
1. Introduction
Executive summary
This guidance is designed to be used by those considering and involved in delivering service change to navigate effectively from initial planning through to implementation of decisions. Service change plays a vital role in addressing the current challenges the NHS faces. To be effective, this transformation needs to occur in compliance with the law and in a way which fosters public confidence. Doing so will help to ensure sustainable improvement to meet patients’ needs.
This guidance has been published by NHS England under section 14Z51 of the National Health Service Act 2006 (as amended by the Health and Care Act 2022) (referred to throughout as the NHS Act 2006). In particular, integrated care boards (ICBs) should have regard to this guidance in the exercise of their public involvement and consultation functions (for example, under section 14Z45 of the NHS Act 2006) and more generally when undertaking service change.
The guidance will also be relevant to NHS trusts, NHS foundation trusts and to NHS England itself, in the exercise of their functions which relate to service change (for example, NHS England’s public involvement and consultation functions under section 13Q and providers’ functions under section 242 of the NHS Act 2006 and/or under the NHS Standard Contract).
It should be noted that this guidance does not supersede the requirements set out in the law. Where there is any uncertainty about applying the law or guidance, individual organisations are recommended to seek legal advice as necessary. Where support from NHS England is required, the first contact should be with your NHS England regional service change representative; current contact details are available from the System and Service Reconfiguration page on the NHS Futures Collaboration Platform (registration required).
Who is this guidance for?
This guidance is for those leading, managing and delivering programmes that are considering or undertaking substantial service change. It will provide useful support whether the changes are considered substantial or not. It aims to support commissioners and their partners to take forward proposals and reach robust decisions on change. Doing this effectively will help drive reform and ensure NHS services meet patients’ needs, both now and in the future.
Integrated care boards (ICBs) need to follow this statutory guidance when working to involve and consult the public and more generally when undertaking service change.
It will also be helpful for all other partners involved with any phase of service change.
Key pointers for scheme programme directors
1. Read this guidance to get an overview of the process and the legislative framework. You may also find it useful to refer to the interactive handbook and support materials available on the System and service reconfiguration page on the NHS Futures Collaboration Platform (registration required).
2. Make contact with the relevant NHS England reconfiguration lead. Contact details are available on the System and service reconfiguration page.
3. Ensure that a clear case for change is being developed.
4. Consider if the change may be ‘substantial variation’, and what engagement with the OSC is required. If determined to be substantial then the scheme will need to notify the Secretary of State (see section in guidance below)
5. Ensure the governance for the programme is clear. In particular, it is important to understand who has the legal responsibility for the decision making and ensure any schemes of delegation that may be required are appropriately established.
Definition of key terms
Commissioner(s)
The term “commissioner” or “commissioners” refers to either ICBs or NHS England or both, depending on the circumstances.
Public
Where we refer to “the public” it should be taken to include current and potential service users and their carers and representatives (if any).
2. Overview and key themes
What is service change?
Broadly speaking, service change is any change to the provision of NHS services which involves a shift in the way front line health services are delivered. This may involve a change to the range of services available and/or the geographical location from which services are delivered. This could include accessibility, whether a change in venue or a shift from walk-in services to requiring pre-booking.
Service change, at times, can be tied to capital investment. For example, proposals to reconfigure services may also require redevelopment of estates to deliver the new service successfully.
“Service change” and “reconfiguration” are often used interchangeably. Service decommissioning can also be a type of service change.
For the purposes of understanding the ministerial intervention powers discussed below, ‘reconfiguration of NHS services’ means a change in the arrangements made by NHS England or an ICB for the provision of services provided as part of the health service in England, where that change has an impact on the manner in which a service is delivered to individuals (at the point when the service is received by users) or the range of health services available to individuals.
Substantial service changes
Some service changes are deemed “substantial” and this triggers certain legal duties. NHS England will assure substantial service changes.
The legislation does not define “substantial” service change. However, there are some customs, practices and precedents set. The courts have also considered the meaning of “substantial” in this context. When deciding if a service change is substantial, it’s generally accepted the following factors need to be considered:
- changes to the accessibility of the services
- the impact on the wider community and other services (including economic impacts)
- the number of patients affected
- the length of time of the impact of the service change
- changes to the method or setting of the service delivery (for example, a move from acute to community setting)
For example, a change of site from which services are delivered, with its consequent impact on patient and visitor travel times, could be a substantial change, even with no changes to the type of services provided. Decommissioning or significantly reducing the extent of the service(s) being provided could also be a substantial change.
Tendering a service by itself is unlikely to be a substantial change unless the new service specification will significantly change the service patients receive.
If it’s unclear whether a change is substantial, there should be discussion with the relevant health oversight scrutiny committee (HOSCs) (typically the HOSC where the service is currently located or the HOSC covering the majority of affected patients) and the NHS England region’s reconfiguration lead.
Duty to consult with the local authority
Under regulation 23 of the s 244 regulations, NHS bodies and health service providers must consult a local authority about any proposal they have “under consideration” for a substantial development or variation in health service provision in the authority’s area.
Where the provider of NHS services has such proposals under consideration, which relate to services commissioned by an ICB or NHS England, the relevant commissioner shall consult with the local authority on the provider’s behalf.
This duty is covered in more detail later in the guidance.
Duty to notify the Secretary of State
Where the duty to consult with the local authority under the section 244 regulations is triggered, the responsible commissioner must also notify the Secretary of State for Health and Social Care.
This process came into force on 31 January 2024. It’s outlined later in this guidance and the statutory guidance, Reconfiguring NHS services – ministerial intervention powers.
Public involvement and consultation
Involvement
The NHS Act 2006 and the NHS Standard Contract for providers outline the duties on NHS bodies to involve the public.
The statutory guidance on working with people and communities highlights the benefits of this approach. It also contains a set of underpinning principles and practical case studies.
NHS commissioners and providers are accountable and liable for compliance with their public involvement obligations. Involvement can be achieved by consulting people, providing people with information, or in other ways. Effective public involvement has many benefits, including helping secure buy-in for proposed changes and ultimately, better service design.
It is important to remember the duty is to involve the public and determine the most appropriate way to do that in the specific circumstances and proportionate to the change being proposed. That means you need to consider the range of involvement options and choose that which fits with the proposal under consideration. It is important to be clear that this is a decision for the relevant commissioner to make in determining how to meet their statutory duties. As a general rule, the greater the extent of the changes and number of people affected, the greater the level of public involvement that is likely necessary.
For example, a mature integrated care system (ICS), which involves the public in an effective, ongoing manner (and where potential issues, barriers and solutions have been developed in partnership), may be able to agree that service changes can proceed based on engagement rather than full public consultation. This decision should be in close discussions with the local authority, and evidence of the decision should be kept.
Commissioner discretion
The case of R (Hinsull) v NHS Dorset CCG [2018] EWHC 2331 and [2019] EWCA Civ 1412 highlights that commissioners have a wide discretion in making decisions regarding health services. It is important that consultation documents adequately explain the proposed changes to health services.
Defining consultation, engagement and communications
Many people use the terms “engagement”, “communications” and “consultation” interchangeably. Yet, in the context of this guidance, they have specific meanings and refer to different actions. These actions can also be facets of “involvement”.
Consultation
This term refers to a formal consideration of views from relevant stakeholders (normally patients and carers, local authorities, representative organisations and the public). The phrase is often associated with consultation with the public, which is the specific period during which the public is formally invited to comment on the plans for reconfiguration before a final decision is reached. A duty to consult may arise under specific statutory duties (such as public involvement duties) or under common law. Under common law, a duty to consult may also arise where there has been a promise to consult, where there has been an established practice of consultation, or, in exceptional cases, where it would be conspicuously unfair not to consult.
The term “consultation” is also used to refer to the requirement under regulation 23 of the Local Authority (Public Health, Health and Wellbeing Boards, and Health Scrutiny) Regulations 2013 (as amended) as detailed in annex 4.
Engagement
This term refers to the ongoing process of eliciting, discussing and understanding the views and experiences of relevant stakeholders, including members of the public, during all stages of the service change programme.
Communications
This term refers to a strategy for how issues and plans will be shared with stakeholders throughout the programme.
Temporary or urgent service changes or closures
Under regulation 23(2) of the section 244 Regulations, where the responsible NHS body is satisfied that a substantial service change decision needs to be taken without allowing time for consultation with the local authority because of a risk to safety or welfare of patients or staff, it may take that decision. In these circumstances it may not be possible, due to the urgency of the change needed, to undertake public involvement or consultation with the local authority in advance of the change being made.
The importance of meaningful public involvement, even where changes are temporary
In determining whether the arrangements for public involvement put in place by the trust were adequate, in the case of ‘R (on the application of Dawson) v United Lincolnshire Hospitals NHS Trust [2021] EWHC 928 (Admin)’, Mr Justice Linden held that: “…ultimately the question is whether the arrangements, looked at as a whole, have secured the opportunity for meaningful involvement or participation in the specified matters…”
The judge observed that the case “illustrates how failure to involve service users in decision-making will foster a sense of injustice or, worse still, undermine confidence in the good faith of the decision-maker.”
Where services need to be closed or suspended at short notice, NHS bodies and their partners should act in accordance with the Joint Working Protocol. In all cases, NHS bodies should adhere to their legal duties and good practice, including:
- keeping good records of the factors they consider in making these decisions
- communicating the changes to affected people
- immediately informing the local authorities in the areas affected about changes and reasons for not consulting them under the regulations
- undertaking as much public and stakeholder engagement as possible in the time available
The local authorities in the affected area(s) should be informed of the changes and the reasons for not consulting at the first opportunity. The relevant NHS bodies should provide a formal update to the HOSC. Where temporary service changes have been made, which might be considered ‘substantial’, the commissioner should also notify their local NHS England regional team.
If a provider is making a temporary service change, it must also ensure the ICB is informed. In turn, ICBs should make NHS England aware of changes as soon as possible.
Where temporary changes are made, a clear plan needs to be established to return the service in a timely manner when practical. Appropriate time scales for this will vary from case to case.
If there is a proposal to make a temporary change permanent or adopt an alternative configuration, which is considered a “substantial service change”, the full process in this guidance must be followed.
Assurance
Overview of NHS England’s assurance role
NHS England supports and assures the development of proposals by commissioners. NHS England regional teams can be a source of informal advice, check and challenge and provide links to best practice.
Reconfigurations that result in substantial changes to services directly commissioned by NHS England also require assurance. NHS England will be mindful of both potential conflicts of interest and the perception of such conflicts when assuring service change proposals. When determining the extent of assurance required, NHS England will, where applicable, consider the same factors as a system-led proposal.
Regional clinical senates
Regional clinical senates are independent, non-statutory advisory bodies that bring together clinicians, patients and other partners. They are often best placed to provide independent review and advice about all stages of service change programmes.
It’s recommended that commissioners considering service changes contact the appropriate regional clinical senate as early as possible so they can give timely support.
Clinical senates will review the clinical case for change and proposed models of care of a service change’s pre-consultation business case (PCBC). They may also use patient and public involvement forums.
The senate formal review mechanism can help commissioners ensure plans are built on the best possible clinical evidence while providing assurance to themselves and their regulators.
Clinical senate reviews can help identify:
- whether the most relevant and up-to-date clinical standards have been used to underpin the development of any new models of care
- if robust and adequate consideration has been given to the clinical interdependency of services
- the appropriate assessment of risks and mitigations associated with the service change proposals
Additional clinical development support may be available from a senate to support proposal design. In these cases clinical senates have conflict of interest policies to ensure the support and review roles remains distinct and robust.
Assurance process
NHS England’s assurance process supports commissioners to develop lawful change proposals and public involvement processes that can enjoy widespread support while mitigating the risk of a successful challenge.
Decisions about the extent of assurance required will be made based on the scale and complexity of the service change proposals under consideration.
