
| Data and digital security: There is a risk that malicious cyber actors deploy widespread, catastrophic cyber-attacks against the NHS leading to patient harm and/or data misuse causing reputational and financial consequences. | The DHSC/NHS England JCU centrally invests in technology and processes to limit security risks posed by systems. A Cyber Risk Management Board is in place to ensure risks for wider NHS England around broader technology investment are understood The JCU runs cyber incident exercises at national level and requires local organisations to run cyber incident exercises that test downtime procedures and recovery capabilities. The aim is to minimise impact in case of a successful attack through robust response processes NHS England has secured programme funding until March 2025, which will allow further promotion of cyber security across the NHS Estate in line with the Cyber Security Strategy for Health and Adult Social Care that was published in March 2023 |
| NHS Funding: There is a risk that strategic priorities do not have adequate funding, which could create material additional financial pressures. | Spending Review preparations, with senior strategic oversight, and financial planning for the medium to long term are underway. Horizon scanning to mitigate the risk that beyond 2024/25, the NHS does not have sufficient funding to deliver its medium term strategic objectives. Tracking of in-year delivery of efficiencies and activity on a monthly basis, as well as reviewing the efficiency assumption for reasonableness to drive further savings through the NHS Productivity and Efficiency Programme. |
| Location, Function, Condition and Age of the NHS Estate: Due to advancements in technology and improved care pathways, 45% of estates infrastructure (including RAAC) is not fit for the services the NHS delivers today. This results in disruption to productive clinical services and can lead to significant risks to patient and staff safety. | NHS England is working with ICSs to pull together infrastructure and investment strategies that set out plans for an estate that is smarter, fairer, better, stronger and greener. Models to support future capital funding decisions are being developed. By April 2025, RAAC to be removed from all known hospitals that do not require full redevelopment Continue to make the case for the hospitals that require full redevelopment to eliminate RAAC from the NHS estate by 2030 |
NHS oversight and support
The NHS Oversight Framework describes NHS England’s approach to oversight and is built around five national themes that reflect the ambitions of the NHS Long Term Plan and apply across trusts and ICBs. These are: quality of care, access and outcomes; preventing ill-health and reducing inequalities; people; finance and use of resources; and leadership and capability.
In line with the framework, organisations’ support needs are regularly assessed, and each organisation is allocated into one of four support segments. Decisions on which support segment organisations are allocated to are routinely reviewed and updated throughout the year and published on our website.
NHS England has met regularly with each ICB throughout the year, reviewing performance and the support needs of each ICB and provider across their ICS footprint. At the end of 2023/24 NHS England was providing intensive support via the Recovery Support Programme to three ICBs and 20 providers, while 22 ICBs and 77 providers were in receipt of segment three support coordinated by their NHS England regional team.
NHS England is committed to ensuring that the model of oversight remains relevant and effective. In our 2023/24 business plan we committed to work alongside ICBs to review the oversight arrangements to ensure these were effective and proportionate. We have worked with stakeholders to develop proposals that we have consulted on in the early part of 2024/25 ahead of implementation.
Quality oversight and assurance
All NHS organisations have responsibility for the quality of services, and both ICBs and NHS England have a statutory duty to act with a view to securing continuous improvement in quality.
NHS England, uses the National Quality Board (NQB) definition of quality as care that is safe, effective, provides a personalised experience, is well-led, sustainable and equitable. Our approach to managing quality is based on methods of quality management systems (combining quality planning, improvement and control activities) and the need to view quality, finance, operations and workforce matters together.
The Quality Committee ensures NHS England’s strategies are continually improving quality, safety, and experience of care. Executive level quality meetings reporting in are the Quality and Performance Committee (QPC) to scrutinise quality, performance, workforce and finance issues, and the Executive Quality Group (EQG) to provide oversight and scrutiny of care quality across regions and receives regional quality insight from ICBs and providers. The EQG is co-chaired by the National Medical Director and Chief Nursing Officer and brings together Regional Medical Directors, Regional Chief Nurses, Directors of Clinical Quality and senior national colleagues, including the Directors for Patient Safety, Patient Experience and Quality and Clinical Effectiveness.
Additionally, NHS England hosts and co-chairs the NQB which champions the importance of quality and drives system alignment across key health and care ALBs (NHS England, CQC, UKHSA, NICE, Health Services Safety Investigations Body, DHSC, Office for Health Improvement and Disparities, National Guardian’s Office and Healthwatch England). NQB discussions are also shared at the Executive Quality Group and Quality and Performance Committee.
Recovery Support Programme
Where a trust is in breach or suspected breach of the conditions of its provider licence, NHS England can use its statutory powers, including legal powers of direction, to intervene in line with the NHS Enforcement guidance.
During 2023/24, seven trusts entered, and five trusts exited the Programme and, by the end of 2023/24, NHS England was providing intensive support via the Recovery Support Programme to 20 trusts.
Regulating independent providers of NHS services
All independent providers of NHS services are required to hold a provider licence, unless exempt, under DHSC regulations. The provider licence gives NHS England the ability to safeguard continuity of services for patients if an independent provider gets into difficulty. As of 31 March 2024, 136 independent providers held a provider licence, as did three NHS-controlled providers.
Under the Commissioner Requested Services policy, commissioners must decide which of their services need the protections of the licence’s continuity of services conditions. Under the ‘Hard to Replace’ policy NHS England can identify providers that should be subject to the continuity of services conditions due to the scale or complexity of their services. As of 31 March 2024, in total 54 licensed providers were subject to the licence’s continuity of services conditions.
During 2023/24, no new formal enforcement action was taken with any independent providers, and as of 31 March 2024, no enforcement undertakings were in place.
Mergers and acquisitions
NHS England is responsible for reviewing statutory transactions between trusts. Our assurance process for significant transactions includes reviewing the strategic cases and full business cases for transactions, to ensure that the transactions have a sound strategic rationale, a deliverable benefits realisation plan, and that all statutory requirements have been met before the transaction can proceed.
We offer bespoke support to trusts considering or proceeding with mergers or acquisitions and help ensure clarity about the intended benefits. Significant transactions completed during the reporting period included:
- Yeovil District Hospital NHS Foundation Trust acquired Somerset NHS Foundation Trust on 1 April 2023, with the newly enlarged trust retaining the Somerset NHS Foundation Trust name
- St Helens and Knowsley Teaching Hospitals NHS Trust acquired Southport and Ormskirk Hospital NHS Trust on 1 July 2023, with the newly enlarged trust renamed Mersey and West Lancashire Teaching Hospitals NHS Trust.
Assurance of the commissioning system
One of NHS England’s functions is to directly commission clinical services which are more appropriately arranged at a national or regional level, including specialised services, health and justice services and those services which support our armed forces and veterans.
Following the establishment of ICBs and having established the principle that commissioning decisions should be made as close to the patient as possible, during 2023/24, some of the commissioning responsibility for these services were in the process of being delegated to ICBs.
Specialised services
Specialised services support people with a range of rare and complex conditions. They often involve innovative treatments for patients with rare cancers, genetic disorders, complex medical conditions, or surgical needs. The specialised commissioning allocation for all specialised services was £25 billion at the end of 2023/24. Most of this allocation is held across seven regional teams for commissioning specialised services, with the balance held centrally to fund national budgets such as the Cancer Drugs Fund and other national programmes.
Since April 2023, commissioning responsibility for 59 specialised services was delegated to nine statutory joint committees formed between ICB and NHS England regions. Following careful assessment and preparations, these services were fully delegated to ICBs in the East of England, Midlands, and the Northwest, commencing April 2024.
NHS England regional teams were the responsible commissioners for the retained (non-delegated) services, working in conjunction with the appropriate national specialised commissioning teams.
NHS England acted as the accountable commissioner for both delegated and retained services, maintaining oversight through regional accountability reporting lines. During 2023/24, the Delegated Commissioning Group for Specialised Services continued to provide strategic direction for the 59 delegated services, set national standards, approve key national transformational gateway documents, and bring together the responsible and accountable commissioners from across the country. Correspondingly, the National Commissioning Group (NCG) for Specialised, Health and Justice Armed Forces Services continued to set strategic direction, set standards, and manage gateway approvals, as well as oversee commissioning of those retained services commissioned by NHS England.
Health and justice
Health and justice services are supported through the Health and Justice Delivery and Oversight Group nationally, this feeds into the NCG. NHS England Regional teams are the responsible commissioners for the retained health and justice services, working in conjunction with the appropriate national health and justice teams.
Armed forces
Armed Forces directly commissioned services are the responsibility of the national armed forces commissioning team. This is overseen by the Armed Forces Oversight Group which feeds into the NCG.
Delegation of primary care services to ICBs
Delegation has been at the forefront of our vision to support more integrated care by ensuring local health and care leaders take collective responsibility for system performance and the transformation of care to improve population health, including primary care. This has strengthened ICBs ability to design care pathways and integrate services, to better meet local priorities and ultimately improve local population health outcomes. 2023/24 was the first year that all 42 ICBs held delegated responsibility for all four primary care services – primary medical, dental (primary, secondary and community), general ophthalmic and pharmaceutical services – with NHS England retaining accountability through a delegation agreement.
NHS England sets out expectations – and obtains assurances that these functions are being discharged effectively – through the Primary Care Commissioning Assurance Framework.
Vaccinations and screening – governance and the Section 7A agreement
The Vaccination and Screening Directorate commissions 11 screening programmes, 20 immunisation programmes, and Child Health Information Services (CHIS). The annual NHS Section 7A public health functions agreement between NHS England and DHSC sets out the arrangements under which the Secretary of State delegates responsibility to the NHS England Board for commissioning certain NHS public health services, including:
- NHS national cancer and non-cancer adult, children, and newborn screening services
- NHS national routine immunisation services for adults, children, and young people
- CHIS including the Red Book
- NHS Sexual Assault Referral Centres (led by Health and Justice Commissioning)
- NHS public health services for people in secure and detained settings (led by Health and Justice Commissioning)
- provision of an effective screening quality assurance service
- promotion of healthcare public health
- seasonal vaccination programmes including flu and COVID-19.
Internal assurance in 2023/24 was provided through the quarterly NHS England Public Health Oversight Group and latterly through the NHS England Delivery and Transformation Board. These were informed by programme-specific boards for screening, vaccinations, and CHIS programmes.
Other assurance
Information Governance
The Information Governance (IG) Delivery teams advise on and assure Data Protection Impact Assessments (DPIAs), and draft and advise on data sharing agreements, data processing agreements and privacy notices, to meet data protection requirements, minimise privacy and confidentiality risks and improve transparency. The team also operate an IG helpline, which provides general IG advice and support. In 2023/24 the helpline service handled 4,144 enquiries.
PTT also advises on the implementation of the digital and data functions which transferred from NHS Digital (data safe haven functions), including agreeing Secretary of State directions and statutory requests for the collection and analysis of data, and advising on compliance with the Statutory Guidance on NHS England’s Protection of Patient Data. During 2023/24 the team supported the development and implementation of 11 new Directions and 23 Direction Specifications.
The Records Management team provide strategic and operational advice on records management across the organisation, contribute to the development of records management policy for the NHS, set records management standards, operate compliance processes, and manage legacy records. It also manages NHS England’s Information Asset Register (IAR) and during 2023/24 worked to successfully merge the legacy NHS Digital, Health Education England, and NHS England IARs, into one combined IAR.
Information Governance Risk and Assurance
The IG Risk and Assurance team provides audit and assurance of IG compliance, including assurance of key suppliers and CSUs, and provides assurance on external data sharing and access. It is also responsible for the NHS England information risk management framework
and carries out day-to-day operational activities of the SIRO (working with IT Operations and Cyber Security), including supporting Information Asset Owners.
PTT co-ordinates and assures NHS England’s annual DSPT submission. In 2023/24 NHS England met all of the mandatory DSPT standards. The DSPT requires all organisations that handle NHS data to self-assess their performance against the National Data Guardian’s 10 data security standards every year, to provide assurance over their data security and handling of personal information. Independent audit teams assessed NHS England’s submission and evidence against a mandatory assessment framework and tested the approach used to ensure a robust self-assessment had been undertaken. The outcome of the audit was ‘substantial’ (green) rating, finding the framework of governance, risk management and control in relation to the submission was adequate and effective.
Data functions transferred from NHS Digital – Assessment under section 13U(2)(d) of the National Health Services Act
Under section 13U(2)(d) of the National Health Services Act 2006, the annual report must contain an assessment of how effectively NHS England has discharged its relevant data functions (Assessment). Relevant data functions are defined in section 253(3) of the Health and Social Care Act 2012 (2012 Act) and broadly comprise of the digital and data functions that transferred from NHS Digital to NHS England on 1 February 2023 when the organisations merged. We refer to these as the data safe haven functions below.
In preparing the Assessment, NHS England has had regard to the guidance issued by the Secretary of State for Health and Social Care under section 274A of the 2012 Act: Statutory guidance: NHS England’s protection of patient data, published 23 May 2023 (Statutory Guidance) and the requirements set out in the Statutory Guidance in relation to the Assessment.
The Assessment provides a summary of how NHS England has complied with its obligations during 2023/24.
Statutory protections
In relation to the exercise of the data safe haven functions during 2023/24:
- NHS England continues to publish all data it collects and obtains, unless restricted from doing so by law. Information about the data we publish is available on NHS England and legacy NHS Digital websites
- NHS England only disseminates data where it has a specific legal power to do so and cannot disseminate confidential patient data unless the recipient has a legal basis under the common law duty of confidentiality to receive and process it. The legal basis for sharing data is assessed as part of information governance procedures and in DPIAs on operational activity. Where NHS England shares directly identifiable patient data or de-identified patient data with third parties for planning, commissioning and research, the legal basis to share data is assessed through the Data Access Request Service with advice from the NHS England Advisory Group for Data (AGD) where applicable
- NHS England has procedures for the making and consideration of requests under section 255 and has published these on our website
- NHS England complies with directions from the Secretary of State for Health and Social Care to establish information systems under section 254, including the existing directions to NHS Digital that were transferred to NHS England to ensure continuity in data collections. During 2023/24, 11 new Directions were issued to NHS England and 23 Direction specifications were amended
- NHS England publishes all directions received from the Secretary of State, all requests to establish information systems under section 255 (Section 255 Requests) and all Data Provision Notices issued under section 259 of the 2012 Act, so there is full transparency on what IT system delivery functions NHS England is carrying out, what data is being collected and analysed, and for what purpose.
- NHS England publishes transparency information for the public on its website in line with its UK GDPR responsibilities about how it collects, uses, and shares data with others.
The level of transparency is the same as NHS Digital achieved prior to the transfer of its functions to NHS England and we strive to be even more transparent in the future:- privacy information relating to transferred data functions is published on the UK GDPR Register pages of our website. Other privacy notices are available through the NHS England Privacy Notice pages of the website. The need to consolidate legacy organisational privacy notices has been identified and is part of the PTT Sub-Directorate work plan in 2024/25
- the need for improvements to the data release registers to address gaps and ensure there is a robust process for updating internal and external data release registers has been identified and will be part of the Data and Analytics Sub-Directorate work plan in 2024/25. Internal and external data release registers are published on our website
- NHS England will have regard to any advice given to it by the Confidentiality Advisory Group (CAG). No such advice has been sought or provided in the 2023/24 financial year
- NHS England has established and sought advice from AGD on specific data access requests and to support the development and maintenance of precedents, standards, and guidance on data access. More information about AGD is set out below.
Governance, scrutiny and accountability
NHS England has established organisational governance arrangements which support high standards of protection for data processed in the discharge of its data safe haven functions.
The Board’s responsibilities for the exercise of the data safe haven are provided in the Corporate Governance Report and published on the website.
Organisational responsibilities
The new NHS England operating model has been designed to comply with the Statutory Guidance to ensure that responsibilities and accountabilities for using the data derived from the exercise of the data safe haven functions are separate from the functions providing assurance and advice on this (to ensure there are no conflicts of interest).
A Conflicts of Interests Policy is in place within NHS England and managing conflicts of interest is also part of the Standards of Business Conduct Policy. An additional specific conflicts of interest policy relating to the role of the SIRO is not yet in place but is part of the PTT work plan for 2024/25. In the meantime, any potential or actual conflicts of interest would be addressed through the Deputy SIRO acting instead of the SIRO.
The SIRO has put in place appropriate accountability and assurance arrangements to ensure that information risk, including security and IT operational information risk, is appropriately managed and mitigated. This includes reporting and escalation arrangements to the SIRO from the CISO and Director of Cyber Operations in relation to internal NHS England cyber and security risks. The roles of the SIRO, Caldicott Guardian, Data Protection Officer and Chief Information Security Officer are also documented in internal NHS England staff policies.
Independent advice
NHS England has operational arrangements in place for obtaining independent advice when exercising its transferred data functions. It has also appointed members to CRSC and DDAT with specialist data security expertise. NHS England has arrangements in place under a memorandum of understanding for seeking advice from CAG. It meets regularly with the National Data Guardian and the ICO. It has also established the AGD under Terms of Reference which reflect all of the functions expected of an advisory data group.
During 2023/34 NHS England has sought independent advice and feedback, including from AGD, the National Data Guardian, the Information Commissioner and from programme specific specialist IG groups, the Health Data Patient and Public Engagement and Communications Advisory Panel, patient groups and privacy groups.
In 2023/24 a range of programme specific expert advisory panels and groups were established to support the implementation of the FDP including the FDP Check and Challenge Group, a Specialist IG Group and a Data Governance Group. More information about FDP and these Groups are published on our website.
Advisory Group for Data
The Statutory Guidance sets out expectations that NHS England should establish a data advisory group, accountable to the SIRO, to provide advice and assurance on access to NHS England data with the ability to provide advice and assurance on a range of matters. The Guidance sets out how the Group should be comprised and operate, what it should be able to provide advice on, that its Terms of Reference and minutes should be published, and its operating processes should be transparent in line with the approach previously taken by the NHS Digital Independent Group Advising on Release of Data (IGARD).
At NHS England’s invitation, the previous members of IGARD agreed to form an interim data advisory group, called the AGD, together with representatives from NHS England in line with the Statutory Guidance, in February 2023. The interim AGD included independent members across specialisms including law, ethics, research and clinical practice, including practicing primary care clinicians. Also, independent lay members, internal representatives from each of the DPO, Caldicott Guardian and Data and Analytics functions, and a representative of the SIRO. Membership during the 2023/24 financial year has not yet included specialist members from adult social care or clinicians from secondary care.
The recruitment plan for AGD to be delivered by the PTT function in 2024/25 will seek to appoint additional members with this expertise to enable AGD to fully operate in line with the expectations set out in the Statutory Guidance in the future.
Representatives from the interim AGD together with representatives from the NDG’s office formed a working group to support the development and drafting of the AGD Terms of Reference by NHS England. The draft Terms of Reference were subject to consultation with and feedback from CRSC, DDAT and NHS England’s Executive Corporate Group. The NDG and Department of Health and Social Care were consulted for their views in line with the Statutory Guidance. Experience from operating AGD as an interim Group fed into the development of the draft Terms of Reference and AGD also reviewed the drafts and provided feedback. AGD operated as an interim Group until the final version of the AGD Terms of Reference, were formally approved by DDAT on behalf of the Board in March 2024, following Executive approvals. The approved AGD Terms of Reference and minutes from its meetings with its advice are published on the NHS England website.
From 1 February 2023, when it was established on an interim basis, to 31 March 2024, AGD met to provide NHS England with advice 51 times. This included advising on:
- over 220 matters relating to applications for external access to data
- 8 new Directions and 2 amendment Directions
- several new precedents
- 4 proposed internal uses of data
Full details of matters AGD have considered, and advice provided are contained within their published minutes.
Procedures for internal access to data
The previous legacy NHS Digital information governance procedures for accessing identifiable data for analysis have been followed to support requests for NHS England analysts to access identifiable data collected and analysed under Directions for other statutory purposes (Internal Analysis Approval Process). This includes requests for data to be de-identified and transferred into an NHS England SDE under the NHS England De-Identified Data Analytics and Publication Directions 2023. Advice and assurance from PTT, the Caldicott Guardian function and AGD is sought on these requests, which are documented and approved on behalf of the SIRO and supported by Data Protection Impact Assessments. Only one new request was approved in 2023/24. This was subject to advice from AGD.