Indicative risk considerations
Low risk
- individual service or site change
- low complexity and limited risk of facing challenges
- potential for an engagement approach
Medium risk
- service change at a single provider level (though it may include multiple sites)
- likely to require formal public consultation
- some political or public campaign interest
- single or moderate HOSC involvement
High risk
- service changes across multiple providers or sites
- joint HOSC arrangements in place
- high level of political and public interest
- formal public consultation is required
- increased risk of formal challenge
Effective assurance is required to secure consistency and reduce risk in respect of:
- compliance with legal duties
- the key tests that should underpin service change proposals
- the strength of pre-consultation business cases, clinical evidence, public involvement and co-creation
- proposals taking into account relevant national guidance, such as from the National Institute for Health and Care Excellence (NICE) and Getting It Right First Time (GIRFT)
- the strategic coherence of proposals, including their whole system impact
- the programme management that underpins the planning and delivery of schemes
- whether the proposal can realistically be delivered and is affordable in capital and revenue terms
In addition to providing advice and support to programmes, NHS England operates 2 formal assurance checks during stages 1 and 2 of the process (detailed below). NHS England may also seek further assurance at the decision-making business case stage (stage 3). NHS England will decide whether this is required on a case-by-case basis.
Adequate time should be included in programme plans for each part of the assurance process to minimise delays and factor in planning for assurance meetings (where required).
Building in periods of pause following an assurance checkpoint and post consultation is advisable. This will give time to address any queries or undertake any additional work that may be required to provide confidence in proposals.
Stage 1 – Strategic sense check
The strategic sense check should occur early in a programme lifecycle. Engagement with key stakeholders should have commenced, and if capital is likely to be required, discussions with the relevant ICB capital and NHS England finance teams should have begun. This will determine the extent of pre-consultation assurance required and the level at which assurance decision-making will take place within NHS England.
The advice of specialised commissioning colleagues should be sought where appropriate to ensure that any impact on specialist services commissioned by NHS England or ICBs is properly considered.
Certain specialised commissioning functions are currently delegated to ICBs. Regardless of this delegation, NHS England will remain the accountable commissioner for the entire portfolio of specialised services and maintain responsibility for setting consistent national standards, service specifications and clinical access policies.
Engagement with regional clinical senates at stage 1 will help them provide the appropriate support. This early contact will allow programmes adequate time to consider and respond to the independent clinical advice received as part of the process. Engagement with senates (and in dialogue with the appropriate regional reconfiguration lead in the NHS England regional team) will also help the programme determine if and when alternative forms of independent clinical advice may be more suitable (for example, clinical networks, Royal Colleges, etc).
In most cases, NHS England will capture the outputs of a strategic sense check in a letter to the chief executive of the lead ICB or other relevant commissioners.
Stage 2 – Assurance checkpoint
The stage 2 assurance checkpoint takes place before any formal public consultation and, therefore, before a decision to proceed with any particular options.
Previous decisions about the required extent of assurance will be reviewed. An NHS England assurance panel will be established, which will consist of suitable members. Any conflict or potential conflict of interest will be declared and appropriately managed.
This stage will assess support for the proposals from providers and other systems significantly impacted by them. Where relevant, letters of support will be required as part of the assurance evidence. Regional NHS England teams can advise where and when these are required.
For substantial or contentious service change, it’s best practice to seek the regional clinical senate’s advice on proposals (the need for which will usually have been identified at stage 1) before this assurance checkpoint. An independent senate review ahead of stage 2 will provide ICBs and other commissioners with:
- an assessment of the underpinning clinical evidence base
- strengths and weaknesses of the clinical models within each service change.
This independent assessment can improve the final range of options for public consultation while also enabling systems to contribute evidence to the assurance process against the 5 tests for service change. In particular, the senate’s independent assessment process can contribute to the tests of clear clinical evidence base and the bed capacity test.
Before public consultation is launched, proposals should be tested to ensure a high degree of confidence that all options could be delivered as proposed and do not imply an unsustainable level of capital expenditure or revenue funding. Service change schemes which require capital financing above delegated limits will need the written support of NHS England before public consultation begins.
In most cases, NHS England will capture the output of the stage 2 assurance checkpoint in a letter to the chief executive of the lead ICB or other relevant commissioners.
Stage 3 – Pre-decision making
A final assurance check may be undertaken before the commissioner makes a decision in any of the following situations:
- there are outstanding queries requiring resolution from the stage 2 checkpoint
- the proposals have changed significantly from those originally assured as a result of the consultation feedback
- there is a need to ensure that the consultation process itself (and the assessment of its findings) was carried out in line with the test of strong public and patient engagement (detailed below).
Clinical senate input into the service change process may also be appropriate at the post-consultation stage before decisions are made. Senate input can be useful when:
- new ideas or variations on proposed clinical models are submitted as part of the public consultation – commissioners can ask senates to review these suggestions in line with any independent clinical assessment before the stage 2 checkpoint, enabling decision-makers to evaluate all options equally and robustly
- there were outstanding issues that need re-visiting (either from a previous senate review before the stage 2 or from NHS England as part of the assurance checkpoint)
National versus regional decision-making criteria
For most proposals, NHS England’s assurance of service change is undertaken at a regional level. However, for some proposals, assurance and decision-making will be undertaken by the relevant NHS England national committee or board, or the NHS England Chief Financial Officer (CFO). This depends on the value of related capital proposals and the relevant segmentation of the provider or its ICB under the NHS Oversight Framework. The relevant thresholds are set out in annex 5.
In some circumstances, assurance and decision-making may be carried out by a different regional team or at a national level to ensure no actual or perceived conflicts of interest.
5 tests for service change
NHS England uses 5 tests to assure service change. These tests are significant at the stage 2 assurance checkpoint.
The 5 tests (4 plus the “bed test”) are:
1. strong public and patient engagement (see guidance on working with people and communities)
2. consistency with current and prospective need for patient choice
3. clear, clinical evidence base
4. support for proposals from clinical commissioners
5. for any proposal, including plans to significantly reduce hospital bed numbers, commissioners need to evidence that they can meet at least 1 of the following 3 conditions:
- demonstrate that sufficient alternative provision, such as increased GP or community services, is being put in place alongside or ahead of bed closures and that the new workforce will be there to deliver it
- show that specific new treatments or therapies, such as new anti-coagulation drugs used to treat strokes, will reduce specific categories of admissions
- demonstrate a credible plan to improve performance without affecting patient care where a hospital has less efficient bed use than the national average (for example, in line with the Getting it Right First Time programme).
These tests provide a broad framework. In seeking assurance of service change proposals, NHS England may also seek to apply a range of good practice checks (see annex 2).
Systems should self-assess against these good practice checks alongside their statutory duties. This should be done throughout the development of their proposals and, in particular, before the stage 1 strategic sense check and stage 2 assurance.
Governance and system alignment
Service change schemes must:
- make clear which public body has the legal powers to make decisions, and put in place governance arrangements to reflect this
- ensure alignment with relevant national and system plans.
Clear decision maker
Good governance and effective public decision-making are critical to service change programmes. Programmes must be clear who the decision-makers are and how they will conduct public consultation and make post-consultation decisions. These arrangements should be clearly stated and referenced in consultation documents. It is vital the public are clear how and by whom decisions will be made.
In some cases, place-based partnerships or provider collaboratives may support or lead aspects of service change proposals. Any decisions by these organisations must be made only where permitted by properly established governance, including falling within the terms of a clearly specified scheme of delegation.
For further information about joint decision-making and delegation of functions to other organisations, as well as restrictions on delegation, see the statutory guidance on arrangements for delegation and joint exercise of statutory functions.
Even where responsibility for aspects of a service change programme is delegated or jointly managed in accordance with properly established governance arrangements, the organisation with the legal duty remains ultimately accountable. In most cases, this is the commissioner of the service, even if the provider is closely involved in developing proposals and supporting engagement. The organisation would also need to assure itself that its duties around public involvement (or consultation where appropriate) are properly complied with.
Multiple commissioners may be involved in service change proposals. For example, if a proposal impacts patient flow in a neighbouring provider or services are being joined up across several commissioning footprints. In this instance, the primary commissioner should engage with all affected commissioners. Where consultation with the local authority is required, the commissioners can do so jointly, or 1 or more commissioners can do so on behalf of others.
Commissioners are under a duty to consider relevant integrated care strategies, joint strategic needs assessments (JSNAs) and joint local health and wellbeing strategies (JLHWSs). Commissioners should consider recording how the duty to consider these key strategies and assessments was fulfilled during the decision-making process.
Engagement and communications
The planning and development of service change proposals are rarely linear.
The most successful proposals ensure that engagement with the local population and key stakeholders starts early, is well planned, strategic, inclusive and forms part of an ongoing discussion.
The local population and key stakeholders should be involved from the very beginning and throughout the process.
Importance of engagement and communications
Systems should be clear on whether they are consulting or engaging and ensure the language reflects the activity. Where public consultation is also required, prior engagement can ensure the proposals are based on firm evidence gathered from the public.
Whether or not they require formal public consultation, all service change programmes should be able to demonstrate meaningful and continuous engagement, which is proportionate to the proposals under consideration.
Deciding on options for public consultation
In the case of ‘R (Nettleship) v NHS South Tyneside [2020] EWCA Civ 46’ the Court of Appeal considered the nature of the public involvement duty. The court judged that the duty did not make it necessary to consult on options which the clinical commissioning groups deemed to be unviable, unrealistic or unsustainable.
The commissioner was only required to consult on genuine proposals for change.
NHS bodies must consider their duty to tackle health inequalities when planning and delivering service change communications. The NHS England commissioned guide to communications and engagement for people working in areas of deprivation can support this.
Stakeholder partnerships
It’s critical to engage stakeholder partners throughout the service change process. This work will include engaging with communities potentially affected by change proposals, as well as the partners that can support dialogue with them.
When setting up governance for a service change programme, programme leads should think about how stakeholders beyond NHS partners will be represented, for example, in reference groups or on decision-making bodies. This approach will support inclusion and bring the benefit of diverse perspectives.
The importance of partnership working
The Independent Reconfiguration Panel (IRP) advice in the matter of ‘Teignmouth Hospital, Devon (IRP advice to Secretary of State December 2021)’ demonstrates how challenging it can be to develop proposals for service change in a fast-moving situation such as the COVID-19 pandemic.
Health and care systems must adapt and learn from this experience. The advice highlights the importance of commissioners working with stakeholders to inform their proposals.
Engagement and communications planning
Service change engagement plans should:
- connect to existing relationships, engagement and strategies already taking place in the area
- be designed and tested with partners and draw on existing guidance (such as the NHS England working in partnership with people and communities guidance)
- be supported by appropriate resources
- be clearly connected to governance milestones for the change programme, allowing engagement insights to inform key decisions and ensure capacity is available when needed
An accurate, up-to-date record of engagement must be maintained and documented in communications and engagement plans and activities. This record must include the insight and feedback gathered at all stages, from defining the case for change to decision-making after formal public consultation. This supports the programme to respond to scrutiny of its processes in the event of challenges. A lack of this evidence is often cited in judicial reviews.
While it is sensible to refine options, programme teams should understand the drawbacks of ruling out options which may be helpful in undertaking subsequent wider stakeholder and public feedback.
While engagement with residents and other stakeholders should occur throughout the programme, public consultation is a specific formal stage when options are formally shared with local people.
Key legal duties
Annex 4 sets out key legal duties which are relevant to service change.
The key legal duties discussed in this section are areas where schemes must be particularly mindful, either because they frequently give rise to grounds for challenge or they are new.
Health inequalities and equalities
Reducing healthcare inequalities is an NHS priority, and tackling inequalities in outcomes, experience and access is one of the four key purposes of ICSs.
Commissioners must pay due regard to the duties placed on them under the Equality Act 2010 regarding the Public Sector Equality Duty (PSED), the duty to reduce health inequalities, and duties under the NHS Act 2006 at all stages of the service change process.