Stakeholder engagement
NHS England has a range of existing and programme specific arrangements in place for engaging with key stakeholders outlined in the Statutory Guidance in relation to the exercise of its relevant data functions as described above. Before establishing an information system under a Direction or Section 255 Request, NHS England also has a responsibility to consult a range of stakeholders including those from whom data is to be collected and those who may wish to use data obtained. This is done through a variety of regular and specific forums and meetings for each Direction and Section 255 Request.
Engagement with devolved administrations
NHS England has published its procedure for managing Section 255 Requests and follows this in relation to any such requests. In 2023/24 NHS England worked with Digital Health and Care Wales in relation to the development of a request and technical arrangements to use NHS login for health services supplied by third party Apps in Wales.
There is ongoing operational engagement between the teams with responsibility for collecting and analysing data in relation to Section 255 Requests from devolved administrations.
Technical measures and controls
NHS England has a number of de-identified technical data processing environments where data which has been de-identified is analysed for the purposes of fulfilling its statutory functions under the NHS England De-Identified Data Analytics and Publication Directions 2023. This includes data processed in the Unified Data Access Layer, the National Commissioning Data Repository and the National SDE. From March 2024 this included the national instance of the FDP for national products which have transitioned from the National Data Platform.
During 2024/25 existing de-identification processes carried out by Data Services for Commissioning Regional Office will be replaced with a new Privacy Enhancing Technology service, the NHS-PET solution procured by NHS England as part of the FDP Programme which will enhance privacy protection and the separation of technical data processing environments for identifiable data and de-identified data.
Progress on NHS England’s SDE is reported in the Transforming health and care section.
Arrangements with third parties for data processing on behalf of NHS England
NHS England uses standard data processing terms which comply with UK GDPR requirements when it appoints data processors, or it works with the internal legal team to review any third party data processing terms to ensure that terms comply with UK GDPR and meet NHS England’s security and data protection standards.
Transparency and reporting
NHS England has continued to operate with the same degree of transparency as NHS Digital previously did and publishes the information required by the Statutory Guidance, as outlined above. This includes maintaining the external data use register and establishing a new internal data use register where data is transferred from an identifiable environment to a de-identified environment under Directions. Improvements to the data use registers have been identified, including improving the content, to ensure that it is clearer to the public what the purposes are for which data is being shared. Also putting in place a new Standard Operating Procedure for updating the data use registers.
Steps taken to protect confidential information
NHS England has published a summary of the way in which it protects and safely uses data in the new NHS England.
A significant part of how we also protect confidential information is through complying with the standards set out in the NHS DSPT. In 2023/24 NHS England met all of the mandatory standards required by the DSPT.
Areas for improvement
In addition to the specific improvements identified above, we have identified a number of general continuous improvement activities to improve our compliance with the Statutory Guidance, including consolidation of legacy business processes and guidance, developing clear and accessible Standard Operating Procedures, updating and assuring internal records and identifying additional assurance activity, including regular assurance reviews to by AGD of data access requests that have been processed under approved precedents to ensure precedents are being applied appropriately.
Independent Advice and Consultation with the National Data Guardian
We have sought advice from the AGD and considered their Annual Report to inform this Assessment. We have also consulted the NDG for her views on this Assessment and have considered her feedback when finalising this Assessment.
Sharing of this Assessment
A copy of the Annual Report containing this Assessment will be shared with the NDG, the Information Commissioner and the Devolved Authority Governments as required by the Statutory Guidance, when the Annual Report is published.
NHS England’s Assessment
NHS England considers that it has effectively discharged its relevant data functions during the course of 2023/24 and that in doing so it has had regard to the Statutory Guidance and has made good progress in meeting most of the requirements of that Guidance and it is effectively protecting patient confidential data.
Where elements of the Guidance are not currently being fully met or where improvements have been identified as outlined above, NHS England is satisfied that there are plans in place to address these in business plans, teamwork plans and as part of corporate risk management and governance frameworks.
Business critical models
We operate a register of business-critical models through which we audit quality assurance, overseen by a committee of experienced analysts. This register works on a rolling basis, supporting a continuous improvement approach to our system of quality assurance. To date all relevant NHS England models in the register have passed.
Service auditor reporting and third-party assurances
NHS England relies on a number of third-party providers (such as NHS SBS, NHS BSA and Capita) to provide a range of transactional processing services ranging from finance to data processing. Our requirements for the assurance provided by these organisations are reviewed every year. Appropriate formal assurances are obtained to supplement routine customer/supplier performance oversight arrangements. During 2023/24, service auditor reports were specifically commissioned to provide assurance over the operation of our control environment and we are working, where appropriate, with our suppliers to implement International Standard on Assurance Engagements (ISAE) 3402 or similar standards to make sure that the relevant internal controls and control procedures operated by our service organisations have operated effectively. Service providers are requested to address any control weaknesses identified during the ISAE 3402 reporting process within an appropriate timescale. The service auditor reports commissioned for 2023/24 have been reviewed and where necessary action plans are being agreed to address any control issues identified.
Commissioning support units
Four NHS CSUs operate across England, providing essential support to many organisations including ICBs, trusts, NHS England, and local authorities. With a workforce of 6,500 people and an income of around £500 million, CSUs deliver a range of support services that have been independently assessed to ensure the NHS receives the benefits derived from working at scale.
As an integral part of the NHS, CSUs operate in accordance with good governance principles. Each CSU is led by a managing director who is accountable to NHS England for their CSU’s performance and delivery.
Supply Chain Coordination Limited
In addition to controls set out in the company’s Articles of Association, NHS England appoints directors who sit on the Board of SCCL and holds quarterly accountability meetings to review performance against KPIs and financial targets, both of which are agreed by the NHS England board annually. Additionally, NHS England is a member of SCCL’s ARAC as shareholder director.
The NAO performed a value for money review of NHS Supply Chain during 2023/24 which identified some recommended areas of focus to enable the NHS to achieve greater efficiencies in procurement, through oversight of and support to NHS Supply Chain, including in the development of NHS Supply Chain’s modernisation programme. The recommendations centred on collection and use of data to highlight opportunities and drive use of NHS Supply Chain, as well as ensuring that savings are transparently reported.
Control issues
Managing third-party contracts
Following NHS England’s merger with NHS Digital and Health Education England, work has been undertaken to align the approach to third-party contract management, based on Government Commercial Function guidance and methodologies.
Contracts have been transferred from legacy organisations, and NHS England’s central commercial team now has overall responsibility for 2,293 contracts worth £6.1 billion (total current value).
All members of the central Contract Management team have government commercial function contract management accreditation. In line with the government’s transparency agenda, we publish quarterly KPI data for our gold/strategic contracts.
Primary care support England performance management
Primary care support services are administration and payment services which support the effective running of primary care. The services are delivered by Capita Business Services Ltd, with the support of three CSUs.
The services:
- pay more than £10 billion each year to primary care providers for NHS services
- invite more than 4.5 million women each year for NHS cervical screening
- process registrations for more than six million patients joining or changing GP
- move 5.8 million patient medical records each year between GPs and store over 15 million records of deceased and unregistered patients on behalf of NHS England
Areas of focus to improve control during 2023/24 include: improving the administration service for GP pensions; responding to an increased volume of activity in the pharmacy market administration service; and assuring the patient registration service following two reported service incidents which may have resulted in the incorrect processing of patient registration transactions or changes. This was reported to the ICO. The investigation of the incidents has not yet concluded but no harm to patients has been identified. NHS England had to ensure that the services were delivered to an appropriate standard and that money paid to primary care providers through these services had been properly controlled. The services were assured throughout 2023/24 by regularly monitoring performance and quality indicators, targeted auditing, and a year-end assessment against International Audit Standard ISAE3402.
NHS England had to ensure that effective future arrangements will remain in place for these services and that they can be safely transitioned at the end of the current contracts with third party providers. The programme to determine the future delivery of primary care support services continued through 2023/24.
Overpayments to medical practitioners
If a medical practitioner is suspended, they may be entitled to receive payments under the statutory regulations if the qualifying criteria is met. During the reporting period, NHS England has made changes to the way that these payments are administered to improve national oversight and to reduce variation in the interpretation of the statutory regulations.
Following review, NHS England has identified one case where the circumstances of the practitioner had changed in November 2023 and the practitioner was no longer eligible but continued to receive payments. This resulted in overpayments equating to £32,662. These payments ceased in June 2024. Any other overpayments relating to the 2023/24 reporting period have already been disclosed in the 2022/23 Annual Report and Accounts, as they were identified prior to the publication of that report.
Overpayments to suspended practitioners is an issue that was first identified in 2021/22. Last year, overpayments equating to £1.3 million were identified, as noted in the losses and special payment disclosures to the 2022/23 annual report and accounts. Recoveries are being sought subject to legal advice.
From April 2024, all payments to suspended practitioners are made from the national team following a standardised approach to applying the guidance and improved monthly assurance on changes in circumstances. A full review has been completed of all cases which identified the single case specified above. This is an improvement on previous years where overpayments have been made to several individuals and of much higher values. The additional national oversight has improved the process for making these payments going forwards.
Review of economy, efficiency and effective use of resources
Allocations
NHS England has responsibility for allocating the NHS funding agreed with DHSC as part of our mandate. Please see the chief financial officer’s report, for information on allocations.
Financial performance monitoring
ICBs and ICSs were in place throughout the 2023/24 financial year.
The financial position across the commissioning system was reported monthly using the Integrated Single Financial Environment (ISFE) system and through provision of supporting information. These collections included key elements of provider reporting which facilitated the focus on overall system reporting. Alongside this, NHS providers continued to report their full data using the Provider Financial Monitoring System. This reporting has enabled a detailed monthly review by regional and national finance leadership teams and NHS England’s Chief Financial Officer.
Individual ICB, system, direct commissioning and provider financial performance is monitored against KPIs including balance sheet indicators and performance against efficiency plans, in addition to the reported forecast and year-to-date position.
The financial position of commissioners is consolidated and reported in the overall NHS England accounts. NHS England is not the parent entity of NHS trusts and NHS foundation trusts; the financial position of providers is reported separately in the consolidated NHS provider accounts.
Cabinet Office efficiency controls
As part of the Government’s control of expenditure, we are subject to specified expenditure controls. These controls cover a range of expenditure categories and require proposed expenditure to be approved to secure best value for money and ensure efficiency is being maximised. For expenditure above certain thresholds in specified categories (including professional services and consultancy), onward approval is also sought from DHSC and for some cases this also requires approval from the Minister, Cabinet Office and/or HM Treasury.
Counter fraud
NHS England has a dedicated counter-fraud team which ensures that appropriate counter-fraud arrangements are in place. This includes proactive activities to prevent and detect fraud, as well as reactive investigation of allegations of fraud related to our functions.
The Director of Financial Control has day-to-day operational responsibility for the function, and the Chief Financial Officer provides executive support and direction.
We continued to work collaboratively with key partners in both proactive and reactive areas, including the Public Sector Fraud Authority, DHSC, NHS Counter Fraud Authority, NHS BSA and law enforcement agencies. During 2023/24 NHS England was assessed by the Health Peer Review Group (HPRG)* as being fully compliant with the Government Counter Fraud Function Standard.
*HPRG was comprised of DHSC, NHS England, NHSBSA and NHS Counter Fraud Authority. It received and reviewed evidence provided by DHSC ALBs against the Government Counter Fraud Function Standard before the introduction of the Continuous Improvement Assessment Framework criteria. The assessment by the HPRG to award full compliance to NHSE was conducted in June 2023 when the HPRG was still active. Following introduction of the Public Sector Fraud Authority Continuous Improvement Assessment Framework, the DHSC Counter Fraud Board agreed to disband the HPRG on 18 April 2024.
NHS England public Inquiries
The Thirlwall Inquiry was announced as a statutory inquiry on 4 September 2023 looking into events at the Countess of Chester Hospital, and the implications of those events following the conviction of Lucy Letby in August 2023. NHS England subsequently appointed an internal response team as well as external legal support.
In 2023/24, NHS England responded to the COVID-19 Inquiry as a Core Participant for Module 1 (Pandemic Preparedness) and Module 2 (Government Decision Making).
NHS England was not asked to provide a witness for oral evidence for Module 1. Our former Chief Executive Officer, Lord Stevens, appeared as witness for Module 2 in November 2023. We are preparing for Module 3 hearings (Impact on Healthcare Systems), Autumn 2024 and we will respond to other modules on Vaccines and Therapeutics, Procurement, Social Care and Test and Trace in 2025.
The Infected Blood Inquiry (IBI) was an independent public statutory Inquiry established to examine the circumstances in which men, women and children treated by the NHS in the UK were given infected blood and blood products, in particular since 1970. On 14 September 2021 NHS England was designated a Core Participant in the inquiry and, in 2023/24 submitted written and oral statements on matters including psychological support services, data collection, digitisation of records, the Patient Safety Incident Response Framework and the Hepatitis C elimination programme. The IBI published its second interim report in April 2023, which primarily focused on recommendations for compensation to those infected and affected. The Government committed to funding this service which is being commissioned by NHS England and is expected to be rolled out in 2024/25.
Ministerial directions
The Secretary of State gave 11 directions to NHS England under section 254 of the Health and Social Care Act 2012 to establish and operate information systems i.e. systems for the collection or analysis of information relating to health or social care. In addition, 23 direction specifications, which connected with existing directions, were also issued. The Secretary of state issued the routine financial directions, making provision for NHS England’s budgets and financial limits.
Head of Internal Audit opinion
Internal audit’s opinion is based on a programme of work designed to address the specific assurance requirements of the NHS England Board and Accounting Officer. Results of internal audit work, including remedial actions agreed with management, have been regularly reported to management and ARAC.
In the context of the overall environment for NHS England for 2023/24, the opinion of internal audit is that the design of the governance and risk management framework at the year-end is effective and provides the foundation of a framework to take the organisation forward during 2024/25.
The organisation has been under significant operational pressure and subject to large scale change because of several factors including delegation of functions to ICBs and the internal reorganisation following the mergers with NHS Digital and Health Education England. Internal audit has reported that the framework for internal control was not being consistently complied with during the year due primarily to operational pressures, changes in roles and responsibilities due to the reorganisation, and in some cases a lack of consistent, integrated processes across the new NHS England to identify and address non-compliance.
Internal audit therefore concluded that limited assurance can be provided over the effectiveness and efficiency of the internal control framework. Internal Audit specifically drew attention to Leavers and Dental Contract Management in their conclusion. In the context of leavers, processes had not been harmonised across legacy organisations and were not consistently completed by line managers and for Dental Contract Management, at the time of the review, there was not a coordinated approach to national and regional oversight of delegated dental services, to ensure compliance with standards. Management has undertaken focused pieces of work to address the issues identified in these reports, which has resulted in the majority of recommendations having been implemented at the time of writing.
Actions have been agreed to address the issues identified by internal audit. Implementing actions in a timely manner has continued to be challenging in the context of the ongoing organisational change programme and operational pressures, and management continues to focus on this. Management is continuing to design and implement measures to improve compliance, including training for line managers on core roles and responsibilities, harmonising and strengthening policies, enhanced corporate reporting, and new compliance checking processes.
Some of the weaknesses in internal controls for core processes were assessed as being fundamental to the system of controls. Management actions have been agreed to address these observations, not all of which have been completed by year end given their nature. Where possible, interim solutions have been put in place.
There remains significant reliance on third party providers of core services, such as payroll processing, and there remains a requirement to further embed the contract management framework to obtain assurance over the delivery of services.
Remuneration and staff report
Our people
Our NHS People Plan ambitions and values drive our workforce strategy, which aims for more staff working flexibly in a compassionate and inclusive culture. Alongside our People Plan, our NHS People Promise sets out our pledge to one another and describes how we want to improve the experience of working in the NHS for everyone.
NHS Digital and Health Education England merger
On 22 November 2021, the Secretary of State for Health and Social Care set out his intention to merge Health Education England with NHS England, (putting recruitment, training and retention of NHS staff at the heart of the NHS in England). In addition, the recommendations of the Laura Wade-Gery Review were accepted, including to merge NHS Digital and NHSX into NHS England, joining up the approach to digital transformation in a single organisation.
The creation of ICBs in July 2022; the merger of NHS England with NHS Digital from January 2023 and Health Education England from April 2023; and the need to re-size our organisation post COVID-19 pandemic, meant we have been able to create a new NHS England. At the same time, we have created a simpler, smaller, organisation that leads the NHS more effectively, with equality, diversity and inclusion at the heart of all we do.
As the new NHS England (this was merger of NHS England, Trust Development Authority and Monitor etc.), we have brought together five arms-length bodies into one new organisation, reducing our combined workforce by over 36% and delivering significant savings, money that can be reinvested into frontline care. We are now embedding our new Operating Framework, transforming our ways of working and developing a new aligned organisational culture.
Staff numbers
On 31 March 2024, NHS England directly employed 16,074 staff (14,578 WTE). Of these, 14,774 were permanently employed, and 1,300 were employed on payroll on fixed term contracts of employment. A further 1,282 people were engaged in an off-payroll capacity, including agency staff and secondees. The chart on the following section shows the headcount by pay band on 31 March 2024. Detail on staff numbers and costs for NHS England and the consolidated group, including CSUs, are presented in section: Employee benefits and staff numbers (subject to audit).
All staff by grade

A voluntary redundancy scheme offered to all eligible employees for a limited period has had an impact on staff numbers. Exit packages agreed over the year are detailed in the exit packages section.
The new NHS England programme was set up to manage the merger of Health Education England with NHS England, NHS Digital and NHSX, and the decommissioning of Public Health England, following the decisions of the then Secretary of State for Health and Social Care. As a result of the programme, we have created a more streamlined and smaller organisation to lead the NHS more effectively and to improve services for patients and communities and the working lives of NHS staff, while making best use of public money. Our organisation will be 36% smaller than the three combined legacy organisations, once the final transfers of staff and functions out of NHS England have taken place.
Staff turnover
Turnover increased in 2023/24 compared to 2022/23. Both the headcount and the number of people leaving the organisation increased. This increase is due to the voluntary redundancy scheme that opened on 18 January 2023 for a limited period.
Staff turnover (%)
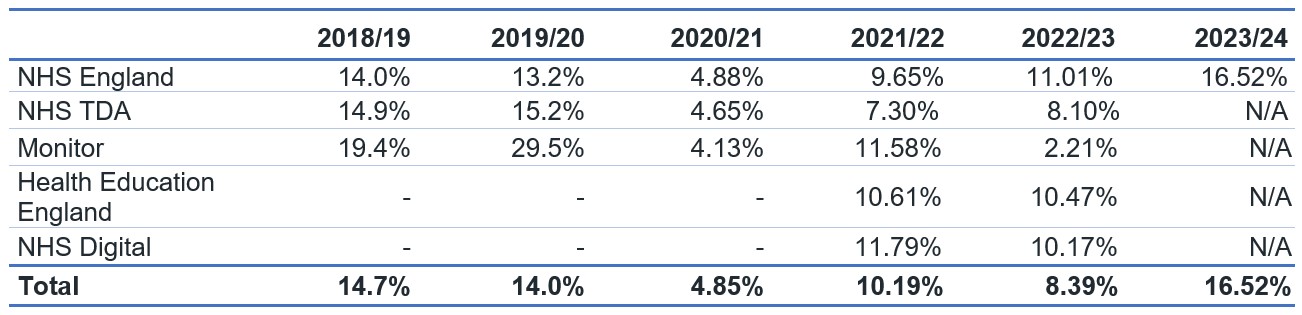
Employment policies
Our priorities for 2023/24 included:
- identifying the key employment policies that applied to staff transferring into NHS England from NHS Digital and Health Education England
- in partnership with our trade unions, forming a new Policy Sub-group encompassing members from legacy NHS England, NHS Digital and Health Education England
- developing a policy work schedule, which includes the harmonisation of the Attendance Management and Pay Protection policies, a review of all other key employment policies to reflect the culture of the new NHS England and the development of two new policies aligned to one of our national programmes.