Service design and communications should be appropriate and accessible to meet the needs of diverse communities.
NHS England has published guidance for commissioners on equality and health inequalities legal duties. There is further guidance from the Office for Equality and Opportunity.
The complexity of decision-making involves balancing competing duties
In ‘R (A and Keppel) v South Kent Coast CCG [2020] EWHC 372 (Admin)’, the Court emphasised that health inequalities duties do not “oust other duties.”
Commissioners have different competing statutory duties to comply with; these relate to a wide range of factors, reflecting the complexity of decision-making in an advanced healthcare system. Commissioners have to exercise substantial discretion and judgment in what are multi-factorial decisions.
Systems need to understand how current provision and potential options may impact groups that experience poorer health outcomes, particularly those in Core20PLUS population groups. Service change programmes will need to complete an impact assessment, taking account of a number of impacts, including equalities.
Mitigating actions should be developed and reviewed to avoid widening health inequalities in access, experience and outcomes as a result of any service changes. This requires involving current or potential service users, along with their carers and representatives, in issues relating to health service access.
NHS bodies should collect, analyse and publish information relating to inequalities in line with NHS England’s statement on information on health inequalities. Any service change proposals involving a shift to digital channels should also consider the impact of digital exclusion on certain population groups and implement the framework for NHS action on digital inclusion.
Triple Aim
Commissioners, NHS trusts and foundation trusts are all under a duty to have regard to the wider effect of decisions (the Triple Aim). Annex 4 sets out the detail of this obligation.
Environmental sustainability
The NHS is committed to reaching net zero in response to the profound and growing threat to heath posed by climate change. Commissioners and providers are each under legal duties to consider and mitigate the impact of climate change in their operations (outlined in annex 4).
In accordance with the NHS Act 2006 (as amended by the Health and Care Act 2022) NHS England, ICBs, NHS trusts, and NHS foundation trusts must have regard to the need to:
- contribute towards compliance with section 1 of the Climate Change Act 2008 (UK net zero emissions target) and section 5 of the Environment Act 2021 (environmental targets)
- adapt to any current or predicted impacts of climate change identified in the most recent report under section 56 of the Climate Change Act 2008.
Delivering a Net Zero NHS report provides statutory guidance about the NHS’s net zero targets. Commissioners and providers should consistently look for ways to contribute to these targets – and to the actions and targets outlined in local trust and ICB green plans – when planning and delivering service change.
Local government
Strong relationships with local authority colleagues are crucial to the successful delivery of effective service change.
Responsibilities and structures
Health oversight scrutiny committees
Health oversight scrutiny committees (HOSCs) exercise the statutory responsibility to scrutinise health and social care services provision in their areas.
The scrutiny role of HOSCs does not detract from local authorities fulfilling their other roles as health and care commissioners and core partners in the integrated care system.
Integrated care partnerships (ICPs)
ICPs are statutory committees jointly formed between the ICB and all upper-tier local authorities within the ICS area. The ICP brings together a broad alliance of partners and is responsible for producing an integrated care strategy for the population in the ICS area.
Plans for changing services should align with the ambitions in system strategic plans, including the integrated care strategy.
DHSC has published principles that set out the expectations around how ICBs, ICPs and HOSCs should work together.
Health and wellbeing boards
Health and wellbeing boards are a formal statutory committee of the local authority and can provide invaluable insights that complement broader discussions. The extent of their involvement depends on local circumstances and how much they’ve been involved in the past.
Plans for service change should align with health and wellbeing boards’ joint strategic needs assessments and joint local health and wellbeing strategies for the area.
Role of local authority health scrutiny
Generally, systems should discuss their proposals with local stakeholders before deciding on a preferred engagement or consultation approach. It will often be appropriate to discuss proposals with:
- regional service change and reconfiguration leads
- ICS leads
- local authorities (for example, the Health and Wellbeing Board)
- local MPs
- affected patient groups
- clinicians and staff
- the public
Broad discussion ensures stakeholders have a shared understanding of the case for change. It also avoids proposals being developed in isolation and makes sure the wider health system and local population health management approach is considered. Discussions should continue throughout the life of the proposal.
Local authorities also have powers and responsibilities relating to the wider determinants of health, such as housing, transport, employment and education, so engagement and collaboration can prove exceptionally beneficial in helping to frame the service change around a population health management approach.
Local authorities have various stages of scrutiny, from informal sessions to borough-based committees, HOSCs and joint HOSCs. Establishing early communication is vital.
Health colleagues should be aware that local elections, pre-election periods, the configuration of the local authority (for example, whether unitary or district) and its constitutional and governance requirements all impact on the efficient and effective scrutiny of health services in a local system. Considering these factors, and any potential implications of the proposed service change, can benefit working relationships.
Consulting with the local authority in practice
Where an NHS body consults a local authority on a proposal under the section 244 NHS Act then the regulations issued under that section, The Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) Regulations 2013 (the Regulations), apply. Case law has established that the NHS body should state it’s consulting under those regulations and give the local authority 2 dates:
- the date by which the NHS body requires the local authority to provide any comments on the proposal
- the proposed date by which the NHS body intends to decide whether to proceed with the proposal
The NHS body must publish these dates and any changes to them, for example as part of ICB board meeting arrangements. It is often appropriate to have a dedicated webpage where key information such as this can be published. It is also important to make sure these dates are shared with the clerk of the HOSC/JHOSC.
In summary, the regulations give local authorities statutory powers to:
- require the relevant NHS body to provide information on matters it’s scrutinising
- require members or employees of the relevant NHS body to attend and answer questions in connection with the matters it is scrutinising
- respond to the consultation and make recommendations the NHS body must consider and respond to.
Where substantial change proposals affect more than one local authority area, the affected local authorities must form a joint committee to be consulted. Where a joint HOSC is required to be formed, only the joint committee may discharge these powers. NHS bodies will have to consider these arrangements early in their planning.
Where NHS bodies and local authorities disagree on the recommendations in response to a change proposal consultation, both parties share a statutory duty to seek an agreement. The local authority and commissioner should involve the relevant provider(s) during this process. NHS England regional teams can be called upon to help support this.
Where plans change or have the potential to change, NHS bodies must still consider legal duties to consult local authorities and whether there is a need to consult further or again. The relevant NHS England regional team should be involved in this discussion.
Consulting local authorities after a significant proposal change
In the case of ‘Regina v North West Thames Regional Health Authority and Others, ex parte Daniels (Rhys William)’, QBD 18 June 1993, although an initial consultation with the council had been held about the transfer of a service from one hospital to another, the court considered a failure to consult again when the proposals significantly changed was unlawful.
Fairness and the need to re-consult
In the case of ‘R(Smith) v East Kent Hospital NHS Trust [2002] EWHC 2640’, the court considered the test for whether consultation is required when proposals change.
Mr Justice Silber set out the approach as follows: “The concept of fairness should determine whether there is a need to re-consult … This means that there should only be re-consultation if there is a fundamental difference between the proposals [already] consulted on and those which the consulting party subsequently wishes to adopt.”
If local authorities are concerned about the approach taken by the NHS bodies or the nature of proposals for service change, they may write to the Secretary of State requesting that the service change be “called in” (as detailed in the statutory guidance). However, DHSC expect such call-in requests only to be used in exceptional situations where local resolution cannot be reached.
Statutory guidance expects NHS commissioning bodies to take a “local solutions first” approach, and for everyone involved to take all reasonable steps to try to resolve issues concerning local proposals.
NHS bodies in England may proceed to make urgent temporary changes to services without consulting local authorities only as detailed in the temporary and urgent service change or closure section of this guidance.
Consideration of when local authority consultation is needed for substantial variation of health services
The case of ‘R (Juttla) v Herts Valley CCG [2018] EHC 267 (Admin)’ highlights the need to look carefully at the nature of the services in question and whether they amount to a substantial variation of health services requiring formal consultation with the local authority.
In this case, the court quashed the clinical commissioning group’s decision to withdraw the funding of the services and required “the regulation 23 path” to be followed.
Interventions by the Secretary of State and the role of the Independent Reconfiguration Panel
Legal framework
DHSC has issued statutory guidance detailing how the Secretary of State’s intervention powers relating to service change will be exercised, and this should be read alongside this guidance for a full understanding of the process.
It highlights a new Secretary of State “call-in” power to intervene in NHS reconfigurations while placing duties on NHS commissioning bodies to notify substantial reconfigurations and for NHS commissioning bodies and NHS trusts and foundation trusts to provide ministers with information and assistance.
Notifying the Secretary of State in practice
NHS commissioning bodies must notify the Secretary of State when proposing a ‘notifiable’ reconfiguration, as detailed in the statutory guidance.
‘Notifiable reconfigurations’ are defined by the National Health Service (Notifiable Reconfigurations and Transitional Provision) Regulations 2024. A reconfiguration is notifiable when it would trigger a consultation with the local authority under regulation 23(1)(a) of the 2013 regulations.
Making a notification to DHSC is the responsibility of the NHS commissioning body which has a substantial change or variation in NHS services under consideration. However, the NHS commissioning body should consider the HOSC’s views on a proposal when deciding whether to notify. They should make clear to the Secretary of State the HOSC’s view of whether the reconfiguration is notifiable. In most cases, this stage will likely occur after the case for change has been developed.
ICBs and providers should work closely with the lead from the relevant NHS England regional team where a proposed service change may be substantial and, therefore, notifiable. NHS England expects this contact to be made prior to notification being submitted.
The NHS England regional reconfiguration lead can support the NHS commissioning body to complete the notification form, ensuring it is submitted at the appropriate point by someone with the appropriate authority.
If the scheme spans multiple ICBs and providers, they should confirm that the notification is made jointly on their behalf.
Certain types of changes do not need to be notified:
- temporary changes made in urgent circumstances in accordance with the Joint Working Protocol
- schemes that are not deemed to be substantial by the NHS commissioner and not requiring consultation with the (J)HOSC
- transactions (which would not be within the scope of the call in power unless the transaction itself resulted in a service reconfiguration).
If a decision is subsequently proposed to make a temporary change permanent or adopt an alternative configuration, where it is considered a ‘substantial service change’, the full process set out in this guidance must be followed. The proposals for change would then require consultation with the HOSC and notification to the Secretary of State.
There is no requirement to pause or amend planned programme activities following the submission of a notification (unless and until a direction by the Secretary of State calling in the proposal is given). If DHSC requires further information following the submission of a notification, programmes should work with NHS England (through the relevant regional reconfiguration lead) and DHSC as required.
Duties to provide information or other assistance
DHSC may require further information on all schemes whether or not they’ve been notified. In practice, there is likely to be an information gathering phase prior to any formal decision to call in a reconfiguration. Both before and during any call in, affected ICBs and providers should be prepared to share information concerning the service change process to date and liaise with NHS England, DHSC and the Independent Reconfiguration Panel (IRP) as appropriate.
Role of the Independent Reconfiguration Panel
The Independent Reconfiguration Panel (IRP) provides expert advice about reconfigurations or significant service change within the NHS in England. The IRP can provide:
- informal advice to determine if a call-in request is appropriate
- support to resolve issues with a proposal locally
- independent advice to help the Secretary of State determine whether to use the call in power
- formal support to the Secretary of State when they have chosen to use their call in power
Systems and schemes should co-operate with the IRP and provide requested information in the given timeframes.
The IRP has also prepared various resources which can support schemes to deliver change effectively. This includes the series of papers Learning from reviews. They identify 6 reasons for success which can reduce likelihood of challenge:
1. The local community is involved from the first stage of considering change.
2. The relevant local authorities affected by the changes are actively engaged throughout the process.
3. The proposals set out a clear vision for joined-up and person-centred health and care with a credible clinical case for change.
4. The planned use of resources is sustainable to maximise the benefits for patients.
5. The proposals address the need to reduce inequalities in health and healthcare.
6. The proposals clearly address any trade-offs and how the risks will be mitigated, including the impact on travel and transport.
Schemes should keep these factors in mind and periodically self-assess against them.
Ability to progress when a reconfiguration has been called in by the Secretary of State
When the Secretary of State has called in a scheme, there are restrictions on what actions can be taken. The legislation states that once a proposal is called in, the commissioning body must stop all actions related to it. They can only proceed to such extent (if any) as allowed by the direction letter issued by the Secretary of State.
Please read the statutory guidance for full information about the direction letter, and the type of actions that may be allowed and the expectations around NHS commissioning bodies’ legal duties to consult the HOSC during a live call in. Where certain actions are permissible under the direction letter, the system will need to decide whether these should take place/be continued or whether it would be preferable to wait until the Secretary of State has reached a decision on the proposal.
Judicial reviews
What can happen if NHS bodies fail to discharge their legal duties?
NHS bodies must act within their powers and in accordance with the law as it applies to them. The legal requirements are designed to make sure NHS bodies take all relevant factors into account in decisions to commission and provide the best services possible.
Anyone with a proper interest may bring a claim for judicial review if they consider that the NHS body has failed to act in accordance with the law. Judicial review can be an expensive and time-consuming process. It’s therefore important not to rush through the development of proposals. Instead, NHS bodies should invest sufficient time and resources to reduce the risk of successful legal challenges.
There are generally 3 grounds on which a challenge can be brought:
- the decision-maker did not have the requisite legal power to make the decision in question
- the decision-maker did not follow a proper, fair and lawful process, that is there is some form of procedural impropriety, in making the decision
- the decision is irrational (sometimes called Wednesbury unreasonable), that it’s so unreasonable that no reasonable person acting reasonably could have made it
The court is not generally interested in the merits or otherwise of the proposed service change. Instead, it concerns itself mainly with legality and process. Hence diligence in ensuring that the decision-making processes comply with legal duties (including that they are fair) is the best strategy for protecting against successful judicial review claims. Most judicial review challenges that are brought against service change decisions relate to a challenge to the process, including a failure to properly exercise or give due regard to a statutory duty.
The possibility of a challenge on the grounds that the body did not have the required legal power to make that decision is why it’s important to clearly establish who the decision-maker is in each case.
Capital
Both service change and capital business cases are designed to support effective decision-making to determine a preferred way forward. Yet, it’s also helpful to understand the important differences between them.
Service change business cases
The core purpose of pre-consultation business cases (PCBC) and decision-making business cases (DMBC) is to use a range of inputs to determine which options are viable and should be pursued to address the issues identified in the case for change. Service change business cases demonstrate the process that has been followed to identify the options and the engagement that has been undertaken; and present options for consultation which are demonstrably deliverable for the NHS in clinical, financial, activity and workforce terms. Service change business cases often contain value-for-money assessments of different options as one of many factors considered.
Service change business cases are typically owned by the ICB and take a system view.
Capital business cases
These business cases are prepared in line with NHS England’s Capital guidance. While capital business cases are also concerned with the appropriateness and deliverability of options, their core function is to ensure that the proposed investment constitutes the best possible value for money to society.
The submission of capital business cases in the standardised format required by the HM Treasury Green Book allows government to compare the expected benefits of investment across all sectors of the economy.
Capital business cases require a detailed cost-benefit analysis to be carried out and net present social value (NPSV) of options to be calculated. This must include a ‘business as usual’ and a ‘do minimum’ option as counterfactuals for the economic evaluation, even if these options are not judged to be feasible (and should not therefore be expressed as viable options for the purpose of the PCBC).
Capital business cases are often owned and submitted by provider organisations, as funding may be linked to the redevelopment of specific parts of their estate.
The capital business case requirements
If capital is required above delegated limits, processes in the Capital guidance must be followed. Centrally funded projects (including those below delegated limits) may be subject to a different approval process. Any queries regarding any centrally funded projects should be raised with the relevant NHS England regional team or NHS England Capital and Cash team.
The capital business case process is a 3-stage approval process.
1. Strategic outline case (SOC)
SOCs are required in cases where the value of the investment exceeds the limit given in the Capital guidance. It documents the strategic case for investment, builds on the decision-making business case and further details the preferred way forward and necessary comparator options. The SOC provides information to NHS England, DHSC and, where appropriate, HM Treasury to decide whether they can approve the project to move to the next stage. You should check the Capital guidance to understand if a SOC is required for your scheme.
2. Outline business case (OBC)
The OBC sets out a more detailed economic and financial appraisal of the options and is aimed at determining 1 or more preferred options for capital investment. Approval of the OBC means the project can start procurement and secure a preferred bidder to deliver the capital project.
3. Full business case (FBC)
The FBC sets out the commercial and contractual arrangements for the negotiated deal (that is confirming the deal is affordable) and the detailed management arrangements for delivery, monitoring and evaluation. Approval of the FBC enables the capital project to proceed to contract signature and start delivery.
The parties that will review these cases are detailed in the Capital guidance and depend on the value of the scheme, applicable delegated limits, and whether the scheme or the financing arrangements are novel, contentious or repercussive.
Timing of public consultation for substantial service changes requiring capital
For substantial service changes that require capital funding, there must be clear and early confidence that any proposal is affordable in capital and revenue terms ahead of any public consultation.
Where options require capital funding above delegated limits, consultation must not be launched without either:
- confirmation that the capital required is affordable within ICS capital envelopes
- agreement in principle that capital funding and capital departmental expenditure limit cover is available
Before a decision-making business case, schemes can develop drafts of their capital business cases and seek feedback from regional teams. However, NHS England and DHSC will not formally consider capital business cases until the service change business case process has concluded, as the capital investment process cannot pre-empt the outcome of public consultation.
Similarly, the options in the pre-consultation business case and conclusions of the decision-making business case should avoid pre-judging the strategic outline case, outline business case or full business case outcome.
Alignment of capital business cases with service change business cases
Those developing service change schemes with associated capital investment can save time during the capital approval process by aligning the service change business cases (PCBC and DMBC) and the capital strategic outline case (SOC).
The case for change should feed into the PCBC, the DMBC and the capital business cases. Although for different purposes and audiences, similar evidence is needed.
For service changes that require capital investment, the PCBC and DMBC should be considered starting points for the SOC (or OBC, if SOC is not required).
Where schemes require capital funding below delegated limits, or are self-funded and the expenditure will not result in a breach of the ICS’s capital departmental expenditure limit, it’s good practice for the PCBC and DMBC to meet the SOC requirements outlined in the HM Treasury Green Book.
In all other schemes requiring capital funding, the PCBC and DMBC must form the basis of the SOC. In these cases, the relevant SOC guidance should be applied when creating the service change business cases.
As schemes should only consult on viable options, this should be reflected in the PCBC. The SOC has slightly different requirements, so the options listed may vary between the 2 documents.
For a Treasury-compliant SOC and outline business case, options should include ‘business as usual’, ‘do minimum’ and 2 others. Developing financial scenarios for ‘business as usual’ and ‘do minimum’ at the PCBC stage is recommended, even if these options may not be included in the public consultation. Doing so will help to mitigate the risk that modelling changes significantly at SOC stage. The ‘business as usual’ option should be the baseline for any ‘value for money’ analysis.
Annex 1 sets out how the SOC requirements, as outlined in the Capital guidance, can be aligned with service change business case requirements. These criteria are not a checklist or a suggested structure, but rather a guideline for what to consider/include. Your NHS England regional reconfiguration leads will be able to advise on ensuring your PCBC is proportionate to your scheme.
Figure 1: Illustrative alignment of service change proposal process and capital proposal process
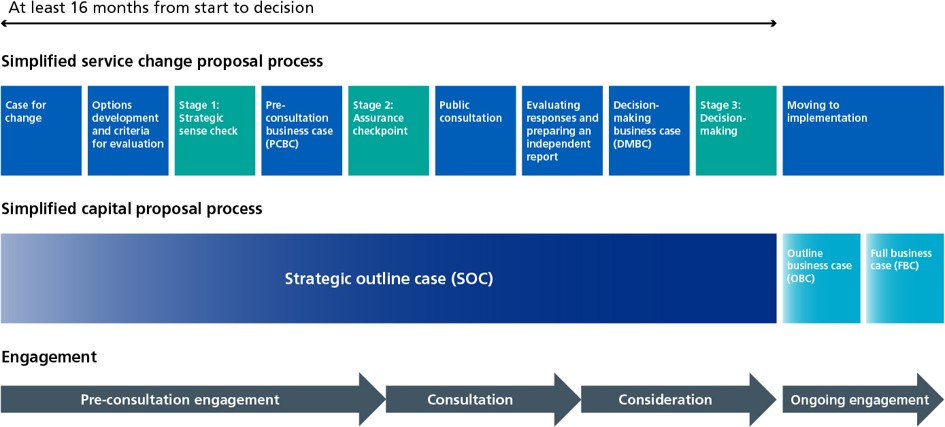
Figure 1 shows 3 horizontal rows indicating how timelines for service change proposals, capital proposals and engagement align and feed into each other. The timeline spans at least 16 months from start to decision.
The top row shows the simplified service change proposal process with the following steps in sequence:
1. case for change
2. options development and criteria for evaluation
3. stage 1: strategic sense check
4. pre-consultation business case (PCBC)
5. stage 2: assurance checkpoint
6. public consultation
7. evaluating responses and preparing an independent report
8. decision-making business case (DMBC)
9. stage 3: decision-making
10. moving to implementation
The second row represents the simplified capital proposal process, which includes:
1. strategic outline case (SOC), which aligns with steps 1 to 9 of the simplified service change proposal process
2. outline business case (OBC), which aligns with the first half of step 10 of the simplified service change proposal process
3. full business case (FBC), which also aligns with the second half of step 10 of the simplified service change proposal process
The final row highlights phases of engagement, displayed as arrows:
1. pre-consultation engagement, which aligns with steps 1 to 5 of the simplified service change proposal process
2. consultation, which aligns with steps 6 and 7
3. consideration, which aligns with steps 8 and part of step 9 of the simplified service change proposal process
4. ongoing engagement, which aligns with part of step 9 and step 10 of the simplified service change proposal process
3. Process
The service change process is designed to support the smooth successful delivery of improvements.
Not all service change schemes must carry out all the detailed stages to the same extent. In particular, some schemes may not require assurance at stage 2.
NHS bodies considering service change should engage as soon as possible with the relevant NHS England regional reconfiguration leads who will be able to offer guidance on the process. Various resources are available to support service change, including best practice examples, case studies and an interactive handbook on the System and service reconfiguration page on the NHS Futures Collaboration Platform (registration required).
Pre-consultation service change stages
Case for change
The case for change is the first key document for a service reconfiguration programme. It introduces the reasons for making a service change, including comprehensively describing the population’s current and future needs, service provision, and the key challenges facing the health and care system.
It provides the platform for change and needs to present a compelling picture of what needs to change and why. However, it does not include firm proposals for future service change. Instead, it makes an argument for why change is needed, without suggesting which specific changes are required.
The NHS England regional team will consider the case for change as part of the strategic sense check, which will determine the level for the next stages of assurance and decision-making.
What needs to be demonstrated in the case for change?
The case for change needs to demonstrate:
- a vision which is aligned with local and national strategic plans and recognises local and national drivers of change
- a clear clinical evidence base, which includes detailed analysis of the performance of local services
- a narrative about the benefits that change aims to deliver
- a plan for how to engage with stakeholders
- a review of financial considerations and other key dependencies, such as workforce, estate and digital
Commissioners should oversee the development of the clinical case for change. The clinical evidence base may include:
- consideration of patient health needs (including health inequalities) and quality improvements required
- latest national, regional and international clinical evidence and clinical standards, including benchmarking data
- local service data (such as patient flows, service utilisation, clinical outcomes and staffing levels)
- qualitative insights from clinical leaders and clinicians from the services affected – it is important that even where changes are focused on 1 area of a pathway or service, input from clinicians across primary and secondary care is appropriately sought
Although schemes should ensure finances are not the only driver for change, the financial implications of the proposed change should be laid out.