Partnership working
NHS England fully recognises the vital contribution of trade unions in representing the interests of colleagues and our organisation. We work closely in partnership with our recognised trade unions on a number of important employment matters. Partnership work includes consulting on organisational change, as a legal requirement, as well as developing and refining our policies and consulting on a wide range of issues affecting people and the organisation.
To facilitate partnership working, NHS England has a National Partnership Forum that meets every quarter. This forum provides strategic direction for other important sub-groups that focus on specific issues. Sub-groups include policy, organisational change, equality and diversity and the Local Negotiating Committee. In addition, we hold regional and corporate engagement forums to address any local issues, which can be escalated to the national partnership structure(s) if necessary.
Over the last year we have, in partnership, reviewed our staff side membership following the merger with NHS Digital and Health Education England to transition representatives from the transferring organisations. A key deliverable this year was the development in partnership of an agreed Change Implementation Framework to underpin the Creating the new NHS England Programme.
Trade union facility time disclosures
We fulfilled our obligations under the Trade Union (Facility Time Publication Requirements) Regulations 2017 for 2023/24 by reporting the information to form part of the Government’s public sector trade union facility time data, published on the gov.uk website in August each year.
Trade union representatives – the total number of employees who were trade union representatives during the relevant period:
| Number of employees who were relevant union officials during the relevant period | WTE employee number |
|---|---|
| 71 | 62.76 |
Percentage of time spent on facility time (duties and activities):
| Percentage of time | Number of employees |
|---|---|
| 0% | 30 |
| 1-50% | 40 |
| 51-99% | 1 |
| 100% | 0 |
Percentage of pay bill spent on facility time:
| Description | Figures |
|---|---|
| Provide the total cost of facility time | £89,974.10 |
| Provide the total pay bill | £1,336,845,732.20 |
| Provide the percentage of the total pay bill spent on facility time, calculated as: (total cost of facility time – total pay bill) x 100 | 0.01% |
Time spent on paid trade union activities as a percentage of total paid facility time hours:
| Description | Figures |
|---|---|
| Hours spent on paid facility time | 3267 |
| Hours spent on paid trade union activities | 183.5 |
| Percentage of total paid facility time hours spent on paid trade union activities | 5.62% |
Equality, diversity, and inclusion
Workforce Disability Equality Standard
In partnership with our disability staff networks, we have developed a new Workforce Disability Equality Standard action plan in co-production with staff disability networks and Human Resource business partners. The plan incorporates the legacy NHS England, Health Education England and NHS Digital delivery plans and Disability Confident employer deliverables. The organisation-wide plan includes 67 individual actions delivering 31 outcomes. Most of the proposed actions are focused on communication, recruitment, selection and retention.
The graphs below show the reporting of all staff and senior manager disability or long-term conditions in Electronic Staff Record (ESR).
Declared disabilities or long-term conditions
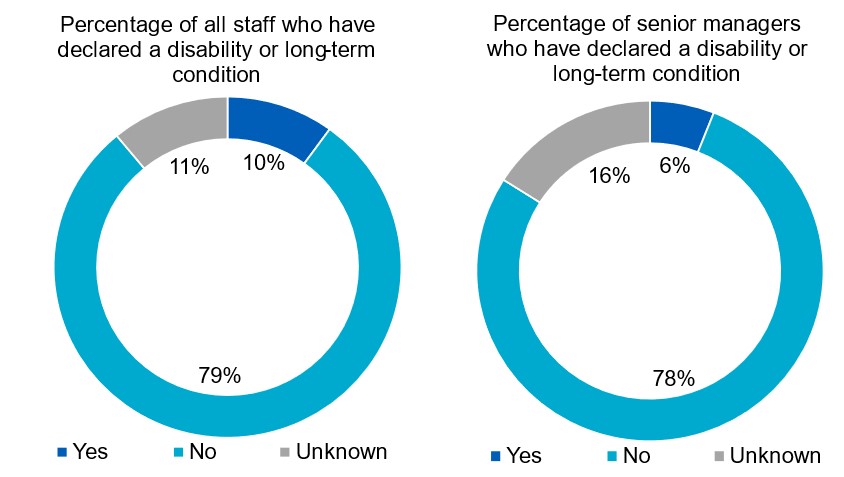
Sexual orientation of staff and senior managers
The percentage of staff who disclose their identity as lesbian, gay and bisexual (LGB) is 4.9% as of March 2024. The breakdown of sexual orientation declaration is detailed below, including an overview of senior managers who have declared as LGB in ESR (3.9%).
Staff and managers by sexual orientation
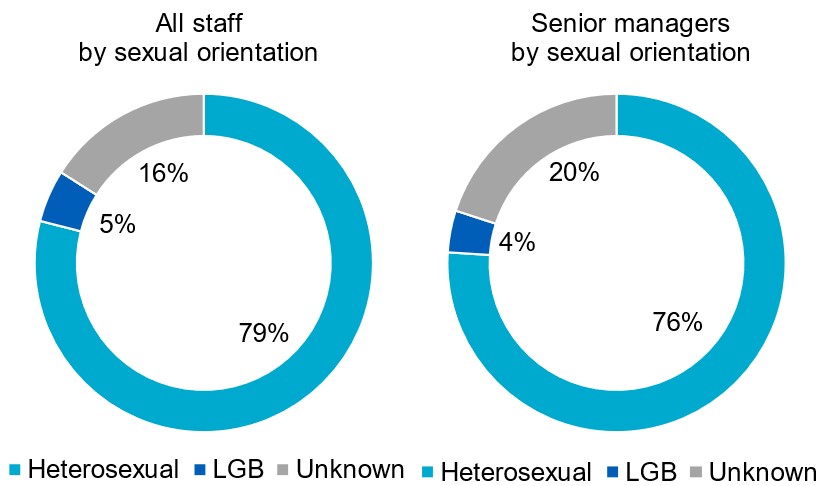
Gender of all staff and senior managers
The female gender profile of the total NHS England on payroll workforce decreased by 0.6% between 31 March 2023 and 31 March 2024. There has been no change in the number of female senior managers which remained at 54.7%. The gender diversity of NHS England Board members is set out in the board diversity section. The graphs below highlight gender reporting in ESR:
All staff and senior managers by gender
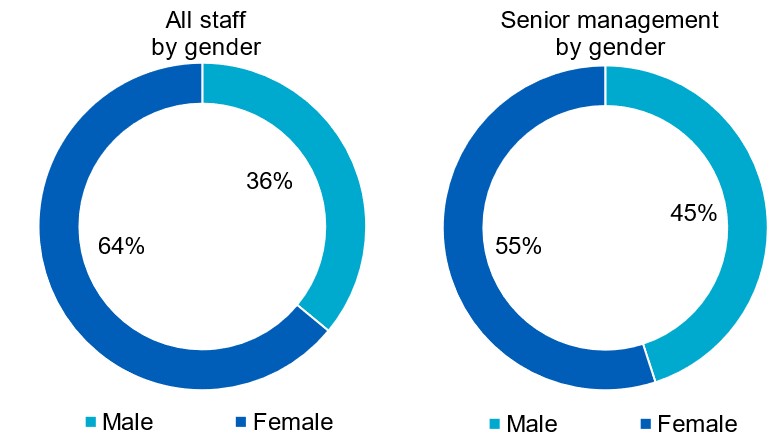
Gender pay gap
All organisations with more than 250 staff are required to publish a gender pay report. We have produced a combined gender pay gap report as at 31 March 2023 for the new NHS England which incorporates the three legacy organisations.
The gender pay gap trend for the new NHS England is positive, with improvements made from the previous year compared to legacy NHS England, NHS Digital and Health Education England. The mean gender pay gap was 11.84% in March 2023, representing a reduction in the gap of almost 2%. The median gender pay gap was 8.87% in March 2023, a more than 2% drop compared to all three legacy organisations.
| Year | Mean gender pay gap |
|---|---|
| 2023 | 11.8% |
| 2022 | 14.7% |
| 2021 | 16.2% |
| 2020 | 16.7% |
| 2019 | 18.3% |
| 2018 | 19.5% |
Pay quartiles by gender in NHS England
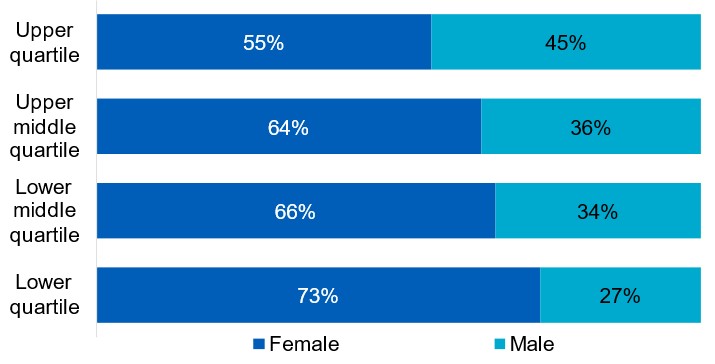
In the new NHS England 55% of women are in the highest paid jobs compared to 45% of men. In contrast, 73% of women are in the lowest paid jobs compared to 27% men.
The pay gap is a result of having a smaller proportion of men in lower pay bands. Although the mean salaries for women across pay bands 2 to 7 are higher, their mean earnings are considerably less than men across bands 8b and above. Similarly, we have the highest proportion of women in pay bands 5 to 8a compared to men, who we have a higher proportion in bands 8b and above.
Ethnicity of all staff and senior managers
Improving our diversity levels at senior pay bands
We are developing a new approach to setting goals to improve representation levels in the new NHS England.
While blanket organisation-wide targets such as the 19% BME aspirational target has driven overall progress in improving representation levels, we want to build on this further and take a more stratified approach.
Our new approach will benchmark against local working population levels and current workforce levels, with an additional focus on structural barriers or ’glass ceilings’ in the workforce, for example at pay bands 8c and above.
Figures below show the overall percentage of BME staff and the change over the last three years:
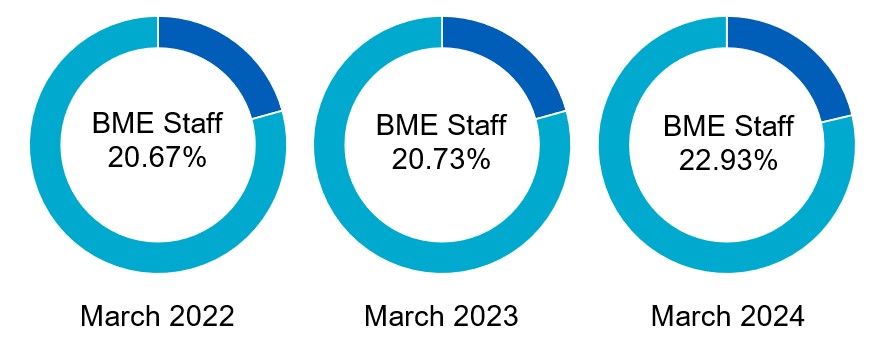
The proportion of people employed by NHS England who consider themselves to be from a BME heritage increased by 2.2 percentage points between 31 March 2023 and 31 March 2024. The proportion of senior managers who identify as black or minority ethnic has increased from 16.4% in 2022/23 to 22.7% in 2023/24.
The graphs below show ethnicity for all staff and senior managers, as reported in ESR.
All staff and senior managers by ethnicity
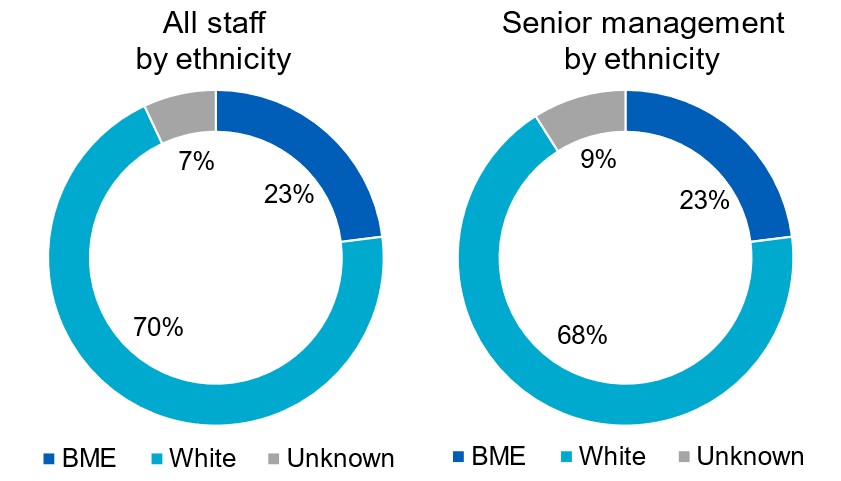
Staff engagement and feedback
Ensuring that we regularly seek views and feedback from employees is a key part of our organisational development and culture work. Employee engagement took place through our pulse check survey and the NHS England Staff Survey.
NHS England staff survey
In January 2024 NHS England launched its first annual staff survey as a newly merged, single organisation. This year’s results will provide a baseline for the organisation and identify key areas of improvement to focus on over the coming year.
The survey achieved a 58% response rate equivalent to 9,646 completed surveys over a reduced survey window of four weeks.
As in past years, local action plans will be developed within each national directorate and region to have targeted focus across the organisation.
Sickness absence
Sickness absence for the period 1 April 2023 to 31 March 2024 was as follows:
| WTE days available | WTE days lost to sickness absence | Sickness absence rate | |
| NHS England | 5,663,098 | 140,459 | 2.48% |
Employee benefits and staff numbers (subject to audit)
Detail on staff numbers and costs for NHS England and the consolidated group, including CSUs, are presented in the following tables:
Average number of people employed
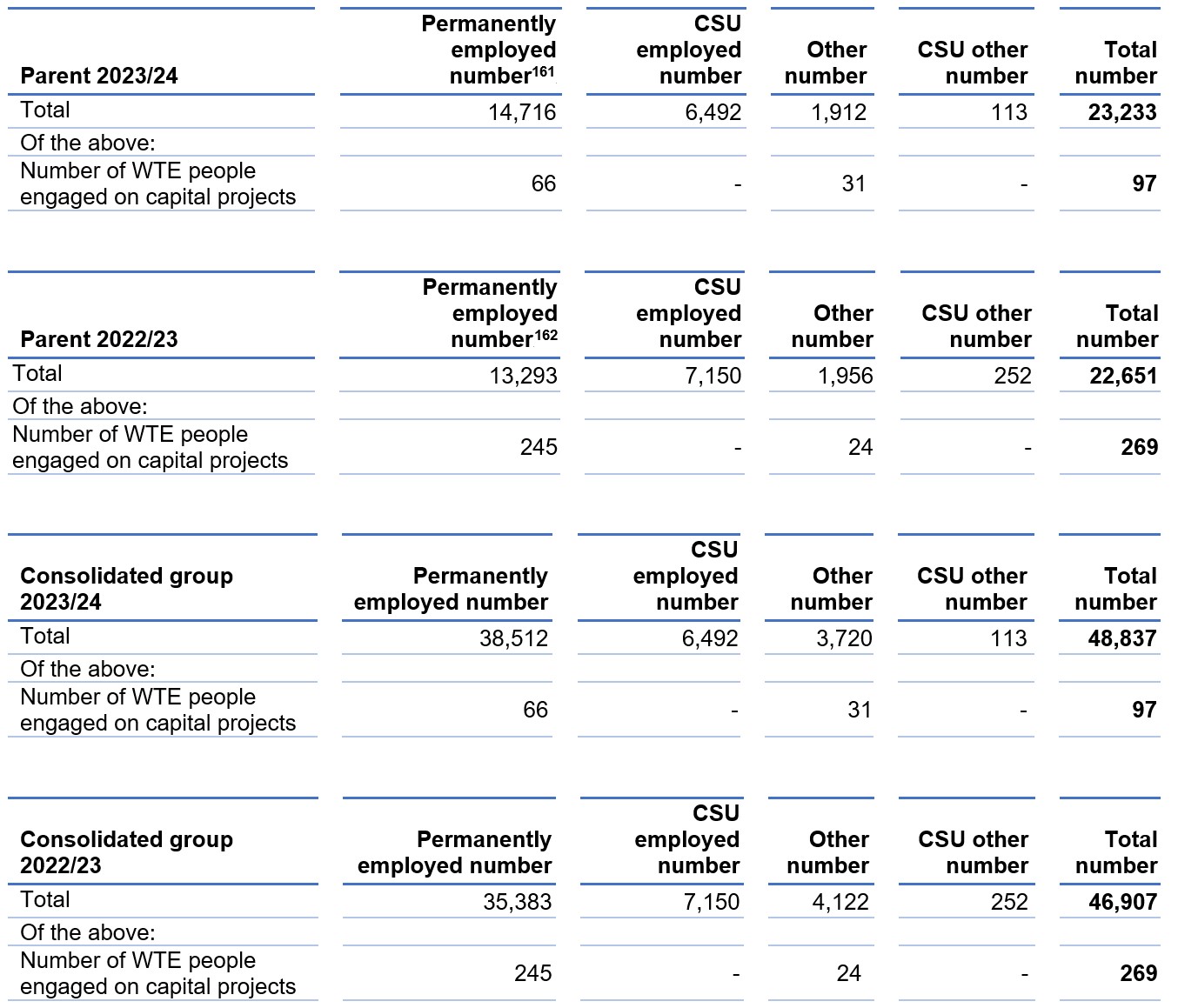
[161] The most significant increase in staffing is including the transfer of staff Health Education England on 1 April 2023.
[162] The most significant increase in staffing is including the transfer of staff from Monitor and Trust Development Authority at 1st July 2022 plus 2 months of NHS digital from 1 February 2023.
Employee benefits
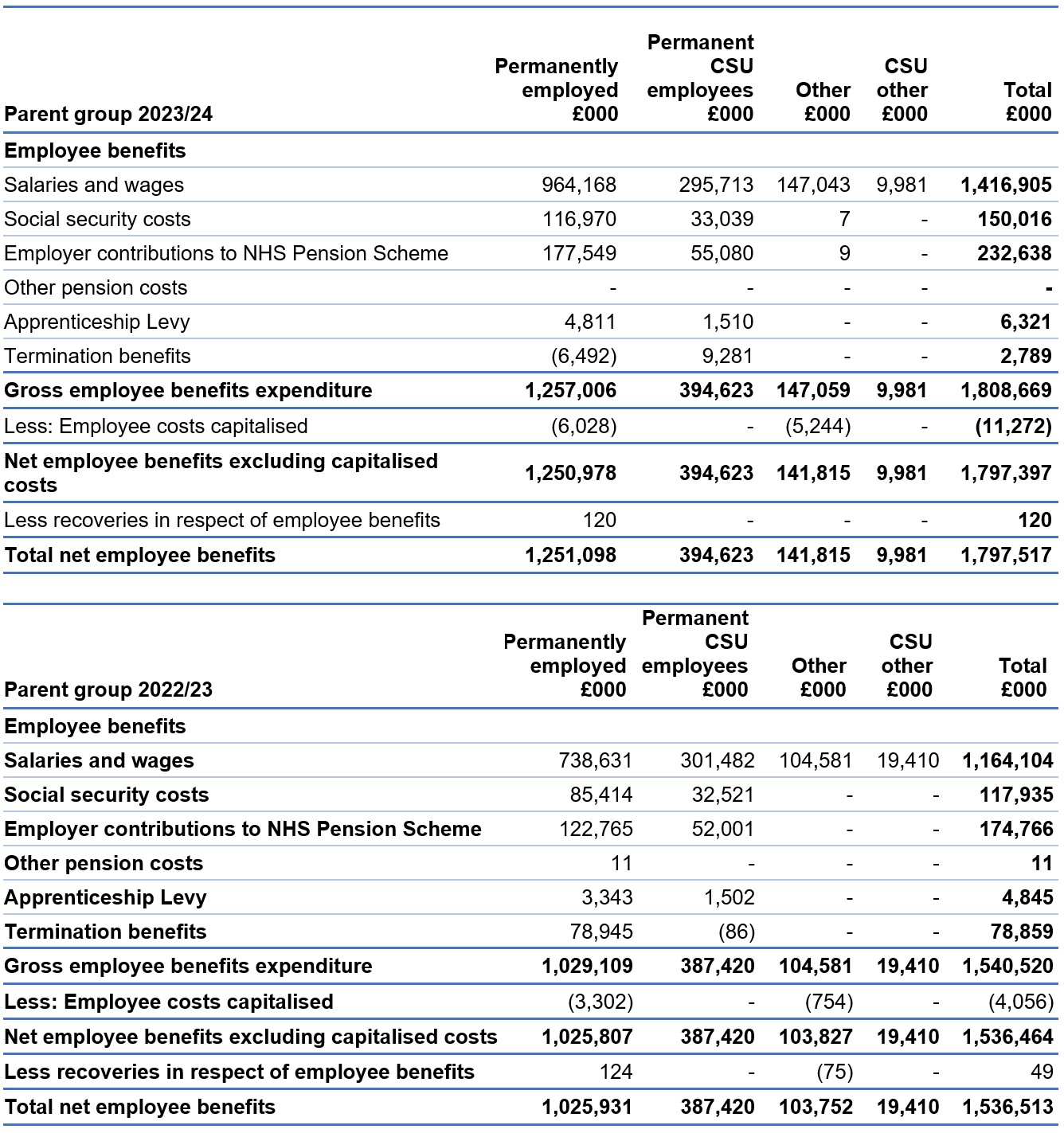
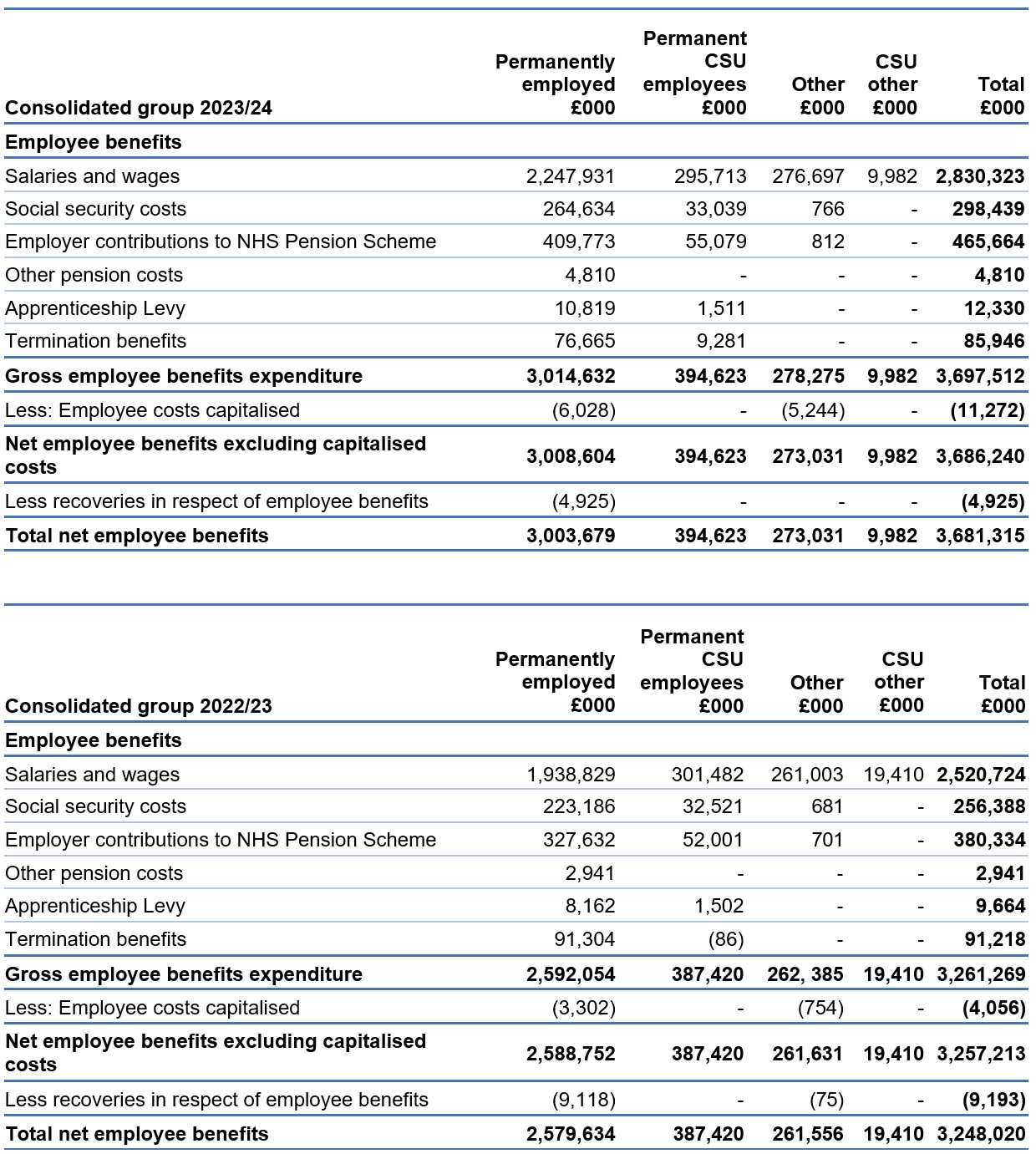
CSUs are part of NHS England and provide services to ICBs.
The employment contracts or secondment agreements of almost all these staff are held for NHS England on a hosted basis by the NHS BSA.
Exit packages, severance payments and off-payroll engagements
Expenditure on consultancy and contingent labour
Expenditure on consultancy is detailed in the Annual Accounts under Note 4: Operating expenses. NHS England and CSUs procured consultancy services worth £17.1 million during the financial year, a decrease of £144k since the previous year (2022/23: £17.3 million).
Across the group, there was a total spend of £57.5 million on consultancy services during the period, against £51.1 million the previous year, reflecting the increased size of the organisation following merger with Health Education England in April 2023.
Expenditure on contingent labour, including agency staff and secondees, is given in the e#employee benefits table, under the ‘other’ column.
Net expenditure for NHS England and CSUs in this area was £157 million in 2023/24, against £124 million in 2022/23. Across the group, there was a total spend of £288.2 million on contingent labour during the year, against £281.8 million the previous year. The increase in group consultancy relates to an increased level of programme in ICBs.
Further detail on efficiency controls, and steps we have taken to improve procurement practices and compliance within NHS England during the year, can be found in our governance statement.
| Contingent labour | 2023/24 £000 | 2022/23 £000 | (Increase) / Decrease £000 |
| Parent inc CSU other | 157,040 | 123,991 | (33,049) |
| Group inc Parent and CSU other | 288,257 | 281,795 | (6,462) |
| Consultancy | 2023/24 £000 | 2022/23 £000 | (Increase) / Decrease £000 |
| Parent consultancy | 17,146 | 17,290 | 144 |
| Group consultancy | 56,457 | 51,147 | (5,310) |
Off-payroll engagements
NHS England is committed to employing a capable, talented, and diverse on-payroll workforce to support the delivery of its business. It is recognised that in some specific circumstances the use of off payroll workers (OPWs), working alongside our on-payroll workforce, can be helpful. For some of our time-limited programmes, short-term contracts are appropriate. The following tables identify OPWs engaged by NHS England at March 2024. OPWs engaged by ICBs are reported in ICB annual reports and published on their websites.
Off-payroll engagements longer than 6 months
Off-payroll engagements on 31 March 2024, covering those earning more than £245 (the £245 threshold is set to approximate the minimum point of the pay scale for a Senior Civil Servant) per day and staying longer than 6 months are as follows:
| Off-payroll engagements longer than 6 months | NHS England (number) | CSUs (number) | Total (number) |
| Number of existing engagements as of 31 March 2024 | 324 | 7 | 331 |
| Of which, the number that have existed: | |||
| for less than 1 year at the time of reporting | 45 | 7 | 52 |
| for between 1 and 2 years at the time of reporting | 47 | 0 | 47 |
| for between 2 and 3 years at the time of reporting | 70 | 0 | 70 |
| for between 3 and 4 years at the time of reporting | 71 | 0 | 71 |
| for 4 or more years at the time of reporting | 91 | 0 | 91 |
Most OPWs who provide services to NHS England are clinical medical staff. All existing off-payroll engagements, outlined above, were subject to a risk-based assessment as to whether assurance was required that the individual was paying the right amount of tax and, where necessary, assurance has been sought.
New off-payroll engagements
New off-payroll engagements or those that reached 6 months in duration, between 1 April 2023 and 31 March 2024, for more than £245 (the £245 threshold is set to approximate the minimum point of the pay scale for a Senior Civil Servant) per day and that last longer than 6 months are as follows:
| New off-payroll engagements | NHS England (number) | CSUs (number) | Total (number) |
| Number of OPWs engaged during the year ended 31 March 2024 | 463 | 185 | 648 |
| Of which: | |||
| Number not subject to off-payroll legislation* | 0 | 0 | 0 |
| Number subject to off-payroll legislation and determined as in-scope of IR35* | 462 | 185 | 647 |
| Number subject to off-payroll legislation and determined as out of scope of IR35* | 1 | 0 | 1 |
| Number of engagements reassessed for compliance or assurance purposes during the year | 0 | 0 | 0 |
| Of which: | |||
| Number of engagements that saw a change to IR35 status following review | 0 | 0 | 0 |
*A worker that provides their services through their own limited company or another type of intermediary to the client will be subject to off-payroll legislation and the Department must undertake an assessment to determine whether that worker is in-scope of Intermediaries legislation (IR35) or out-of-scope for tax purposes.
Off-payroll board member/senior official engagement
Off-payroll engagements of Board members and/or senior officials with significant financial responsibility between 1 April 2023 and 31 March 2024 are shown in the table below:
| Off-payroll board member/senior official engagement | NHS England (number) | CSUs (number) | Total (number) |
|---|---|---|---|
| Number of off-payroll engagements of Board members and/or senior officers with significant financial responsibility, during the financial year | 0 | 0 | 0 |
| Total number of individuals on-payroll and off-payroll who have been deemed ‘Board members and/or senior officials with significant financial responsibility’ during the financial year | 330 | 0 | 330 |
Senior officials are defined as those at pay grade ESM 1 and ESM2, shown on the chart.
Details of exit packages agreed over the year are detailed in the following tables. All contractual severance payments were subject to full external oversight by DHSC.
Exit packages agreed during the year (subject to audit)
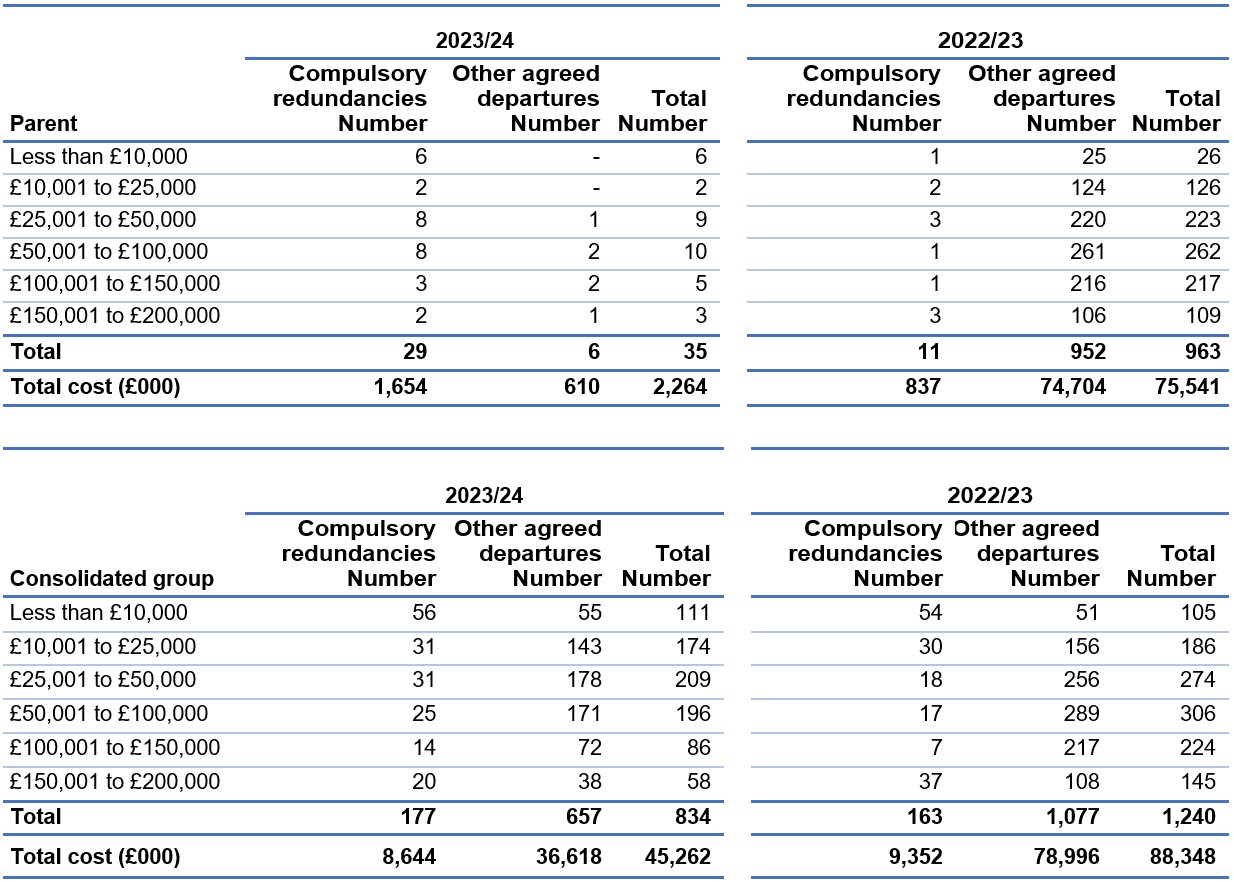
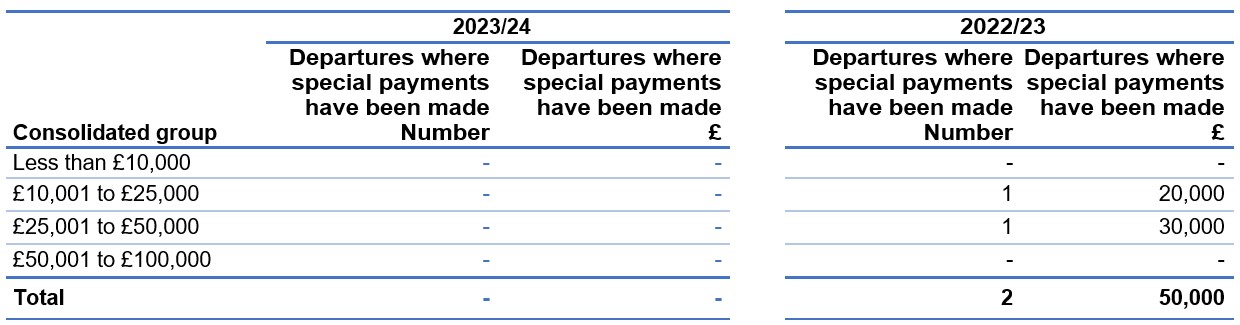
Analysis of other agreed departures (subject to audit)
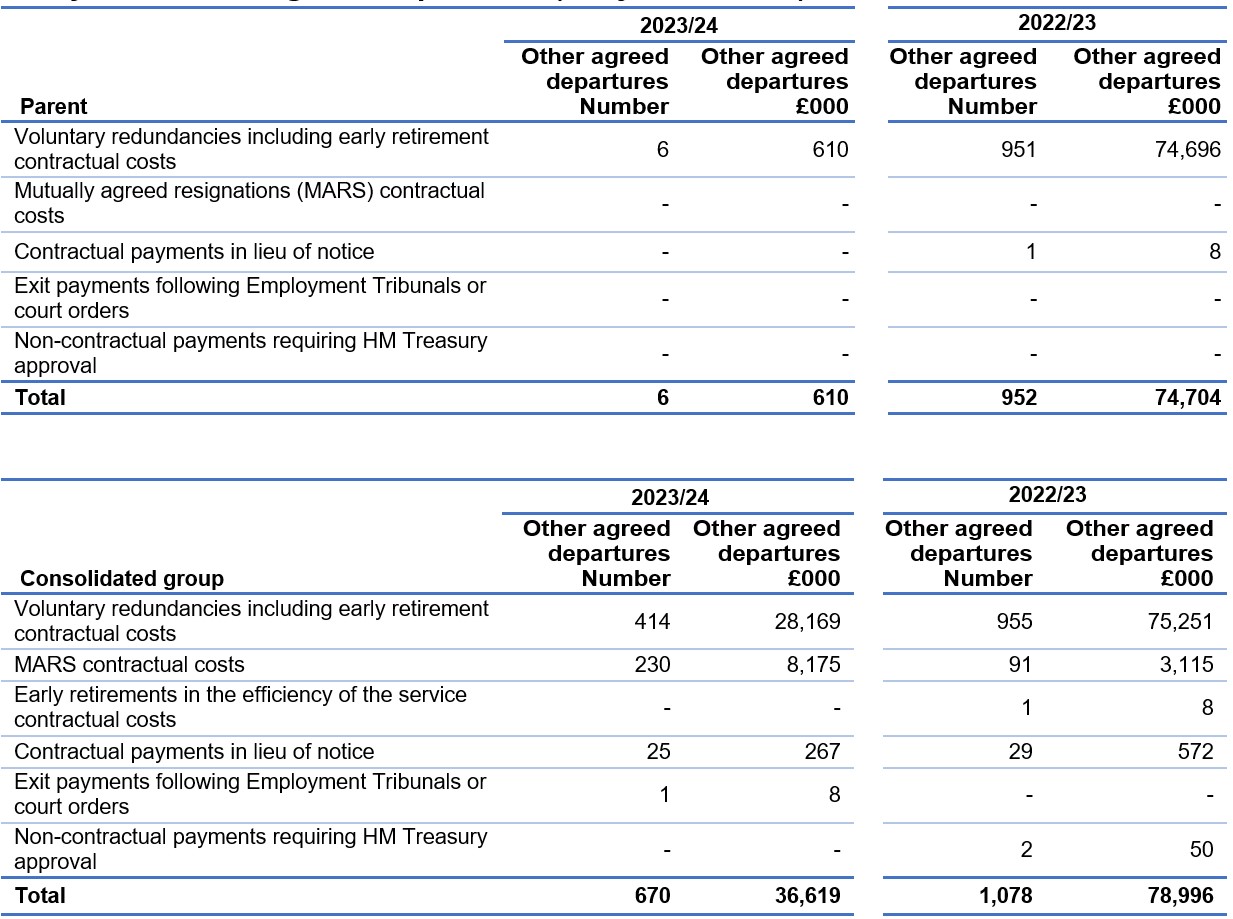
As a single exit package can be made up of several components, each of which will be counted separately in this table, the total number of exit packages will not necessarily match the total number in the table above.
These tables report the number and value of exit packages agreed in the financial year. The expense associated with these departures may have been recognised in part or in full in a previous period.
Redundancy and other departure costs have been paid in accordance with the provisions of NHS England.
Exit costs are accounted for in accordance with relevant accounting standards and at the latest in full in the year of departure.
Where NHS England, ICBs and CCGs have agreed early retirements, the additional costs are met by NHS England or the ICB or the CCG and not by the NHS Pension Scheme and are included in the tables. Ill-health retirement costs are met by the NHS Pension Scheme and are not included in the tables. The Remuneration Report includes the disclosure of exit payments payable to individuals named in that report.
People and Remuneration Committee
Detail on the role and activity of the People and Remuneration Committee is given in our Directors’ Report.