Early planning should also consider patient health needs, health inequalities, net zero targets and quality improvements.
Proposals should also consider required capital investment, estate strategies and the 5 tests for service change.
It’s important to discuss with NHS England at an early stage. This is particularly important where trusts need to access capital to deliver options that may be consulted on. Any schemes that require capital investment will need agreement in principle before they can move to public consultation.
Options development and appraisal
The options appraisal process is a systematic way to help decide between different options. It will help identify a preferred way forward to address the issues in the case for change.
For schemes that will receive stage 2 assurance, the process followed to develop and appraise options will be considered as part of the assurance exercise. The process must, therefore, be designed so that the preferred way forward addresses the issues in the case for change. It must also differentiate between options.
What needs to be demonstrated?
Commissioners and providers have a statutory duty to involve service users in the development of service change proposals. This involvement should not be a single standalone exercise but an ongoing dialogue throughout the development of plans.
This stage of the service change process gives opportunities to:
- design proposals with a range of staff, service users, carers, voluntary, community, social enterprise, local government and other partners
- test emerging options
- involve the public in criteria setting and options appraisal
This approach enables the programme to gauge views and understand emerging concerns (such as those about transport and accessibility), the impact on the wider system (such as community-based services), and the impact of change on different population groups.
Pre-consultation staff engagement is a critical, but sometimes neglected part of engagement programmes.
The development of evaluation criteria and how proposals are assessed against these criteria must be consistent with the HM Treasury Green Book approach. Where possible, the criteria should be co-designed with stakeholders.
Once the service change programme has developed the options and criteria, they must choose which options will be formally consulted on (if required) and included in the pre-consultation business case.
Stages for deciding on a shortlist of proposals that can be consulted on
1. Draw up a longlist of a wide range of possible options for achieving project objectives and critical success factors. This must include business as usual and a realistic do minimum. These options should be generated through facilitated workshops with stakeholders.
For all given options, apply ‘hurdle’ criteria that must be met to proceed to the next stage (typically including factors such as clinical, financial, workforce and the four/five tests).
2. Draw up a shortlist. The options framework in the HM Treasury Green Book provides a structured approach to identifying and filtering options. Score options against the ‘desirable’ criteria (co-designed with the public where possible)
3. Finalise ranked shortlist or preferred option(s). The preferred way(s) forward is identified at the strategic outline case stage. From a service reconfiguration perspective, this is the pre-consultation business case stage.
Criteria to consider when choosing your preferred way(s) forward are likely to include:
- clinical evidence
- financial modelling
- the whole system impact
- accessibility and travel impacts
- workforce considerations
- the ability to implement options
- the impact of the scheme on inequalities
- the impact of the scheme on environmental sustainability
Clinical evidence
Clinical evidence should:
- demonstrate how proposals respond to clinical needs identified in relevant joint strategic needs assessments and joint local health and wellbeing strategies, the integrated care strategy, ICS joint forward plans and NHS England national strategy
- consider alignment with published guidance on clinical best practice
- identify any clinical co-dependency issues, including any potential impact on the current or future commissioning or provision of other services
Financial modelling for capital and revenue
If service change options require capital, advice should be sought from NHS England (and from DHSC and HM Treasury if appropriate) so it can underpin subsequent provider business case processes.
To test value for money (VFM), we recommend the use of the comprehensive investment appraisal (CIA) model. Doing so at the pre-consultation and decision-making business case (PCBC and DMBC) stages will save time later. If a high-level VFM analysis is included in the PCBC or DMBC, the incremental benefit of the proposal should be shown versus a business as usual scenario.
Service change programmes should carry out sensitivity analysis around key assumptions if these could have a material impact on the outcome. No service change option should be exposed to public engagement or consultation unless before launch:
- there is a high degree of confidence that it can be delivered as proposed
- it does not imply an unrealistic level of capital expenditure or projected spend profiles that cannot be reconciled to available resources and will not be affordable in revenue terms
All options must be affordable within commissioner revenue allocations and provider revenue financial targets.
It’s strongly recommended that the financial and economic models used at the PCBC and DMBC stages continue to be used and further developed at the strategic outline case (SOC), outline business case (OBC) and full business case (FBC) stages. This will help ensure a consistent economic and financial thread runs through all the business cases.
The SOC, OBC and FBC will need to be submitted with a letter of ICB support, confirming the revenue assumptions are aligned with commissioner plans and any operational capital funding.
NHS England will assure all options requiring capital before any public consultation and, where appropriate, will engage with DHSC to ensure:
- each option is sustainable in service, revenue and capital affordability terms
- the scheme size is proportionate
- it is capable of meeting applicable VFM and return on investment criteria
Schemes requiring larger amounts of capital (over delegated limits) will be required to provide more detail and be subject to higher levels of scrutiny before consultation.
Whole system impact
Major service change is likely to have an impact on the whole health system. This could mean other providers lose or gain income because of the change in patient and financial flows.
These impacts must be reflected when evaluating and selecting preferred options.
Accessibility and travel impacts
A large proportion of formal consultation feedback is likely to concern issues for patients beyond the clinical services themselves, such as accessibility, transport links and ambulance availability. It’s therefore important to carry out a comprehensive travel analysis (for example, private car, public transport, transfers and ambulance impacts) where applicable.
The impacts of proposed changes on people living in deprived areas need to be analysed, including potential socio-economic impacts of capital building projects and changes to training and employment opportunities for local people.
Environmental sustainability impacts also need to be covered, such as changes that affect carbon footprint (for example, travel times or modernised estates).
Workforce
Any proposals should consider the workforce implications and ambitions of the NHS Long Term Workforce Plan. There should also be consideration of:
- any known recruitment and retention difficulties
- to what degree current workforce numbers and requirements fit with existing and planned workforce numbers
- what changes might mean for staff travel
- what training and education might be required for any new or existing staff members if you need to grow or develop the workforce
- any feedback to date about the challenges and opportunities
Implementation
When selecting options, it’s important to show there has been consideration of how proposals will be implemented. This includes having approval in principle for any capital investment required.
Revenue and contractual implications should be considered early on in developing and assessing options. The indicative timeline for implementation of different options should also be reviewed. This includes factors like the phasing of building work and need for any decant arrangements.
Pre-consultation business case
The pre-consultation business case (PCBC) is the document that will be assured in stage 2 of the service change process and sets out the options that will be publicly consulted on.
The lead commissioner should prepare the PCBC with involvement from the other stakeholders, including the relevant local authority organisations. The PCBC informs assessment of proposals against the 5 tests for service change.
The PCBC seeks to:
- build alignment between NHS commissioners, local authorities and other stakeholders
- build on the case for change
- demonstrate that all options, benefits and impact on service users have been considered
- demonstrate that the planned consultation will seek the views of service users, members of the public and other stakeholders who the proposals may potentially impact
Schemes should seek advice from NHS England regional teams about PCBC development. Their support will help determine an appropriate and proportionate approach to potential solutions that may have been identified as part of the options appraisal.
Systems should self-assess against the best practice checks set out in annex 2, and in particular pay attention to the red flags. Key areas that need to be considered and articulated in the PCBC are (in no particular order):
- strategic fit
- finance
- clinical quality
- ambulance services and emergency care
- activity
- workforce
- travel
- estates and infrastructure
- communication and engagement
- equality and environmental impact
- IT
- programme management
- risk and resilience
When thinking about these areas, those responsible for service change schemes must be able to demonstrate:
- how the 5 key tests are satisfied
- compliance with key statutory duties (for example, on equalities, the NHS Triple Aim and environmental sustainability)
Failure to adequately consider these could result in the service change being challenged.
A PCBC cannot pre-empt the outcome of public consultation.
Public consultation
Public involvement duties have applied to commissioners and providers for many years and are largely unchanged. However, the Health and Care Act 2022 made it a legal requirement for arrangements for public involvement to secure the involvement of carers and representatives (if any), as well as service users themselves.
Subject to consideration of the feedback from local authorities and NHS England assurance, the NHS commissioner may decide to progress to formal public consultation on the range of options that will be tested with staff, patients and the public.
A formal public consultation must be carefully planned as a specific step or steps within the overall service change programme, with a suitable budget. It’s also strongly recommended that programmes develop and test the public consultation approach with a range of stakeholders, including the relevant HOSC and the public or community groups.
In a formal public consultation, as with previous stages of the process, it’s very helpful to have clinicians leading the dialogue with their peers and local people on proposed changes. This engagement aspect needs to be resourced with training, communication and ongoing support, especially if proposed changes are likely to be contentious.
A considered approach to public consultation
In the case of R (on the application of Cherwell DC) v Oxfordshire CCG [2017] EWHC 3349, the judge, while expressing his reservations about the risks of the approach of splitting the consultation into 2 phases, concluded that on the particular facts of this case there had been no material, significant unfairness.
Stakeholders will want to know how engagement so far has shaped the proposals for consultation. They will also want to be satisfied that a variety of methods have been used to reach different groups in the community and hear their views, particularly groups that experience poorer health outcomes.
Programmes usually draw on a combination of internal resource and externally commissioned support for a formal public consultation, depending on the individual circumstances. Examples of external support that can be commissioned include:
- a telephone or online survey with a representative sample of the local population
- outreach support from voluntary, community and social enterprise sector partners to hear from ‘seldom heard’ groups and communities
- citizens juries and citizens panels
- independent analysis and reporting of consultation feedback from both structured surveys and other engagement activities, to inform decision-making on completion of the consultation
Fair and proportionate
Public bodies are expected to take an approach that is fair and proportionate to the individual circumstances of a proposed service change.
Fair
Acting fairly is an important duty which applies to all public bodies. The courts have established guiding principles for what constitutes a fair consultation exercise, which are known as the ‘Gunning’ principles.
The Gunning principles
- Proposals are still at a formative stage. A final decision has not yet been made, or predetermined, by the decision makers.
- There is sufficient information to give ‘intelligent consideration’. The information provided must relate to the consultation and must be available, accessible and easy to interpret so consultees can provide an informed response.
- There is adequate time for consideration and response. There must be sufficient opportunity for consultees to participate in the consultation. There is no set timeframe for consultation, despite the widely accepted 12-week consultation period, as the length of time given for the consultee to respond can vary depending on the subject and extent of impact of the consultation.
- ‘Conscientious consideration’ must be given to the consultation responses before making a decision. Decision-makers should be able to provide evidence that they took consultation responses into account.
Proportionate
A service change programme must consider the impact of proposals on people who may be affected. As a general rule, the greater the extent of changes and number of people affected, the greater the level of activity that is likely to be necessary.
Location, access and demographic issues need to be considered. For example, service change proposals should think about how a population in a rural area, or children and young people may be particularly affected by a change. These issues also need to be considered when planning participation itself. For example, in a small market town, it may be best to carry out surveys on a market day when there are more people around.
The Working in partnership with people and communities statutory guidance and the Get involved section of the NHS England website provide further useful advice.
The programme should assess the effectiveness of public involvement throughout the formal consultation process. The following are examples of potential issues that may warrant further consideration:
- feedback suggests that the needs of a particular group (possibly with a shared protected characteristic) have not been adequately considered as part of the proposal
- there is an unexpectedly small response from a group that staff anticipated would be significantly affected by the proposal
- a lot of feedback queries the same point, suggesting that it has not been clearly conveyed or there was insufficient information
- the response to a consultation or attendance at public events has been lower than expected
If such issues arise, the programme should try to understand why this is the case and how to address it. This could include attempting different engagement methods or approaching partners for advice on how to reach certain groups.