Percentage change in remuneration of highest paid director (subject to audit)
| Percentage change in remuneration of the highest paid director | Salary and allowances | Performance pay and bonuses |
|---|---|---|
| The percentage change from the previous financial year in respect of the highest paid director | 3.88% | 0% |
| The average percentage change from the previous financial year in respect of employees of the entity, taken as a whole | 15.86% | -100% |
The large average percentage increase in salary and allowances from 2022/23 to 2023/24 can be explained by NHS England merging with NHS Digital on 01 February 2023 and Health Education England on 01 April 2023 and the resulting change in organisational staff profile.
The large average percentage decrease in performance pay and bonuses across NHS England from 2022/23 to 2023/24 can be explained by the retrospectively agreed Government’s AfC 2022/23 Non-Consolidated Pay Award that consisted of 2 one-off, non-consolidated awards on top of the 2022/23 consolidated award.
In 2022/23, employees received a non-consolidated award worth 2%, in addition to a one-off NHS backlog bonus worth an additional 4% of the AfC pay bill to recognise the sustained pressure facing the NHS following the COVID-19 pandemic, however these one off non-consolidated awards were not payable in 2023/24.
Pay ratio information (subject to audit)
Reporting bodies are required to disclose the relationship between the total remuneration of the highest-paid director/member in their organisation against the 25th percentile, median and 75th percentile of remuneration of the organisation’s workforce. Total remuneration of the employee at the 25th percentile, median and 75th percentile is further broken down to disclose the salary component.
The banded remuneration of the highest paid director/member in NHS England in the financial year 2023/24 was £265,000 to £270,000 (2022/23: £255,000-£260,000). The relationship to the remuneration of the organisation’s workforce is disclosed in the below table.
| 2023/24 | 25th percentile | Median | 75th percentile |
| Total remuneration (£) | 37,350 | 51,558 | 72,245 |
| Salary component of total remuneration (£) | 37,350 | 50,952 | 70,417 |
| Pay ratio information | 7.16:1 | 5.19:1 | 3.70:1 |
| 2022/23 | |||
| Total remuneration (£) | 37,633 | 50,847 | 69,855 |
| Salary component of total remuneration (£) | 35,572 | 48,526 | 67,064 |
| Pay ratio information | 6.84:1 | 5.06:1 | 3.69:1 |
The pay ratio information for the 2023/24 financial year is consistent with the pay, reward and progression policies for the employees taken as a whole, due to applying all nationally mandated pay awards where applicable and adhering to the relevant pay progression principles.
In 2023/24, no employees received remuneration in excess of the highest-paid director/ member (2022/23: none). Remuneration ranged from £7,883 to £270,000 (2022/23: £7,883 to £260,000).
Total remuneration includes salary, non-consolidated performance-related pay (PRP), benefits-in-kind, but not severance payments. It does not include employer pension contributions and the cash equivalent transfer value (CETV) of pensions.
Policy on remuneration of senior managers
The framework for the remuneration of executive directors is set by DHSC through the ESM pay framework for ALBs.
It is NHS England’s policy to pay salaries that are appropriate to recruit senior managers with the necessary skills, capability and experience for the effective running of a more than £175 billion organisation, while recognising the importance of demonstrating pay restraint at a time of considerable pressure on NHS finances. Recommending appropriate remuneration for executive directors was undertaken by the People and Remuneration Committee and the Nominations Committee. Final decisions are made by the DHSC ALB Remuneration Committee and HM Treasury, where appropriate.
Performance-related pay
The PRP arrangements for national (executive) directors are set out in the ESM pay framework for ALBs. They follow guidance prescribed by DHSC and are in line with HM Treasury requirements. As a local policy decision, NHS England does not currently allocate any funding for PRP non-consolidated bonus payments. In recognition of the current economic climate and the need to provide effective system leadership for the NHS, the decision was taken by the Executive HR Group and the People and Remuneration Committee not to allocate funds for PRP non-consolidated bonus payments for 2023/24.
Secondees are subject to the terms and conditions of their employing organisation.
Policy on senior managers’ contracts
Contracts of employment for senior managers are open-ended and recurrent, unless otherwise specified. Notice periods follow the provisions of the ESM contract of employment, as applied by NHS England, of 6 months’ contractual notice.
Termination payments can only be authorised where they are contractual and, subject to the value involved, may still require further approval from the DHSC Governance and Assurance Committee.
Any proposed non-contractual special severance payment requires formal approval from DHSC and HM Treasury.
Payments for loss of office (subject to audit)
No payments were made to any senior manager to compensate for loss of office in 2023/24.
Payments to past directors (subject to audit)
No payments have been made to past directors and no compensation has been paid on early retirement. This is subject to audit.
Senior managers’ service contracts
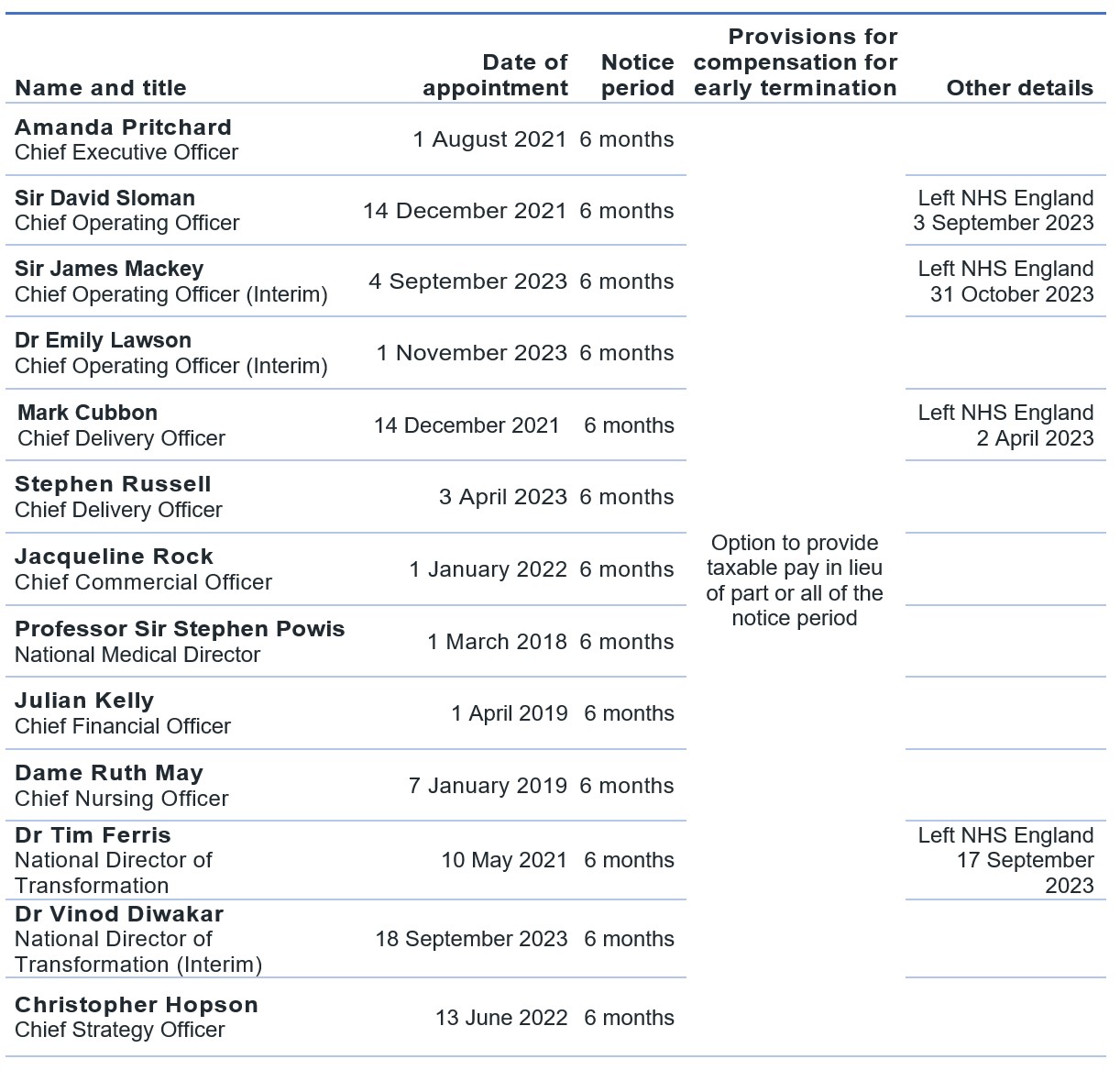
Remuneration (salary, benefits in kind and pensions) 2023/24 (subject to audit)
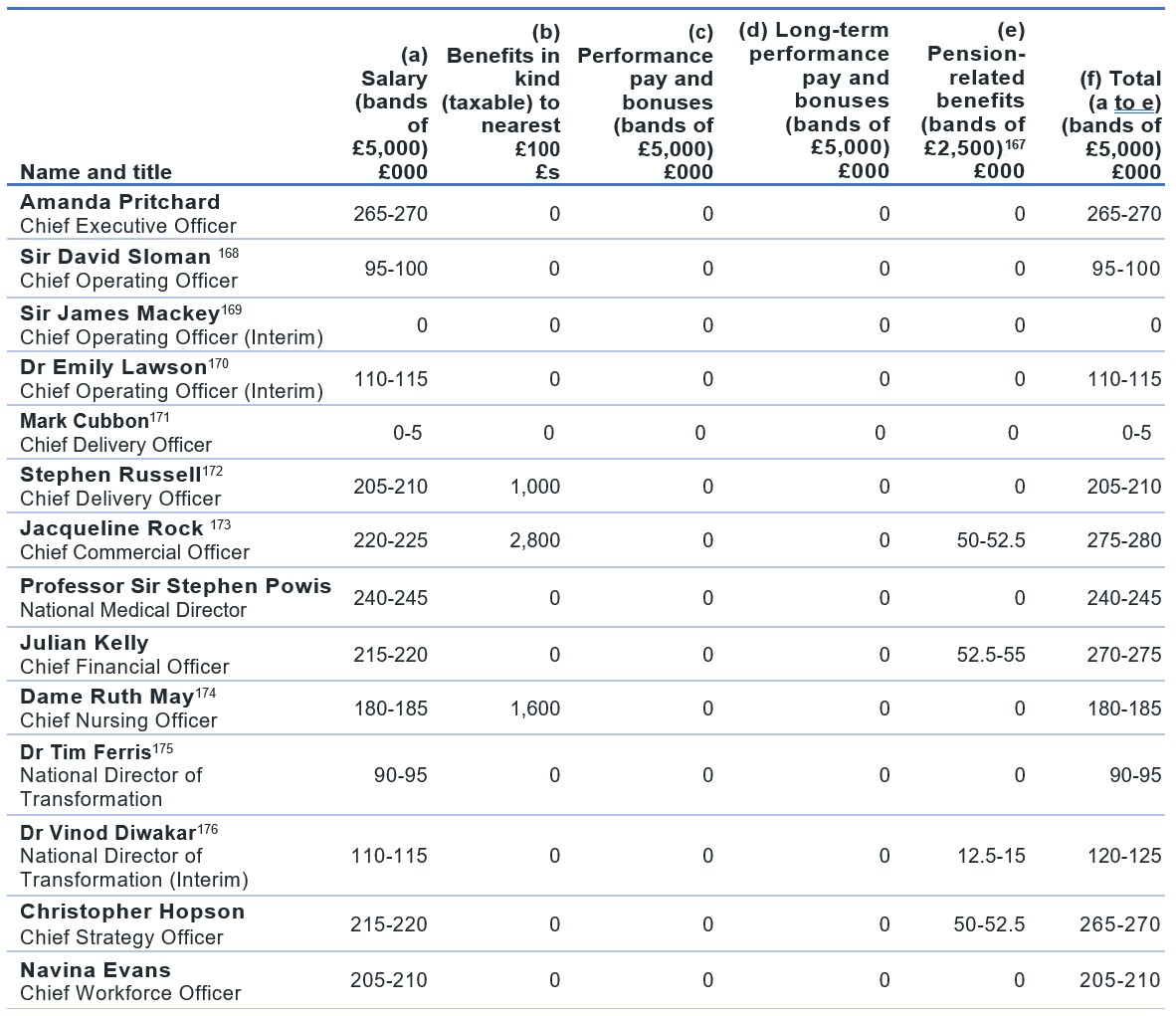
[167] The value of pension benefits accrued during the year is calculated as the real increase in pension multiplied by 20, less the contributions made by the individual. The real increase excludes increases due to inflation or any increase or decrease due to a transfer of pension rights. This value derived does not represent an amount that will be received by the individual. It is a calculation that is intended to provide an estimation of the potential benefit of being a member of the pension scheme.
[168] Sir David Sloman’s salary was recharged to NHS England from the Royal Free London NHS Foundation Trust where he was also formally employed and retained a post. Sir David Sloman left NHS England on 03 September 2023. The full year equivalent salary is £230,000-£235,000.
[169] Sir James Mackey covered this post on an interim basis from 04 September 2023 to 31 October 2023 on an NHS assignment. Sir James Mackey’s salary costs were retained wholly by Northumbria NHS Foundation Trust where he was formally employed and retained a post.
[170] Dr Emily Lawson commenced in post on an interim basis on 01 November 2023. The full year equivalent salary is £250,000-£255,000.
[171] Mark Cubbon’s salary was recharged to NHS England from Portsmouth Hospitals NHS Trust where he was also formally employed and retained a post. Mark Cubbon left NHS England on 02 April 2023. The full year equivalent salary is £220,000-£225,000.
[172] Stephen Russell commenced in post on 03 April 2023. Stephen Russell’s benefit in kind relates to a Lease Car.
[173] Jacqueline Rock’s benefit in kind relates to a Lease Car.
[174] Dame Ruth May’s benefit in kind relates to a Lease Car.
[175] For the period 01 April 2023 to 09 May 2023 80% of the salary costs for Dr Tim Ferris were recharged to NHS England from Mass General Brigham Inc. where is he was also formally employed and retained a post, with NHS England directly funding the remaining 20%. For the period 10 May 2023 to 17 September 2023 NHS England directly funded 100% of the salary costs. Dr Tim Ferris left this post on 17 September 2023. The full year equivalent salary is £190,000-£195,000. NHS England also paid Mass General Brigham Inc. a retirement contribution of $0,000-$5,000.
[176] Dr Vinod Diwakar commenced in post on an interim basis on 18 September 2023. The full year equivalent salary is £205,000-£210,000.
Remuneration (salary, benefits in kind and pensions) 2022/23 (subject to audit)
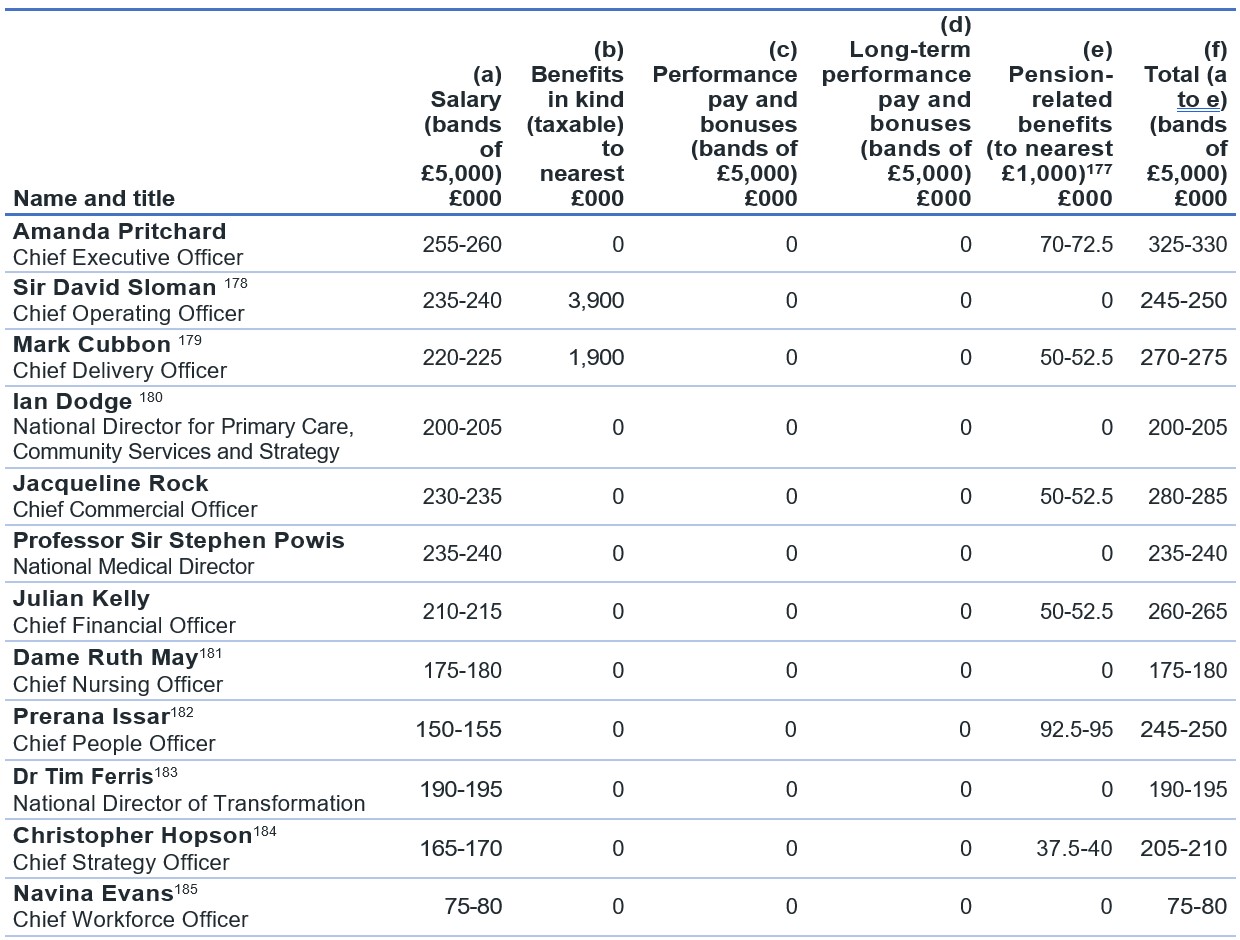
[177] The value of pension benefits accrued during the year is calculated as the real increase in pension multiplied by 20, less the contributions made by the individual. The real increase excludes increases due to inflation or any increase or decrease due to a transfer of pension rights. This value derived does not represent an amount that will be received by the individual. It is a calculation that is intended to provide an estimation of the potential benefit of being a member of the pension scheme.
[178] Sir David Sloman’s salary was recharged to NHS England from the Royal Free London NHS Foundation Trust where he was also formally employed and retained a post.
[179] Mark Cubbon’s salary was recharged to NHS England from Portsmouth Hospitals NHS Trust where he was also formally employed and retained a post. Mark Cubbon left NHS England on 2 April 2023.
[180] Ian Dodge left NHS England and NHS Improvement on 30 June 2022 and was paid a redundancy payment in the salary range of £160,000-£165,000 in July 2022 as compensation for loss of office; this is included in the salary band disclosed within the table. The full-year equivalent salary is £175,000-£180,000.
[181] Dame Ruth May retired on 16 June 2022 to access NHS Pension benefits and returned to post 18 June 2022 following the required 24 hours’ break in service. The full-year equivalent salary is £180,000-£185,000.
[182] Prerana Issar left NHS England on 04 October 2022. The full year equivalent salary is £230,000-£235,000.
[183] 80% of the salary costs for Dr Tim Ferris are recharged to NHS England and NHS Improvement from Mass General Brigham Inc. where is he is also formally employed and retains a post, with NHS England and NHS Improvement directly funding the remaining 20%. The full year equivalent salary is £190,000-£195,000. NHS England and NHS Improvement also paid Mass General Brigham Inc. a retirement contribution of $35,000-$40,000. Incorrect enrolment into the NHS Pension Scheme on commencement resulted in an underpayment of salary during 2021/22 due to pension contributions being deducted from his salary in error and these contributions were refunded during 2022/23.
[184] Christopher Hopson commenced in post on 13 June 2022. The full year equivalent salary is £205,000-£210,000.
[185] Navina Evans commenced in post on 01 July 2022 and 50% of the salary costs are recharged to NHS England from Health Education England where she was also formally employed and retained a post during 2022/23. As such, the above figures disclose 50% of salary, with Health Education England disclosing the remaining 50%. Dr Evans also received a payment for unused annual leave of £10-£15k, however Health Education England absorbed this full cost and 50% was not re-charged to NHS England. The full year equivalent salary is £205,000-£210,000.
Pension benefits (subject to audit)*
*Any members affected by the Public Service Pensions Remedy were reported in the 2015 scheme for the period between 01 April 2015 and 31 March 2022 in 2022/23 but are reported in the legacy scheme for the same period in 2023/24.
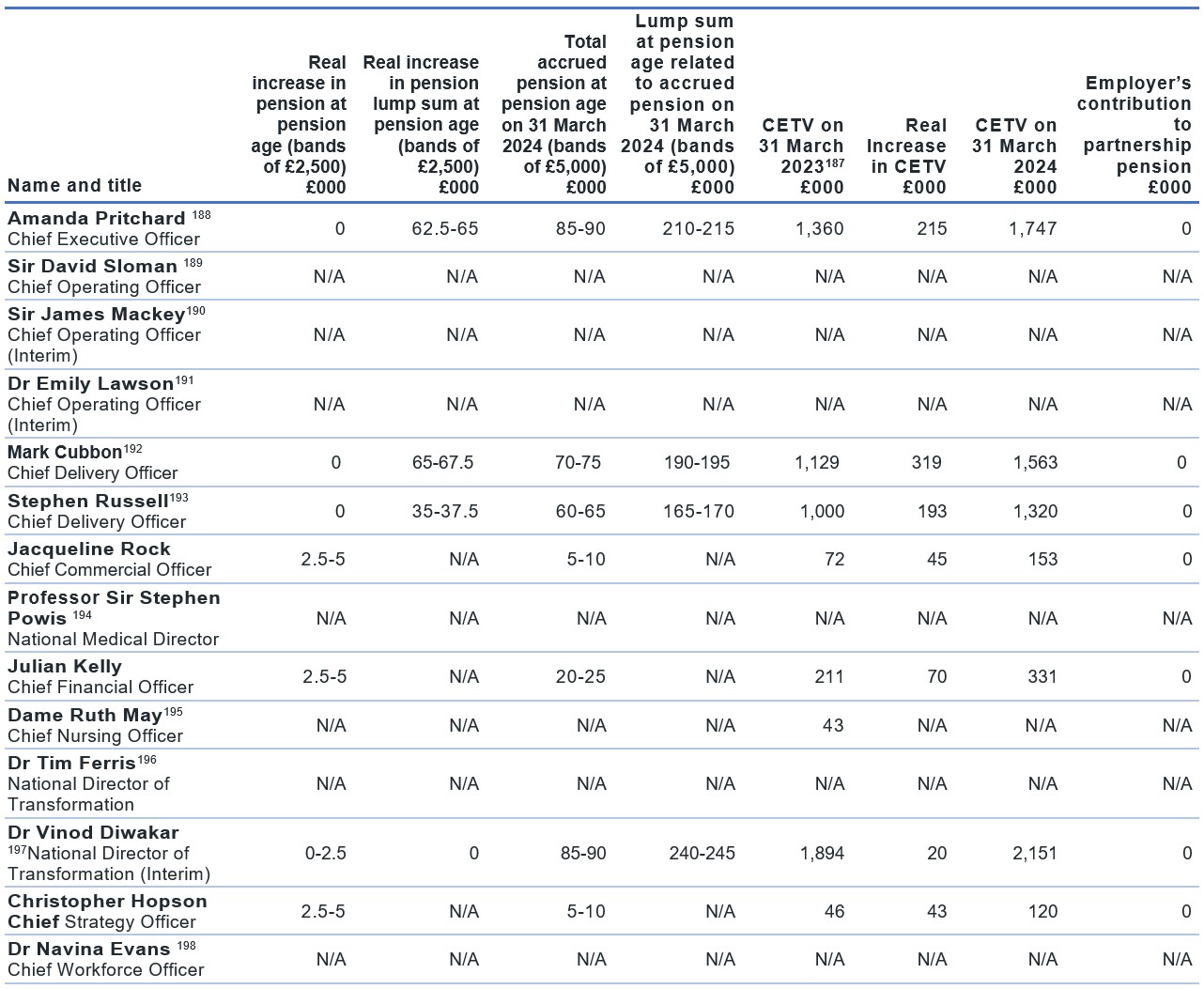
[187] As per previous submissions, the column Cash Equivalent Transfer Value on 31 March 2021 is the uninflated value whereas the real increase in CETV is the employer-funded increase.
[188] Amanda Pritchard is affected by the Public Service Pensions Remedy and their membership between 1 April 2015 and 31 March 2022 was moved back into the 1995/2008 Scheme on 01 October 2023. Negative values are not disclosed in this table but are substituted for a zero.
[189] Sir David Sloman chose not to be covered by the NHS Pension arrangements during the reporting period.
[190] Sir James Mackey chose not to be covered by the NHS Pension arrangements during the reporting period.
[191] Dr Emily Lawson chose not to be covered by the NHS Pension arrangements during the reporting period.
[192]Mark Cubbon left NHS England on 02 April 2023, therefore the Pension Benefits disclosed are pro-rata for this period.
[193] Stephen Russell is affected by the Public Service Pensions Remedy and their membership between 1 April 2015 and 31 March 2022 was moved back into the 1995/2008 Scheme on 01 October 2023. Negative values are not disclosed in this table but are substituted for a zero.
[194] Professor Sir Stephen Powis chose not to be covered by the NHS Pension arrangements during the reporting period.
[195] Dame Ruth May was covered by the NHS Pension arrangements during 2022/23 hence disclosure of the CETV at 31 March 2023, however accessed NHS 1995 Pension Scheme benefits during 2022/23 and chose not to be covered by the NHS Pension arrangements during this reporting period.
[196] Dr Tim Ferris was not eligible to be covered by NHS Pension arrangements during the reporting period.
[197] Dr Vinod Diwakar commenced in post on 18 September 2023 and is affected by the Public Service Pensions Remedy and their membership between 1 April 2015 and 31 March 2022 was moved back into the 1995/2008 Scheme on 01 October 2023. Negative values are not disclosed in this table but are substituted for a zero.
[198] Dr Navina Evans chose not to be covered by the NHS Pension arrangements during the reporting period.
Cash equivalent transfer values (subject to audit)
A CETV is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time.
The benefits valued are the member’s accrued benefits and any contingent spouse’s (or other allowable beneficiary’s) pension payable from the scheme.
A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme.
The pension figures shown relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies.
The CETV figures and the other pension details include the value of any pension benefits in another scheme or arrangement which the individual has transferred into the NHS Pension Scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
Real increase in CETV
This reflects the increase in CETV effectively funded by the employer. It does not include the increase in accrued pension due to inflation or contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement) and uses common market valuation factors for the start and end of the period.
Pensions liability
Past and present employees are covered by the provisions of the NHS Pension Schemes. Details of the benefits payable and rules of the schemes can be found on the NHS Pensions website. Both the 1995/2008 and 2015 schemes are accounted for, and the scheme liability valued, as a single combined scheme. Both are unfunded defined benefit schemes that cover NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State for Health and Social Care in England and Wales. They are not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, each scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS body of participating in each scheme is taken as equal to the contributions payable to that scheme for the accounting period.
In order that the defined benefit obligations recognised in the financial statements do not differ materially from those that would be determined at the reporting date by a formal actuarial valuation, the FReM requires that the period between formal valuations shall be four years, with approximate assessments in intervening years. An outline of these follows:
a) Accounting valuation
A valuation of scheme liability is carried out annually by the scheme actuary (currently the Government Actuary’s Department) as at the end of the reporting period. This utilises an actuarial assessment for the previous accounting period in conjunction with updated membership and financial data for the current reporting period and is accepted as providing suitably robust figures for financial reporting purposes. The valuation of the scheme liability as at 31 March 2024, is based on valuation data as 31 March 2023, updated to 31 March 2024 with summary global member and accounting data. In undertaking this actuarial assessment, the methodology prescribed in IAS 19, relevant FReM interpretations, and the discount rate prescribed by HM Treasury have also been used.
The latest assessment of the liabilities of the scheme is contained in the Statement by the Actuary, which forms part of the annual NHS Pension Scheme Annual Report and Accounts. These accounts can be viewed on the NHS Pensions website and are published annually. Copies can also be obtained from The Stationery Office.
b) Full actuarial (funding) valuation
The purpose of this valuation is to assess the level of liability in respect of the benefits due under the schemes (taking into account recent demographic experience), and to recommend contribution rates payable by employees and employers.
The latest actuarial valuation undertaken for the NHS Pension Scheme was completed as at 31 March 2020. The results of this valuation set the employer contribution rate payable from 1 April 2024 to 23.7% of pensionable pay. The core cost cap cost of the scheme was calculated to be outside of the 3% cost cap corridor as at 31 March 2020. However, when the wider economic situation was considered through the economic cost cap cost of the scheme, the cost cap corridor was not similarly breached. As a result, there was no impact on the member benefit structure or contribution rates.
Policy on remuneration of non-executive directors
The remuneration of non-executive directors is set by DHSC on appointment and is non-pensionable. All non-executive directors are paid the same amount, except the Chair and Chair of ARAC, to reflect the equal time commitment expected from each non-executive director. The Chair and Chair of ARAC are entitled to higher amounts to reflect the increased time commitment associated with their respective roles.
Some non-executive directors, including one of the Deputy Chairs, have opted to waive their contractual remuneration. Non-executive directors do not receive PRP or pensionable remuneration.
Non-executive director service contracts
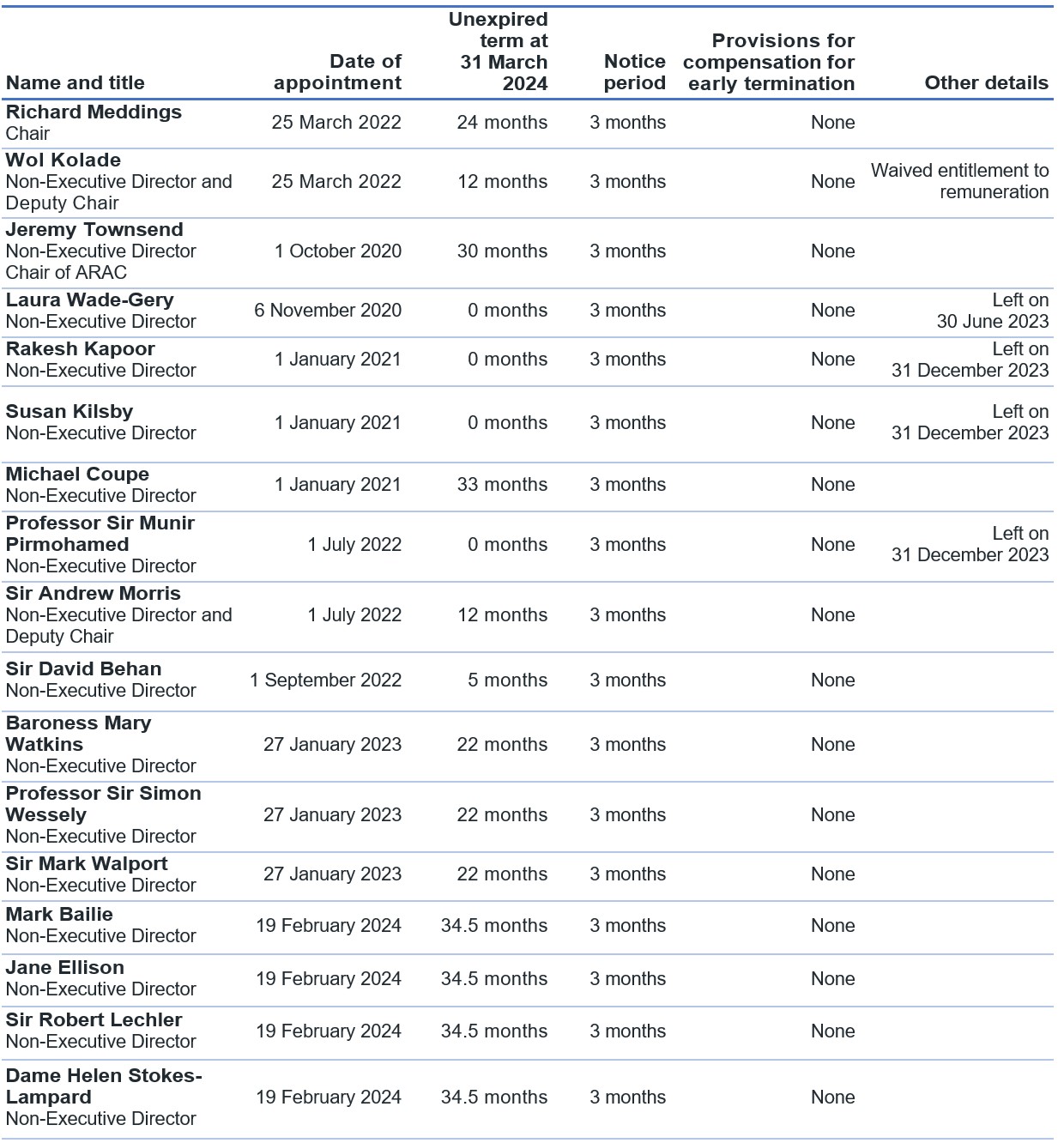
Non-executive director remuneration (including salary entitlements)
Salaries and allowances 2023/24 (subject to audit)
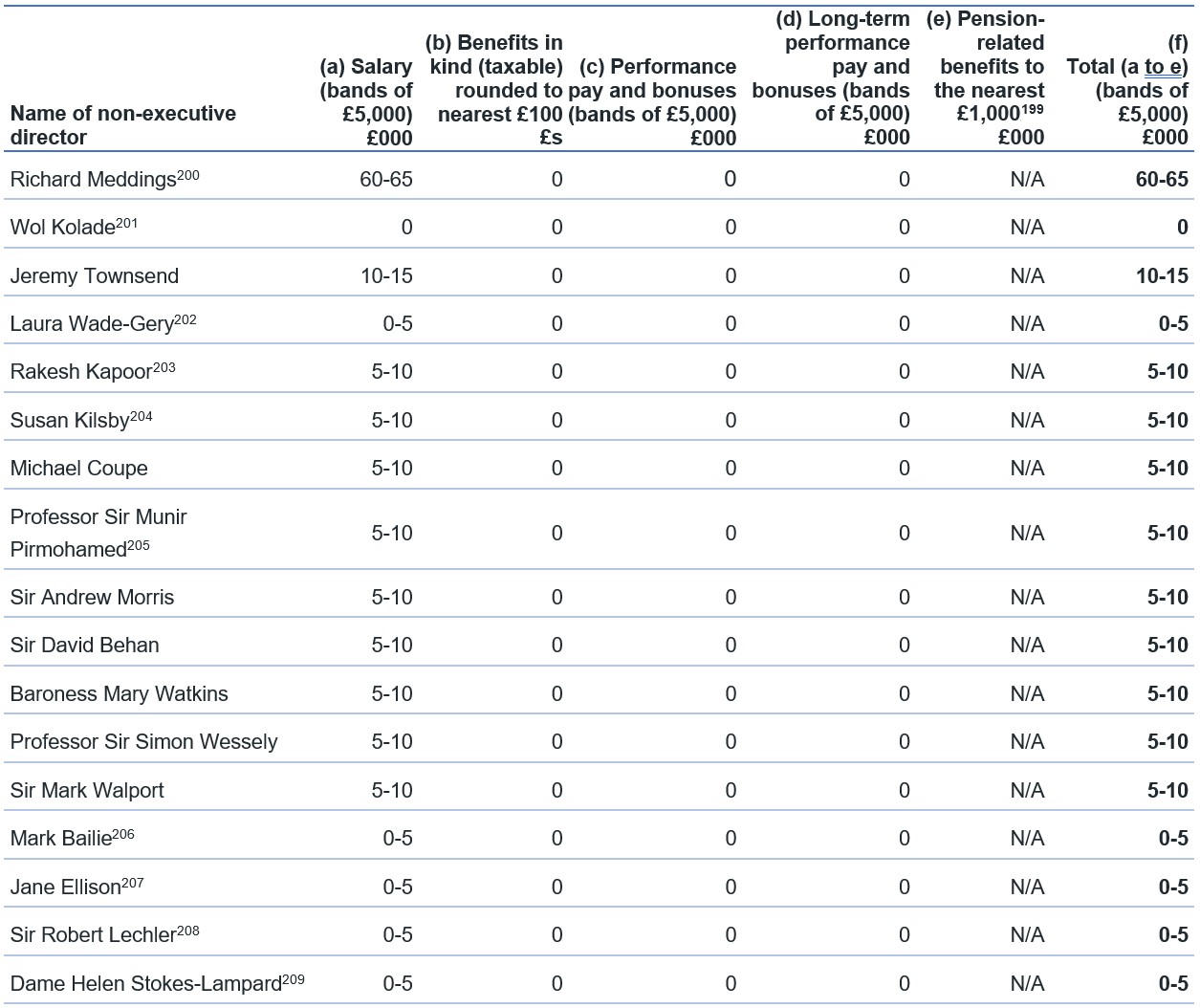
[199] Non-executive directors do not receive pensionable remuneration and therefore have no pension-related benefits
[200] Richard Meddings donated 100% of his non-executive director remuneration to charity via NHS England’s Give As You Earn scheme for the period 01 April 2023 to 31 October 2023, and 50% of his non-executive director remuneration from 01 November 2023.
[201] Wol Kolade waived his entitlement to non-executive director remuneration.
[202] Laura Wade-Gery left NHS England on 30 June 2023. The full-year equivalent salary is £5,000-£10,000.
[203] Rakesh Kapoor left NHS England on 31 December 2023. The full-year equivalent salary is £5,000-£10,000.
[204] Susan Kilsby left NHS England on 31 December 2023. The full-year equivalent salary is £5,000-£10,000.
[205] Professor Sir Munir Pirmohamed left NHS England on 31 December 2023. The full-year equivalent salary is £5,000-£10,000.
[206] Mark Bailie joined NHS England on 19 February 2024. The full-year equivalent salary is £5,000-£10,000. Mark Bailie donated 100% of his non-executive director remuneration to charity via NHS England’s Give As You Earn scheme.
[207] Jane Ellison joined NHS England on 19 February 2024. The full-year equivalent salary is £5,000-£10,000.
[208] Sir Robert Lechler joined NHS England on 19 February 2024. The full-year equivalent salary is £5,000-£10,000.
[209] Dame Helen Stokes-Lampard joined NHS England on 19 February 2024. The full-year equivalent salary is £5,000-£10,000.