The importance of taking a responsive approach
In the case of R (Royal Brompton Hospitals NHS Foundation Trust) v The Joint Committee of Primary Care Trusts [2011] EWHC 2986 (Admin) and [2012] EWCA Civ 472, the Court of Appeal noted that a consultation may evolve.
A public body has a “toolbox full of tools at its disposal to deal with objections that need further consideration. It can engage in further consultation… it can commission a further expert report… it can return to the centres to ask for more information… none of these tools [in the toolbox] needs or ought to need an order of the court… courts, should, in general, do so only if there is some irretrievable flaw in the consultation process.”
Decisions on whether to hold a public consultation on proposals for service change as a means to discharge the ‘duty to involve’ should take account of:
- the description of arrangements for patient and public involvement that must be included in an ICB’s constitution in response to its statutory public involvement duty
- any local patient and public involvement strategy or policy documents
- other established practices, undertakings and previous commitments made
Irrespective of how a decision to hold a public consultation is arrived at, the common law duty of procedural fairness and health inequality duties will inform how the consultation should be conducted. As explained above, due regard should also be had to the Public Sector Equality Duty and wider duty to reduce inequalities of access.
Each NHS organisation should satisfy itself that its public involvement duty and duty to consult affected local authorities has been met. In practice, a single, well-resourced consultation period can satisfy commissioners’ and providers’ respective duties.
Public consultation will normally end before local authority consultation. It’s sensible for the outcome of public consultation to feed into local authority health scrutiny decision-making.
The responses to a consultation must be reported fairly, in a format that allows decision-makers to take them fully into account in their considerations.
Analysis of consultation responses
In the case of R (Kohler) v The Mayor’s Office for Policing and Crime [2018] EWHC 1881, the court was not satisfied on the evidence that the deputy mayor herself had read all relevant responses. Further, it was found that there had been a failure to take into account a material point on postponing a decision pending an evaluation of the impact of new technology.
It’s advisable to engage an independent body to run the consultation analysis and brief them on decision-making requirements before the public consultation is launched.
Based on the output of a public consultation, an NHS body may wish to adapt its published proposals to an extent that warrants consideration of further consultation. There should be further consultation if there is a fundamental difference between the proposals consulted on and those which the consulting party subsequently wishes to adopt.
Decision-making
Decision-making business case
Following consultation, the programme should develop a decision-making business case (DMBC) that builds on the pre-consultation business case and enables decision-making. The DMBC explains the rationale for final decision(s) following consultation. Much of the PCBC content can be used to complete the DMBC, which also needs to reflect the responses from consultation and updated information on the proposals.
Progress toward implementation should be informed by a thorough analysis of the consultation results, and careful consideration of the feedback that was received. NHS England and DHSC should be updated about any capital that has been planned. NHS England should be informed of the proposed next steps once all feedback from the consultation has been gathered and analysed. The equality impact analysis should also be updated based on the responses received and consideration given to the need for any action plan to tackle the issues raised.
The commissioner’s decision is to be based on the best balance of clinical evidence and evidence gained through public engagement and consultation. A clear audit trail to evidence how the decision was reached, and the considerations taken, is to be captured. The whole process should be clear, transparent and legally robust.
Any key decisions should be made in public and communicated to the relevant stakeholders.
The DMBC should:
- ensure that the final proposal is sustainable in service, economic and financial terms
- show how views captured by consultation have been carefully considered
- demonstrate that funding has been agreed in principle and that the proposal can be delivered within the planned capital spend
- describe the full range of options on which a decision will be made and show how the views expressed in consultation or engagement informed the final decision.
Clearly communicating ‘you said, we did’ is good practice irrespective of scheme size. This approach can be built from the pre-consultation business case, and the stakeholders’ work will inform the development of the capital investment business case if required.
For more complex schemes, the DMBC may be assured by NHS England before decision-making. The decision on whether the DMBC needs to be formally assured will be discussed at the assurance 2 checkpoint. This ensures that any major changes from the original proposals have been reviewed. It also confirms that the new proposals have been consulted on, are clinically sound and financially viable.
It’s normal for decision-makers to set out a list of recommendations for implementing their decision. This allows continued public involvement and assurance that continuing duties, such as reducing inequalities of access and outcomes, are being met.
Moving into implementation
Benefits realisation
Following the decision on which option (or variant) to take forward, the implementation plan should be updated. This should set out how the changes will be taken forward, when and by whom.
The plan should identify a clear benefits realisation timetable with key milestones against which progress can be monitored. NHS England’s regional teams will offer commissioners support, guidance and ongoing assurance throughout the implementation phase.
System-wide impacts, benefits and drawbacks of a scheme should be identified and monitored following implementation. This forms part of the system’s ongoing delivery of their long-term ambitions.
Ongoing capital processes
For those programmes which require capital, once the DMBC is approved, formal consideration of the capital investment business case can commence.
If a draft strategic outline case (SOC) has been developed, review it after the DMBC stage. Check if the consultation or other work done at this stage requires any changes to the SOC, and update the SOC as needed.
Annex 1. Fundamental criteria for pre-consultation and decision-making business cases and strategic outline case
A set of criteria for the pre-consultation business case (PCBC) has been developed, and aligns with the strategic outline case (SOC) criteria. Ensuring the PCBC follows the 5 case model required by the HM Treasury Green Book guidance will allow you to convert the PCBC and subsequent decision-making business case (DMBC) to a SOC more easily.
This alignment reduces duplication. If the PCBC criteria are met, the PCBC and subsequent DMBC can be used as the foundation for the SOC.
NHS England and DHSC have developed the SOC fundamental criteria to help assess whether the business case is sufficiently robust before the detailed review process is begun. The SOC needs to comply with the HM Treasury Green Book.
For those schemes that are likely to require capital investment, it’s possible to reduce the time taken to produce a SOC by meeting all the criteria set out in this annex. This will also reduce the time between the submission of a SOC and its approval and reduce the risk that a proposal is delayed because it’s deemed not to meet the required SOC criteria.
These criteria are not a checklist or a suggested structure, but a guideline for what to consider and include. NHS England regional reconfiguration leads will be able to offer advice on how to ensure the PCBC is proportionate to your scheme.
Green Book: 5 case model
Strategic case
It demonstrates that the proposal is strategically aligned and is supported by a compelling case for change. It asks: why are you doing this project?
Economic case
It ensures that a wide range of investment options have been evaluated and that the preferred option optimises value for money. It asks: what is the best way of doing it?
Financial case
It demonstrates that the preferred solution is affordable and can be funded. It asks: how will you pay for it?
Management case
It provides assurance that processes and capabilities are in place to ensure that the preferred solution can be successfully delivered. It asks: how will you manage the delivery?
Commercial case
It ensures that any proposed procurement is commercially attractive and viable. It asks: how will you manage procurement?
What criteria should you focus on?
You will not have to complete a SOC for schemes that do not require capital. In this case, your PCBC should meet the criteria in the first 2 table columns (that is ‘1. PCBC only criteria’ and ‘2. PCBC and SOC criteria’).
If your service change scheme will also require capital, you may need to complete both a PCBC and a SOC. In this case, you should be mindful of the overlap between what is needed in both the PCBC and SOC (column 2 of the table) so that you can optimise the work to be completed to reduce duplication.
You will need to consider how and when in your process you will do the work detailed in all 3 table columns. Column ‘2. PCBC and SOC criteria’ shows where there is likely to be most overlap between the content needed for the PCBC and for the SOC. The categories used within the table have been taken from the Green Book: 5 case model. PCBC criteria have been allocated to these sections to support you in reducing duplication.
Where to find out more information on the capital business case processes?
For the development of the SOC – or in cases where the change is capital only – please refer to Capital investment and property business case approval guidance and the HM Treasury Green Book: appraisal and evaluation in central government.
A summary of the SOC criteria is available for your reference. The latest version of the fundamental criteria checklist for the capital business cases, covering SOCs, OBCs and FBCs is published in the NHS England Capital investment and property business case approval guidance
Annex 2. Best practice checks for pre-consultation business case (PCBC)
These are some of the best practice checks that should be undertaken when preparing the PCBC and prior to stage 2 assurance.
Through our review we seek to identify whether any major problems or red flags would risk the proposal not proceeding to a successful conclusion.
A non-exhaustive list of red flags is set out within the assurance checks section below. Red flags are marked with asterisk (*). These red flags have been identified from what we have learned from previous service changes, as well as reflecting on the current financial and operational pressures faced by systems. They may make it harder to set up the service changes for success and thus pose a risk to services for patients.
In applying our assurance approach, we aim to take a flexible and proportionate approach.
5 tests for service change
Key tests
- strong public and patient engagement
- consistency with current and prospective need for patient choice
- a clear clinical evidence base
- support for proposals from clinical commissioners
Example evidence
- a narrative against the tests
- see communications, clinical quality and activity sections below
- documented evidence of support
Additional fifth test
Proposals including significantly reducing hospital bed numbers will have to meet any of the following 3 conditions:
- demonstrate that sufficient alternative provision, such as increased GP or community services, is being put in place alongside or ahead of bed closures, and that the new workforce will be there to deliver it
- show that specific new treatments or therapies, such as new anti-coagulation drugs used to treat strokes, will reduce specific categories of admissions
- demonstrate a credible plan to improve performance without affecting patient care where a hospital has less efficient bed use than the national average (for example, in line with the Getting it Right First Time programme).
Example evidence to meet 1 of the 3 conditions
- analysis of alternative provision and workforce plan
- clinically approved analysis of admissions reductions anticipated with new treatments or therapies (clinical senates and regional medicines optimisation committees may be sources of independent advice)
- analysis of hospital bed efficiency, a credible plan to improve performance and modelling of its impact
Assurance checks
Strategic fit checks
- Is there evidence of system alignment?*
- Is there alignment with integrated care system (ICS) delivery?
- Has there been an inclusive, transparent scenario-development process (which includes a robust options appraisal) that is coherent with case for change, programme objectives and insight obtained?*
- Has a full robust options appraisal been undertaken (including network approach, cooperation and collaboration with other sites and organisations). Where the proposal requires capital funding is the options appraisal Green Book compliant?*
- Has macro-impact been properly considered including on other organisations and systems?
- If 1 or more of the NHS trusts or foundation trusts within the system has any current formal ICS or NHS England escalated oversight arrangements, do the proposals consider and seek to address the quality related issues?*
- Does the proposal align to the aims of national strategies and targets?
Example evidence
- documented evidence of ICS support, for example, from Partnership Board or all system alternative and the proposal contributes to the ICS 5-year plan delivery
- narrative demonstrating alignment and interdependencies
- options appraisal which demonstrates a long-to-shortlisting process, methodology and underpinning criteria
- an options appraisal that is Green Book compliant where capital is required
- analysis of macro-impact
- evidence of how the proposals address NHS England or the Care Quality Commission’s concerns over the system’s quality issues, as appropriate
Clinical quality checks
- Does the proposal facilitate a population health approach, seek to address population health management or health improvement priorities in the service delivery of the change?*
- Has there been a full impact analysis of the proposals across ICB and any NHS England commissioned services and shared sign up of all parties to the analysis?
- Is there clear articulation of quality, experience and outcome benefits quantified where possible?
- Does the clinical case fit with best practice or emerging national models?
- Have all key clinical interdependencies have been fully considered?
Example evidence
- evidence that the proposal has taken account of relevant national and local plans (for example, local maternity and neonatal systems, local Green Plan)
- feedback from early stakeholder engagement demonstrating that key system partners are supportive of proposed options
- analysis of impact on ICB and NHS England commissioned services, including potential co-dependencies and unintended consequences, endorsed by relevant parties.