Salaries and allowances 2022/23 (subject to audit)
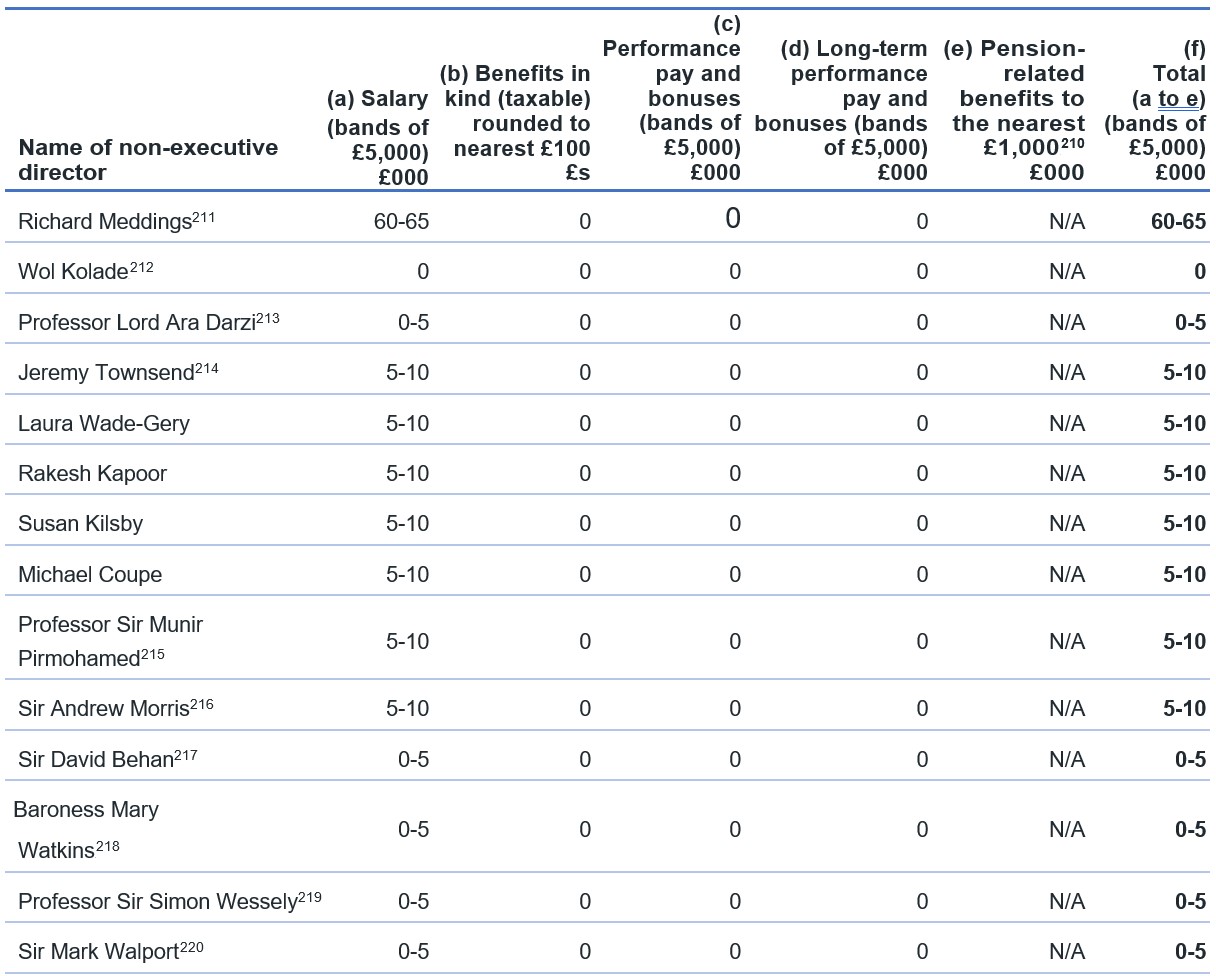
[210] Non-executive directors do not receive pensionable remuneration and therefore have no pension-related benefits.
[211] Richard Meddings donated his non-executive director remuneration to charity via NHS England’s Give As You Earn scheme.
[212] Wol Kolade waived his entitlement to non-executive director remuneration.
[213] Professor Lord Ara Darzi left NHS England on 30 June 2022. The full-year equivalent salary is £5,000-£10,000.
[214] Jeremy Townsend returned from a temporary transfer to NHS Improvement in the same role and salary of Non-Executive Director and Chair of ARAC on 1 July 2022. The full-year equivalent salary is £10,000-£15,000.
[215] Professor Sir Munir Pirmohamed transferred from NHS Improvement to NHS England in the same role and salary of Non-Executive Director on 1 July 2022. The full-year equivalent salary is £5,000-£10,000.
[216] Sir Andrew Morris transferred from NHS Improvement where he held the role of Interim Chair at a salary of £60,000-65,000 to NHS England as a Non-Executive Director on 1 July 2022. The full-year equivalent salary is £5,000-£10,000.
[217] Sir David Behan joined NHS England on 1 September 2022 and waived entitlement to non-executive director remuneration due to also being the Chair of Health Education England. The full-year equivalent salary is £5,000-£10,000.
[218] Baroness Mary Watkins joined NHS England on 27 January 2023. The full-year equivalent salary is £5,000-£10,000.
[219] Professor Sir Simon Wessely joined NHS England on 27 January 2023. The full-year equivalent salary is £5,000-£10,000.
[220] Sir Mark Walport joined NHS England on 27 January 2023. The full-year equivalent salary is £5,000-£10,000.
Parliamentary accountability and audit report
All elements of this report are subject to audit.
Remote contingent liabilities
There were no remote contingent liabilities.
Notation of gifts over £300,000
NHS England made no political or charitable donations of gifts during 2023/24.
Regularity of expenditure: Losses and special payments
Losses and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed legislation. By their nature they are items that ideally should not arise and are therefore subject to special control procedures compared to the generality of payments. They are divided into different categories, which govern the way that individual cases are handled.
Details of any losses and special payments relating to ICBs and CCGs can be found within individual ICBs and CCGs annual reports which are published on ICB websites. A list of ICBs and CCGs, along with links to their websites, can be found on the NHS England website.
Losses
The total number of NHS England losses cases, and their total value, was as follows:
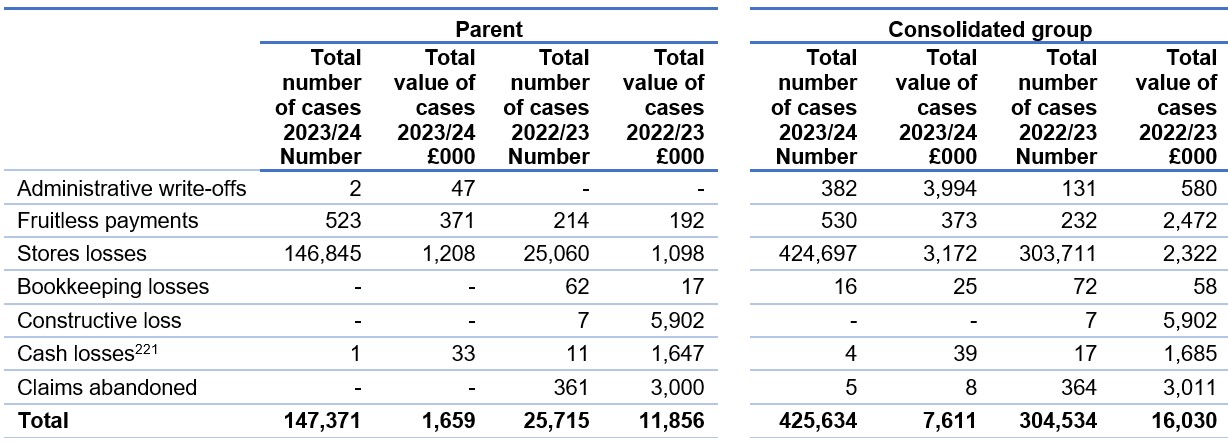
2023/24 Disclosure: Store losses
£1.2 million – there is one instance comprising of multiple individual items for £1.1 million that relates to various stock items that cannot be utilised in healthcare facilities, as the stock has reached the manufacturer’s expiry date and therefore requires writing off.
2022/23 Disclosure: Fruitless Payment
£0.6 million – NHS Gloucestershire ICB have agreed and paid a legal settlement agreement granted by the court in financial year 2022/23. The ICB settled a court order agreement in breach of the Public Contracts Regulations 2015 in their award of the contract for advice and guidance services in 2022/23.
£0.9 million -NHS Bath and North East Somerset, Swindon and Wiltshire ICB have agreed and paid a legal settlement agreement granted by the court in financial year 2022/23. The ICB settled a court order agreement in breach of the Public Contracts Regulations 2015 in their award of the contract for advice and guidance services in 2022/23.
2022/23 Disclosure: Store losses
£1.10 million – This case relates to various stock items that cannot be utilised in healthcare facilities as the stock has reached the manufacturer’s expiry date and therefore requires
writing off.
2022/23 Disclosure: Constructive losses
£1.102 million- This case relates to the disposal of six vaporisers which support the provision of oxygen to patients. The vaporisers were purchased in March 2020 by NHS England for the London Nightingale Hospital at the ExCeL. Following decommissioning of the facility, the vaporisers were placed into storage to be available if ever required. As many hospital facilities have since been upgraded, these vaporisers are no longer compatible to be deployed into a hospital facility and are therefore surplus to requirements.
£4.80 million – This case relates to stock that was procured as part of the Vaccine Deployment Programme in response to the COVID-19 pandemic. The stock was procured in extreme urgency and considerable uncertainty in terms of supply chains and demand. The stock is now deemed as surplus to requirement and retaining the stock in storage will not equate to value for money when compared to the continuing costs of storage.
2022/23 Disclosure: Cash losses
£0.73 million – This relates to two cases of overpayments for suspended medical practitioners who were both paid incorrectly and not in accordance with the Secretary of State guidance. The first case relates to a General Practitioner who was overpaid during the period of March 2020 to June 2022 equating to the sum for £0.42 million and the second to a General Practitioner overpaid £0.31 million between April 2019 and March 2022. Both of these overpayments were caused by the failure to cease payments when the suspended GPs had resigned as practice partners, therefore would not qualify for any suspension payments in accordance with the Secretary of State Payment Determination guidance.
£0.31 million – This case relates to non-delivery of contractual dental units of activity as part of the General Dental Service. The registered performer failed to deliver the contractually agreed units of dental and orthodontic activities for the financial periods commencing from 2016 to 2022. In addition, as part of the new COVID-19 rules issued by NHS England, the registered performer did not comply with new contractual obligations to provide urgent face to face dental care. The sum being reported represents the totality of payments made where there has been no benefit to NHS England or patients.
2022/23 Disclosure Claims abandoned
£2.83 million- This case relates to the request to write off a grant awarded by a local health authority in 1989 to develop a mental health facility. The value of the write off includes the total of the original grant of £1.75 million and the subsequent capital gain on the property equating to £1.08 million. The funded asset was utilised for the provision of mental health care within Trust grounds by a charitable organisation. A decision was taken to dispose the funded asset to the Trust as part of a modernisation programme for mental health inpatient facilities. The capital grant agreement included a legal charge in favour of the Secretary of State for the receipts in the event that the applicant disposes of the funded asset. NHS England is the successor of health authorities and primary care trusts for the purposes of this capital grant agreement.
Special payments
The total number of NHS England special payments cases, and their total value, was as follows:
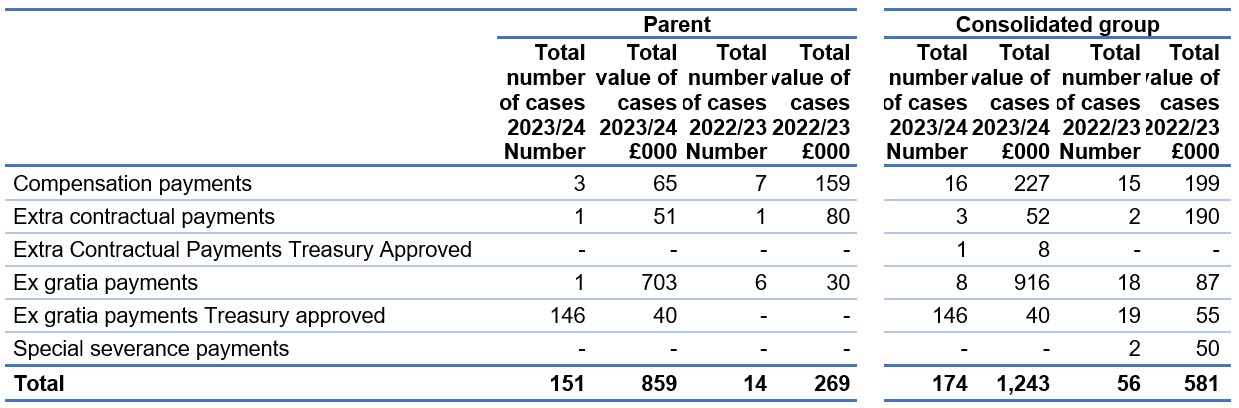
All cases classified as special severance payments are subject to HM Treasury approval.
2023/24 Ex Gratia Payments
£703k- This case relates to the IR35 employment status assessments for all relevant OPW engagements relating to the financial periods 2017 to 2019. 159 engagements of OPW were deemed to have been subject to IR35 regulations and the payment due reflects the outcome of the assessment carried out.
This payment relates to the negotiated settlement of the sum including interest due to HMRC in relation to those OPWs who based on a more recent understanding of HMRC interpretation of the rules and indicators, may have been incorrectly deemed out-of-scope.
2022/23 Special severance payments
During 2022/23 SCCL paid two special severance payments for £30,000 and £20,000 respectively. The payment of £30,000 relates to a non-contractual amount to terminate employment and the payment of £20,000 relates to a non-contractual payment in relation to a dispute settlement. These payments were not approved by NHS England and are therefore irregular.
Cost allocation and setting of charges
NHS England certifies that it has complied with the HM Treasury guidance on cost allocation and the setting of charges. The following table provides details of income generation activities whose full cost exceeded £1 million or was otherwise material:
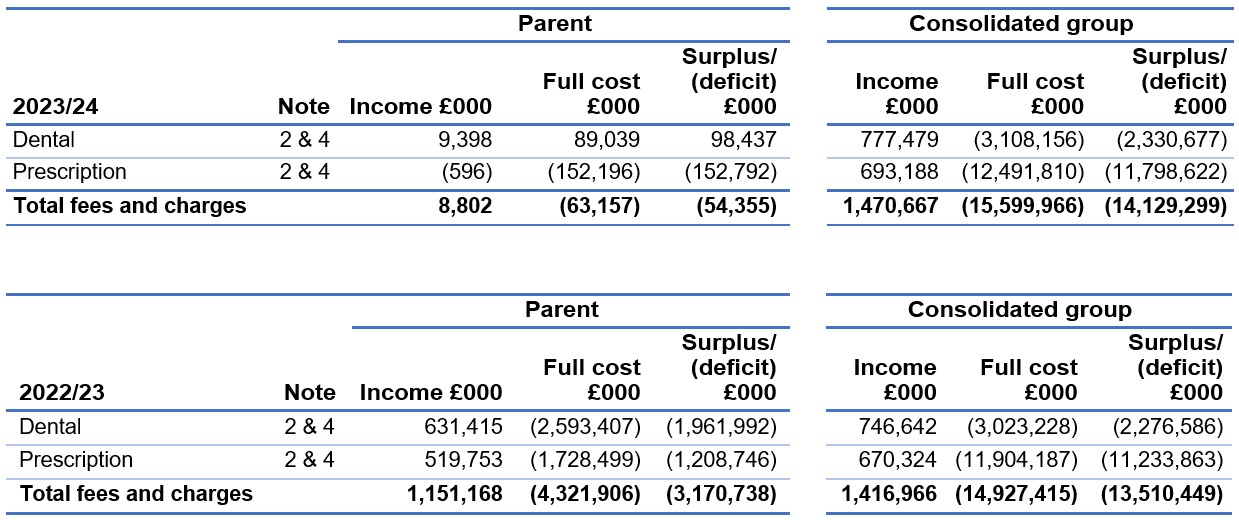
The fees and charges information in this note is provided in accordance with section 3.2.12 of the Government FReM. It is provided for fees and charges purposes and not for international financial reporting standards (IFRS) 8 purposes. The financial objective of prescription and dental charges is to collect charges only from those patients that are eligible to pay.
Prescription charges are a contribution to the cost of pharmaceutical services including the supply of drugs. In 2023/24, the NHS prescription charge for each medicine or appliance dispensed was £9.65. However, around 90% of prescription items are dispensed free each year where patients are exempt from charges. In addition, patients who were eligible to pay charges could purchase pre-payment certificates at £31.25 for three months or £111.60 for a year. A number of other charges were payable for wigs and fabric supports.
Those who are not eligible for exemption are required to pay NHS dental charges which fall into three bands depending on the level and complexity of care provided. From 24 April 2023, the charge for Band 1 treatments was £25.80, for Band 2 was £70.70 and for Band 3 was £306.80. Prior to this uplift the charge for Band 1 treatments was £23.80, for Band 2 was £65.20 and for Band 3 was £282.80.
The certificate of the Comptroller and Auditor General to the Houses of Parliament
Opinion on financial statements
I certify that I have audited the financial statements of NHS England and its group for the year ended 31 March 2024 under the National Health Service Act 2006 and the Health and Social Care Act 2012.
The financial statements comprise NHS England and its group’s:
- Statement of Financial Position as at 31 March 2024
- Statement of Comprehensive Net Expenditure, Statement of Cash Flows and Statement of Changes in Taxpayers’ Equity for the year then ended and
- the related notes including the significant accounting policies.
The financial reporting framework that has been applied in the preparation of the group financial statements is applicable law and UK adopted International Accounting Standards.
In my opinion, the financial statements:
- give a true and fair view of the state of NHS England and its group’s affairs as at 31 March 2024 and their total net expenditure for the year then ended; and
- have been properly prepared in accordance with the National Health Service Act 2006 and the Health and Social Care Act 2012 and Secretary of State directions issued thereunder.
Opinion on regularity
In my opinion, in all material respects, the income and expenditure recorded in the financial statements have been applied to the purposes intended by Parliament and the financial transactions recorded in the financial statements conform to the authorities which govern them.
Basis for opinions
I conducted my audit in accordance with International Standards on Auditing (UK) (ISAs UK), applicable law and Practice Note 10 Audit of Financial Statements and Regularity of Public Sector Bodies in the United Kingdom (2022). My responsibilities under those standards are further described in the Auditor’s responsibilities for the audit of the financial statements section of my certificate.
Those standards require me and my staff to comply with the Financial Reporting Council’s Revised Ethical Standard 2019. I am independent of NHS England and its group in accordance with the ethical requirements that are relevant to my audit of the financial statements in the UK. My staff and I have fulfilled our other ethical responsibilities in accordance with these requirements.
I believe that the audit evidence I have obtained is sufficient and appropriate to provide a basis for my opinion.
Conclusions relating to going concern
In auditing the financial statements, I have concluded that NHS England and its group’s use of the going concern basis of accounting in the preparation of the financial statements is appropriate.
Based on the work I have performed, I have not identified any material uncertainties relating to events or conditions that, individually or collectively, may cast significant doubt on NHS England and its group’s ability to continue as a going concern for a period of at least twelve months from when the financial statements are authorised for issue.
My responsibilities and the responsibilities of the Board and the Accounting Officer with respect to going concern are described in the relevant sections of this certificate.
The going concern basis of accounting for NHS England and its group is adopted in consideration of the requirements set out in HM Treasury’s Government Financial Reporting Manual, which require entities to adopt the going concern basis of accounting in the preparation of the financial statements where it is anticipated that the services which they provide will continue into the future.
Other Information
The other information comprises the information included in the Annual Report but does not include the financial statements nor my auditor’s certificate and report thereon. The Board and Accounting Officer is responsible for the other information.
My opinion on the financial statements does not cover the other information and, except to the extent otherwise explicitly stated in my certificate, I do not express any form of assurance conclusion thereon.
My responsibility is to read the other information and, in doing so, consider whether the other information is materially inconsistent with the financial statements, or my knowledge obtained in the audit, or otherwise appears to be materially misstated.
If I identify such material inconsistencies or apparent material misstatements, I am required to determine whether this gives rise to a material misstatement in the financial statements themselves. If, based on the work I have performed, I conclude that there is a material misstatement of this other information, I am required to report that fact.
I have nothing to report in this regard.
Opinion on other matters
In my opinion the part of the Remuneration and Staff Report to be audited has been properly prepared in accordance with Secretary of State directions issued under the National Health Service Act 2006 and the Health and Social Care Act 2012.
In my opinion, based on the work undertaken in the course of the audit:
- the parts of the Accountability Report subject to audit have been properly prepared in accordance with Secretary of State directions made under the National Health Service Act 2006 and the Health and Social Care Act 2012; and
- the information given in the Performance and Accountability Reports for the financial year for which the financial statements are prepared is consistent with the financial statements and is in accordance with the applicable legal requirements.
Matters on which I report by exception
In the light of the knowledge and understanding of NHS England and its group, and its environment obtained in the course of the audit, I have not identified material misstatements in the Performance and Accountability Reports.
I have nothing to report in respect of the following matters which I report to you if, in my opinion:
- adequate accounting records have not been kept by NHS England and its group or returns adequate for my audit have not been received from branches not visited by my staff; or
- I have not received all of the information and explanations I require for my audit; or
- the financial statements and the parts of the Accountability Report subject to audit are not in agreement with the accounting records and returns; or
- certain disclosures of remuneration specified by HM Treasury’s Government Financial Reporting Manual have not been made or parts of the Remuneration and Staff Report to be audited is not in agreement with the accounting records and returns; or
- the governance statement does not reflect compliance with HM Treasury’s guidance.
Responsibilities of the Board and Accounting Officer for the financial statements
As explained more fully in the Statement of Accounting Officer’s responsibilities, the board and Accounting Officer are responsible for:
- maintaining proper accounting records;
- providing the C&AG with access to all information of which management is aware that is relevant to the preparation of the financial statements such as records, documentation and other matters;
- providing the C&AG with additional information and explanations needed for his audit;
- providing the C&AG with unrestricted access to persons within NHS England and its group from whom the auditor determines it necessary to obtain audit evidence;
- ensuring such internal controls are in place as deemed necessary to enable the preparation of financial statement to be free from material misstatement, whether due to fraud or error;
- preparing financial statements which give a true and fair view in accordance with Secretary of State directions made under the National Health Service Act 2006 and the Health and Social Care Act 2012;
- preparing the annual report, which includes the Remuneration and Staff Report, in accordance with Secretary of State directions made under the National Health Service Act 2006 and the Health and Social Care Act 2012; and
- assessing NHS England and its Group’s ability to continue as a going concern, disclosing, as applicable, matters related to going concern and using the going concern basis of accounting unless the Accounting Officer anticipates that the services provided by NHS England and its group will not continue to be provided in the future.
Auditor’s responsibilities for the audit of the financial statements
My responsibility is to audit, certify and report on the financial statements in accordance with the National Health Service Act 2006 and the Health and Social Care Act 2012.
My objectives are to obtain reasonable assurance about whether the financial statements as a whole are free from material misstatement, whether due to fraud or error, and to issue a certificate that includes my opinion. Reasonable assurance is a high level of assurance but is not a guarantee that an audit conducted in accordance with ISAs (UK) will always detect a material misstatement when it exists. Misstatements can arise from fraud or error and are considered material if, individually or in the aggregate, they could reasonably be expected to influence the economic decisions of users taken on the basis of these financial statements.
Extent to which the audit was considered capable of detecting non-compliance with laws and regulations including fraud
I design procedures in line with my responsibilities, outlined above, to detect material misstatements in respect of non-compliance with laws and regulations, including fraud. The extent to which my procedures are capable of detecting non-compliance with laws and regulations, including fraud is detailed below.
Identifying and assessing potential risks related to non-compliance with laws and regulations, including fraud
In identifying and assessing risks of material misstatement in respect of non-compliance with laws and regulations, including fraud, I:
- considered the nature of the sector, control environment and operational performance including the design of NHS England and its group’s accounting policies, key performance indicators and performance incentives.
- inquired of management, NHS England’s head of internal audit and those charged with governance, including obtaining and reviewing supporting documentation relating to NHS England and its group’s policies and procedures on:
- identifying, evaluating and complying with laws and regulations;
- detecting and responding to the risks of fraud; and
- the internal controls established to mitigate risks related to fraud or non-compliance with laws and regulations including NHS England and its group’s controls relating to NHS England’s compliance with the National Health Service Act 2006, Health and Social Care Act 2012, Health and Care Act 2022 and Managing Public Money.
- inquired of management, NHS England’s head of internal audit and those charged with governance whether:
- they were aware of any instances of non-compliance with laws and regulations; and
- they had knowledge of any actual, suspected, or alleged fraud;
- discussed with the engagement team regarding how and where fraud might occur in the financial statements and any potential indicators of fraud.
As a result of these procedures, I considered the opportunities and incentives that may exist within NHS England and its group for fraud and identified the greatest potential for fraud in the following areas: revenue recognition, posting of unusual journals, complex transactions, and bias in management estimates. In common with all audits under ISAs (UK), I am also required to perform specific procedures to respond to the risk of management override.
I obtained an understanding of NHS England and its group’s framework of authority and other legal and regulatory frameworks in which NHS England and its group operate. I focused on those laws and regulations that had a direct effect on material amounts and disclosures in the financial statements or that had a fundamental effect on the operations of NHS England and its group. The key laws and regulations I considered in this context included the National Health Service Act 2006, Health and Social Care Act 2012, Health and Care Act 2022, Managing Public Money, employment law, tax legislation, relevant legislation relating to fees charged by the NHS England, and regulations relating to suspension payments to suspended medical practitioners.
In addition, I considered regulations and regularity relating to exit packages and, in particular, special severance payments, as I identified the completeness and regularity of exits packages as a significant risk.
Audit response to identified risk
To respond to the identified risks resulting from the above procedures:
- I reviewed the financial statement disclosures and testing to supporting documentation to assess compliance with provisions of relevant laws and regulations described above as having direct effect on the financial statements;
- I enquired of management and the Audit and Risk Assurance Committee concerning actual and potential litigation and claims;
- I reviewed minutes of meetings of those charged with governance and the board and internal audit reports;
- I addressed the risk of fraud through management override of controls by testing the appropriateness of journal entries and other adjustments; assessing whether the judgements on estimates are indicative of a potential bias; and evaluating the business rationale of any significant transactions that are unusual or outside the normal course of business; and
- I reviewed all special severance payments included in the NHS England’s group Remuneration and Staff Report.
I communicated relevant identified laws and regulations and potential risks of fraud to all engagement team members and remained alert to any indications of fraud or non-compliance with laws and regulations throughout the audit.
A further description of my responsibilities for the audit of the financial statements is located on the Financial Reporting Council’s website at: www.frc.org.uk/auditorsresponsibilities. This description forms part of my certificate.
Other auditor’s responsibilities
I am required to obtain evidence sufficient to give reasonable assurance that the expenditure and income recorded in the financial statements have been applied to the purposes intended by Parliament and the financial transactions recorded in the financial statements conform to the authorities which govern them.
I communicate with those charged with governance regarding, among other matters, the planned scope and timing of the audit and significant audit findings, including any significant deficiencies in internal control I identify during my audit.
Gareth Davies, Comptroller and Auditor General
National Audit Office, 157-197 Buckingham Palace Road, Victoria, London SW1W 9SP
7 October 2024
The report of the Comptroller and Auditor General to the Houses of Parliament
Introduction
1. The National Health Service Act 2006 and the Health and Social Care Act 2012 requires NHS England to prepare consolidated annual accounts for each financial year. The consolidated accounts must contain NHS England’s annual accounts and a consolidation of NHS England’s annual accounts, the annual accounts of each Integrated Care Board (ICB), and the annual accounts of the Supply Chain Coordination Limited (SCCL). NHS England’s consolidated accounts are in turn consolidated in the accounts of the Department of Health and Social Care (DHSC). I consider NHS England to be a significant component of DHSC and my audit of NHS England must be complete before I complete my audit of DHSC.
2. I am required to examine, certify, and report on NHS England’s consolidated accounts. I provide an opinion on whether the consolidated accounts give a “true and fair” view of NHS England’s finances for the year. I also provide an opinion on whether the transactions recorded in NHS England’s consolidated accounts have been applied to the purposes intended by Parliament and whether they conform to the authorities which govern them (“regularity”).
3. In 2022-23 and 2021-22, I qualified my regularity opinion on NHS England’s consolidated accounts due to ineligible suspension payments made to suspended medical practitioners (a medical practitioner could be a doctor, dentist or optician), as I considered the payments, which were not made in accordance with the relevant statutory regulations to be irregular and material by their nature. Details of the prior year qualification are provided on pages 125 to 135 of the NHS England annual report and accounts 2022 to 2023.
4. In this report, I explain why I have decided not to qualify my regularity opinion on NHS England’s 2023-24 consolidated accounts. I also provide an update on the performance of ICBs in delivering accounts to support the timely production of NHS England’s consolidated accounts, given significant delays experienced in 2022-23. In addition, I highlight the current state of NHS financial sustainability, and refer to a more detailed report I published in July 2024 on NHS financial management and sustainability.
Suspension payments to suspended medical practitioners
5. Under certain qualifying circumstances NHS England can make suspension payments to medical practitioners who have been suspended as set out in relevant statutory regulations. Under statutory regulations, issued by the Secretary of State for Health and Social Care, NHS England may suspend a medical practitioner when satisfied that it is necessary to do so for the protection of patients or members of the public or that it is otherwise in the public interest. A suspended medical practitioner may be entitled to receive suspension payments if the medical practitioner meets certain qualifying conditions. If the medical practitioner qualifies for suspension payments, such payments may continue until a relevant tribunal has considered the suspension and either ends the suspension or removes the medical practitioner from the medical register. For example, the General Medical Council (GMC) maintains a medical register of doctors licensed to practise medicine. The GMC considers suspensions concerning doctors. The General Dental Council and General Optical Council perform a similar role for dentists and opticians, respectively.
6. In 2022-23 and 2021-22 it was identified, by NHS England and my staff, that 14 medical practitioners had received ineligible suspension payments over the 2017-18 to 2022-23 financial years. During my 2022-23 audit, 12 medical practitioners were identified as having received ineligible suspension payments over the 2017-18 to 2022-23 financial years, totalling £1,298,033. During my 2021-22 audit, two medical practitioners were identified as having received ineligible suspension payments over the 2017-18 to 2021-22 financial years, totalling £963,513.
7. I qualified my regularity opinion in 2022-23 and 2021-22 in relation to these ineligible suspension payments. As the suspension payments I refer to in paragraph 6 were made contrary to the statutory regulations governing such payments, I considered them to be irregular. The circumstances that led to these irregular payments being made were such that I considered that insufficient regard had been paid to the framework of authorities and use of public funds and that the payments are therefore material by virtue of their nature. Additionally, suspension of a medical practitioner often involves serious misconduct, and I considered payment of ineligible suspension payments in those circumstances to be contentious. NHS England should have had checks in place to prevent or detect such payments. I therefore qualified my regularity opinion on the consolidated accounts in 2022-23 and 2021-22.
8. My staff were content that all suspension payments made to suspended medical practitioners in 2023-24, they selected for review, were paid in accordance with the regulations and therefore regular. In 2023-24, NHS England made suspension payments to 42 suspended medical practitioners, totalling £2,102,652. As part of my 2023-24 audit, my staff selected a risk based sample of 21 suspended medical practitioners, who had received suspension payments during 2023-24, and reviewed all suspension payments made to the selected medical practitioners. My staff were content all the payments they tested in 2023-24 were regular.
9. The only ineligible suspension payments made to a medical practitioner in 2023-24 related to a case I identified as part of my 2022-23 regularity qualification. As part my 2022-23 audit, my staff identified a suspended medical practitioner who had received ineligible suspension payments from 2017-18 to 2022-23. However, as my staff were performing their testing on the 2022-23 audit in 2023-24, the ineligible suspension payments to this suspended medical practitioner continued into 2023-24. When NHS England undertook a full review of this case in July 2024, they identified that the medical practitioner received £60,918 in ineligible suspension payments in 2023-24 and £9,322 in 2024-25.
10. Prior to 1 April 2024, NHS England administered suspension payments to suspended medical practitioners on a regional basis, meaning seven separate regional teams were involved in determining the eligibility for suspension payments, confirming the amounts to be paid and confirming continuing eligibility. This regional system was partly the reason why ineligible suspension payments had been made, as staff, in some cases, appeared to have misunderstood the statutory regulations, which lead to suspended medical practitioners receiving suspension payments to which they were never entitled or at the wrong amount. Additionally, staff in regional teams did not adequately confirm medical practitioners’ continuing eligibility to suspension payments; nor did they always act on information received from medical practitioners themselves, that the practitioners in question were no longer eligible to the suspension payments.
11. From 1 April 2024, suspension payments to suspended medical practitioners are administered by a single national team. NHS England made the change from a regional to national process for administering suspension payments to suspended medical practitioners, as it considers a single national team will develop a more detailed understanding of the statutory regulations, resulting in fewer mistakes and more consistent processes for establishing eligibility, amounts to be paid, and confirming continued eligibility. My staff will review this new process as part of my 2024-25 audit. My staff liaised with the new national team to complete testing of 2023-24 suspension payments. My staff consider this new national team had a better understanding of the statutory regulations and the individual cases and were able to answer questions and address queries far better than when the process was administered regionally.
12. I have not qualified my regularity opinion in 2023-24. As the only ineligible suspensions payments made to a medical practitioner in 2023-24 related to a case I identified as part of my 2022-23 regularity qualification, I have decided not to qualify my regularity opinion in 2023-24. I do not consider the amounts involved to be material by value or nature. In making this decision I have taken into account the changes NHS England has made for administering suspension payments, which I outline in paragraph 11, which I consider should result in more accurate administration of the system for making suspension payments.
13. NHS England has not recovered most of the ineligible suspension payments it made. Ineligible suspension payments made to four of the 12 medical practitioners in 2022-23 have been recovered in full by NHS England. These recoveries amount to £48,917. Following legal advice NHS England will not be attempting to recover ineligible suspension payments relating to three medical practitioners (totalling £908,139) as it concludes pursuing recovery is unlikely to be a good use of public funds.. NHS England are seeking to recover any other ineligible suspension payments it made.
Audit of Integrated Care Boards
14. NHS England group entities are audited by a number of different audit firms. ICBs are responsible for appointing their external auditors (‘local auditors’). Local auditors must comply with the Code of Audit Practice (‘the Code’). Under the Local Audit and Accountability Act 2014 (‘the 2014 Act’), I am responsible for the preparation, publication, and maintenance of the Code. The Code sets out what local auditors are required to do to fulfil their statutory responsibilities under the 2014 Act. For 2023-24, ICB audits were undertaken by six audit firms, the same number as in 2022-23.
15. The Code stresses the need for local auditors to report on a timely basis. Section 1.19 of the Code requires local auditors to report on a timely basis. Timely reporting includes producing audit reports in time, insofar as the auditor can do so under auditing standards, to allow local bodies to comply with the requirements placed on them to publish their audited financial statements. It also means ensuring that when matters of concern arise during the audit, the auditor raises them promptly with the body and considers whether the matter needs to be brought to public attention at the appropriate time.
16. In 2022-23 there were significant delays in commissioners finalising their audited accounts. In 2022-23 NHS England required commissioners to have their statutory audits completed by 30 June 2023. In 2022-23 there were 106 Clinical Commissioning Groups (CCGs) until 30 June 2022. CCGs were replaced by 42 ICBs on 1 July 2022. CCGs and ICBs were collectively referred to as commissioners. CCGs had to produce three month closure accounts from 1 April to 30 June 2022, and ICBs had to produce nine month opening accounts from 1 July 2022 to 31 March 2023. This resulted in a large NHS England group structure for 2022-23 with 149 group entities (106 CCGs for three months, 42 ICBs for nine months and SCCL).
17. Less than four fifths of bodies achieved the target date set by NHS England in 2022-23, with 117 commissioner audits completed by 30 June 2023. By 31 July 2023, 131 (88.5%) commissioner audits were completed, with 134 (90.5%) commissioner audits completed by 31 October 2023. This was the latest practical date to enable certification of the NHS England and DHSC annual report and accounts by 30 November 2023, which was the original planned certification date for 2022-23.
18. At the point NHS England finalised its 2022-23 accounts, nine commissioner audits remained outstanding. By Christmas 2023, 139 commissioner audits were completed, with the remaining nine audits outstanding as the NHS England accounts were finalised. NHS England performed alternative procedures to obtain sufficient assurance that the material transactions streams in the outstanding commissioners were not materially misstated, in the context of the NHS England group accounts. My staff reviewed the procedures performed by NHS England and were content that, in the context of the NHS England group accounts, the results provided sufficient and appropriate assurance for my audit. I therefore issued an unqualified ‘true and fair’ audit opinion in respect of the NHS England annual report and accounts 2022-23.
19. DHSC committed to laying its 2023-24 annual report and accounts before the end of 2024. At a Public Accounts Committee hearing on 13 March 2024, regarding the DHSC annual report and accounts 2022-23, DHSC’s stated aspiration “is to bring it (laying of the annual report and accounts) forward by at least a month each year”. Before the Covid-19 pandemic, DHSC and NHS England routinely laid their annual reports and accounts in Parliament before the Parliamentary summer recess. The last time this happened was for the 2018-19 annual report and accounts. For the 2023-24 accounts, NHS England and my staff agreed a target date of October 2024 for audit certification, to enable DHSC to lay its annual report and accounts before the 2024 Parliamentary Christmas recess.
20. In 2023-24 the NHS England group had far fewer consolidating entities, with 42 ICBs and SCCL. In 2023-24 the NHS England group consisted of the NHS England parent, 42 ICBs and SCCL. While there were fewer commissioners to consolidate, on average ICBs are significantly larger than CCGs. NHS England was proactive in 2023-24 in monitoring the progress of ICB accounts delivery, including engaging with the ICBs, local auditors, my staff, HM Treasury and the Financial Reporting Council (which regulates local audit firms).
21. NHS England set a deadline of 28 June 2024 for ICBs to have their 2023-24 annual reports and accounts audited. By 28 June 2024, 38 (90.5%) ICB annual report and accounts were audited, and this number increased to 41 (97.6%) by 31 July 2024. This is a significant improvement compared to 2022-23 and in large part due to the reduced number of commissioners and proactive monitoring by NHS England.
22. At the point NHS England finalised its 2023-24 group accounts, only one ICB audit remained outstanding. The only ICB not to have its 2023-24 annual report and accounts audited, at the point NHS England finalised its group accounts was North West London ICB. This ICB has not yet had its 2022-23 annual report and accounts certified. NHS England and my staff will continue to monitor progress on the timeliness of this ICB’s accounts production and audit. NHS England performed alternative procedures to obtain sufficient assurance that the material transaction streams in Northwest London ICB’s draft 2023-24 accounts were not materially misstated, in the context of the NHS England group accounts. My staff reviewed the procedures performed by NHS England and are content that, in the context of the NHS England group accounts, the results provide sufficient and appropriate assurance for my audit. I have therefore issued a clean ‘true and fair’ audit opinion in respect of the NHS England annual report and accounts 2023-24.
23. I continue to have concerns given the wider local audit challenges, as set out in my report, Timeliness of local auditor reporting on local government in England. Whilst the number of commissioner accounts in 2023-24 reduced to 42, and overall these accounts were audited much earlier in 2023-24 than in 2022-23, there could still be some risk in the delivery of NHS local audits going forward, due to the wider local audit system issues and significant delays in local government audits as the auditors work to clear this backlog. I have developed a new draft Code which has been laid in Parliament following a consultation that is intended to support measures taken by the Ministry of Housing, Communities and Local Government (MHCLG) to address the current backlog of local government audits. MHCLG has also laid regulations to introduce statutory deadlines for publication of audited accounts, which is intended to work alongside the draft Code.
Financial sustainability in the NHS
24. On 23 July 2024, I published a report on NHS Financial Management and Sustainability, highlighting the unprecedented scale of challenges facing the NHS today and in the years ahead. I reported that the NHS’s financial position is worsening because of a combination of long-standing and recent issues, including failure to invest in the estate, inflationary pressures, and the cost of post-pandemic recovery. Many NHS bodies failed to break even in both 2022-23 and 2023-24.
25. The overall financial performance of the NHS England group, together with the NHS provider sector, will be reported in the DHSC annual report and accounts 2023-24, when it is published later this year. I will comment on this in my report on the DHSC annual report and accounts 2023-24.
Gareth Davies, Comptroller and Auditor General
National Audit Office, 157-197 Buckingham Palace Road, Victoria, London SW1W 9SP
7 October 2024