- alignment with ICS delivery
- modelling demonstrating contribution to the gaps against national strategies and targets
- core narrative and communications materials
- clinical case for change
- reference to evidence base (such as national clinical director reports, NICE, royal colleges, new models of care) and national strategies
- independent clinical assurance by clinical senate or appropriate other body
Ambulance services and emergency care checks
- Have the implications for ambulance services (emergency and patient transport services) been identified and impact assessed, and appropriate discussions been held with ambulance service providers?
- Have the implications for emergency care provision been identified, and impact assessed, and appropriate discussions been held with emergency care providers?*
Example evidence
- impact assessment
- statement from ambulance service
- statement from emergency care providers
Finance checks
- Are the proposals financially deliverable, affordable and value for money?*
- Are planned savings reasonable and realistic?
- If NHS England has concerns over the system’s finances, do the proposals consider and seek to address these concerns?* These could be cases where:
- 1 or more NHS trust or foundation trust has enforcement in place relating to financial matters
- 1 of more ICBs has enforcement in place relating to financial matters
- 1 or more organisation with a significant underlying deficit and no plan for achieving sustainability
- Is it clear how the proposal fits into the ICS long-term financial plan and estates strategy? Is the contribution to achieving financial balance for the health economy clearly stated and robust?
- Are the impacts on all providers and commissioners understood?
- Is there a reasonable level of financial risk assessment undertaken with supporting sensitivity analysis and downside planning and mitigation?
- Are the transitional costs (including revenue and capital) identified and properly accounted for? Is there a clearly identified source of funding for transitional costs (capital and revenue)?*
- Is there a clearly identified source of capital funding to support the proposal? Have the capital investment implications been considered in terms of the viability, deliverability and sustainability of the proposal and the economic (value for money and return on investment) impact? Have a number of capital funding options been considered?*
- Is the proposal a strategic capital priority for the ICS?
- Is each option for consultation sustainable in service and revenue and capital affordability terms and can each option demonstrate that it is proportionate and that it is capable of meeting applicable VFM and return on investment criteria?
- Is there a financial model underpinning the analysis, including costed models to support transformation and service reconfiguration proposals?
- Does the financial modelling have a robust starting point (for example, alignment to allocation and system envelopes, understanding of underlying position)?
- Are demand management and activity growth assumptions reasonable in the context of national benchmarks? Is there evidence to support the expected impact of proposed new models of delivery?
- Is the financial modelling consistent with the workforce and activity modelling?
Example evidence
- business case, including worked through financial models
- evidence of aligned financial, workforce and activity models (such as ICS level financial and activity model)
- evidence of how the proposals address NHS England concerns over the system’s finances
- detail on key assumptions used in financial modelling and sensitivity analysis and testing on these assumptions
- capital investment implications and clear source for all options – status of any application for capital is explicit in business case and public facing documents
- confirmation of capital affordability should include a clearly identified source of capital funding that aligns with current NHS capital investment policy and requirements
- revenue and capital affordability of each consultation option is confirmed with appropriate modelling and comparison to base case
- NHS England, programme or HM Treasury correspondence indicating a clearly identified source of capital funding, both in terms of scale of investment and timescale
Activity checks
- Are all relevant patient flows and capacity properly modelled, and are assumptions clear and reasonable?*
- What are the changes in bed numbers?
- Is activity and capacity modelling clearly linked to service change objectives?
- Is the activity linked consistently to workforce and finance models?
- Has there been modelling of significant activity, workforce and finance impacts on other locations and organisations?*
Example evidence
- outputs of accurate modelling with assumptions clearly stated and sensitivity analysis
- clear explanation of changes to bed numbers and application of NHS beds test
- narrative explaining link between modelling and service change objectives
- aligned financial, workforce and activity models
- evidence that impacted organisations support the implication of the outputs of the financial, workforce and activity models
- analysis of key risks and any mitigating actions
Workforce checks
- Do you have a workforce plan integrated with finance and activity plans?*
- Are you making most effective use of your workforce for service delivery and is it compliant with all appropriate guidance?
- Have you considered the implications for future workforce?
- Have staff been properly engaged in developing the proposed change?
Example evidence
- supply high level workforce risks and mitigating actions
- statement of assurance, including reference to appropriate standards
- changes to provider learning development agreements
- evidence of appropriate staff engagement
Travel checks
- Has the travel impact of proposed change been modelled for all key populations, including analysis of available transport options, public transport schedules and availability and affordability of car parking?*
- Has there been consideration of the environmental impact of changes to travel?
Example evidence
- travel impact assessment
- evidence (possibly in the form of a sustainability impact assessment) about how net zero/greener NHS ambitions have been built into plans (noting that for some proposals balance may be needed between clinical sustainability and net zero ambitions)
Estates and infrastructure checks
- Have credible analyses been done on activity, capacity and design that align with current estates strategies at site, provider and ICS levels? Are indicative capital costs based on standard benchmarks, following all design, technical, building and space requirements? Have site limitations and important nearby facilities been identified and planned for?
- Has there been consideration given to the most effective use of estates?
- Has there been consideration given about how the proposed change will contribute to greener NHS and net zero ambitions?
Example evidence
- outputs of activity analysis clearly linked with estates strategy
- capital costs clearly identified (see finance section) and confirmation they comply with the standards described
- estates impact assessment
- evidence (possibly in the form of a sustainability impact assessment) about how net zero and greener NHS ambitions have been built into plans (noting that for some proposals balance may be needed between clinical sustainability and net zero ambitions)
Communications and engagement checks
- Are there plans to appropriately and effectively engage and involve all stakeholders appropriately and fulfil commitments under public involvement duties?* Stakeholders to include:
- staff in affected service
- patients
- carers
- the public
- Healthwatch
- GPs
- media
- local authority overview and scrutiny functions
- health and wellbeing boards
- MPs
- voluntary and community sector strategic partners
- other partners and organisations
Example evidence
- involvement or consultation plan
- draft consultation document
- a clear and well-reasoned public and stakeholder involvement strategy
- communications plan, including stakeholder map with timelines, key messages, named clinical spokespersons, sample materials, plans to reach seldom heard groups, and resource identified to deliver the plan
- PCBC should detail engagement with all parties to date, issues identified, and responses to issues
Equality impact checks
- Has there been an appropriate assessment of the impact of the proposed service change on relevant, diverse groups?
- Does the proposal seek to address health inequalities that exist within the system?*
- Has engagement taken place with any groups that may be affected?
- What action will be taken to mitigate any adverse impacts?
Example evidence
- completed equality impact assessment and action plan
- evidence that decision-making arrangements will pay due regard to equalities issues
IT checks
- Does the proposal support the ICS digital strategy?
- Does the proposal make best use of technology?
- Has there been an assessment of the impact on local informatics strategy and IT deployments?
- Are there likely to be any data migration costs or implications for specialist or network technology/equipment contracts associated with the service?
Example evidence
- evidence of a review of how technology may support the service change been undertaken
- detail of any changes to local informatics strategy and deployment plan, including information flows and governance. Key risks are highlighted and mitigating actions identified
Programme management checks
- Are there robust programme and risk management arrangements?
- Are there clear and comprehensive succession plans to mitigate against effects of turnover within the programme team?*
- Are there clear plans for how each option will be implemented?*
Example evidence
- gateway review report and response to recommendations
- evidence of clear and comprehensive succession plans
- clear plan for delivery of the options
Risk and resilience checks
- Has there been consideration of how to identify and reduce privacy risks?
- How will the proposed change impact on the ability of the local health economy to plan for, and respond to, a major incident?*
- Has a business impact analysis been conducted for all impacted organisations and appropriate changes made to business continuity plans?
- Has there been a local health resilience partnership impact assessment on resilience?
- Has there been a clear consideration of statutory duties under the NHS Act 2006, as mentioned in this guidance? (for example, general duties on ICBs on 14Z32 to 14Z44)
Example evidence
- conduct a privacy impact assessment
- statement of assurance
- evidence the proposed service change and the impact on resilience has been assessed at the local health resilience partnership business impact analysis
Annex 3. NHS England support and further resources
National support
The Service change and reconfiguration page on the NHS Futures Collaboration Platform (registration required) has been developed to support you through the service change process. It explains the national support offer, where to go for regional support, and allows access to a range of resources and forums. It’s recommended that you request access to this page as soon as possible.
Regional support
Before starting any service reconfiguration, your first point of contact should be with your NHS England regional service reconfiguration lead. They have the expertise to guide you through the process.
Their contact details can be found through the NHS Futures Collaboration Platform page.
Skills development
Regional strategy and transformation teams can offer support to build skills and strengthen delivery, including:
- expert advice and support from senior leaders
- sharing of best practise and networking
- resources, tools and templates
- training modules, including business case development
- tailored hands-on support, including for engagement and consultation
More information on current support offers can be found on the Futures Collaboration Platform page.
General guidance by theme
Capital
- Capital investment and property business case approval guidance for NHS trusts and foundation trusts
- Green Book: appraisal and evaluation in central government
- Guide to developing the project business case
- Guide to developing the programme business case
Communication and engagement
- Communications and engagement toolkit for people working in areas of deprivation
- The Cabinet Office Consultation Principles (2018)
Environmental
- NHS England – Evergreen sustainable supplier assessment
- Greener NHS Knowledge Hub – Future Collaboration Platform
Health inequalities and equality
- NHS England’s statement on information on health inequalities
- A national framework for NHS – action on inclusion health
- Core20PLUS5 (adults) – an approach to reducing healthcare inequalities
- Working in partnership with people and communities: statutory guidance
- Health inequalities within the southeast region through a service change lens
Scrutiny
Healthwatch
Partnership working
Workforce
Statutory guidance
- Statutory guidance on the new intervention power for the Secretary of State (January 2024)
- NHS England – Delivering a ‘Net Zero’ National Health Service
- Working in partnership with people and communities
Annex 4: Statutory and general duties relating to service change and reconfiguration in England
The information below summarises selected key statutory duties that should be considered in relation to service change proposals in England.
Careful consideration of these duties, alongside consideration of this guidance, may help reduce the risk of legal challenge and call in by the Secretary of State.
The focus of this annex is the duties which apply to integrated care boards (ICBs) and NHS England. The description of the duties is provided in summary form. As always, we would strongly advise that you consider the full text of the legal provisions and liaise with your regional lead, clinical senate and, where necessary, seek your own legal advice.
Key statutory duties under the NHS Act 2006 (as amended)
NHS England and its general functions
NHS England duty
S1H(2).
Description of duty
NHS England is subject to a duty concurrently with the Secretary of State to continue the promotion in England of a comprehensive health service designed to secure improvement in:
- the physical and mental health of the people of England
- the prevention, diagnosis and treatment of physical and mental illness
Secretary of State’s Mandate to NHS England
NHS England duty
Section 13A(7).
Description of duty
NHS England must seek to achieve any objectives and comply with any requirements specified in the Secretary of State’s Mandate to NHS England.
Duty of ICBs to commission certain health services
ICB duty
Section 3.
Description of duty
An ICB must arrange for the provision of the matters listed in section 3 (such as hospital accommodation, nursing and ambulance services) to such extent as it considers necessary to meet the reasonable requirements of the people for whom it has responsibility.
In exercising its functions, an ICB must act consistently with:
- the discharge by the Secretary of State and NHS England of their duty to promote a comprehensive health service
- the objectives and requirements specified in the Secretary of State’s Mandate to NHS England
Duty to promote the NHS Constitution
ICB duty
Section 14Z32.
NHS England duty
Section 13C.
Description of duty
NHS England and ICBs must, in the exercise of their functions, act with a view to securing that health services are provided in a way which promotes the NHS Constitution and awareness of the NHS Constitution among patients, staff and members of the public.
Duty as to effectiveness, efficiency and economy
ICB duty
Section 14Z33.
NHS England duty
Section 13D.
Description of duty
NHS England and ICBs must exercise their functions effectively, efficiently and economically.
NHS trusts and foundation trusts have equivalent duties under sections 26 and 63 of the NHS Act 2006 respectively.
Duties as to improvement in quality services
ICB duty
Section 14Z35.
NHS England duty
Section 13E.
Description of duty
NHS England and ICBs must exercise their functions with a view to securing continuous improvement in the quality of services provided to individuals for, or in connection with:
- the prevention, diagnosis or treatment of illness
- the protection or improvement of public health
In discharging these duties, NHS England and ICBs must in particular, act with a view to securing continuous improvement in the outcomes that are achieved from the provision of the services. Those outcomes include, in particular, outcomes which show the effectiveness of the services, the safety of the services and the quality of the experience undergone by patients.
In discharging this duty, NHS England must also have regard to documents published by the Secretary of State for these purposes and quality standards published by NICE.
Duties as to reducing inequalities in access and outcomes
ICB duty
Section 14Z35.
NHS England duty
Section 13G.
Description of duty
NHS England and ICBs must, in the exercise of their functions, have regard to the need to:
- reduce inequalities between persons with respect to their ability to access health services
- reduce inequalities between patients with respect to the outcomes achieved for them by the provision of health services
Those outcomes again include the effectiveness of the services, the safety of the services and the quality of the experience undergone by patients.
Duty as to patient choice
ICB duty
Section 14Z37.
NHS England duty
Section 13I.
Description of duty
NHS England and ICBs must, in the exercise of their functions, act with a view to enabling patients to make choices with respect to aspects of health services provided to them.
Duty to obtain appropriate advice
ICB duty
Section 14Z38.
NHS England duty
Section 13J.
Description of duty
NHS England and ICBs must obtain advice appropriate for enabling them to effectively discharge their functions from appropriate persons who (taken together) have a broad range of professional expertise in the prevention, diagnosis or treatment of illness and the protection or improvement of public health.
Duty to promote innovation
ICB duty
Section 14Z39.
NHS England duty
Section 13K.
Description of duty
NHS England and ICBs must, in the exercise of their functions, promote innovation in the provision of health services (including innovation in the arrangements made for their provision).
Duty in respect of research
ICB duty
Section 14Z40.
NHS England duty
Section 13L.
Description of duty
NHS England and ICBs must, in the exercise of their functions, facilitate or otherwise promote research on matters relevant to the health service, and the use in the health service of evidence obtained from research.
Duty to promote education and training
ICB duty
Section 14Z41.
NHS England duty
Section 13M.
Description of duty
So as to assist with the duty of the Secretary of State and NHS England under section 1F (to secure an effective system for the planning and delivery of education and training), NHS England and ICBs must, in exercising their functions, have regard to the need to promote education and training for persons who are employed, or who are considering becoming employed, in an activity which involves or is connected with the provision of services as part of the health service in England.
Duty as to promoting integration
ICB duty
Section 14Z42.
NHS England duty
Section 13N.
Description of duty
Where NHS England and ICBs consider that doing so would: improve the quality of the services (including the outcomes that are achieved from their provision); reduce inequalities between persons with respect to their ability to access those services; or reduce inequalities between persons with respect to the outcomes achieved for them by the provision of those services, they must exercise their functions with a view to securing that:
- health services are provided in an integrated way
- the provision of health services is integrated with the provision of health-related services or social care services
Duty to have regard to the wider effect of decisions (the Triple Aim)
ICB duty
Section 14Z43.
NHS England duty
Section 13NA.
Description of duty
In making decisions about the exercise of their functions, NHS England and ICBs must have regard to all likely effects of those decisions in relation to:
- the health and wellbeing of the people of England
- the quality of services provided to individuals by the NHS or in pursuance of arrangements made by the NHS, or in connection with the prevention, diagnosis or treatment of illness, as part of the health service in England
- efficiency and sustainability in relation to the use of resources by relevant bodies for the purposes of the health service in England
In discharging this duty NHS England and ICBs must have regard to any guidance about the Triple Aim which NHS England may publish under section 13NB.
NHS trusts and foundation trusts have equivalent duties under sections 26A and 63A of the NHS Act 2006 respectively.
Duties as to climate change
ICB duty
Section 14Z44.
NHS England duty
Section 13NC.
Description of duty
NHS England and ICBs must, in the exercise of their functions, have regard to the need to:
- contribute towards compliance with the UK net zero emissions target (under the Climate Change Act 2008) and certain environmental targets (under the Environment Act 2021)
- adapt to any current impacts of climate change identified in reports on the assessment of risks of climate change laid before Parliament by the Secretary of state under section 56 of the 2008 Act
In discharging this duty NHS England and ICBs must have regard to any guidance about such matters which NHS England may publish under section 13ND.
NHS trusts and foundation trusts have equivalent duties under sections 26B and 63B of the NHS Act 2006 respectively.
Other key statutory duties
Public Sector Equality Duty (PSED)
Source
Section 149, Equality Act 2010.
Description
The PSED imposes a duty on public bodies, in the exercise of their functions, to “have due regard” to the need to:
- eliminate discrimination, harassment victimisation and any other conduct that is prohibited by the Equality Act 2010
- advance equality of opportunity, and foster good relations, between people who share a relevant protected characteristic and people who do not share it
The full text of section 149 is available on the gov.uk website. The Equality and Human Rights Commission has published Technical guidance on the Public Sector Equality Duty: England.
Duty to have regard to the NHS Constitution
Source
Section 2, Health Act 2009.
Description
In performing health service functions, NHS bodies (and other specified bodies) must have regard to the NHS Constitution.
Duty to have regard to assessments and strategies
Source
Section 116B, Local Government and Public Involvement in Health Act 2007.
Description
In exercising their functions, NHS England and ICBs (and local authorities) must, so far as relevant, have regard to:
- any joint strategic needs assessment prepared in relation to the responsible local authority’s area
- any joint local health and wellbeing strategy prepared by the responsible local authority and ICB
- any integrated care strategy prepared in relation to the area
Armed Forces Covenant Duty
Source
Section 343AA Armed Forces Act 2006.
Description
In exercising their healthcare functions, including functions under the NHS Act 2006, NHS England, ICBs, trusts and foundation trusts must have due regard to:
(a) the unique obligations of, and sacrifices made by, the armed forces
(b) the principle that it is desirable to remove disadvantages arising for service people from membership, or former membership, of the armed forces, and
(c) the principle that special provision for service people may be justified by the effects on such people of membership, or former membership, of the armed forces.
Regard must also be had to statutory guidance issued under section 343AE.
Key public involvement and consultation statutory duties
Public involvement and consultation
Duty
- NHS England: Section 13Q, NHS Act 2006.
- ICBs: Section 14Z45, NHS Act 2006.
- (NHS trusts and NHS foundation trusts have similar duties under section 242 NHS Act 2006).
Description of duty
In relation to any health services which are, or are to be, commissioned by NHS England or ICBs, those bodies must make arrangements to secure that individuals to whom the services are being or may be provided, and their carers and representatives (if any), are involved (whether by being consulted or provided with information or in other ways) in:
- the planning of the commissioning arrangements
- the development and consideration of proposals by them for changes in the commissioning arrangements where the implementation of the proposals would have an impact on the manner in which the services are delivered to the individuals (at the point when the service is received by them) or the range of health services available to them
- decisions of NHS England affecting the operation of the commissioning arrangements where the implementation of the decisions would (if made) have such an impact
Review and scrutiny by the local authority
Duty
- Regulation 21, The Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) Regulations 2013.
Description of duty
Regulation 21 enables a local authority to review and scrutinise matters relating to the planning, provision and operation of the health service in its area. It sets out duties that the local authority must discharge in carrying out such review and scrutiny. Regulation 21 also sets out duties that apply where a matter is referred to a local authority by a local Healthwatch organisation or a representative of such an organisation.
Consultation with the local authority
Duty
- Regulation 23, The Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) Regulations 2013 [as amended by the Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) (Amendment and Saving Provision) Regulations 2024].
Description of Duty
Regulation 23 confers a duty, and sets out a procedure around, consulting with the local authority, where NHS England or an ICB (or service provider) has under consideration any proposal for substantial development of the health service in the area of the local authority, or for substantial variation in the provision of such service.
There are some exceptions to this requirement, such as where the responsible commissioner is satisfied that a decision has to be taken without allowing time for consultation because of a risk to safety or welfare of patients or staff.
The Secretary of State has published guidance on local authority health scrutiny.
Secretary of State’s intervention powers in relation to the reconfiguration of NHS services
Duty to notify the Secretary of State of reconfiguration proposals
Source
Paragraph 2 of Schedule 10A, NHS Act 2006. [See also: The National Health Service (Notifiable Reconfigurations and Transitional Provision) Regulations 2024].
Summary
If NHS England or an ICB proposes a notifiable reconfiguration of NHS services, it must notify the Secretary of State.
A proposal will be notifiable if it is one which would oblige consultation with the local authority under Regulation 23 of the 2013 Regulations described above (that is if it amounts to a substantial development of the health service or a substantial variation in the provision of such a service).
The Secretary of State publishes statutory guidance about these intervention powers, which NHS bodies must have regard to.
Secretary of State’s power to call-in a reconfiguration of services
Source
Paragraph 3 of Schedule 10A, NHS Act 2006.
Summary
The Secretary of State may give an NHS commissioning body a direction calling in any proposal by the body for the reconfiguration of NHS services. This can be as a result of a person requesting that the Secretary of State does so, or may be of the Secretary of State’s own volition.
The Secretary of State may, within the period 6 months beginning with the date of the direction calling-in the proposal, take any decision in relation to the proposal that could have been taken by the ICB. This could include the Secretary of State:
- deciding whether a proposal should, or should not, proceed, or should proceed in a modified form
- deciding particular results to be achieved by the ICB in taking decisions in relation to the proposal
- retaking any decision previously taken by the ICB
Any decision taken, and reasons for it, must be published by the Secretary of State.
Before exercising this power the Secretary of State is required to give the ICB and/or NHS England (as relevant), the local authority and any other person who the Secretary of State considers appropriate, an opportunity to make representations.
The statutory guidance referred above provides guidance on how the Secretary of State will exercise this function.
Secretary of State’s power to direct a reconfiguration of services
Source
Paragraph 5 of Schedule 10A, NHS Act 2006.
(Not yet in force)
Summary
The legislation anticipates that the Secretary of State will be granted the power to direct NHS commissioners to consider a reconfiguration of NHS services. Any such direction, and reasons for it, must be published by the Secretary of State. However, this power is not yet in force as of 25 June 2026.
Annex 5: NHS England thresholds for assurance decisions on service change
The level at which assurance decisions for service change will be made is determined by the criteria below:
1. The relevant NHS England national committee or board will review the assurance conclusions and take decisions for all schemes where 1 or more of the following conditions applies:
- requires transition or transaction support of more than £20 million from NHS England funds (not including ICB funds)
- the total turnover of the affected services (for all sites impacted by the transition, at current prices) is above £500 million in any 1 year
- the likely capital value of the scheme is above £100 million (gross capital value of the scheme, even if the actual value is lower because it’s funded through capital receipts)
- The proposed service change impacts on any NHS trust or NHS foundation trust that is in segment 4 and red capability of NHS England’s NHS Oversight Framework
2. The NHS England chief financial officer will review the assurance conclusions and take decisions for all schemes where 1 or more of the following conditions applies:
- impact on any of the distressed health economies as currently or subsequently defined (given ICBs were not segmented in 2025/26, this is likely to be linked to an ICB’s NHS Oversight Framework segment and/or capability assessment)
- requires transition or transaction support from NHS England funds (not including ICB funds)
- the total turnover of the affected services (for all sites impacted by the transition, at current prices) is above £350 million in any 1 year
- the likely capital value of the scheme is above £50 million (gross capital value of the scheme, even if the actual value is lower because it is funded through capital receipts)
3. All other schemes to be determined by the relevant regional director.
Publication reference: PRN01528